intravenous therapy - mchest.com · definition 2. signs and symptoms 3 ... providing drug...
TRANSCRIPT

- 1 -
INTRAVENOUS THERAPY
PROCEDURE MANUAL

- 2 -
LETTER OF ACCEPTANCE
__________________________________________ hereby approves (Facility)
the attached Reference Manual as of _____________________. (Date)
The Intravenous Therapy Procedure Manual will be reviewed at least annually or more often when deemed appropriate. Revisions will be
reviewed as they occur.
Current copies of the Intravenous Therapy Procedure Manual shall be maintained at each appropriate nursing station.
I have reviewed this manual and agree to its approval.
__________________________ (Administrator)
__________________________ (Director of Nursing)
__________________________ (Medical Director)

I
TABLE OF CONTENTS
TABLE OF CONTENTS INTRODUCTION
A. Purpose 1
B. Local Standard of Practice 1
RESPONSIBILITIES
1
1
1
A. Responsibilities: M Chest Pharmacy
B. Responsibilities: Administrator
C. Responsibilities: Director of Nursing Services (DON/DNS)
D. Skills Validation 2
AMENDMENTS
GUIDELINES
A. Resident Candidacy for IV Therapy 1
B. Excluded IV Medications and Therapies 1
C. Processing the IV Order 1
D. IV Solutions/Medications: Storage 2
E. IV Solutions/Medications: Handling 3
F. IV Solutions and Supplies: Destroying and Returning 4
G. IV Tubing 5
H. Peripheral IV Catheters and Needles 6
I. Central Venous Devices 7
J. Documentation and Monitoring 8
K. IV Medication Administration Times 9
L. Emergency IV Supplies 10

II
TABLE OF CONTENTS
PROTOCOLS
A. IV Antibiotic 1
1. Purpose
2. Guidelines
3. Nursing Responsibilities
B. IV Push 2
1. Purpose
2. Guidelines
C. Anaphylaxis Allergic Reaction 4
1. Purpose
2. Guidelines
3. Nursing Responsibilities and Interventions
4. Signs and Symptoms of Anaphylaxis
5. Drugs Used to Treat Anaphylaxis
6. Physician Protocol
PRACTICE GUIDELINES
A. Purpose 1
B. Personnel 1
C. Competencies 1
D. Definitions 1
E. Resident Outcome 2
F. Staff Outcome 2
G. System Outcome 2
H. Implementation Parameter 3
I. Area of Intervention Responsibility 4
1. Assessment
2. Planning
3. Implementation
4. Outcome Evaluation
5. Documentation

III
TABLE OF CONTENTS
PROCEDURES
A. Peripheral IV: Insertion of a Catheter or Needle 1
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
B. Peripheral IV: Conversion of a Continuous IV to a Heparin Lock 6
1. Purpose
2. Equipment
3. Procedure
4. Documentation
C. Peripheral/Midline Catheter Flush 8
1. Purpose
2. Policy
3. Equipment
4. Procedure
D. Peripheral IV: Site Monitoring 10
1. Purpose
2. Guidelines
3. Procedures
4. Documentation
E. Peripheral IV: Removal 12
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
F. Peripheral IV: Intermittent Medication Administration via a Heparin Lock 14
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
IV
TABLE OF CONTENTS
PROCEDURES (Continued)
G. Central Venous Catheters: Dressing Change 17
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
H. Central Venous Catheters: Cap Change 21
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
I. Central Venous Catheters: Heparinization 24
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
J. Central Venous Catheters: Intermittent Medication Administration 27
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
K. Central Venous Catheters: Removal 29
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
L. Peripherally Inserted Central Catheters (PICC) and Extended
Peripheral Catheters: Care and Maintenance 32
1. Purpose
2. Guidelines
3. Procedure
4. Documentation

V
TABLE OF CONTENTS
PROCEDURES (Continued)
M. IV Solutions: Bag or Container Change 35
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
N. IV Tubing: Change 37
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
O. IV Tubing Intermittent Therapy via Secondary Line (IV Piggy Back) 39
1. Purpose
2. Guidelines
3. Equipment
4. Procedure
5. Documentation
P. IV Flow Rate: Calculating 42
1. Purpose
2. Guidelines
CONTINUOUS QUALITY IMPROVEMENTS/QUALITY ASSESSMENT INDICATOR (CQI/QAI)
PROGRAM
A. Purpose 1
B. Methods 1
C. Implementation 1
D. Areas of Responsibility 1
1. Director of Nurses (DON)
2. Consultant Pharmacist
3. CQI/QAI Council
VI
TABLE OF CONTENTS
CONTINUOUS QUALITY IMPROVEMENTS/QUALITY ASSESSMENT INDICATOR (CQI/QAI)
PROGRAM (Continued)
E. Audit Process 2
Annual Continuous Quality Improvement Activities Calendar 3
CQI/QAI Council Quarterly Report 4
CQI/QAI Data Collection Tool Aspect of Care: Central Venous
Access Device 5
CQI/QAI Data Collection Tool Aspect of Care: Intravenous
Tubing/Solutions 6
CQI/QAI Data Collection Tool Aspect of Care: IV Pumps – Electronic 8
CQI/QAI Data Collection Tool Aspect of Care: Peripheral
Intravenous Device 9
CQI/QAI Monitoring Tool Aspect of Care: Central Venous Access Device 10
CQI/QAI Monitoring Tool Aspect of Care: Intravenous Tubing/Solutions 11
CQI/QAI Monitoring Tool Aspect of Care: IV Pumps – Electronic 13
CQI/QAI Monthly Meeting Suggested Agenda 14
CQI/QAI Monthly Monitoring Tool 15
INFECTION CONTROL
A. Purpose 1
B. Special Considerations for the Nursing Staff 1
C. Special Consideration for the Housekeeping Staff 1
D. Infection Control Methods 2
E. Disposal of Contaminated Waste 2
F. Management of IV Related Infections 3
COMPLICATIONS MANAGEMENT
A. Purpose 1
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
B. How to Use This Section: Nursing Process Actions 1
C. Peripheral IV: Hematoma 1
1. Definition

VII
TABLE OF CONTENTS
COMPLICATIONS MANAGEMENT (Continued)
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
D. Peripheral IV: Infiltration 3
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Preventative Measures
E. Peripheral IV: Phlebitis 4
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
F. Peripheral IV: Site Infection 5
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
G. Peripheral IV: Clotting 6
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
H. Peripheral IV: Catheter Embolism 7
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
VIII
TABLE OF CONTENTS
COMPLICATIONS MANAGEMENT (Continued)
I. Peripheral and Central Venous Catheters: Air Embolism 9
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
J. Central Venous Catheters: Occlusion 10
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
K. Central Venous Catheters: Deep Vein Thrombosis 11
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
L. Central Venous Catheters: Local Infection 13
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
M. Systemic Infection 15
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
N. Circulatory Overload 17
1. Definition
2. Signs and Symptoms
3. Possible Causes
4. Nursing Actions
5. Prevention Measures
IX
TABLE OF CONTENTS
FORMS
A. Annual IV Skills Competency Validation Checklist – Use to validate staff skills
B. CQI/QAI Forms – Use these forms with CQI/QAI/QA processes, facility specific
Annual Continuous Quality Improvement Activities Calendar
CQI/QAI Council Quarterly Report
CQI/QAI Data Collection Tool Aspect of Care: Central Venous Access Device
CQI/QAI Data Collection Tool Aspect of Care: Intravenous Tubing/Solutions
CQI/QAI Data Collection Tool Aspect of Care: IV Pumps - Electronic
CQI/QAI Data Collection Tool Aspect of Care: Peripheral Intravenous Device
CQI/QAI Monitoring Tool Aspect of Care: Central Venous Access Device
CQI/QAI Monitoring Tool Aspect of Care: Intravenous Tubing/Solutions
CQI/QAI Monitoring Tool Aspect of Care: IV Pumps - Electronic
CQI/QAI Monitoring Tool Aspect of Care: Peripheral Intravenous Device
CQI/QAI Monthly Meeting Suggested Agenda
CQI/QAI Monthly Monitoring Tool
C. IV Medication Sheet – Use for documenting nursing actions for routine IV
medications
D. IV Piggy Back Competency Validation Checklist – Use to validate staff skills
E. IV Starts Competency Validation Checklist – Use to validate staff skills
F. Peripheral IV Starts Competency Validation Checklist – Use to validate staff skills
G. Physician’s Protocol for Anaphylaxis – Us for initial/first dose antibiotics
- 1 -
QUALIFICATIONS FOR CONTROL OF PROGRAM
POLICY
To identify the qualifications of the person supervising, directing, and
controlling the IV program.
PROCEDURE
The person designated for the direction, supervision, and control of the
IV Program must:
1. Be a licensed Physician or Registered Nurse of this State.
2. Be knowledgeable of Facility Policy and Procedure
3. Be knowledgeable of State Regulations pertaining to the IVprogram.
4. Have knowledge of infection control as it relates to IV
Therapy.
5. Be responsible for participating in the quality assurance of the
program.
6. Attend ongoing education programs related to IV Therapy.

- 1 -
INTRODUCTION
This IV Reference Manual was developed to guide a nurse working in a long-term care facility.
This manual was written for Registered Nurses with IV Therapy
experience and for LVN/LPNs who are qualified in IV Therapy.
A. Purpose
The purpose of this reference manual is to:
1. Establish uniform policies, procedures, practice guidelines andprotocols for long-term care facilities.
2. To serve as reference and standard for members of the healthcare team.
3. Provide criteria to measure the effectiveness of IV Therapy in
a long-term care setting.
B. Local Standard of Practice
1. Amendments made to this manual by the local governingbody shall supersede the information contained herein when
the amendment is added to the reference manual.
2. The physician’s order shall in every instance override thepractice guidelines and protocols outlined in this reference
manual. The licensed nurse shall be accountable for clarifying
orders in this reference manual. The licensed nurse shall beaccountable for clarifying orders which present a conflict with
this reference manual. The clarification of the physician’sorder shall be documented according to the facility medical
records procedures.

- 1 -
RESPONSIBILITIES
A. Responsibilities: M Chest Pharmacy
M Chest Pharmacy will be the primary supplier of all IV
solutions, supplies and equipment necessary to provide the IV
therapy. On occasion, another pharmacy may be designated by
M Chest Pharmacy. It is the responsibility of the facility to
notify M Chest Pharmacy of IV orders in a timely manner.
The pharmacy will be directly responsible for, but not limited to,
the following:
i. Providing IV drugs prepared aseptically, on a timelybasis, 24 hours/day.
ii. Monitoring all IV drugs for dose appropriateness.iii. Providing Pharmacist and/or IV Registered Nurse
consultant.iv. Providing drug information as requested; i.e., drug
incompatibility, dosage and side effects.v. Providing delivery and preparation of all drugs, supplies
and pumps according to State and Federal guidelines.
vi. Providing an IV emergency kit.vii. Monitoring use of and replacing used IV emergency kit.
viii. Replacing supplies in a timely manner.
B. Responsibilities: Administrator
The administrator is responsible for approving the reference manual.
C. Responsibilities: Director of Nursing Services (DON/DNS)
The DON/DNS is responsible for providing adequate 24-hour
coverage with IV qualified licensed staff, in accordance to State and Federal regulations. The DON/DNS will maintain RN and
LVN/LPN performance of IV procedures in accordance to the
State Board of Nurse Examiners rules and regulations.

- 2 -
RESPONSIBILITIES D. Skills Validation
The LVN/LPN’s IV technique must be demonstrated, approved
and documented by an IV RN, Director of Nursing Services or other designated qualified nurse. This validation will be
documented on the IV Starts Competency Validation Checklist or
the Annual IV Skills Validation Checklist.

- 1 -
REFERENCE MANUAL REVISION/UPDATE RECORD The individual facility using this reference manual may make revisions
specific to the needs of the facility’s operations. Any revisions made should be noted in this record and the resulting written documents
added to the appropriate section of the Table of Contents and the applicable section.
DATE SECTION ITEM OLD
PAGES
NEW
PAGES
SIGNATURE

- 1 -
GUIDELINES I. Resident Candidacy for IV Therapy
1. The resident medically needs an IV and the diagnosis is on
the chart.
i. If the IV therapy is ordered for four (4) or more weeks,
it is recommended that the patient have a venous access device placed.
ii. The resident has adequate vascular access to complete
the course of ordered IV Therapy.
2. The IV solutions are medically safe for IV administration.
3. A physician initiates the orders and is available for complications and emergencies.
II. Excluded IV Medications and Therapies
1. Investigational drugs.
2. Chemotherapy Agents
3. Total Parenteral Nutrition (TPN)
4. IVs in lower extremities, unless specifically ordered by a physician.
5. Removal of clots from an IV catheter by irrigation. Refer to
declotting procedure.
III. Processing the IV order
1. The IV order should be received from a physician by either verbally or written form. The order shall then be faxed or
phoned in to the pharmacy, transcribed onto the IV
Medication Sheet, Telephone Order Slip (if appropriate) and Physician Order Sheet. When completed, the order will be
signed and dated.
2. A licensed nurse must call or fax in all IV orders or refills for solutions and medications.
- 2 -
GUIDELINES 3. Stat IV orders must be called into the pharmacy by a nurse as
soon as the order is received.
4. A complete IV order should include the following:
Primary IV Order
i. Resident’s Name
ii. Diagnosis for IV Therapy iii. Route (central or peripheral)
iv. IV solution, volume v. Any additives
vi. Rate, length of therapy vii. Heparin flush strength, volume and frequency
viii. Doctor’s Name ix. Date, Time and nurse’s signature if a telephone order
Heparin Lock/IVPB
i. Resident’s Name
ii. Diagnosis for IV Therapy
iii. Route (central or peripheral) iv. Medication (strength/dose)
v. Frequency of administration vi. Length of therapy
vii. Rate of infusion viii. Normal saline flush before and after medication
ix. Heparin flush strength, volume and frequency x. Doctor’s Name
xi. Date, Time and nurse’s signature if a telephone order
5. Licensed practitioner orders without specific time frame as to duration of therapy will have a facility stop order policy.
i. IV solutions _______ days
ii. Antibiotic therapy _______ days
IV. IV Solutions/Medications: Storage
1. Solutions should remain in their original packaging until ready for use

- 3 -
GUIDELINES
2. Solutions should be stored in a cool, dry area unless
refrigeration is indicated.
i. Remove one (1) liter bags from the refrigerator 1 hourprior to infusion.
ii. Remove bags containing more than one (1) liter 2 hoursprior to infusion.
iii. Remove 50-250 cc bags from the refrigerator ½ hour
before infusion.
iv. DO NOT USE MICROWAVE to warm IV bags: unevenheating may occur.
v. Do not expose IV solutions to direct sunlight.
3. Adequate refrigerator space to store solutions and
medications must be provided.
4. The refrigerator temperature should be set between 36° and
46° F to maintain stability.
5. Upon delivery, arrange older solutions so they will be infusedbefore the more recently prepared solutions.
V. IV Solutions/Medications: Handling
1. All IV solutions will be changed every 24 hours once spiked.
2. The nurse hanging the IV solutions/medications will label the
bag with the date, time and initials.
3. All IV solutions with medications added by the pharmacist willbe labeled according to pharmacy procedures.
4. If an IV rate has been changed from the rate stated on thepharmacy label, the facility nurse should label the IV
container with the current rate and notify the pharmacy.
5. IV solutions/medications will be administered within the StateGuidelines for that drug category.

- 4 -
GUIDELINES
6. All IV solutions/medications will be documented on the IV
Medications Sheet or approved facility form.
7. All IV containers will be inspected for integrity, including:
i. Cracks---if bottle form
ii. Cloudiness or discolorationiii. Damage to container
iv. Particlesv. Expiration date
8. All solutions/medications will be labeled and billed as resident
specific items.
9. All supplies and pumps will be provided and billed as residentspecific items.
VI. IV Solutions and Supplies: Destroying and Returning
1. All IV narcotic drugs will be destroyed by a pharmacist and
RN (or according to state and federal regulations) and
documented.
2. Return Drug Rules and Regulations vary by state and shouldbe made available by the IV pharmacy provider.
3. The following items may not be returned:
i. Narcotic IV medications
ii. Medications pre-mixed in a syringe, bag or bottleiii. TPN solutions
iv. Contaminated or damaged preparations, unless relatedto a resident reaction.
v. Opened or expired medications, solutions or suppliesvi. IV bags or bottles without a prescription label attached.
4. Only unopened plain IV solutions, factory added KCl andsupplies may be returned to the pharmacy with the
prescription label intact for credit to the resident’s account.Refer to #2 above.

- 5 -
GUIDELINES
5. IV solutions prepared with an Add-Vantage bag and vial or
snap vial and bag may be returned to the pharmacy with the prescription label intact if done so before the 4 week
expiration for credit to the resident’s account if/when the IV solution is used for another patient.
6. It is the facility’s responsibility to return all resident specific IV equipment within the billing month. The resident’s account
will then be credited.
VII. IV Tubing
1. All IV tubing should be labeled when hung with date, time and nurse’s initials.
2. Tubing should be changed as follows:
i. Continuous peripheral IV tubing is to be changed every
24 hours unless otherwise specified by facility. ii. Continuous central line tubing is changed every 24
hours.
iii. Intermittent IV Therapy via heparin or saline lock tubing is changed every 24 hours and the needle or needleless
connector is changed before every dose administration. iv. IV piggyback or secondary tubing is changed every 24
hours. v. All IV tubing and needles should be changed
immediately upon suspected contamination, or if not labeled with a date and time hung.
3. All tubing changes will be documented consistently.
4. All tubing connections will be secured with a luer locking
system or line connections securing device.
- 6 -
GUIDELINES
VIII. Peripheral IV Catheters and Needles
1. All peripheral venous catheters and needles will be changed
every 72 hours and PRN signs or symptoms of complications.A physician’s order is required to leave an IV in for longer
than 72 hours, except where the manufacturer of the device
has provided FDA clearance for longer dwell times
2. Manufacturer written recommendations will serve as theguideline for specific venous access device dwell times.
3. Residents with limited access and long-term therapy should
be considered for a central venous access, deep peripheralaccess or midline access devices.
4. Only radiopaque IV catheters should be used.
5. Products should be inspected for integrity and sterility. All
damaged products should be reported to the pharmacy andnot used on a resident.
6. Discard all IV needles and stylets, uncut/unclipped, uncappedin a rigid one-way sharps container, which has a clear
observation panel.
7. A new sterile IV catheter or needle is required for every IVinsertion attempted.
8. All peripheral IVs will have an injection cap extension set
attached to the catheter hub to maintain a closed system.The injection cap extension set will be changed with routine
IV site changes.
9. Transparent film dressings will be changed with every IV siterotation, if it becomes soiled or non-occlusive (non-adherent)
to the skin.
10. Transparent film dressings will be changed every 72 hours.

- 7 -
GUIDELINES
11. If a gauze dressing is used, and the site cannot be visualized,
the dressings will be changed every 24 hours to permit assessment of the site for complications.
12. All IV dressings should be labeled with date, time gauge,
length of IV canula and nurse’s initials.
I. Central Venous Devices
1. All central lines will be luer lock capped or have a luer lock
infection cap extension set applied to maintain a closed system.
2. Extension sets and/or injection caps will be changed twice
weekly with the dressing change and PRN leakage or suspected contamination.
3. A smooth Dravon clamp will be at the bedside of every
resident with a central venous catheter except Groshong catheters and PICC lines.
4. A transparent film dressing is the preferred type of central line dressing for ease of site assessment. This transparent
film dressing is changed weekly and PRN soiling, contamination and non-occlusiveness (non-adherent).
5. A gauze dressing may be used for the first 24 hours after the
insertion of a central venous device. The gauze dressing should be changed every 24 hours and PRN saturation or
dislodgement.
6. If a 2x2 gauze is used under the transparent dressing, then the dressing should be changed every 24 hours to permit
assessment of the site.
7. All dressings should be labeled with date, time and nurse’s
initials.
8. Heparin flushes must be ordered by the physician and should include strength, amount and frequency of flushing.
- 8 -
GUIDELINES
9. Heparin flushes are intended to maintain patency by filling the IV device, to prevent blood coagulation.
10. Recommended flushing guidelines:
i. 1-3 cc of 100 units/cc of Heparin Flush solution per lumen or multi-lumen catheters.
ii. Heparin Flush solution at a volume 1.5 times the internal volume of the catheter/device.
iii. Implantable vascular access devices (Mediport, Port-a-
cath, etc.) are accessed and flushed every month with 5cc of Heparin Flush solution 100 units/cc. Accessed ports are flushed and maintained using the standard flush protocol.
11. A 5cc Normal Saline flush should be used to flush central line IVs before and after medication administration.
12. Finish with Heparin flush.
13. A positive pressure flushing technique should be used.
14. Acetone alcohol must not be used on or near the central venous catheter.
J. Documentation and Monitoring
1. The IV Medication Sheet is part of the medical record.
2. All IV medications, solutions and flushes will be documentedon the IV Medication Sheet or facility specific form.
3. Intake and Output records are maintained for all residents
receiving hydration and electrolyte replacement. IV Intakerecords are appropriate when intermittent IV Piggyback in
small volumes is the single IV therapy.
4. All IV procedures will be documented consistently on the IV
Medication Sheet or in the progress notes. Areas to bedocumented should include:

- 9 -
GUIDELINES
i. IV insertion documentation: Catheter type, gauge and
length, insertion site, number of insertion attempts, type of dressing, type of flush used and amount,
resident’s response, date, time and nurse’s signature. ii. Routine shift monitoring documentation: IV site
appearance and location, signs and symptoms of
complications and interventions, resident’s response to therapy, date, time, and signature.
iii. Removal of IV device removed, location of device removed, resident’s response, date, time and
signature.
5. Documentation should be done at least every shift
6. All documentation will include date, time and IV nurse’s signature or initials.
7. All residents receiving IV Therapy need a nursing care plan
reflecting the goals and outcomes of therapy.
8. Routine charting in the progress notes should be done
according to facility, State and Federal regulations.
K. IV Medication Administration Times
1. Medication administration times may differ from the standard medication pass time schedule.
2. If an IV medication dose is off schedule by more than one (1)
hour, the following actions should be taken:
i. Record the actual IV medication administration time in both the IV Medication Sheet and Resident Progress
Notes; include the reason for variance in administration time.
ii. Re-time IV medication dosing schedule
iii. Continue with therapy, using new time schedule iv. Notify MD
v. Notify Pharmacy

- 10 -
GUIDELINES
L. Emergency IV Supplies
1. An emergency locked IV kit will be provided for the facility by M Chest Pharmacy.
2. A backup infusion control device may be provided for the
facility.
3. Emergency supplies are to be stored according to facilitypolicy.
4. Use of the Emergency Kit is to be documented on the
Emergency Kit Usage form and faxed to the pharmacy so thatthe correct patient’s account is charged. Items used from the
kit and not charged to a resident will be charged to thefacility.
5. The pharmacy will exchange opened emergency kits on a
routine basis. The nurse opening the IV Emergency kit isresponsible for notifying the pharmacy and completion of the
Patient Charge Slip.

- 1 -
PROTOCOLS A. IV Antibiotic
1. Purpose: Antibiotic therapy is the administration of
medication, specifically designed to destroy organisms causing infections. The intravenous route is used to
maintain a therapeutic blood level and produce an effect to
eradicate or reduce infective agents.
2. Guidelines
i. Only FDA approved drugs will be administered ii. Drugs will be reconstituted per manufacture’s
recommendations and guidelines. iii. Antibiotics will be available and administered within
State guidelines. iv. IV first dose recommendations:
1. Resident has no known history of allergic reactions
to the ordered medication or related medications. 2. Will be determined on a case-by-case basis
a. The nurse receiving the antibiotic order
should request PRN orders for allergic/anaphylactic reaction and
document these orders
3. Nursing Responsibilities
i. Know the resident’s allergy profile. ii. Notify the pharmacy of all resident allergies.
iii. Know facility’s policy and procedures for allergic reactions to drugs.
iv. Know signs and symptoms of a drug allergy response. v. Observe the resident closely during the first through the
third dose of a new antibiotic for signs and symptoms of an adverse allergic reaction.
vi. Administer the medication on time and infuse as
ordered. vii. Monitor the resident for a minimum of every 30 minutes
during antibiotic infusion. viii. If the resident exhibits any signs of an allergic reaction
or anaphylaxis: (loss of consciousness, shock, hives, sudden onset of pain)
- 2 -
PROTOCOLS 1. Stop IV agent
2. Establish/maintain airway 3. Call 911 and attending physician
4. Maintain a patent IV 5. Have normal saline or lactated ringers available
6. Refer to Anaphylaxis/Allergic Reaction Protocol
B. IV Push
1. Purpose: IV push medication administration is the direct
injection of undiluted medication into a vein. IV pushes are used to:
Administer a bolus dose of a drug
intravenously Administer a drug that cannot be diluted; i.e.
Lasix Give an emergency dose to provide an
immediate drug effect Achieve immediate peak drug levels in the
bloodstream
2. Guidelines
i. All IV push medications must be administered by an IV
qualified nurse, based upon facility specific job descriptions or individual State Board of Nurse
Examiner’s rules and regulations. ii. IV push medications may be injected directly into the
vein, through an existing IV line, or through a heparin lock.
iii. If using a pre-existing IV line:
1. Use the closest injection port to the catheter 2. Close the roller clamp on the tubing to prevent
back flow of medication
3. Flush with normal saline 0.9% 1cc 4. Give the IV push medication, using correct rate
5. Flush with normal saline 0.9% 1cc using the same rate as the IVP medication
6. Open the roller clamp and resume the infusion

- 3 -
PROTOCOLS
iv. Residents will be monitored closely throughout the
entire administration time and IV push will be stopped immediately if any adverse reaction occurs.
v. Complications of any medication administered IV may include “speed shock” or anaphylaxis. Specific
complications will relate to the individual drug
administered. vi. The qualified nurse, administering IV push
medications is responsible for knowing:
1. The indication for the drug 2. Usual IV actions, adverse actions and side effects
3. Rate of administration 4. Dilution factors, if any, required by manufacturer
5. Monitoring and assessment parameters for the medication.
v. Categories of IV push drugs may include: diuretics,
corticosteroids, dextrose, anti-emetics, narcotics and antihistamines.
vi. IV push medication considerations should include
expertise of staff and the type of monitoring required (i.e. cardiac monitor) in evaluating the
appropriateness of administration in the long-term care setting.
- 4 -
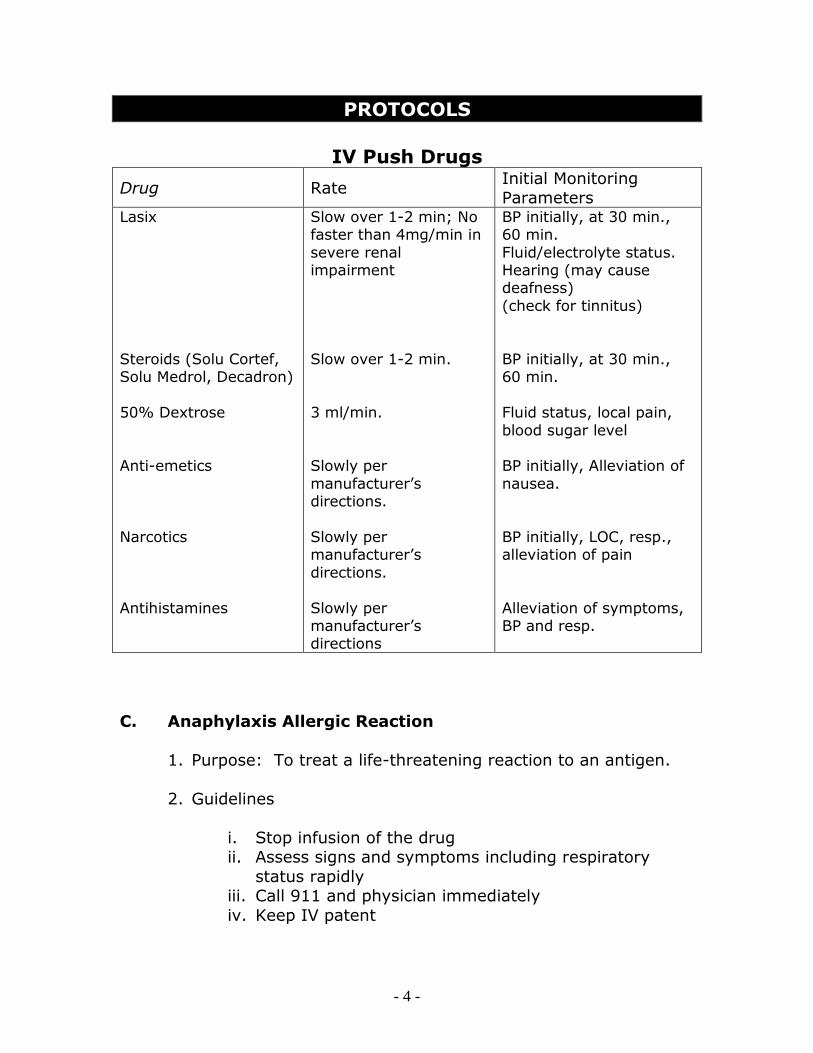
PROTOCOLS
IV Push Drugs
Drug Rate Initial Monitoring Parameters
Lasix
Steroids (Solu Cortef, Solu Medrol, Decadron)
50% Dextrose
Anti-emetics
Narcotics
Antihistamines
Slow over 1-2 min; No faster than 4mg/min in
severe renal impairment
Slow over 1-2 min.
3 ml/min.
Slowly per
manufacturer’s directions.
Slowly per manufacturer’s
directions.
Slowly per manufacturer’s directions
BP initially, at 30 min., 60 min.
Fluid/electrolyte status. Hearing (may cause deafness)
(check for tinnitus)
BP initially, at 30 min., 60 min.
Fluid status, local pain,
blood sugar level BP initially, Alleviation of
nausea.
BP initially, LOC, resp., alleviation of pain
Alleviation of symptoms, BP and resp.
C. Anaphylaxis Allergic Reaction
1. Purpose: To treat a life-threatening reaction to an antigen.
2. Guidelines
i. Stop infusion of the drug ii. Assess signs and symptoms including respiratory
status rapidly iii. Call 911 and physician immediately
iv. Keep IV patent

- 5 -
PROTOCOLS
v. Be ready to start IV infusion of normal saline or
lactated ringers and to administer epinephrine. vi. Monitor resident’s vital signs. If resident becomes
hypotensive, elevate his legs and keep him supine. vii. If cardiopulmonary arrest occurs, initiate resuscitation
(or in accordance with Advance Directives).
3. Nursing Responsibilities and Interventions
i. Always check resident’s allergy history before
treatment ii. Be cautious with residents who have many allergies
iii. Know the location and contents of the IV emergency supply kit.
iv. Know your local emergency unit telephone number and send second rescuer to call.
v. Check vital signs frequently (every 10-15 minutes) until resident is transported. If resident remains at
facility assess vital signs every 15-30 minutes for the first four hours after onset of the reaction.
vi. Observe and record changes in respiratory or
cardiovascular status for severe reactions, look for another reaction 12-24 hours later.
**Note: The resident is still at risk for
bronchospasms, upper respiratory obstructions, tachycardia and hypotension for 24 hours after
reaction.
4. Signs and Symptoms of Anaphylaxis
i. Dermatologic: First symptoms most commonly seen may include the following: pruritus (itching), urticaria
(skin eruption, also called hives), angioedema (swelling involving the hands, feet, face, neck, larynx
and genitalia).
ii. Respiratory: Shortness of breath, difficulty breathing, wheezing, cyanosis and choking
iii. Central Nervous System: Headache, Dizziness, Seizures, decreased level of consciousness, syncope
iv. Cardiovascular: Rapidly falling blood pressure, thready pulse, chills and sweating
- 6 -
PROTOCOLS v. Gastrointestinal: Cramping, diarrhea (sometimes
bloody), incontinence, nausea and vomiting.
5. Drugs Used to Treat Anaphylaxis
i. Drug: Diphenhydramine hydrochloride (Benadryl)
Classification: Antihistamine
Indications and Actions: Relieves the
symptoms of allergic reactions and treat allergic manifestations such as rash, urticaria,
angioneurotic edema. Decreases allergic response by blocking the action of histamine.
Dosage and Route: 25-50 mg PO, IM or IV
every 4-6 hours.
Nursing Considerations:
Administer IV doses slowly 25 mg/min as
ordered by physician. Monitor resident for therapeutic response
Drug may cause hypotension, dizziness and drowsiness; exercise environmental
safety measures.
ii. Drug: Epinephrine Hydrochloride (Epi-Pen)
Classification: Adrenergic, sympathomimetic
Indications and Actions: Relieves the symptoms of acute hypersensitivity reactions
including anaphylaxis, asthma, angioneurotic edema, bronchospasm and allergic reactions.
Acts directly on alpha and beta adrenergic
receptors. Relaxes smooth muscles, causes bronchodilation, cardiac stimulation, increases
blood pressure, inhibits histamine release, decreases syntheses and release of chemical
mediator.
- 7 -
PROTOCOLS Dosage and Route: 0.1 – 1.0 ml of 1:1,000 SC
or IM every 10-15 min.; 1-3 ml of 1:10,000 IV slowly over 3-5 min., may repeat every 10-15
min. or follow by a continuous infusion. 1-4 mcg/min. continuous IV (mix 1 ml of 1:1,000
epinephrine in 250 ml D5W to get a
concentration of 4 mcg/ml.)
Nursing Considerations:
Double check drug concentration before administration, 1:1,000 is for SC or IM,
1:10,000 is for IV use. Onset OF Action is 3-5 min. after SC or
IM administration, 1 min. after IV administration.
Use a large vein and infusion controller or pump for IV administration or give as
a push through the injection port of the IV tubing.
Monitor resident for therapeutic
response. Call 911
Monitor blood pressure and heart rate Do not use if solution is discolored.
iii. Drug: Hydrocortisone (Solu-Cortef)
Classification: Corticosteroid
Indications and Actions: Relieve allergic and
inflammatory conditions including anaphylaxis, respiratory distress, angioneurotic edema,
urticaria. Decreases capillary permeability and inhibits synthesis of mediators.
Dosage and Route: 5-30 mg PO every 6-12 hrs; 100-250 mg IM, IV every 4-12 hours.
- 8 -
PROTOCOLS Nursing Considerations:
Monitor resident for therapeutic
response. Monitor fluid and electrolyte balance, I &
O and blood pressure.
Taper medication, per physician order, when discontinuing.
Onset of action is 20 minutes after IM or IV administration.
6. Physician Protocol
Suggested protocol for physician approval in event of anaphylaxis
i. Assessment Parameters
1. Loss of consciousness
2. Rapid rise or fall in blood pressure, pulse or
respiratory rate (from baseline values) 3. Rapid onset of chest or back pain, or general
discomfort within five minutes of initiating infusion.
4. Acute, rapid onset of respiratory distress.
ii. Planning Parameters
1. Rapidly evaluate vital signs and symptoms 2. Positive assessment finding for Anaphylaxis
Reaction
iii. Implementation Parameters
1. Stop IV Infusion
2. Start infusion of Normal Saline 0.9% 500cc to infuse at 100cc/hr
3. Immediately have another staff member notify physician, nurse to remain with patient
4. Administer Epinephrine 0.5cc of 1:1000 (Epi-pen) SC, may repeat in 3-5 minutes
- 9 -
PROTOCOLS 5. Administer Diphenhydramine (Benadryl) 50 mg
IVP or SC, one time dose 6. Notify Emergency Medical Service of need for
transport (for severe reactions) 7. If respiratory distress present, Oxygen at 4-6
liters/minute
iv. Evaluation Parameters
1. Reassess vital signs every 5 minutes or until
stable 2. Assess airway, respiration and heart rate
3. Start CPR, if cardiopulmonary arrest occurs 4. Assess need for supplemental Oxygen
v. Documentation Parameters
1. Document course of events in detail
2. Document implementation of protocol and specific actions taken, medications administered.
3. Document resident’s response/disposition.
4. Complete incident report according to facility guidelines

- 1 -
PRACTICE GUIDELINES A. Purpose
This practice guideline is provided as a suggested tool for use by
facilities that provide IV Therapy services. Implementation of this practice guideline should occur after the facility has reviewed and
approved it for use.
B. Personnel
The practice guideline is implemented by a Registered Nurse, Licensed
Vocational or Practical Nurse. Licensed Vocational or Practical Nurses function under the direction of a Registered Nurse.
C. Competencies
Documentation is on file that the nursing staff has received in service
education on Intravenous Therapy. The individual personnel file shall be the permanent file.
D. Definitions
1. Intravenous Therapy (IV): Administration of solutions and medications via venous access devices.
2. Peripheral venous access: Intravenous access line that is placed in the extremities and the tip of the device does not extend into
the central body core. 3. Central Venous Access: Intravenous access line that is placed in
the extremities, chest wall or upper thigh and the tip of the device extends into the central body core.
4. SASH: Protocol for flushing an intravenous line—S=saline flush, A=administer drug, S=saline flush and H=heparin flush.
(Heparin concentration for this protocol is 10 u/cc) 5. Rate Control Device: A mechanical, disposable device used to
control the rate of flow of an IV solution. (May be Dial-a-flow, Intermate, Volutrol, etc.)
6. Electronic Pump: An electronic device, programmable, to control
the rate of flow of an IV solution. 7. Central Arterial Access: Intra-arterial access line which is placed
in any artery. This facility does not admit or retain residents requiring arterial line monitoring.
- 2 -
PRACTICE GUIDELINES E. Resident Outcome
1. The resident at risk for fluid volume excess or depletion receives appropriate intervention.
2. The resident at risk for infectious disease process receives appropriate intervention.
3. The resident with active infections will receive appropriate
intervention. 4. The resident at risk for pain is identified.
5. The resident with active pain receives the appropriate pain intervention.
6. The resident at risk for clinical malnutrition is identified. 7. The resident with actual malnutrition receives appropriate
intervention.
F. Staff Outcome
1. Nursing staff identify at risk factors present in resident. 2. Nursing staff implements early interventions for prevention of
complications. 3. Nursing staff notify physician for appropriate medical orders.
4. Nursing staff implement the correct Resident Assessment
Protocol, i.e., Dehydration, Dementia, Fluid Maintenance or Nutrition.
5. Nursing staff update the comprehensive plan of care to reflect condition.
G. System Outcome
1. The subject of Intravenous Therapy intervention is part of every
Registered Nurse and Licensed Vocational or Practical Nurse’s in service education.
2. The education program for Intravenous Therapy includes information on the following:
i. Risk factors and customary interventions
ii. Types of access and performance techniques
iii. Equipment – mechanical and electronic iv. Scope of practice
- 3 -
PRACTICE GUIDELINES v. Nursing process – Fluid volume assessment; intake and
output assessment; signs and symptoms of complications; laboratory value interpretation.
vi. Non-invasive interventions for managing volume abnormalities, nutritional needs and symptoms of infections
processes.
vii. Instruction of accurate documentation of resident data.
3. Facility Administration provides and has on hand the necessary procedures and supplies to implement the correct
interventions.
H. Implementation Parameter
1. Assess a resident for implementation of this practice guideline whenever any of the following at risk factors are
demonstrated or elicited on assessment.
i. Resident becomes confused or has altered mental status from usual state.
ii. Resident exhibits decreased or intake of food and fluids.
iii. Resident displays decreased urine output, concentration of urine.
iv. Resident displays chronic or acute onset of constipation. v. Resident develops peripheral edema, not resolved by
usual measures. vi. Resident displays shortness of breath or dyspnea or
exertion or has diminished endurance. vii. Resident has elevated temperature, increase or decrease
in heart rate. viii.Resident has wounds or lesions which are inflamed,
draining or painful. ix. Resident complains of unrelenting pain at rest or on
exertion. x. Resident complains of pain not relieved by oral or topical
analgesia.
- 4 -
PRACTICE GUIDELINES I. Area of Intervention Responsibility
Area of Responsibility Interventions
1. Assessment 1.1 The licensed nurse observes the resident
and reviews the MD and RAP: Nutritional
Status; Dehydration and Fluid Maintenance and Delirium for the
following risk factors: Fluid volume excess/deficit
Decreased food/fluid intake Change in vital signs
Decreased urine output Chronic constipation
Wounds/lesions Respiratory changes
Edema Pain
Alteration in mental status Signs/symptoms of infection
1.2 The Dietary Manager observes the resident at mealtime and reviews the MDS
and RAP for weight loss, sudden change in eating habits, chewing or swallowing
problems, refusal supplements.
1.3 The licensed nurse reviews pertinent laboratory values for variance to normals,
albumin and protein and creatinine levels. The licensed nurse evaluates the need for
monitoring of laboratory values.
2. Planning 2.1 The licensed nurse collaborates with the physician and the members of the
interdisciplinary team to develop a CPC
for the resident. This plan is individualized and periodically
reevaluated.

- 5 -
PRACTICE GUIDELINES 2.2 The nursing staff maintains a
current list of all residents identified at risk of needing intravenous therapy.
2.3 The nursing staff maintains a
current list of all residents who are
actively on intravenous therapy.
3. Implementation 3.1 Interventions for Volume Deficit
Resident is placed on intake and output
Color character and quality of urine is assessed.
Skin turgor is assessed daily. Bowel habits are monitored
daily. The nurse aide reports hard
stool or frequent diarrhea to the nurse.
Assess for altered mental
status-may be slow onset. Consider need for IV hydration.
3.2 Interventions for Volume Excess
Monitor intake of fluids
Review medications for diuretic effectiveness
Elevate extremities Assess for anti-embolism
stockings Ambulate resident more
frequently Measure urine output
Evaluate need for
laboratory work up Observe for shortness of
breath or dyspnea Assess for crackles or rales
in lung fields

- 6 -
PRACTICE GUIDELINES Assess for weakness,
diminished endurance Assess for acute onset of
altered mental status Consider IV medications for
increased effectiveness
3.3 Interventions for Malnutrition
Observe and record food
intake Monitor weight more
frequently Observe skin integrity
Observe for listlessness or obtundedness
Refer for dietician consult Confer with physician for
lab work up Consider Total or
Peripheral Parenteral
Nutrition
3.4 Interventions for Pain
Assess pain using pain scale
Assess activity that causes onset of pain
Assess for patterns in pain abatement/onset
Evaluate for causes of break through pain and
return to prior functional status
Interview patient for pain
history and psycho-social aspects and interventions
Administer oral analgesia as necessary
Confer with physician for topical analgesia
- 7 -
PRACTICE GUIDELINES Consider IV pain
management – continuous or patient
controlled with nurse bolus
3.5 Interventions for Infectious Disease Processes
Assess for open wounds, lesions,
pressure areas Assess weekly and record
assessment Observe for intermediate changes
in wounds.
Observe color, odor, quantity, character and location of
drainage Observe for redness, warmth,
pain in affected area. Review need for culture and
sensitivity. Observe sputum for color and
consistency Observe urine for color and
consistency. Consider IV antibiotics
4. Outcome Evaluation 4.1 The resident’s status and response to
the interventions are reassessed.
5. Documentation 5.1 The resident’s CPC includes specific data
on:
Who should provide the care The frequency of care or
observation Supplies and equipment needed
How the care is undertaken
- 8 -
PRACTICE GUIDELINES 5.2 There is daily documentation of the
medical record of the resident at risk to conditions treated by IVs that nursing
assessment and observation has occurred.
5.3 The results of the interventions, the care provided, adjustments in the
interventions and the response are documented in the residents medical
chart.
- 1 -
PROCEDURES
A. Peripheral IV: Insertion of a Catheter or Needle
1. Purpose: To provide venous access for the administration of fluids and/or medications.
2. Guidelines
a. Plastic radiopaque catheters shall be used for routine peripheral venous access
b. Winged-tip needles may be used for short-term (8 hours) or
one-dose infusions.
c. Always use the smallest, shortest device possible to achieve efficient delivery with minimal irritation to the lumen of the
vein
d. Stylets are never to be re-inserted into plastic catheters, since this may puncture and/or sever the catheter, causing
catheter embolism
e. A new sterile IV catheter or needle is required for every IV
insertion attempted
f. Peripheral IV sites shall be changed routinely every 72 and PRN complications unless a doctor’s order is received to keep
the line in longer.
g. Residents with poor venous access may extend time between IV site changes with a physician’s order and if no signs or
symptoms of complications are present
h. Gloves shall be worn to start all IVs
i. Attempts to initiate IV access: total of seven as follows:
First facility nurse- Two (2) attempts
Second facility nurse – Two (2) attempts IV RN support – Two (2) attempts; one (1) additional
if different device is used

- 2 -
PROCEDURES
j. Cannulas shall not be inserted into veins in the lower
extremities without a physician’s order
k. All peripheral IVs will have an injection cap extension tube attached to the catheter hub, to maintain a closed system.
l. Should hair removal be necessary, never shave hair at the venipuncture site. Clip hair with scissors before starting
procedure.
3. Equipment
a. IV start kit may contain: povidone-iodine prep, alcohol prep(s), tourniquet, 2x2 gauze, tape, ID label, latex gloves,
injection port, 4-6” extension tubing and transparent film dressing.
b. Injection port (if not in start kit)
c. 4-6” extension tubing (if not in start kit)
d. Radiopaque peripheral intravenous catheter (size appropriate 18g to 24g)
e. Sterile 3cc syringe
f. Heparin Flush solution 10 units/cc and Normal Saline 0.9%
flush
4. Procedure/*Key Points
a. Check Physician’s Order
b. Explain procedure to resident and assess veins *To ease fear gain cooperation
c. Wash hands thoroughly *Infection control
d. Assemble equipment on a clean surface and prime injection
plug extension tube.
- 3 -
PROCEDURES e. Apply tourniquet to arm and select venipuncture site.
*Care must be taken to apply tourniquet with enough pressure to impede venous flow and allow arterial flow to
be maintained. Palpation of pulse should be present.
*If limited venous access, apply warm, moist towel around
extremity to aid in vein dilation.
*Start IV Therapy in distal (farthest) point of upper extremities. Avoid bony prominences and areas of flexion.
f. Cleanse site with povidone-iodine working from the center
outward using a circular motion for 30 seconds. Allow 1-2 minutes to dry.
*Always check for iodine allergy and use alcohol as a substitute PRN. Povidone-iodine may be removed with an
alcohol swab for better visualization.
g. Put on gloves *Universal Precaution
h. Inspect intravenous catheter for any defects. Do not pull stylet out of catheter, as this will disrupt the manufacturer
coating applied to ease insertion.
i. Place thumb below intended venipuncture site and gently draw skin toward to secure vein.
j. For Plastic Catheter:
(1) Insert catheter through skin and into vein at 10°-30°
angle with bevel up. Decrease angle and advance about ¼” into vein.
*Do not attempt more than one venipuncture per IV device
(2) Hold the flash chamber of stylet steady and advance plastic catheter over stylet into vein, up to catheter hub.
*Never re-insert stylet after removal from catheter.
(3) Remove tourniquet

- 4 -
PROCEDURES (4) Remove stylet from catheter and attach heparin lock
extension tube.
*To maintain a closed system and reduce risk of infection.
(5) Observe for signs of infiltration at venipuncture site.
*Swelling and/or pain indicate that catheter
k. If IV is to be used for intermittent therapy, flush device with
5cc of Normal Saline 0.9%.
It is necessary to flush with normal saline prior to and after medication administration, since not all medications are
compatible with heparin. Saline flushing will also allow the nurse to assess IV patency. Never use force while flushing.
*Always use positive pressure when flushing an IV.
l. Cover insertion site with transparent dressing, leaving
extension tube connection exposed.
m. Anchor extension tube in a “U” shape with tape.
n. Stabilize extremity on passed arm board or dynamic
wrist/elbow support, if necessary.
*If IV is at point of flexion, immobilization of joint will help maintain IV site.
o. Check and regulate flow rate according to physician’s order.
p. Label IV dressing with the following:
(1) Date and Time
(2) Type, length and gauge of needle
(3) Initials of IV nurse
q. Discard used equipment appropriately.

- 5 -
PROCEDURES 5. Documentation
a. Record the procedure in the resident’s medical record.
Include the following:
1) Date and time of insertion
2) Type, length and gauge of catheter 3) Location of insertion site
4) Number of IV attempts 5) Type of dressings applied
6) Resident’s response 7) Nurse’s signature

- 6 -
PROCEDURES B. Peripheral IV: Conversion of a Continuous IV to a Heparin Lock
1. Purpose: To keep a vein open for intermittent therapy
2. Equipment
a. Heparin Lock – flush syringe
b. Normal saline
c. Injection plug extension tube
d. Alcohol swab
e. 3cc syringe with 20 gauge 1 inch needle or smaller
f. Gloves
3. Procedure/*Key Points
a. Wash hands. Apply clean gloves
*Infection control. Universal precautions.
b. Prime injection plug extension tube with normal saline, leave
syringe in injection cap
*Eliminates risk of recapping syringe
c. Disconnect IV tubing and attach injection plug extension tube to catheter hub.
d. Flush system with 5cc of normal saline
*To check IV patency
e. Flush with heparin lock flush if ordered by physician
*Clean injection plug with alcohol before each needle entry

- 7 -
PROCEDURES 4. Documentation
Document conversion of IV to heparin lock in the resident’s
medical record, the amount of fluid infused on I&O sheet and if continuous IV fluids have been stopped.
a. Include date, time, condition of IV site, location of IV site, IV conversion to heparin lock, and resident’s response to
procedure and nurse’s signature.

- 8 -
PROCEDURES
C. Peripheral/Midline Catheter Flush
1. Purpose: To maintain patency of a peripheral cannula and allow for the administration of incompatible medications.
2. Policy
a. This procedure shall be done:
1. After each use
2. At least every 24 hours
b. Positive pressure shall be used for the flush procedure (i.e. at last ½ cc, simultaneously inject while slowly withdrawing
needle from cap)
c. Flushing with normal saline shall be done prior to and after
administration of medications.
3. Equipment
a. Anti-microbial liquid soap
b. Alcohol swab
c. Optional:
1. 10 ml Syringe filled with 5-10 cc normal saline
2. Sharps Container
4. Procedure
a. Explain procedure to patient
b. Wash hands thoroughly
c. Arrange supplies on a clean surface

- 9 -
PROCEDURES d. Clean the injection cap with alcohol swab, using friction and
let dry.
e. Slowly inject flush solution maintaining positive pressure in the cannula. For needle-less system, follow product
manufacturer’s recommendations.
f. Document procedure in patient’s medical record.

- 10 -
PROCEDURES
D. Peripheral IV: Site Monitoring
1. Purpose: To assure proper infusion of IV solutions, reduce risk of complications, and allow for early detection of IV related
complications.
2. Guidelines
a. IV sites will be monitored at least once every shift by a
licensed nurse
b. Peripheral IV devices will be removed and restarted in another site routinely every 72 hours
*A physician’s order is required to leave an IV in longer
than 72 hours
c. Peripheral IV devices will be removed and restarted in another site at the first sign of complications.
d. Occluded IVs should be removed: NOT irrigated.
3. Procedures/*Key Points
a. Observe IV site for:
1. Edema
*swelling is an early sign of infiltration
2. Redness
*Redness noted in the area of the tip of the catheter and along the vessel is an indication of phlebitis
3. Moisture or exudates at the insertion site
*Check for loose connections. If purulent drainage is present, notify physician immediately. Obtain
cultures of catheter and exit site.

- 11 -
PROCEDURES
b. Palpate the IV site for the following:
1. Tenderness
*Pain indicates early signs of phlebitis.
2. Temperature change
*Coolness can indicate infiltration: heat can indicate infection, inflammation or phlebitis
3. Palpable vein cord
*Hard vein cord indicates phlebitis
4. Observe IV tubing for following:
i. Kinking or obstruction
ii. Flow rate
*Note whether solution is infusing at prescribed rate.
4. Documentation
a. Document clearly all observations of IV in the resident’s
record.
b. Record routine observations in the resident’s medical record. Include the following:
1. IV site appearance, condition and location
2. Signs and symptoms of complications and appropriate actions
3. Resident’s tolerance and response to therapy 4. IV restarts
5. Date and time
6. Nurse’s signature

- 12 -
PROCEDURES E. Peripheral IV: Removal
1. Purpose: To safely remove a peripheral IV catheter or needle
2. Guidelines
a. IV peripheral catheters shall be removed routinely after 72 hours
*A physician’s order is required to lean IV longer than 72
hours
b. IV catheters shall be removed if there is pain, redness, tenderness or swelling noted at the insertion site
c. To determine complete removal of the catheter, the nurse
will observe the appearance of the device and its tip, and note the length. If the catheter does not appear to be intact,
apply tourniquet proximal to site and call physician immediately.
3. Equipment
a. Sterile 2x2 inch gauze
b. Band-Aid
c. Gloves
4. Procedure/*Key Points
a. Wash hands thoroughly
b. Clamp infusion tubing
c. Loosen dressing and tape
*Observe site for signs of infection
d. Apply gloves
*Universal precaution

- 13 -
PROCEDURES e. Holding sterile 2x2 inch gauze pad over site, quickly
withdraw device; pull out in a straight line.
5. Documentation
a. Document procedure in resident’s medical record:
i. Type, length and condition of device removed and
location of site device was removed from.
ii. Reason for catheter removal and condition of site
iii. Indicate actions taken if catheter was removed due to complications
iv. Indicate resident’s response to procedure
v. Date, time and nurse’s signature

- 14 -
PROCEDURES F. Peripheral IV: Intermittent Medication Administration via a
Heparin Lock
1. Purpose: A Heparin lock is used for therapy when a main hydration therapy is not necessary. It allows ready access for intermittent IV
Therapy without requiring multiple needle sticks.
2. Guidelines
a. Intermittent IV Therapy
b. It is recommended to flush the intermittent injection port
with 5cc of normal saline 0.9% before and after the therapy, then finish with the prescribed heparin flush.
c. IV heparin lock injection port tubing should be changed at the
time of routine IV site changes; and whenever the IV site is changed.
d. IV heparin locks offer several advantages to the resident.
These include:
i. Reduced need for multiple needle sticks
ii. Reduced activity restrictions required when on a continuous infusion
iii. Reduced danger of thrombophlebitis, air embolism and circulatory overload
3. Equipment
a. IV catheter or needle
b. Injection plug extension tube or injection cap with luer lock
or luer slip adapter
c. 5cc of normal saline pre-filled syringe with 22 gauge, 1 inch
needle or smaller
d. Tourniquet
e. Tape

- 15 -
PROCEDURES f. Gloves
g. IV start kit
h. IV site dressing
4. Procedure/*key Points
a. Explain procedure to resident
*Refer back to peripheral IV insertion of catheter or needle
b. Wash hands
*Infection control
c. Prime injection plug extension tube with normal saline
d. Start IV using the standard venipuncture procedure
*Gloves are required; universal precautions
e. Connect injection cap or injection plug extension tube to
catheter hub
f. Apply IV dressing according to procedure
g. Flush the device with 5cc of normal saline 0.9%
*To ensure placement, look for pain or swelling
h. When preparing to infuse IV therapy, clean cap with alcohol before entering with a needle
i. Use 5cc of normal saline to flush device
j. Administer IV therapy with an approved device through the injection port
k. Flush again with 5cc of normal saline 0.9%
- 16 -
PROCEDURES *To flush drug out of catheter and prevent a chemical
reaction with heparin
5. Documentation
a. Record flush on the resident’s IV medication sheet and
indicate time schedule for future flushes.
b. Document heparin lock IV insertion in resident’s medical record. Include:
i. Date and Time
ii. Reason for heparin lock placement iii. Insertion site
iv. Number of insertion attempts v. Type, gauge and length of IV device
vi. Dressing vii. Heparin flush volume and strength
viii. Resident’s response ix. Nurse’s signature

- 17 -
PROCEDURES G. Central Venous Catheters*: Dressing Change
*Any vascular access device where the tip of the catheter is in the
body core. Examples include: Hickman Type, Groshong®, Broviac, Subclavian and Jugular Lines
1. Purpose: A sterile dressing is applied to central venous catheters to provide a barrier, and thereby reduce the risk of infection to the
insertion or exit site and surrounding areas.
2. Guidelines
a. Dressings are to be changed using sterile technique
b. Transparent film dressings are changed at least one (1) time per week, and more frequently if not adhering to the skin, or
if soiled.
c. Gauze and tape dressings are changed at least every 24 hours to assess the site.
d. Acetone alcohol can dissolve some types of central venous catheters and must never be used on or near the catheter.
e. Nurses who have been trained in sterile central line dressings
change technique and demonstrate competency may change central venous catheter dressings.
f. A smooth (non-teethed) Dravon clamp should be at the
bedside of every resident with a central venous catheter, except when using a Groshong catheter.
g. Scissors should never be used near the central venous
catheter or on the dressing.
3. Equipment
a. Sterile central venous catheter dressing change kit includes:
sterile gloves, (3) povidone swabsticks, (3) isopropyl alcohol swabsticks, split gauze pad, 2x2 and 4x4 gauze pads,
povidone ointment, 4x5 transparent film dressing, label, tape (contents are similar, but vary by manufacturer).
- 18 -
PROCEDURES b. Clean Towel
c. Clean gloves
d. Infectious waste bag
4. Procedure/*Key Points
a. Wash hands thoroughly.
b. Assemble supplies.
c. Explain procedure to resident.
*Alleviates fears and encourages resident’s cooperation.
d. Place resident in a flat position with head turned away from site.
e. Place Chux or towel under central line site.
f. Put on clean gloves.
*Universal precaution
g. Carefully remove soiled dressing by loosening all edges first and stabilizing catheter with one hand.
h. Remove and discard gloves
i. Evaluate catheter exit site; observe for the following:
Skin breakdown
Bleeding or drainage at exit site Erythema
Puffiness or swelling
Heat Induration
Leaking connections Catheter integrity (kinks, ruptures, etc.)
Any change in catheter position Broken or loose sutures
- 19 -
PROCEDURES *Observation of any abnormality must be reported to the
physician as soon as possible.
j. Open sterile dressing change kit.
k. Put on sterile gloves.
*If patient has a subclavian type central line, hold line in
place with one gloved hand at all times.
l. With gloved hand, use alcohol swabsticks; cleanse skin around catheter site and surrounding area three (3) times
and let dry one (1) minute.
*Always cleanse from the center outward in a circular motion. Substitute Hibiclens or hydrogen peroxide if allergic to iodine.
m. Cleanse sutures and under the catheter hub if necessary.
n. Repeat procedure with three (3) povidone swabs and let dry
one (1) minute.
o. Apply sterile dressing.
*If transparent dressing is used and fresh sutures are
present, protect the sutures with gauze, then cover with a transparent dressing and change every 48 hours.
p. Reinforce and seal catheter exit from dressing with tape.
q. Label dressing with:
i. Time and ate of dressing change.
ii. Initials of nurse
r. Discard used supplies

- 20 -
PROCEDURES 5. Documentation
a. Document dressing change in resident’s medical record.
include:
i. Date and Time
ii. Appearance of site iii. Presence of suture if applicable
iv. Type of dressing v. Nurse’s signature
- 21 -
PROCEDURES H. Central Venous Catheters*: Cap Change
*Hickman Type, Global Groshong®, Broviac and Subclavian Lines
1. Purpose: A sterile luer lock injection port with a 3” – 6” extension set is used to maintain a closed system and reduce the risk of
infection and air embolism.
2. Guidelines
a. The 3” – 6” extension set(s) and/or injection port(s) will be
changed one (1) time a week with the sterile dressing change procedure and PRN contamination or leakage.
b. Multi-lumen catheters will require cap changes for each lumen
with the same frequency as a single lumen catheter, even if not all lumens are being used.
c. A smooth Dravon clamp should be at the bedside of every
resident with a central venous catheter, except when using a Groshong catheter.
3. Equipment
a. Sterile luer lock injection port or,
b. Sterile 3” – 6” luer lock extension tube with injection cap
c. Gloves
d. Three (3) alcohol preps or swabsticks
e. 3cc normal saline in 10cc syringe with 22 gauge, 1 inch needle or smaller
4. Procedure/*Key Points
a. Prime injection cap or extension set with normal saline
b. Loosen old extension set or cap, but do not remove
*Avoid pulling or any “in and out” manipulation of the catheter *Clamp catheter

- 22 -
PROCEDURES
c. Cleanse catheter junction with three (3) alcohol preps or swabs,
using firm rubbing action.
*Alcohol is preferred to betadine, since betadine tends to stick when dry
d. Put on gloves
*Universal precaution
e. For subclavian lines: Instruct resident to inhale, HOLD BREATH and bear down. This is known as the Valsalva maneuver.
For Hickman type catheter: Apply a clamp to distal portion of
catheter.
*Coordinate change with exhalation if resident is unable to follow instructions. There is always a possibility of negative
pressure with central lines when open to air and this could cause an air embolism.
f. Quickly and aseptically remove old extension set or cap and connect a new sterile extension set or cap to catheter.
*Be careful not to touch or contaminate catheter hub or end of
new cap or extension set.
g. Instruct resident to breath normally or unclamp catheter.
h. Clean injection plug with alcohol
i. Gently flush catheter with 1-5cc normal saline, based on physician’s order, to assess catheter patency.
*Forceful irrigation may rupture the catheter. If resistance is
met, catheter may be partially occluded or kinked.
j. Maintain positive pressure on plunger of syringe while
withdrawing from injection cap.
*Prevents backflow of blood into catheter.
- 23 -
PROCEDURES
k. Reconnect to IV administration set and resume infusion or flush
with appropriate dose of heparin lock flush.
5. Documentation
a. Document cap or extension tube change in resident’s medical
record. Include:
i. Date and time ii. Device attached (cap or extension tube)
iii. Condition of catheter (i.e., patent, no leaks or cracks) iv. Flush solution and volume
v. Nurse’s signature

- 24 -
PROCEDURES I. Central Venous Catheters: Heparinization
1. Purpose: To maintain patency of central vascular access device.
2. Guidelines
a. Heparin lock flush will be ordered by a physician in a prescribed dose that does not alter the resident’s clotting
factors.
b. Standard heparin flush amounts and concentrations:
i. Heparin Flush concentration is 10 units/cc ii. Each catheter has a unique, internal volume
iii. The physician’s order should specify the volume for the flush based on the internal volume of the catheter –
usually 1-5 cc.
c. Standard normal saline 0.9% flush amount:
i. The physician’s order should specify the volume for the
flush based on the internal volume of the catheter – usually 5-10cc
ii. Central venous catheters are flushed at least every 24 hours before and after each intermittent infusion
d. Implanted ports (Mediport/Port-A-Cath) are flushed as
follows:
i. The physician’s order should specify the volume for the flush based on the internal volume of the catheter –
usually 5-10 cc. ii. Accessed ports, but not in use for infusion – Flush once
per week with Normal saline 0.9% 10cc and Heparin flush solution 10 untis/cc 5cc. Use a pulsatile flushing
technique to aid in reducing sludging in these ports.
iii. Accessed ports in active use for infusion – Flush with Normal saline 0.9% before and after medications, then
flush with Heparin Flush Solution 10 units/cc 5cc.
- 25 -
PROCEDURES e. Groshong Catheters are flushed as follows:
i. In active use for infusion – Normal saline 0.9% 5cc
before and after each use. ii. Not in active use for infusion – Normal saline 0.9% flush
once weekly
f. Use the needleless cannulas to access ports for flushing
central catheters.
g. Each line of multi-lumen catheter will be treated as a single lumen catheter for purpose of heparinization, saline flushing
and care.
h. Always maintain positive pressure by simultaneous injection of flush while withdrawing needleless cannula from injection
port.
i. If steel needles are used the maximum gauge and length are 22” x 1” for injection ports.
3. Equipment
a. Povidone-iodine or alcohol swabs
b. Prescribed volume and concentration of heparin flush in a syringe
c. Prescribed volume of normal saline flush in a syringe
d. Injection port or extension tube for central line, if not already
in place
4. Procedure/*Key Points
a. Wash hands
b. Explain procedure to resident
*Decrease resident anxiety
c. Scrub injection port with alcohol swab
- 26 -
PROCEDURES
d. Insert Normal Saline syringe adapter into center of injection
port.
*Check to be sure that catheter is unclamped.
e. Inject normal saline
*To clear catheter of solution, blood, and check patency.
f. Insert Heparin flush syringe adapter into the center of the
injection port.
*Maintain positive pressure
g. Inject prescribed amount of heparin.
5. Documentation
Document heparin flush on IV Medication Sheet. Include:
a. Date and time
b. Volume and strength of heparin and saline flush c. Nurse’s signature

- 27 -
PROCEDURES I. Central Venous Catheters: Intermittent Medication Administration
1. Purpose: To safely administer intermittent drug therapy via a
central vascular access device
2. Guidelines
h. The guidelines for Normal saline and Heparin flush apply
i. Injection ports and lumens of catheters will be flushed
following all intermittent infusions and at least once every 24 hours
j. IV administration tubing sets used for intermittent
administration will be changed every 24 hours
k. IV administration tubing sets will be used for only one medication. Each medication requires dedicated
administration tubing prior to each infusion.
l. A new sterile needle or needleless cannula will be placed on
the end of the intermittent IV administration tubing prior to each infusion.
m. Injection ports will be prepped with an alcohol or povidone
swab prior to each access
n. IV administration tubing sets will be labeled with date, time and nurse’s initials.
3. Equipment
a. Medication and/or solution
b. Needleless cannula, click lock needle and housing or 22g 1
inch needle
c. Two (2) normal saline 10cc syringes for flushing before and
after medication
d. Alcohol swabs

- 28 -
PROCEDURES
e. Heparin lock flush syringe
4. Procedure/*Key Points
a. Compare medication label to physician’s order
b. Wash hands
c. Spike the intermittent infusion bag or solution and prime solution through tubing set
d. Prep the injection port with alcohol or povidone swab
e. Perform first Normal saline flush
*Ensures catheter patency
f. Connect medication/solution to IV tubing or injection port
with the needleless cannula, click lock needle and housing or 22g 1 inch steel needle.
g. Label tubing with date, time and nurse’s signature
h. Initiate infusion at prescribed rate
i. Disconnect the tubing from the injection port
Tape the used tubing set connector to the IV pole until the next use. A new sterile connector, regardless of type
is placed on the tubing prior to the next use
j. Perform the second Normal saline flush
k. Perform the heparin flush using positive pressure flush techniques while withdrawing connector from injection ports
l. Tape the used tubing set connector to the IV pole until next use.
5. Documentation

- 29 -
PROCEDURES
a. Document administration of medication, dose, time of
infusion, volume, flush, and resident’s response on IV Medication Sheet.
J. Central Venous Catheters: Removal
1. Purpose: To provide procedures for the removal of Central Venous Catheters. To identify the Central Venous Catheters that may be
removed in the facility.
2. Guidelines
d. Registered Nurses who have the knowledge, education and validated skills to do so may perform this procedure
e. The Central Venous Catheters that may safely be removed in
the facility are:
i. Non-tunneled, non-surgically placed catheters, i.e., Triple, double or single lumen subclavian or jugular vein catheters
ii. Peripherally Inserted Central Catheters (PICCs)
f. The Central Venous Access Devices that may not safely be
removed in the facility are:
i. Tunneled, surgically placed catheters (Groshongs, Hickmans, Broviacs, etc.)
ii. Implanted venous access devices, i.e., Port-a-caths, Mediports, CathLINK 20, Oamya Reservoirs, etc.
iii. A specific physician’s order is required to perform this procedure
iv. A physician’s order is required to culture the tip of the catheter
v. This procedure is performed using sterile technique
3. Equipment
a. Central Line Dressing change tray
b. Suture removal kit (if sutures were present) c. Additional sterile 4x4 gauze sponges
d. Clean, latex examination gloves e. Sterile gloves, mask, goggles (gown is optional)

- 30 -
PROCEDURES f. Sterile specimen cup (for catheter tip culture)
4. Procedure/*Key Points
a. Assess the site and the catheter for any signs of complications
*If the site is draining culture exudates and the catheter tip
b. Prepare a sterile field using the Central Line Dressing Change Tray and Suture Removal Kit.
c. Don examination gloves and remove the soiled dressing
d. Don sterile gloves and prepare the site using the guidelines
under Central Lines Dressing Change. This is a sterile procedure.
e. Don a new pair of sterile gloves.
f. Clip any anchoring sutures
*Instruct the resident that a pull or slight twinge may occur
g. Prepare a bolus of 4x4 gauze sponges to use as pressure pad
h. Using a single 4x4 gauze sponge gold firmly onto the catheter near the exit site
i. Instruct the patient to hold their breath for a few seconds
j. Using a firm, slow, steady pressure remove the catheter from
the site and instruct the patient to resume normal respiration.
k. Immediately place the bolus of gauze sponges over the exit site and apply direct, firm pressure for five (5) minutes.
l. Do not contaminate the catheter tip. Using the sterile scissors from the Suture Removal Tray, clip the top of the
catheter off into the sterile specimen cup and send to the lab for C&S.
- 31 -
PROCEDURES m. Gently remove the gauze bolus and assess the exit site for
active bleeding
*If active bleeding is assessed, reapply the pressure for an additional five (5) minutes
n. Prepare a small bolus of sterile 4x4 gauze sponges. Apply over the exit site.
o. Apply the transparent film dressing. Label with date, time
and initials.
*It is not unusual for the exit site to have moderate serosanguinous drainage for up to 24 hours after removal.
p. Document procedure and resident’s tolerance
q. Remove transparent film dressing twenty-four (24) hours
later and reassess site
r. If free of complications, apply a band-aid
s. Document exit site in clinical record
5. Documentation
a. Document site and catheter at dressing removal
b. Document patient instruction and tolerance to procedure c. Document disposition of catheter tip
d. Document follow-up to site in twenty-four (24) hours.
- 32 -
PROCEDURES K. Peripherally Inserted Central Catheters (PICC) and Extended
Peripheral Catheters: Care and Maintenance (i.e., Landmark, L-Cath, Per-Q Cath)
1. Purpose: To safely care for, maintain and monitor PICC lines and
extended peripheral catheters.
2. Guidelines
a. Definition: A PICC line and extended peripheral catheter is an
IV catheter which is inserted peripherally through an antecubital vein using sterile technique. The tip of the
catheter is threaded to the desired location, either peripherally (axillary vein or below) or centrally (subclavian vein or
superior vena cava). Many of these catheters are made of silastic material, making them soft and flexible; other
biocompatible materials are also used. These catheters provide reliable vascular access for long or short term
therapies.
b. PICC lines are inserted by RNs or MDs with advanced IV skills.
c. An over-penetrated x-ray film is required to confirm catheter
tip placement in the superior vena cava before using the catheter. Obtain a written x-ray report and file on the clinical
record.
d. Only a registered nurse, based upon facility specific job description or individual State Board of Nurse Examiner’s rules
and regulations, should perform this procedure.
e. The extended peripheral catheter is considered a peripheral IV. Dressings may be changed by qualified nurses, in accordance
with specific job description.
f. PICC lines and extended peripheral catheters may be removed
by RNs in the long-term care facility if trained in this procedure.

- 33 -
PROCEDURES g. The catheter insertion site should be monitored along with the
upper arm for redness, swelling or tenderness. It may be necessary to record circumference measurements for accurate
assessment.
h. Catheter insertion records should include:
i. Type of catheter placed
ii. Size and gauge of catheter iii. Insertion site by specific vein
iv. Length of catheter threaded into the vein v. Length of catheter remaining out of the insertion site
vi. Intended catheter tip location
i. A 4.0 French or 20 gauge PICC line or larger may be used for blood sampling. A physician’s order must be obtained to draw
blood.
j. Do not use extended peripheral catheters for blood sampling.
k. It is recommended that an infusion pump be used to deliver all
therapies through these catheters.
l. Catheters should not be clamped, as this may damage or sever the catheter.
m. Catheters should have a luer lock injection plug extension tube
attached to catheter hub to reduce catheter stress and maintain a closed system.
3. Procedure/*Key Points
a. Heparinization and Flushing
i. Catheters and injection ports should be flushed as follows:
Before and after each use, or at least Once every 24 hours
Normal Saline 0.9% 5-10cc before and after each medication
Heparin Flush solution 10 units/cc 1-3cc when line is not in use
- 34 -
PROCEDURES
b. Dressing change and injection port/extension Tubing change
c. Catheters should be covered with a transparent film dressing.
d. The transparent dressing, injection port and extension tubing are changed every 7 days and PRN soiling or non-adherence.
e. Extreme care is required during dressing change procedures so as not to pull out the catheter and to maintain sterility.
f. Follow sterile central line dressing change procedure in this
manual.
4. Documentation
a. Document procedures as recommended in this manual for each procedure performed.
- 35 -
PROCEDURES
L. IV Solutions: Bag or Container Change
1. Purpose: To change solution and/or medication container, while
maintaining aseptic technique.
2. Guidelines
a. IV solutions, spiked in the facility, may not hang longer than
24 hours.
b. IV solutions, cassettes and cartridges prepared under a sterile hood in the pharmacy may be used until empty, provided the
system has not been opened.
c. Strict aseptic technique during this procedure is necessary to prevent contamination of the entire IV system.
d. Light sensitive solutions should be protected with a light proof
cover during infusion and stored in a closed wrapper or box.
e. Solutions for IV administration should be clear and free of
particles.
f. Emulsified solutions for IV administration should be uniform in color and consistency.
g. Solutions suspected for contamination should be returned to
the dispensing pharmacy.
3. Equipment
a. IV solution
b. Label
4. Procedure/*Key Points
a. Prepare new container in advance
1. Compare label with physician’s orders.
2. Inspect container integrity.

- 36 -
PROCEDURES 3. Refrigerated solutions should be brought to room
temperature by removing them from the refrigerator as follows:
Volume Time
Less than 1,000 cc 30 minutes prior to infusion 1,000 cc 1 hour prior to infusion
2,000 cc 2 hours prior to infusion Over 2,000 cc 3 hours prior to infusion
*To prevent resident discomfort.
b. When present container is empty or has been in use for 24
hours:
1. Wash hands. 2. close roller clamp on IV tubing.
3. Remove tubing spike from old container and push spike into new container.
*Remove protective cover from container’s spike port.
*Keep tubing spike sterile
c. Invert and hang new container.
d. Prime tubing and filters to remove air.
e. Open roller clamp and re-establish prescribed flow rate.
f. Label new container with date, time hung and nurse’s initials.
5. Documentation
a. Record change on IV Medication Sheet.
b. Verify that new IV container is labeled with resident’s name,
IV solution and rate.

- 37 -
PROCEDURES M. IV Tubing: Change
1. Purpose: To change IV administration set (IV tubing) on a routine
basis and prevent contamination of the IV system.
2. Guidelines
a. Intravenous administration sets used for continuous IV
infusions will be changed at least every 48 hours and PRN
b. IV tubing used for intermittent (heparin lock) therapy or IV piggy back shall be changed every 24 hours.
c. IV tubing change should be done in conjunction with the first
container change of the day to avoid unnecessary manipulation of the system.
d. All IV tubing should be labeled with time and date of the
tubing change and initials of nurse performing the procedure.
e. Filters, if present, are changed with administration sets.
3. Equipment
a. IV administration set
b. Solution container
c. IV tubing label
d. Connector for IV tubing to injection port (lever lock, cannula
adapter, click lock needle and housing or 22g needle)
e. Alcohol prep
f. Tape
4. Procedure/*Key Points
a. Wash hands thoroughly.
* Infection control

- 38 -
PROCEDURES b. Close roller clamp on new tubing and attach needle to tubing
end.
c. Remove protective covers from IV solution
d. Insert tubing spike into solution container.
*Take care not to touch tubing spike to prevent
contamination.
e. Invert container and hang on IV pole.
f. Squeeze drip chamber to fill halfway.
*Some IV tubing sets do not have drip chambers.
g. Slowly prime fluid through entire length of IV tubing.
*Check to be sure all air is out of tubing before connection to resident.
h. Close flow clamps on both old and new tubing
i. Disconnect old tubing from injection plug extension set.
j. Clean extension set injection plug with alcohol using firm pressure for 30 seconds.
k. Connect new tubing to injection plug and secure with tape or
line locking device.
l. Establish flow rate according to physician orders.
m. Label new tubing and IV solution container with:
1. Date
2. Time 3. Nurse’s initials
5. Documentation
a. Record procedure on resident’s medical record.

- 39 -
PROCEDURES N. IV Tubing: Intermittent Therapy Via Secondary Line (IV Piggy
back, IVPB)
1. Purpose: To administer intermittent fluid or medication while infusing a primary IV solution.
2. Guidelines
a. IV Piggy back tubing shall be changed every 24 hours
b. Tubing will be labeled with date, time and nurse’s initials.
c. All tubing connections will be secured with tape or a line securing device.
3. Equipment
a. IV fluid/medication
b. Secondary administration set with connector and wire hanger
c. Alcohol prep
d. Tape
4. Procedure/*Key Points
a. Wash hands.
*Infection control
b. Close clamp on secondary tubing.
c. Attach injection port connector to tubing set if not present.
d. Remove protective covers from IVPB solution and tubing
spike.
e. Insert tubing spike into solution container.
f. Hang IVPB bag on IV pole and lower primary container on wire hanger.

- 40 -
PROCEDURES g. Squeeze drip chamber to fill halfway.
h. Open clamp and prime IV line completely.
i. Close clamp.
j. Cleanse upper Y-site infection plug on primary set with alcohol prep.
*If primary IV has a back check valve, select injection plug
below the valve.
k. Insert secondary tubing set connector.
*Tape or secure with a line connection device to avoid accidental disconnection.
l. Open clamp on secondary set to control flow rate. Back-
check valve on primary set will prevent flow from secondary container into primary container.
m. Label IVPB bag with date, time and nurse’s initials.
n. If using infusion pump, set secondary rate and begin infusion.
*Most electronic infusion pumps will automatically return to the primary flow rate when IVPB is complete
*Leave empty IVPB bag attached, keeping system closed,
until next dose is needed.
*Check compatibility of primary and secondary infusions
Subsequent
o. Close clamp on primary set.
p. Lower empty IVPB (with attached secondary set) below drip
chamber on primary set. Allow primary solution to fill secondary set until secondary drip chamber is half full.
q. Close clamp on secondary set.

- 41 -
PROCEDURES r. Remove empty container and spike new secondary IVPB
container.
s. Hang new IVPB container on IV pole and lower primary container on wire hanger.
t. Label IVPB bag with date, time and nurse’s initials.
u. Open clamp on secondary set. Adjust flow rate with clamp on primary set or with pump.
5. Documentation
a. Record medication on resident’s medical record.
b. Record resident’s response to medication.
c. Record IVPB volume infused on I&Os.

- 42 -
PROCEDURES O. IV Flow Rates: Calculating
1. Purpose: To accurately deliver the ordered rate of IV fluid via
gravity drip administration.
2. Guidelines
a. Identify manufacturer’s drip rate of tubing being used.
Macrodrip comes in 10 drops/cc, 15 drops/cc and 20 drops/cc. Microdrip is 60 drops/cc.
b. Identify hourly flow rate ml/hr ordered by physician or calculate
hourly rate using formula:
Total volume of solution (cc’s) ---------------------------------- = ml/hr
Total hours of administration
c. Calculate drop per minute from hourly rate:
Tubing drip rate
ml/hr x --------------------- = drops/min 60
d. Universal IV formulas:
1. For time in hours:
Total volume (ml) tubing drip rate
-------------------- X ------------------- = drops/min Total time (hours) 60
i. Example: Give 2 liters of D5W IV every 24 hours
(tubing drip rate is 10 drops/ml.)
2000 ml 10
--------- X ---- drops/cc = 13.8 or 14 qtt/min 24 hrs 60

- 43 -
PROCEDURES 2. For time in minutes:
Total volume (ml)
----------------------- X tubing drip rate = qtt/min Total time (minutes)
i. Example: Give 50cc D5W IV over 30 min (tubing drip rate is 60 qtt/ml).
50 ml
-------- X 60 qtt/ml = 100 qtt/min 30 min
e. After calculating the flow rate, hold your watch next to the drip
chamber and observe your watch and count the drops for one full minute and adjust the roller clamp until the desired rate is
achieved.
f. When regulating IV flow rates by a roller clamp, monitor the IV frequently for proper infusion rate.
g. Several factors can affect the flow rate of a gravity drip IV. These may include:
1. Height of the IV solution container
2. Size of IV catheter 3. Position of IV catheter
4. Position of resident 5. Condition of vein
6. Clot or kink in catheter or tubing
h. A time tape is recommended to aid in monitoring IV gravity drip flow rates.
1. Calculate hourly rate of ordered IV.
2. Place tape on IV solution container and mark off (one) 1
hour volume increments. 3. Write starting time at top of tape.
4. Label each mark on tape with time.
*Do not write directly onto IV bag with marker, as it may absorb ink into the solution.

- 44 -
PROCEDURES Example:
_____________________ 12/1 2pm-
3pm- 4pm-
5pm-
6pm- 7pm-
8pm- _____________________
j. If IV gravity drip infusion rate is off (too slow or too fast),
regulate IV to ordered flow rate, record actual amount of fluid given on I&O. Do not try to “catch up” a slow IV.

- 1 -
CONTINUOUS QUALITY IMPROVEMENTS/ QUALITY ASSESSMENT INDICATOR (CQI/QAI) PROGRAM
A. Purpose
To identify the opportunities for performance improvement related to
intravenous therapy through continuous performance measurement and evaluation of the care and services provided by facility nursing
personnel.
B. Methods
1. Direct monitoring by peer review
2. Monthly audits as Performance indicates.
3. Quarterly/Annual Review of performance standards by CQI/QAI
Council.
C. Implementation
1. Periodic review of performance by CQI/QAI Council.
2. Monthly data collection and reporting.
3. Quarterly trending/analysis of data collected.
4. Annual updates and periodic remedial education as indicated.
D. Areas of Responsibility
1. Director of Nurses (DON)
a. Review QA audit results with auditor.
b. Implement CQI/QAI Council recommendations.
c. Report findings/trend to Council.
d. Maintain a list of all IV qualified licensed nursing staff.
- 2 -
CONTINUOUS QUALITY IMPROVEMENTS/ QUALITY ASSESSMENT INDICATOR (CQI/QAI) PROGRAM
2. Consultant Pharmacist
a. Review for dosage, drug appropriateness and/or side effects.
b. Review for clinical indicators reflecting effectiveness of
medications.
c. Evaluate IV labeling, storage, delivery.
d. Monitor laboratory values for therapeutic clinical management of IV therapy.
3. CQI/QAI Council
a. Review results of monthly audits as appropriate
b. Review results of quarterly performance audits.
c. Recommend implementation parameters to address opportunities to improve performance.
d. Perform annual review.
E. Audit Process
1. The person assigned responsibility for data collection will complete
the IV audit tools monthly report.
2. The audit tools will be summarized on the Monthly Monitoring Tool.
3. The Monthly Monitoring Tool will be used as the basis for monthly
reporting to the CQI/QAI Council.
4. The Council will review the results and make recommendations to the Director of Nurses and pharmacy to resolve opportunities for
performance improvement.
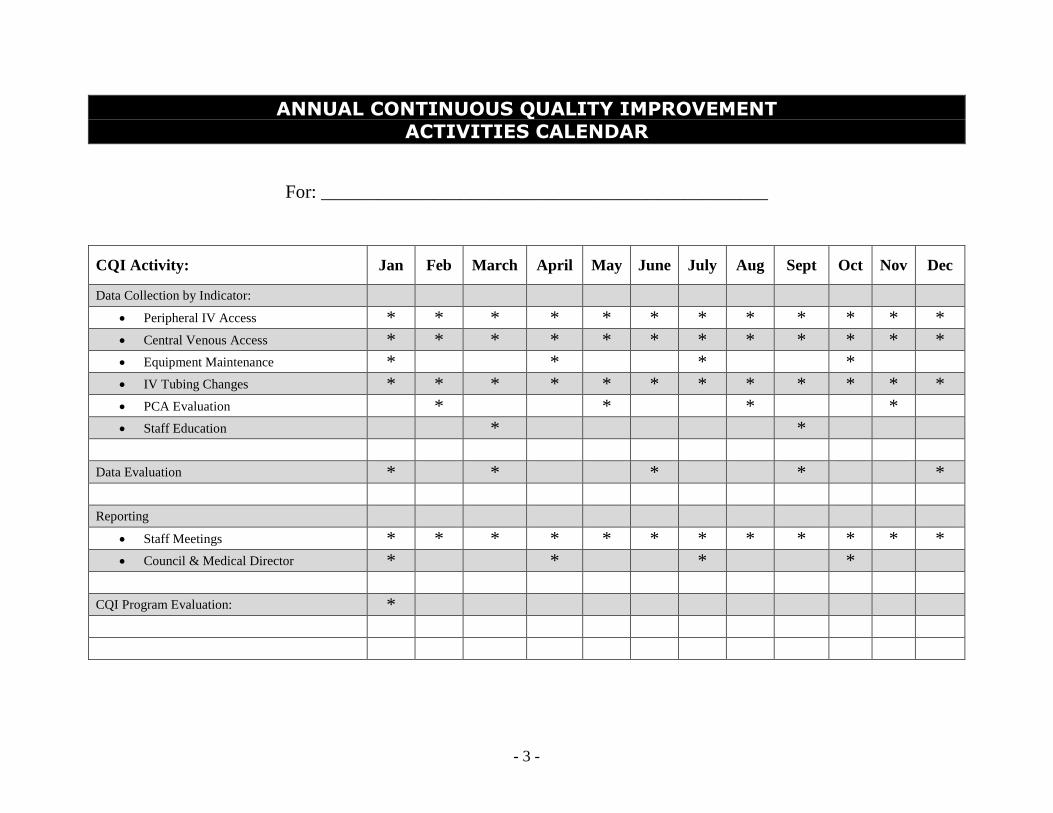
- 3 -
ANNUAL CONTINUOUS QUALITY IMPROVEMENT ACTIVITIES CALENDAR
For: ________________________________________________
CQI Activity: Jan Feb March April May June July Aug Sept Oct Nov Dec
Data Collection by Indicator: Peripheral IV Access * * * * * * * * * * * * Central Venous Access * * * * * * * * * * * * Equipment Maintenance * * * * IV Tubing Changes * * * * * * * * * * * * PCA Evaluation * * * * Staff Education * *
Data Evaluation * * * * * Reporting
Staff Meetings * * * * * * * * * * * * Council & Medical Director * * * *
CQI Program Evaluation: *

- 4 -
CQI/QAI COUNCIL QUARTERLY REPORT
Reported by ________________________________
Date of report ________________________________
For quarter ended ________________________________
I. Aspects of care/services reviewed this quarter:
__________________________________ ___________________________________
__________________________________ ___________________________________
__________________________________ ___________________________________
II. Describe opportunities to improve performance in care/services:
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
III. Summary of actions implemented to address opportunities to improve performance:
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
IV. Progress toward unresolved opportunities to improve performance from previous report:
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
___________________________________________ ________________________
Signature Date

- 5 -
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: CENTRAL VENOUS ACCESS DEVICE
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-)
N/A Central Venous Access Device Dressings:
Changed per MD order or 2 times weekly Dressing labeled with date, time and initials Injection ports changed per MD order or 2 times weekly Dressing are dry and occlusive Dravon clamp at bedside (except Groshong/PICC)
Documentation includes observations of the following: Type of central venous access device in use Location of exit site Appearance of exit site Type of dressing and appearance Signs and symptoms of complications and nursing actions
Central Venous Access Device Flushing Protocols (Heparin): MD order includes strength, volume and frequency Volume of flush appropriate for device in place Implanted ports accessed and flushed monthly Groshong catheters flushed weekly, when not in use
Emergency IV Box: If opened, sealed with red seal and pharmacy notified □ Yes □ No If sealed, expiration date of oldest item listed □ Yes □ No Contents list attached to outside □ Yes □ No Physician’s Authorization, if required, is present □ Yes □ No
Problems identified:_____________________________________________
__________________________________________________________________________________________________________________________
Recommendations/solutions:___________________________________________________________________________________________________
_____________________________________________________________

- 6 -
Signature of auditor _____________________________ Date___________
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Intravenous Tubing (includes filters/extension tubing):
Each IV tubing labeled with date, time and initials IV tubing used for continuous infusion changed
every 48 hours
IV tubing used for intermittent therapy changed every
24 hours
Injection port adapter for intermittent therapy changed
prior to each use
Vented tubing used with glass containers
Intravenous Solutions: All IV solutions are changed every 24 hours IV solution containers are labeled with date, time hung,
and initials
Pharmacy label attached to all solutions with complete
order
IV solution matched physician’s orders IV rate is consistent with physician’s orders IV basic solution is within expiration date or label
expiration date
Medication Label Additive stickers present and
complete for meds added in facility
(continued)

- 7 -
CQI/QAI DATA COLLECTION TOOL
ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Documentation
Tubing changes consistently documented in clinical
record
Administration of solutions documented in clinical
record
Medication administration documented in clinical
record
Intake and output documented in appropriate clinical
record
Weights recorded in clinical record Current lab results present in clinical record with
proper physician notification
Physician orders, medication administration record and
label agree
Physician orders include name of drug, strength, dose,
route of administration, frequency and duration and,
if PRN, a reason
Storage of Solutions Solutions with “refrigerate” warning labels are in the
refrigerator
Solutions are removed from the refrigerator and
brought to room temperature prior to administration
Sterile pathway protectors and present on all stored
containers
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________

- 8 -
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: IV PUMPS - ELECTRONIC
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Electronic Pumps
Operating Manual available for each pump Pumps plugged into a grounded outlet Back-up batteries available (ambulatory pumps) Pump alarms are audible at nurses station Soiled pumps stored in soiled utility room
(must be returned to Pharmacy for cleaning)
Pumps securely mounted on wide base poles Ambulatory pumps have “fanny packs” for carriers
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
_____________________________________________________________
_____________________________________________________________
Signature of auditor _____________________________ Date___________

- 9 -
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: PERIPHERAL INTRAVENOUS DEVICE
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Insertion of Peripheral Intravenous Device
Peripheral access initiated by qualified nurse Peripheral sites rotated every 72 hours If longer than 72 hours, a physician order approves
the extension
Physician order present for low extremity access Extension sets and injection ports present on all
peripheral catheters
Peripheral dressing labeled with date, time,
initials and gauze/length
Peripheral Intravenous Device Documentation Insertion documentation includes:
o Catheter type, length and gauge o Location of site o Number of attempts o Type of dressing applied, date, time o Resident’s toleration of procedure
Daily documentation includes: o Insertion site location and appearance o Condition of dressing o S/S of complications and nursing interventions
Removal of Peripheral Intravenous Access Device: o Saline flushes recorded o Heparin flushes, strength and account o Physician order gives strength, volume and
frequency
Tubing changes documented in clinical record
Problems identified:_____________________________________________
__________________________________________________________________________________________________________________________
Recommendations/solutions:___________________________________________________________________________________________________
_____________________________________________________________
Signature of auditor _____________________________ Date___________

- 10 -
CQI/QAI MONITORING TOOL ASPECT OF CARE: CENTRAL VENOUS ACCESS DEVICE
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
Central Venous Access Device dressings: Number Percentage
Change per MD order or 2 times weekly of
Dressing labeled with date, time and initials of
Injection ports changed per MD order or
2 times weekly of
Dressings are dry and occlusive of
Dravon clamp at bedside (except Groshong/PICC) of
Documentation includes observation of the following:
Type of central venous access device in use of
Location of exit site of
Appearance of exit site of
Type of dressing and appearance of
Signs and symptoms of complications and nursing actions of
Comprehensive plan of care includes Intravenous Therapy of
Central Venous Access Device Flushing Protocols
(Heparin): of
MD order includes strength, volume and frequency of
Volume of flush appropriate for device in place of
Implanted ports accessed and flushed monthly of
Groshong catheters flushed weekly, when not in use of
Emergency IV Box:
If opened, sealed with red weal and pharmacy notified □ Yes □ No
If sealed, expiration date of oldest item listed □ Yes □ No
Contents list attached to outside □ Yes □ No
Physician’s Authorization, if required, is present □ Yes □ No
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________
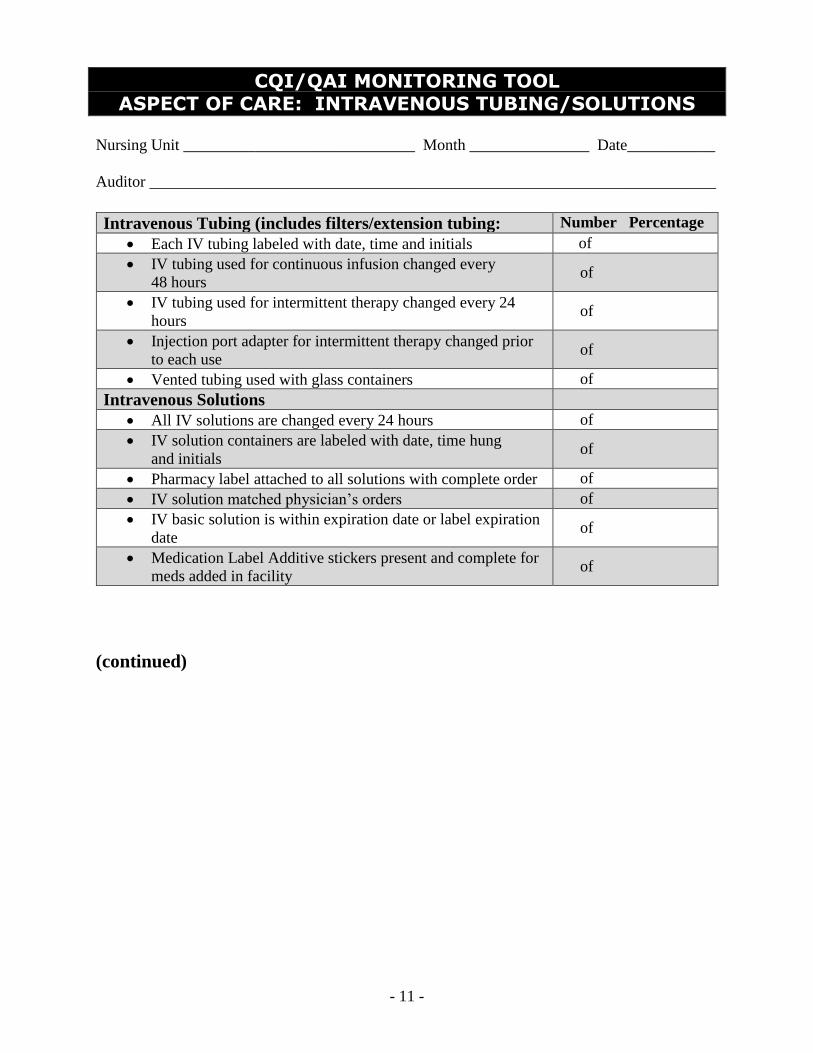
- 11 -
CQI/QAI MONITORING TOOL ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
Intravenous Tubing (includes filters/extension tubing: Number Percentage
Each IV tubing labeled with date, time and initials of
IV tubing used for continuous infusion changed every
48 hours of
IV tubing used for intermittent therapy changed every 24
hours of
Injection port adapter for intermittent therapy changed prior
to each use of
Vented tubing used with glass containers of
Intravenous Solutions
All IV solutions are changed every 24 hours of
IV solution containers are labeled with date, time hung
and initials of
Pharmacy label attached to all solutions with complete order of
IV solution matched physician’s orders of
IV basic solution is within expiration date or label expiration
date of
Medication Label Additive stickers present and complete for
meds added in facility of
(continued)
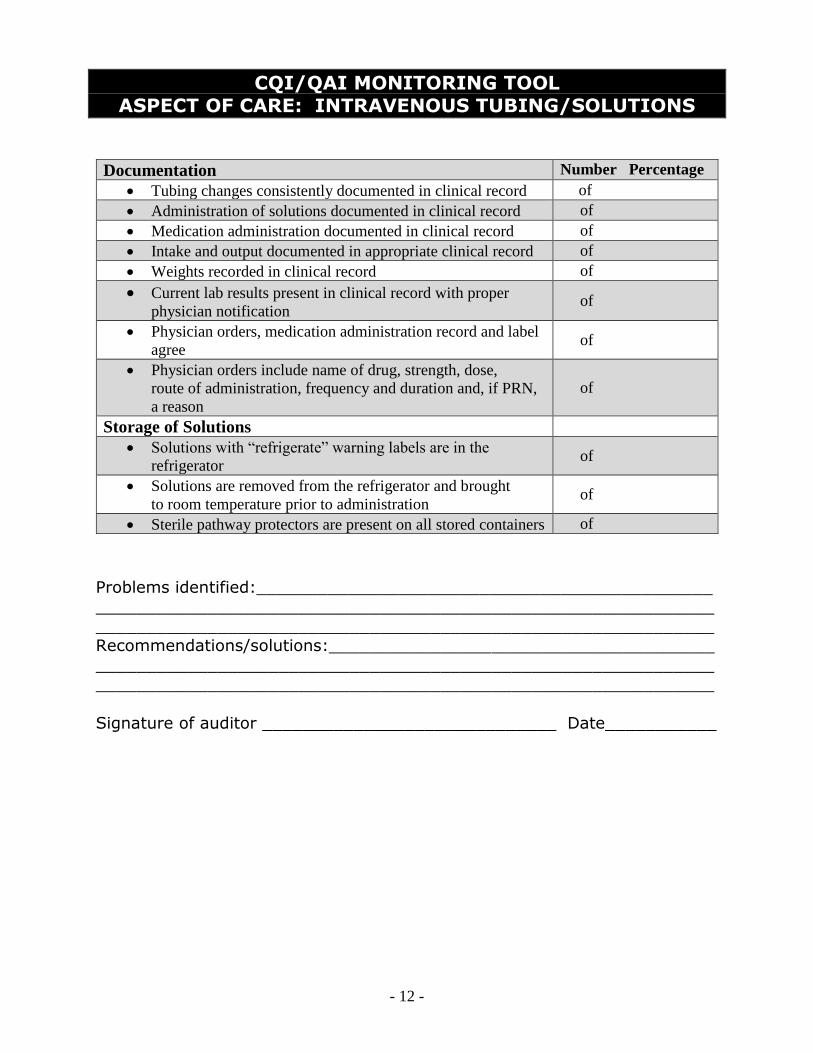
- 12 -
CQI/QAI MONITORING TOOL ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
Documentation Number Percentage
Tubing changes consistently documented in clinical record of
Administration of solutions documented in clinical record of
Medication administration documented in clinical record of
Intake and output documented in appropriate clinical record of
Weights recorded in clinical record of
Current lab results present in clinical record with proper physician notification
of
Physician orders, medication administration record and label
agree of
Physician orders include name of drug, strength, dose,
route of administration, frequency and duration and, if PRN,
a reason
of
Storage of Solutions
Solutions with “refrigerate” warning labels are in the
refrigerator of
Solutions are removed from the refrigerator and brought
to room temperature prior to administration of
Sterile pathway protectors are present on all stored containers of
Problems identified:_____________________________________________
__________________________________________________________________________________________________________________________
Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________
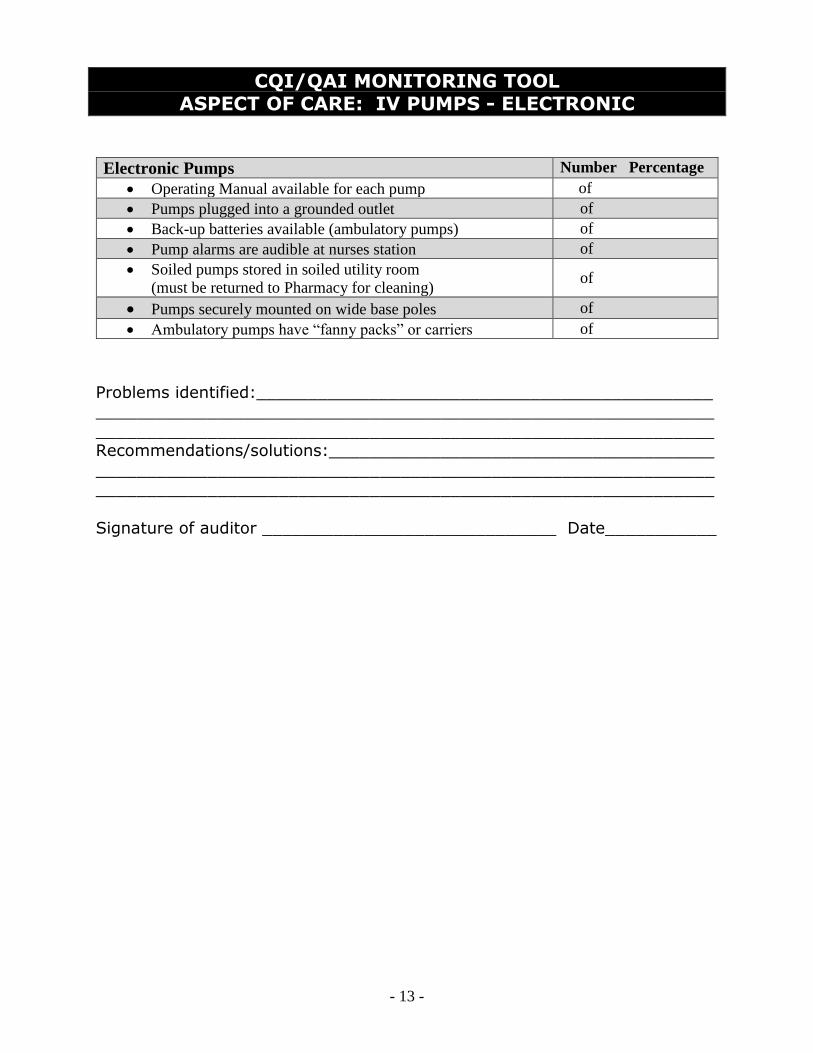
- 13 -
CQI/QAI MONITORING TOOL ASPECT OF CARE: IV PUMPS - ELECTRONIC
Electronic Pumps Number Percentage
Operating Manual available for each pump of
Pumps plugged into a grounded outlet of
Back-up batteries available (ambulatory pumps) of
Pump alarms are audible at nurses station of
Soiled pumps stored in soiled utility room
(must be returned to Pharmacy for cleaning) of
Pumps securely mounted on wide base poles of
Ambulatory pumps have “fanny packs” or carriers of
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________
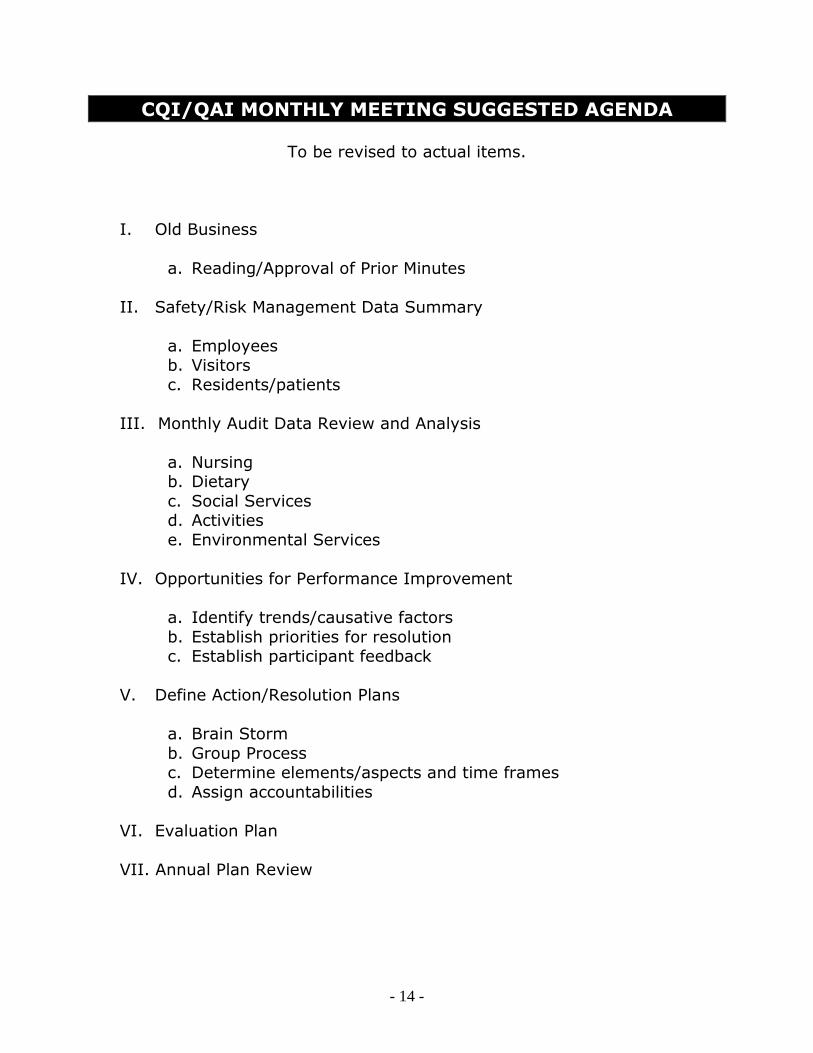
- 14 -
CQI/QAI MONTHLY MEETING SUGGESTED AGENDA
To be revised to actual items.
I. Old Business
a. Reading/Approval of Prior Minutes
II. Safety/Risk Management Data Summary
a. Employees b. Visitors
c. Residents/patients
III. Monthly Audit Data Review and Analysis
a. Nursing b. Dietary
c. Social Services d. Activities
e. Environmental Services
IV. Opportunities for Performance Improvement
a. Identify trends/causative factors
b. Establish priorities for resolution c. Establish participant feedback
V. Define Action/Resolution Plans
a. Brain Storm
b. Group Process c. Determine elements/aspects and time frames
d. Assign accountabilities
VI. Evaluation Plan
VII. Annual Plan Review

- 15 -
CQI/QAI MONTHLY MONITORING TOOL
Month ___________________ Quarter ______________ Year __________
Characteristics of population receiving care/services:
Types/Placement of Lines Total Number Percentage
Central Lines ___________ ___________ Peripheral Lines ___________ ___________
Total Number of Access ___________ ___100%___
Complications of IV Lines Total Number Percentage
Site Infections ___________ ___________
Infiltrations ___________ ___________ Suspected Over hydration ___________ ___________
Failures to Access ___________ ___________ Suspected Drug Reactions ___________ ___________
Total Number of Complications ___________ ___100%___
Type of Therapies Delivered Total Number Percentage
Hydration ___________ ___________ Antibiotics ___________ ___________
Pain Management ___________ ___________ Cytotoxic Agents ___________ ___________
Chemotherapeutic Agents ___________ ___________ Total Parenteral Nutrition (TPN) ___________ ___________
Peripheral Parenteral Nutrition (PPN) ___________ ___________ Blood or Blood Products ___________ ___________
IVIG/Immunoglobulins ___________ ___________ IV Push Medications ___________ ___________
Other ______________________ ___________ ___________
Total Number of Therapies ___________ ___100%___
Opportunities to improve performance identified in the above data: _______
__________________________________________________________________________________________________________________________
Suggest an indicator or aspect for increased monitoring: _______________
__________________________________________________________________________________________________________________________
_____________________________________________________________
- 1 -
INFECTION CONTROL A. Purpose
1. To establish the underlying principles of Universal Precautions as
the basis for infection control in this facility.
2. To prevent and/or minimize the occurrence of infectious disease
and cross contamination in this facility.
3. The OSHA guidelines are appropriate and applicable to the work environment of a nurse performing IV therapy procedures.
4. The staff receives training and education in Infection Control as part
of the facility general orientation.
B. Special Considerations for the Nursing Staff
1. Certain health hazards are inherent in maintaining an IV Therapy Program because of the nurse’s exposure to blood. The nurse may
be exposed to residents whose disease is transmitted via blood. Care in initiating IV therapy should be taken with all residents,
whether or not the admitting diagnosis indicates infectious status.
2. Good hand washing technique is imperative before and after
resident contact and immediately if hands are contaminated. Gloves must be worn at all times when there is the likelihood of
contact with blood and/or body fluids.
3. Protective gowns should be worn when there is the potential for contamination of clothing with blood, body fluids and communicable
disease. Masks and goggles should be worn when there is the likelihood of splashing blood and/or body fluids.
4. Sharp items present the greatest risk of exposure and must be
disposed of in a puncture-resistant container designated for sharps. Never shave the hair around a venipuncture site; clip hair with
scissors before starting venipuncture.
C. Special Considerations for the Housekeeping Staff
1. Equipment and floors which may have been contaminated with
blood should be washed immediately.
- 2 -
INFECTION CONTROL 2. Rubber household gloves should be worn for these cleaning and
decontamination procedures involving the likelihood of contact with blood and/or body fluids.
D. Infection Control Methods
1. Document suspected IV infections and promptly inform the physician.
2. Secure IV administration set junctions with luer lock or junction-
clasping device.
3. Employ strict aseptic techniques when piggy-back medications or bolus medication injections are administered through injection
ports.
4. Disinfect injection ports on tubing prior to inserting needle.
5. Use a new sterile needle or catheter for every insertion attempted.
6. Monitor resident closely for signs of phlebitis; rotate peripheral site
every 72 hours.
*A physician’s order is required to leave an IV in longer than 72 hours.
7. If contamination is suspected, cultures are taken to determine
source and type of micro-organism.
8. Change tubing and solutions at intervals stated in this manual.
9. Maintain closed systems.
E. Disposal of Contaminated Waste
1. All infections or contaminated wastes shall be disposed of in the
following manner:
a. Used syringes, needles and IV catheters: All needles, syringes and IV catheters will be discarded uncapped and uncut into a
one-way, puncture-proof waste container.

- 3 -
INFECTION CONTROL b. IV dressings: All contaminated waste shall be double-bagged (in
plastic) for disposal. Do not throw away in bedside trash receptacle.
F. Management of IV Related Infections
1. Even with the most conscientious care by all members of the IV team, infusion-related infections may occur. When an infusion-
related infection is suspected, both the cannula and a sample of the IV solution should be cultured. (Contact physician for specific
orders.)
2. Refer to Facility’s Infection Control Manual for complete measures in infection control.

- 1 -
COMPLICATIONS MANAGEMENT A. Purpose
1. To provide guidelines to nursing staff for the immediate nursing
intervention and management of complications arising from IV therapy for residents/patients.
2. To establish that Nursing Process is the basis of all nursing interventions. The five steps in Nursing Process are:
a. Assessment
b. Problem Identification (nursing diagnosis) c. Planning
d. Implementation e. Evaluation
B. How to Use this Section: Nursing Process Actions
1. Perform a physical assessment and record observation
(assessment)
2. Identify signs and symptoms present which lead to identification of
a problem, i.e., hematoma (nursing diagnosis).
3. Review nursing actions in this section appropriate to the nursing diagnosis (planning).
4. Implement nursing actions or contact the physician for orders
(implementation).
5. Reassess the resident/patient on an ongoing basis for resolution of the problem or progress toward goals (evaluation).
C. Peripheral IV: Hematoma
1. Definition: Raised, discolored area caused by leakage of blood at
venipuncture site.
2. Signs and symptoms
a. Tenderness at venipuncture site.
b. Area around site appears “bruised” or discolored.

- 2 -
COMPLICATIONS MANAGEMENT c. Inability to advance or flush IV.
d. Swelling around venipuncture site.
3. Possible causes
a. Vein “blown” or punctured through back wall at time of venipuncture.
b. Leakage of blood from needle displacement.
c. Not applying pressure to IV site after removal of IV.
d. Reapplying tourniquet to extremity immediately after an
unsuccessful IV insertion attempt or IV removal.
4. Nursing actions
a. Remove IV device.
b. Apply firm pressure to site and cold soaks to affected area for
first 24 hours. Apply warm soaks thereafter.
c. Raise extremity above heart.
d. Recheck for bleeding.
e. Document all symptoms, actions taken and patient response.
5. Prevention measures
a. Do not advance needle further if resistance is met on venipuncture
b. Choose a vein that can accommodate size of IV device
c. Do not reapply tourniquet to an extremity immediately after removing the IV.
d. When discontinuing an IV, apply pressure to the site 1-2 minutes
after removing the IV.

- 3 -
COMPLICATIONS MANAGEMENT D. Peripheral IV: Infiltration
1. Definition: Leakage of IV fluid into surrounding tissues
2. Signs and symptoms
a. Swelling tenderness above IV site that may extend along entire limb.
b. Cool skin temperature around site.
c. Fluid continues to infuse even when vein is occluded.
d. Backflow of blood may be absent.
e. IV flow rate slower or stopped.
f. Resident complains of pain in affected area
3. Possible causes
a. Needle dislodged from vein or vein perforated.
4. Nursing actions
a. Remove IV device
b. Apply warm soaks to aid absorption.
c. Elevate extremity.
d. Restart IV infusion above infiltration or in another limb.
e. Document infiltration, symptoms, actions taken and patient response.
5. Preventative measures
a. Check IV site frequently (especially when using IV pump).
b. Do not obscure area above site with tape.

- 4 -
COMPLICATIONS MANAGEMENT c. Avoid placing IV in area of flexion.
d. If site is located at area of flexion, restrict movement of limb by
placing on arm board.
e. Teach appropriate resident to observe the IV site and report any
pain, swelling, etc.
E. Peripheral IV: Phlebitis
1. Definition: Irritation along vein
2. Signs and symptoms
a. Area along vein is red, tender, warm and swollen.
b. Vein “hard” and cord like when palpated
c. Decreased IV flow rate.
d. Irritation increases with infusion.
3. Possible causes
a. Hypertonic medications or solutions.
b. Repeated use of same vein for therapy or not rotating IV site
every 72 hours.
c. Movement of device in vein.
d. Device too large or flow rate too rapid for size of vein.
e. Clotting at tip of catheter (Thrombophlebitis).
4. Nursing actions
a. Remove IV device
b. Apply warm soaks; elevate extremity.
c. Notify physician.
- 5 -
COMPLICATIONS MANAGEMENT d. Restart IV infusion in a different limb.
e. Document location of phlebitis, symptoms, actions taken and
resident’s response.
5. Prevention measures
a. Use large or central veins for hypertonic solution infusion.
b. Choose smallest device fore viscosity of infusate and size of vein.
c. Rotate IV site every 72 hours
d. Verify drug compatibilities prior to infusion.
e. Stabilize the device to decrease movement in vein.
F. Peripheral IV: Site Infection
1. Definition: Local contamination of insertion site.
2. Signs and symptoms
a. Pain, redness, warmth, tenderness and swelling at IV site.
b. Possible exudates of purulent material at IV site.
c. Possible spike in temperature.
3. Possible causes
a. Failure to maintain aseptic technique during insertion or site care.
b. Failure to rotate site every 72 hours and PRN.
c. Immunosuppression
4. Nursing actions
a. Remove IV.

- 6 -
COMPLICATIONS MANAGEMENT b. Culture tip of device and IV site if physician orders.
c. Clean site and apply bacteriostatic ointment
d. Notify physician
e. Restart IV in a new location
f. Document location, symptoms, actions taken and resident’s response.
5. Prevention Measures.
a. Wash hands before starting IV.
b. Maintain aseptic technique during insertion
c. Use only sealed sterile IV catheters.
d. Disinfect skin before IV insertion.
e. Apply occlusive sterile dressing to IV site.
f. Change IV site per policy.
g. Educate staff on site monitoring and aseptic technique.
h. Check site frequently
G. Peripheral IV: Clotting
1. Definition: Blockage at end of device in resident’s vein.
2. Signs and symptoms
a. Unable to flush easily.
b. Tenderness at IV site.
c. Sluggish flow rate.
3. Possible causes

- 7 -
COMPLICATIONS MANAGEMENT
a. IV not heparinized per policy.
b. IV allowed to run dry.
c. Gauge of catheter larger than lumen of vein.
d. IV rate too slow to keep vein open.
4. Nursing actions
a. Do not attempt to aspirate clotting with syringe.
b. If resistance is encountered, do not irrigate; this could result in causing an emboli (traveling blood clot), which is potentially
fatal.
c. Remove and restart IV.
d. Document symptoms, actions taken and resident’s response.
5. Prevention measures
a. Routine saline/heparin flushes as ordered.
b. Monitor IV and solution frequently.
c. Use an IV catheter which is smaller than the vein lumen.
H. Peripheral IV: Catheter Embolism
1. Definition: All or part of IV device shears into vein.
2. Signs and symptoms
a. Related to specific location of embolus: discomfort, decreased
B/P, cyanosis, increased pulse, respiratory distress, and
unconsciousness.
3. Possible causes
a. Use of scissors near IV site (i.e., to remove tape).

- 8 -
COMPLICATIONS MANAGEMENT b. Reinserting (needle) stylet through IV catheter (catheter
shearing).
c. Using a needle longer than 1 inch through the PRN injection plug cap.
4. Nursing actions
a. Apply tourniquet above IV site.
b. Stop IV flow.
c. Call 911 for transport to acute hospital.
d. Notify physician.
e. Immediately obtain X-ray.
f. Document symptoms, action taken and patient response.
5. Prevention measures
a. Do not use scissors near IV site.
b. Withdraw IV device and stylet, together if IV insertion is
unsuccessful.
c. Inspect IV device before insertion for flaws.
d. Never use a needle longer than 1 inch through an injection plug cap.
e. Never reinsert stylet or needle through IV catheter.
f. Label all IVs with catheter length
g. Inspect all discontinued IVs to see if catheter is intact.
h. Use only radiopaque IV catheters.

- 9 -
COMPLICATIONS MANAGEMENT I. Peripheral and Central Venous Catheters: Air Embolism
1. Definition: Air in the circulatory system; more common with a
central venous catheter.
2. Signs and symptoms
a. Respiratory distress, unequal breath sounds
b. Weak, rapid pulse
c. Decreased B/P
d. Loss of consciousness
e. Cyanosis
f. Churning murmur over heart
3. Possible causes
a. Disconnected IV tubing.
b. IV tubing not purged of air before infusion
c. Broken or cracked central catheter.
d. Cap loose or missing from central catheter hub.
e. Catheter clamp or Valsalva maneuver not used during cap or extension set change.
4. Nursing actions
a. Discontinue IV flow.
b. Turn resident to left side, head down and administer oxygen
c. Clamp with Darvon clamp if catheter is broken or “open to air”. With a Groshong catheter, fold tubing to occlude lumen and
tape.
- 10 -
COMPLICATIONS MANAGEMENT d. Notify physician
e. Document symptoms, action taken and patient response
5. Prevention measures
a. Prime tubing before administering.
b. Secure connections.
c. Utilize luer lock injection cap on all central lines.
d. Teach resident to hold breath and to bear down (Valsalva maneuver) during cap change or clamp central catheter.
e. Utilize in line air eliminating filters
f. Monitor IV infusions frequently
g. Dravon clamp taped at head of bed with all patients having
central venous catheter except when using a Groshong catheter.
J. Central Venous Catheters: Occlusion
1. Definition: Blockage of catheter
2. Signs and symptoms
a. Inability to withdraw blood.
b. Inability to flush or infuse solution without resistance.
3. Possible causes
a. Failure to flush catheter, per protocol, or improper flushing
technique.
b. Blood clot formation in catheter.
c. Formation of fibrin sheath on catheter

- 11 -
COMPLICATIONS MANAGEMENT d. Infusion of incompatible infusates resulting in precipitate
formation in catheter
e. IV allowed to run dry.
f. Blood backed up into catheter
4. Nursing actions
a. Do not forcefully irrigate (catheter may rupture).
b. Reposition resident, have resident lie on side, cough, raise are
on side of catheter or sit up. Gently attempt to flush catheter with 5cc of normal saline.
c. Attempt to aspirate clot (do not flush).
d. Notify physician.
e. Obtain a dye study x-ray of catheter, if ordered.
f. Declot catheter with a fibrinolytic agent as ordered by physician.
g. Document symptoms, action taken and patient response.
5. Prevention measures
a. Heparin flush catheter routinely with positive pressure technique.
b. Use infusion pump
c. Saline flush catheter before and after medication administration to prevent precipitate formation.
K. Central Venous Catheters: Deep Vein Thrombosis
1. Definition: Formation of a thrombus (clot) in the large vessel where the central catheter is placed.
2. Signs and symptoms
- 12 -
COMPLICATIONS MANAGEMENT
a. Edema and tenderness or pain at catheter insertions site, neck,
face, shoulder or arm on the same side as the catheter.
b. Signs and symptoms of pulmonary embolism
c. Sluggish flow.
3. Possible causes
a. Traumatic catheter insertion
b. Composition of catheter material (i.e., PVC catheters are more
stiff and thrombogenic).
c. Clotting disorder of resident.
d. Infusion or irritating IV fluid
e. Repeated use or prolonged usage of same vessel.
f. May be related to diameter or catheter in relation to resident’s
vessel size.
4. Nursing actions
a. Notify MD
b. Verify thrombosis via X-ray
c. Infuse heparin or thrombolytic therapy as ordered by the physician.
d. Apply warm compress locally.
e. Do not use limb on affected side for subsequent venipuncture.
f. Document
5. Prevention measures
a. Maintain steady flow rate.
- 13 -
COMPLICATIONS MANAGEMENT b. Use catheters of less thrombogenic materials
c. Dilute irritating fluids.
d. Use heparin flush per protocol.
e. Use 0.22-micron filter
f. Avoid excessive movement of catheter during dressing change procedures.
L. Central Venous Catheters: Local Infection
1. Definition: Local contamination of insertion site, exit site, or
infection of subcantaneous tunnel.
2. Signs and symptoms
a. Redness, warmth, tenderness, or swelling at site.
b. Possible exudates of purulent material.
c. Local rash or pustules.
d. Elevated temperature, chills, malaise.
3. Possible causes
a. Failure to maintain aseptic technique during insertion or catheter
care.
b. Failure to comply with dressing change protocol; wet or soiled dressing left on site.
c. Immunosuppression
d. Irritated suture line.
e. Resident sensitive to povidone-iodine.

- 14 -
COMPLICATIONS MANAGEMENT
4. Nursing actions
a. Notify physician.
b. Monitor temperature frequently.
c. Culture site.
d. Use topical antibiotic ointments or commercial bacteriostatic dressings as ordered.
e. Daily site care and dressing change with gauze dressing; no
transparent occlusive dressings, until infection resolves.
f. Treat systemically with appropriate medications
g. Catheter may be removed
h. Remove sutures, if involved.
i. Document
5. Prevention measures
a. Maintain strict aseptic technique
b. Adhere to sterile dressings change protocol, including frequency
of change
c. Teach resident regarding care (i.e., during bathing).
d. Change dressing immediately if soiled or wet.
e. Change dressing more frequently, if around a trach or femoral area.
f. Complete ostomy care and wound dressings after central catheter care.
g. Maintain aseptic technique during solution and tubing changes
and use appropriate filter.
- 15 -
COMPLICATIONS MANAGEMENT h. Adhere to IV tubing and injection cap extension tube protocols,
including frequency of change.
M. Systemic Infection
1. Definition: Septicemia or bacteremia caused by introduction of
microorganisms into the circulatory system. Primary: from catheter itself.
Secondary: from other source seeded to catheter.
2. Signs and symptoms
a. Elevated temperature, chills without other apparent reason
b. Leukocytosis (elevated WBC)
c. Nausea and vomiting; malaise
d. Elevated blood glucose levels.
e. Headache
f. Shock
3. Possible causes
a. Contaminated catheter, hub or infusate
b. Failure to maintain aseptic technique during procedures
c. Contaminated injection cap
d. Frequent opening of catheter and system
e. Long-term use
f. Immunosuppression
g. Non-catheter related sepsis

- 16 -
COMPLICATIONS MANAGEMENT
4. Nursing actions
a. Notify physician
b. Draw central and peripheral blood cultures. If the same
organism is cultured form both sites, then the catheter may be
the primary source of sepsis and may be removed. If the cultures do not match but are both positive, the infection may be
treated with antibiotics through the catheter or the catheter may be removed. If only the peripheral culture is positive, then the
catheter is not the source.
c. Culture catheter tip if removed
d. Discontinue infusion, change IV solution, tubing and filter.
e. Evaluate for other sources of infection.
f. Monitor resident closely.
g. Document symptoms, actions taken and patient response.
5. Prevention measures
a. Examine fluid container for cloudiness, leakage and turbidity
before infusing
b. Before infusing, monitor glucose levels on TPN residents; notify physician if elevated.
c. Use strict sterile technique for all procedures
d. Use appropriate filter.
e. Avoid opening system and disinfect injection plug before each
entry.
f. In-service ancillary staff regarding proper precautions in
maintaining dressing integrity.
g. Secure all connections.

- 17 -
COMPLICATIONS MANAGEMENT N. Circulatory Overload
1. Definition: more fluid volume than system can manage.
2. Signs and symptoms
a. Resident discomfort, neck vein engorgement
b. Increased B/P
c. Shortness of breath, rales, fluid in lungs
d. Fluid intake greater than fluid output
e. Edema and weight increase
3. Possible causes
a. Infusing without pump (gravity drip)
b. Roller clamp fully opened
c. Resident unable to tolerate calculated fluid requirements
d. Incorrect infusion rate
4. Nursing actions
a. Slow or stop infusion rate.
b. Raise head of bed.
c. Monitor vital signs and respiratory status.
d. Keep resident warm to promote peripheral circulation and ease
the stress on central veins.
e. Notify physician.
f. Document symptoms, actions taken and resident response.
- 18 -
COMPLICATIONS MANAGEMENT
5. Prevention measures
a. Double check IV order for rate. Check fluid requirement for age,
size and condition of resident.
b. Educate resident not to manipulate pump or roller clamp.
c. Monitor I&O
d. Use a controlling device to infuse all IV solutions
e. Check IV flow rate frequently.
I
FORMS
The following forms are intended to be used as a guideline for the facility.
The facility may choose to use different forms which meet the internal
requirements of the facility. M Chest Pharmacy recommends that each
facility carefully review form utilization to ensure legal, regulatory and
clinical standards of practice.
Contents
Annual IV Skills Competency Validation Checklist – Use to validate staff skills
CQI/QAI Forms – Use these forms with CQI/QAI/QA processes, facility specific.
Annual Continuous Quality Improvement Activities Calendar
CQI/QAI Council Quarterly Report CQI/QAI Data Collection Tool Aspect of Care: Central Venous Access
Device CQI/QAI Data Collection Tool Aspect of Care: Intravenous
Tubing/Solutions CQI/QAI Data Collection Tool Aspect of Care: IV Pumps - Electronic
CQI/QAI Data Collection Tool Aspect of Care: Peripheral Intravenous
Device CQI/QAI Monitoring Tool Aspect of Care: Central Venous Access
Device CQI/QAI Monitoring Tool Aspect of Care: Intravenous
Tubing/Solutions CQI/QAI Monitoring Tool Aspect of Care: IV Pumps - Electronic
CQI/QAI Monitoring Tool Aspect of Care: Peripheral IntravenousDevice
CQI/QAI Monthly Meeting Suggested Agenda CQI/QAI Monthly Monitoring Tool
IV Medication Sheet – Use for documenting nursing actions for routine IV
medications. IV Piggy Back Competency Validation Checklist – Use to validate staff skills
IV Starts Competency Validation Checklist – Use to validate staff skills
Peripheral IV Starts Competency Validation Checklist – Use to validate staff Skills
Physician’s Protocol for Anaphylaxis – Use for initial/first dose antibiotics

II
ANNUAL IV SKILLS COMPETENCY VALIDATION CHECKLIST
PROCEDURES
DATES
COMPLETED
PRECEPTOR’S
INITIALS IV Starts (3)
Heparin Lock Flush Peripheral/Central Line (RN)
Accessing Central Lines & Implantable Port (RN)
Blood Specimens from a
Central Line (RN)
Central Line Dressing
Documentation
IV Pump Orientation & Usage
Review of IV P&P Manual
IV Ordering Procedures with
Pharmacy
TPN Pre-admission Process
Contents of IV ER Box
Verify RN’s & LVN/LPN’s License & Proof of IV Training and
Certification; i.e., copy of Orientation & Review or
Certification Course
Staff Nurse’s Name (print): _______________________________________
Staff Nurse’s Signature: _______________________ Date: ____________
Preceptor’s Name & Title (print):___________________________________
Preceptor’s Signature: _________________________ Date: ____________
Note: Complete this checklist annually for all staff members involved in the IV Therapy program. This form is to be kept in the Personnel File.
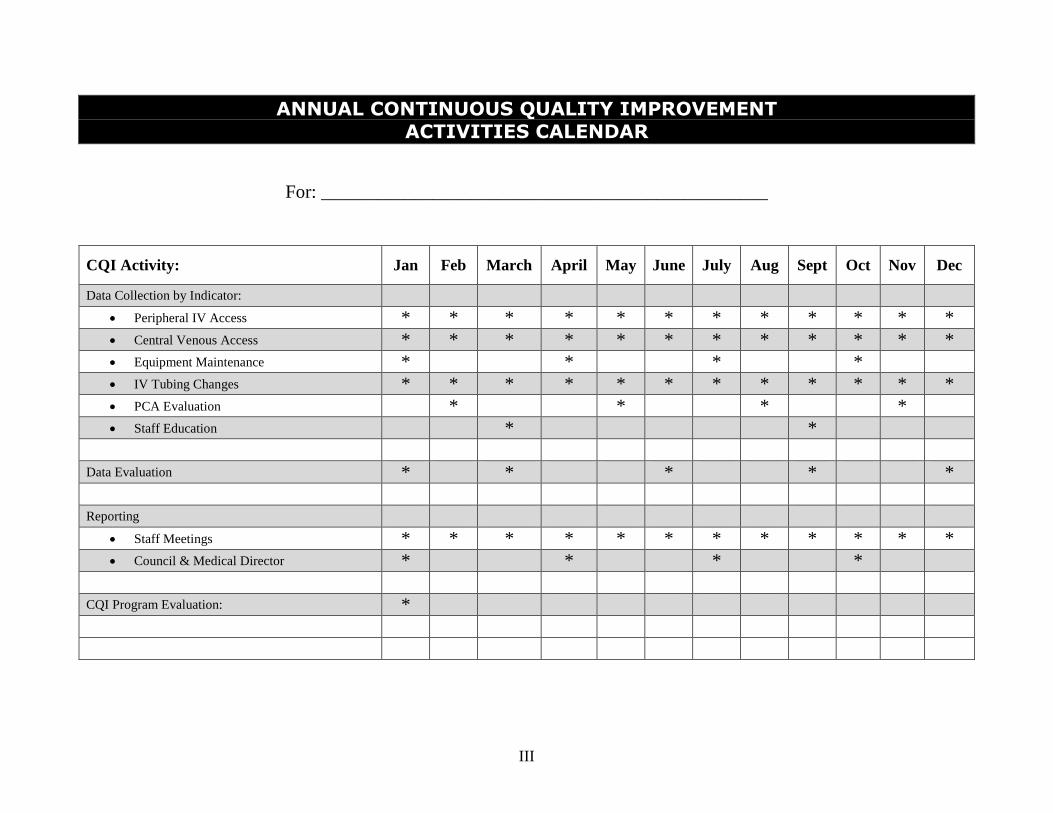
III
ANNUAL CONTINUOUS QUALITY IMPROVEMENT ACTIVITIES CALENDAR
For: ________________________________________________
CQI Activity: Jan Feb March April May June July Aug Sept Oct Nov Dec
Data Collection by Indicator: Peripheral IV Access * * * * * * * * * * * * Central Venous Access * * * * * * * * * * * * Equipment Maintenance * * * * IV Tubing Changes * * * * * * * * * * * * PCA Evaluation * * * * Staff Education * *
Data Evaluation * * * * * Reporting
Staff Meetings * * * * * * * * * * * * Council & Medical Director * * * *
CQI Program Evaluation: *

IX
CQI/QAI COUNCIL QUARTERLY REPORT
Reported by ________________________________
Date of report ________________________________
For quarter ended ________________________________
V. Aspects of care/services reviewed this quarter:
__________________________________ ___________________________________
__________________________________ ___________________________________
__________________________________ ___________________________________
VI. Describe opportunities to improve performance in care/services:
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
VII. Summary of actions implemented to address opportunities to improve performance:
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
VIII. Progress toward unresolved opportunities to improve performance from previous report:
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
___________________________________________ ________________________
Signature Date

X
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: CENTRAL VENOUS ACCESS DEVICE
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-)
N/A Central Venous Access Device Dressings:
Changed per MD order or 2 times weekly Dressing labeled with date, time and initials Injection ports changed per MD order or 2 times weekly Dressing are dry and occlusive Dravon clamp at bedside (except Groshong/PICC)
Documentation includes observations of the following: Type of central venous access device in use Location of exit site Appearance of exit site Type of dressing and appearance Signs and symptoms of complications and nursing actions
Central Venous Access Device Flushing Protocols (Heparin): MD order includes strength, volume and frequency Volume of flush appropriate for device in place Implanted ports accessed and flushed monthly Groshong catheters flushed weekly, when not in use
Emergency IV Box: If opened, sealed with red seal and pharmacy notified □ Yes □ No If sealed, expiration date of oldest item listed □ Yes □ No Contents list attached to outside □ Yes □ No Physician’s Authorization, if required, is present □ Yes □ No
Problems identified:_____________________________________________
__________________________________________________________________________________________________________________________
Recommendations/solutions:___________________________________________________________________________________________________
_____________________________________________________________

XI
Signature of auditor _____________________________ Date___________
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Intravenous Tubing (includes filters/extension tubing):
Each IV tubing labeled with date, time and initials IV tubing used for continuous infusion changed
every 48 hours
IV tubing used for intermittent therapy changed every
24 hours
Injection port adapter for intermittent therapy changed
prior to each use
Vented tubing used with glass containers
Intravenous Solutions: All IV solutions are changed every 24 hours IV solution containers are labeled with date, time hung,
and initials
Pharmacy label attached to all solutions with complete
order
IV solution matched physician’s orders IV rate is consistent with physician’s orders IV basic solution is within expiration date or label
expiration date
Medication Label Additive stickers present and
complete for meds added in facility
(continued)
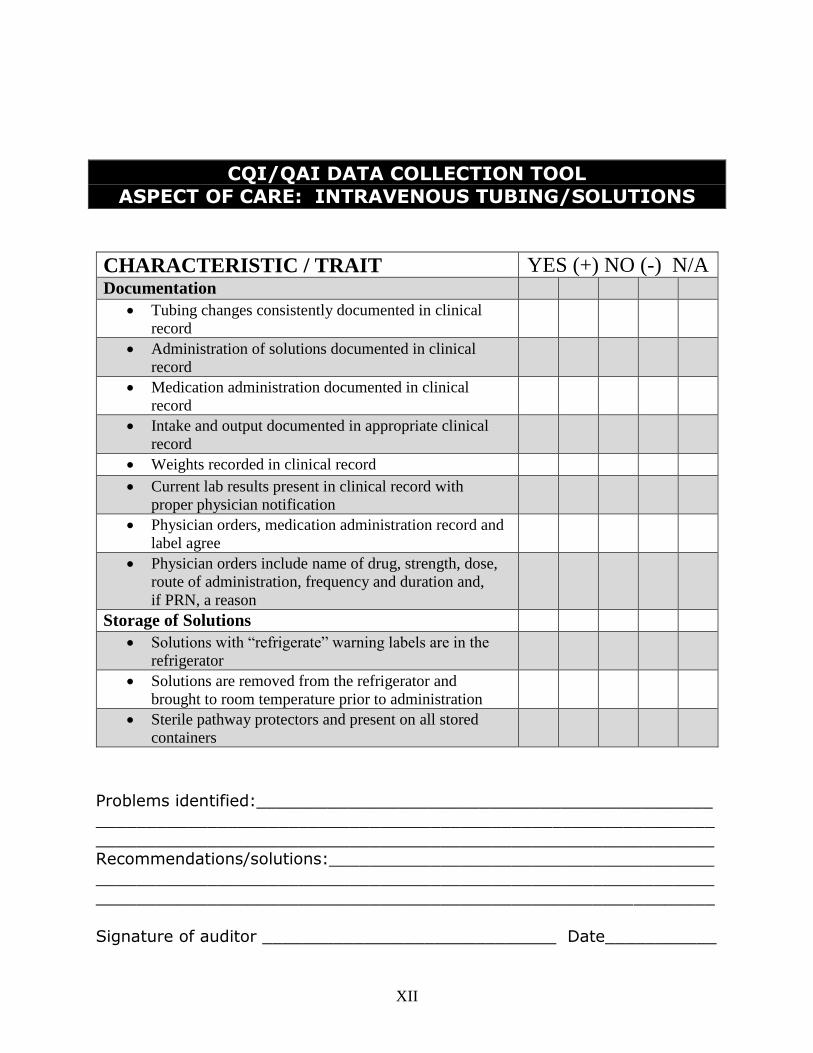
XII
CQI/QAI DATA COLLECTION TOOL
ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Documentation
Tubing changes consistently documented in clinical
record
Administration of solutions documented in clinical
record
Medication administration documented in clinical
record
Intake and output documented in appropriate clinical
record
Weights recorded in clinical record Current lab results present in clinical record with
proper physician notification
Physician orders, medication administration record and
label agree
Physician orders include name of drug, strength, dose,
route of administration, frequency and duration and,
if PRN, a reason
Storage of Solutions Solutions with “refrigerate” warning labels are in the
refrigerator
Solutions are removed from the refrigerator and
brought to room temperature prior to administration
Sterile pathway protectors and present on all stored
containers
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________

XIII
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: IV PUMPS - ELECTRONIC
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Electronic Pumps
Operating Manual available for each pump Pumps plugged into a grounded outlet Back-up batteries available (ambulatory pumps) Pump alarms are audible at nurses station Soiled pumps stored in soiled utility room
(must be returned to Pharmacy for cleaning)
Pumps securely mounted on wide base poles Ambulatory pumps have “fanny packs” for carriers
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
_____________________________________________________________
_____________________________________________________________
Signature of auditor _____________________________ Date___________
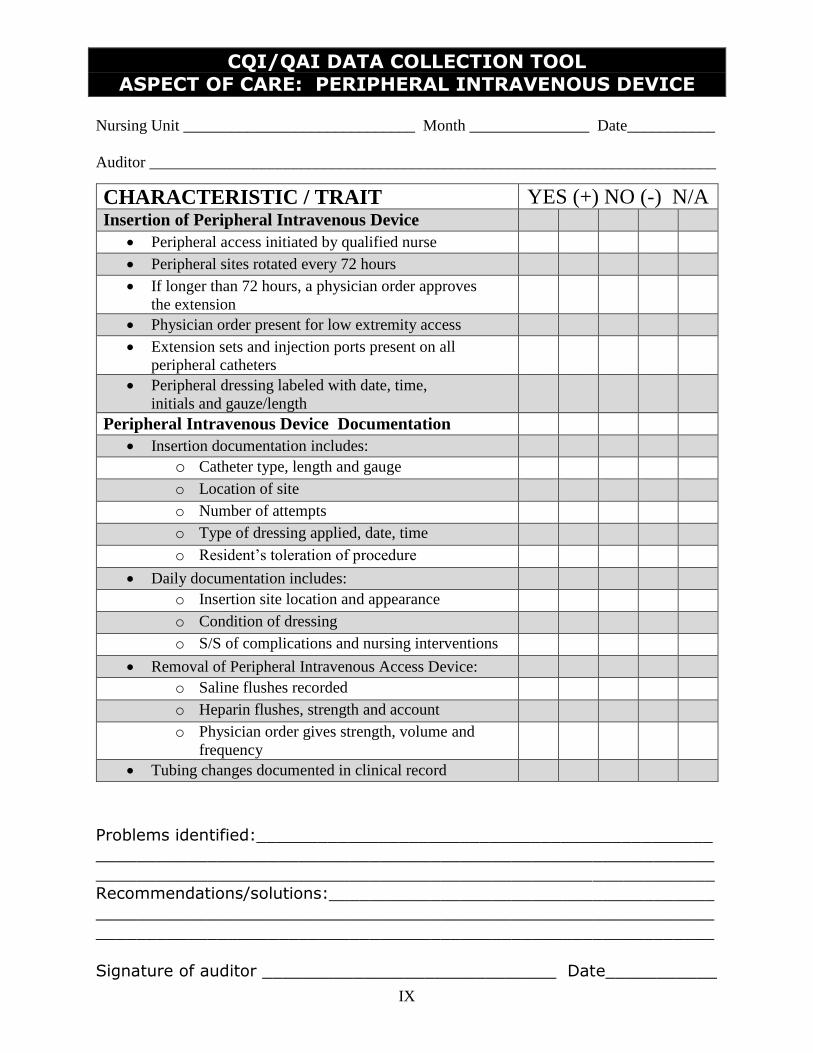
IX
CQI/QAI DATA COLLECTION TOOL ASPECT OF CARE: PERIPHERAL INTRAVENOUS DEVICE
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
CHARACTERISTIC / TRAIT YES (+) NO (-) N/A Insertion of Peripheral Intravenous Device
Peripheral access initiated by qualified nurse Peripheral sites rotated every 72 hours If longer than 72 hours, a physician order approves
the extension
Physician order present for low extremity access Extension sets and injection ports present on all
peripheral catheters
Peripheral dressing labeled with date, time,
initials and gauze/length
Peripheral Intravenous Device Documentation Insertion documentation includes:
o Catheter type, length and gauge o Location of site o Number of attempts o Type of dressing applied, date, time o Resident’s toleration of procedure
Daily documentation includes: o Insertion site location and appearance o Condition of dressing o S/S of complications and nursing interventions
Removal of Peripheral Intravenous Access Device: o Saline flushes recorded o Heparin flushes, strength and account o Physician order gives strength, volume and
frequency
Tubing changes documented in clinical record
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________
Recommendations/solutions:___________________________________________________________________________________________________
_____________________________________________________________
Signature of auditor _____________________________ Date___________

X
CQI/QAI MONITORING TOOL ASPECT OF CARE: CENTRAL VENOUS ACCESS DEVICE
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
Central Venous Access Device dressings: Number Percentage
Change per MD order or 2 times weekly of
Dressing labeled with date, time and initials of
Injection ports changed per MD order or
2 times weekly of
Dressings are dry and occlusive of
Dravon clamp at bedside (except Groshong/PICC) of
Documentation includes observation of the following:
Type of central venous access device in use of
Location of exit site of
Appearance of exit site of
Type of dressing and appearance of
Signs and symptoms of complications and nursing actions of
Comprehensive plan of care includes Intravenous Therapy of
Central Venous Access Device Flushing Protocols
(Heparin): of
MD order includes strength, volume and frequency of
Volume of flush appropriate for device in place of
Implanted ports accessed and flushed monthly of
Groshong catheters flushed weekly, when not in use of
Emergency IV Box:
If opened, sealed with red weal and pharmacy notified □ Yes □ No
If sealed, expiration date of oldest item listed □ Yes □ No
Contents list attached to outside □ Yes □ No
Physician’s Authorization, if required, is present □ Yes □ No
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________

XIV
CQI/QAI MONITORING TOOL ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
Intravenous Tubing (includes filters/extension tubing: Number Percentage
Each IV tubing labeled with date, time and initials of
IV tubing used for continuous infusion changed every
48 hours of
IV tubing used for intermittent therapy changed every 24
hours of
Injection port adapter for intermittent therapy changed prior
to each use of
Vented tubing used with glass containers of
Intravenous Solutions
All IV solutions are changed every 24 hours of
IV solution containers are labeled with date, time hung
and initials of
Pharmacy label attached to all solutions with complete order of
IV solution matched physician’s orders of
IV basic solution is within expiration date or label expiration
date of
Medication Label Additive stickers present and complete for
meds added in facility of
(continued)

XV
CQI/QAI MONITORING TOOL ASPECT OF CARE: INTRAVENOUS TUBING/SOLUTIONS
Documentation Number Percentage
Tubing changes consistently documented in clinical record of
Administration of solutions documented in clinical record of
Medication administration documented in clinical record of
Intake and output documented in appropriate clinical record of
Weights recorded in clinical record of
Current lab results present in clinical record with proper physician notification
of
Physician orders, medication administration record and label
agree of
Physician orders include name of drug, strength, dose,
route of administration, frequency and duration and, if PRN,
a reason
of
Storage of Solutions
Solutions with “refrigerate” warning labels are in the
refrigerator of
Solutions are removed from the refrigerator and brought
to room temperature prior to administration of
Sterile pathway protectors are present on all stored containers of
Problems identified:_____________________________________________
__________________________________________________________________________________________________________________________
Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________

XIII
CQI/QAI MONITORING TOOL ASPECT OF CARE: IV PUMPS - ELECTRONIC
Electronic Pumps Number Percentage
Operating Manual available for each pump of
Pumps plugged into a grounded outlet of
Back-up batteries available (ambulatory pumps) of
Pump alarms are audible at nurses station of
Soiled pumps stored in soiled utility room
(must be returned to Pharmacy for cleaning) of
Pumps securely mounted on wide base poles of
Ambulatory pumps have “fanny packs” or carriers of
Problems identified:_____________________________________________ _____________________________________________________________
_____________________________________________________________ Recommendations/solutions:______________________________________
__________________________________________________________________________________________________________________________
Signature of auditor _____________________________ Date___________

XVI
CQI/QAI MONITORING TOOL ASPECT OF CARE: PERIPHERAL INTRAVENOUS DEVICE
Nursing Unit _____________________________ Month _______________ Date___________
Auditor _______________________________________________________________________
Insertion of Peripheral Intravenous Device Number Percentage
Peripheral access initiated by qualified nurse of
Peripheral sites rotated every 72 hours of
If longer than 72 hours, a physician order approves
the extension of
Physician order present for low extremity access of
Extension sets and injection ports present on all
peripheral catheters of
Peripheral dressing labeled with date, time,
initials and gauze/length of
Peripheral Intravenous Device Documentation of
Insertion documentation includes: of
o Catheter type, length and gauge of
o Location of site of
o Number of attempts of
o Type of dressing applied, date, time of
o Resident’s toleration of procedure of
Daily documentation includes: of
o Insertion site location and appearance of
o Condition of dressing of
o S/S of complications and nursing interventions of
Removal of Peripheral Intravenous Access Device: of
o Saline flushes recorded of
o Heparin flushes, strength and account of
o Physician order gives strength, volume and
frequency of
Tubing changes documented in clinical record of
Problems identified:_____________________________________________
__________________________________________________________________________________________________________________________
Recommendations/solutions:___________________________________________________________________________________________________
_____________________________________________________________
Signature of auditor _____________________________ Date___________
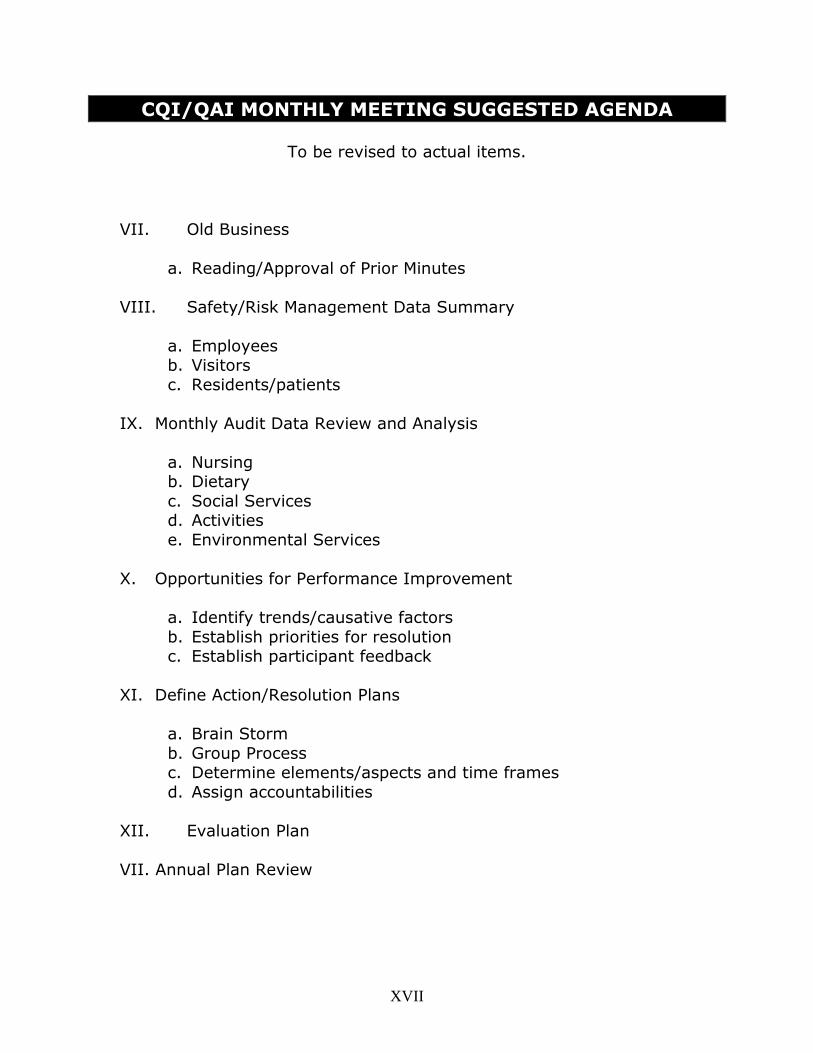
XVII
CQI/QAI MONTHLY MEETING SUGGESTED AGENDA
To be revised to actual items.
VII. Old Business
a. Reading/Approval of Prior Minutes
VIII. Safety/Risk Management Data Summary
a. Employees b. Visitors
c. Residents/patients
IX. Monthly Audit Data Review and Analysis
a. Nursing b. Dietary
c. Social Services d. Activities
e. Environmental Services
X. Opportunities for Performance Improvement
a. Identify trends/causative factors
b. Establish priorities for resolution c. Establish participant feedback
XI. Define Action/Resolution Plans
a. Brain Storm
b. Group Process c. Determine elements/aspects and time frames
d. Assign accountabilities
XII. Evaluation Plan
VII. Annual Plan Review

XVIII
CQI/QAI MONTHLY MONITORING TOOL
Month ___________________ Quarter ______________ Year __________
Characteristics of population receiving care/services:
Types/Placement of Lines Total Number Percentage
Central Lines ___________ ___________ Peripheral Lines ___________ ___________
Total Number of Access ___________ ___100%___
Complications of IV Lines Total Number Percentage
Site Infections ___________ ___________
Infiltrations ___________ ___________ Suspected Over hydration ___________ ___________
Failures to Access ___________ ___________ Suspected Drug Reactions ___________ ___________
Total Number of Complications ___________ ___100%___
Type of Therapies Delivered Total Number Percentage
Hydration ___________ ___________ Antibiotics ___________ ___________
Pain Management ___________ ___________ Cytotoxic Agents ___________ ___________
Chemotherapeutic Agents ___________ ___________ Total Parenteral Nutrition (TPN) ___________ ___________
Peripheral Parenteral Nutrition (PPN) ___________ ___________ Blood or Blood Products ___________ ___________
IVIG/Immunoglobulins ___________ ___________ IV Push Medications ___________ ___________
Other ______________________ ___________ ___________
Total Number of Therapies ___________ ___100%___
Opportunities to improve performance identified in the above data: _______
__________________________________________________________________________________________________________________________
Suggest an indicator or aspect for increased monitoring: _______________
__________________________________________________________________________________________________________________________
_____________________________________________________________
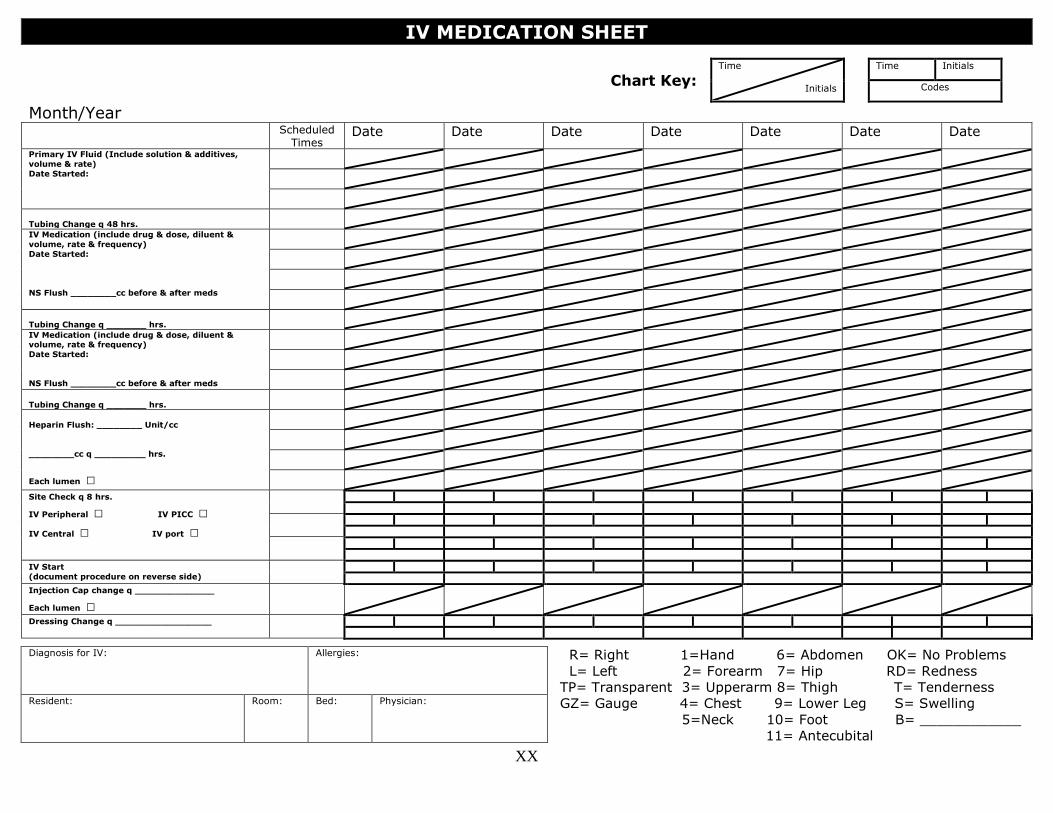
XX
IV MEDICATION SHEET
Chart Key: Time
Initials
Time Initials
Codes
Month/Year
Scheduled Times
Date Date Date Date Date Date Date
Primary IV Fluid (Include solution & additives,
volume & rate)
Date Started:
Tubing Change q 48 hrs.
IV Medication (include drug & dose, diluent &
volume, rate & frequency)
Date Started:
NS Flush ________cc before & after meds
Tubing Change q _______ hrs.
IV Medication (include drug & dose, diluent & volume, rate & frequency)
Date Started:
NS Flush ________cc before & after meds
Tubing Change q _______ hrs.
Heparin Flush: ________ Unit/cc
________cc q _________ hrs.
Each lumen □
Site Check q 8 hrs.
IV Peripheral □ IV PICC □
IV Central □ IV port □
IV Start
(document procedure on reverse side)
Injection Cap change q ______________
Each lumen □
Dressing Change q _________________
R= Right 1=Hand 6= Abdomen OK= No Problems
L= Left 2= Forearm 7= Hip RD= Redness
TP= Transparent 3= Upperarm 8= Thigh T= Tenderness
GZ= Gauge 4= Chest 9= Lower Leg S= Swelling
5=Neck 10= Foot B= ____________
11= Antecubital
Diagnosis for IV: Allergies:
Resident: Room: Bed: Physician:
XXI

XXII
INIT. Signature INIT. Signature INIT. Signature
DATE TIME Comments: Use space below to explain procedures from other side, if needed – (i.e. reason for site change) Nurse’s Initials

XXIV
IV PIGGY BACK COMPETENCY VALIDATION CHECKLIST
Attempt # 1 Attempt # 2 Attempt # 3
Critical Elements DATE PI* DATE PI* DATE PI*
Confirms physician orders for completeness
Checks IV Piggy Back labels for conformity
to physician orders
Verbalizes the indications, side effects
and contraindications of IV Drug
Selects correct Administration set for IVPB
therapy
Calculates flow rate of IV Pump or
gravity infusion and sets rate correctly
Assesses IV site for signs and
symptoms of complications
Instructs resident in procedure and
duration of treatment/therapy
Knows SASH protocol for flushing access
device correctly
Connect tubing sets using aseptic
technique and changes adapter
Initiates IVPB with concurrent hydration
fluids
Initiates IVPB with Heparin Lock only
Documents nursing actions in the clinical
record
Notifies the physician of adverse effects of
outcomes
* Preceptor Initials
Attempt # 1 Attempt # 2 Attempt # 3
_________________ _______ ________________ _______ _________________ _______
RN Preceptor Date RN Preceptor Date RN Preceptor Date
Staff Nurse Name (print): _____________________________________ Title: _____________________
Staff Nurse Signature: ________________________________________ Date Complete: _____________
Note: This checklist indicates the necessary activities to perform Intravenous Piggy Back skills. The checklist
is designed to provide for three precepted attempts to start a peripheral IV. This facility may require less or
more than three precepted attempts. Enter the number of precept attempts required: __________________.

XXV
IV STARTS COMPETENCY VALIDATION CHECKLIST
Critical Elements DATE PI* DATE PI* DATE PI*
Aseptic technique
Selects necessary venipuncture equipment
according to P&P
Applies tourniquet properly
Preps site according to P&P
Performs venipuncture
according to P&P
Release tourniquet
Aseptically attaches IV extension
tubing
Dresses IV catheter site according
to P&P
Documentation according to P&P * Preceptor Initials
Nurse Name (print): _____________________________________________________________________
Nurse Signature: ___________________________________________ Date: _____________________
Preceptor Signature: _________________________________________ Date: _____________________
Note: This checklist indicates the necessary activities to perform IV Starts Skills. The checklist may be used to
help learn the skills. The evaluator will use this form to verify performance of the skills. All activities are
critical and must be included in the skills performance to be rated successful. This form should be used with all
new staff members involved in initiating venipunctures and should be kept in the Personnel Records.
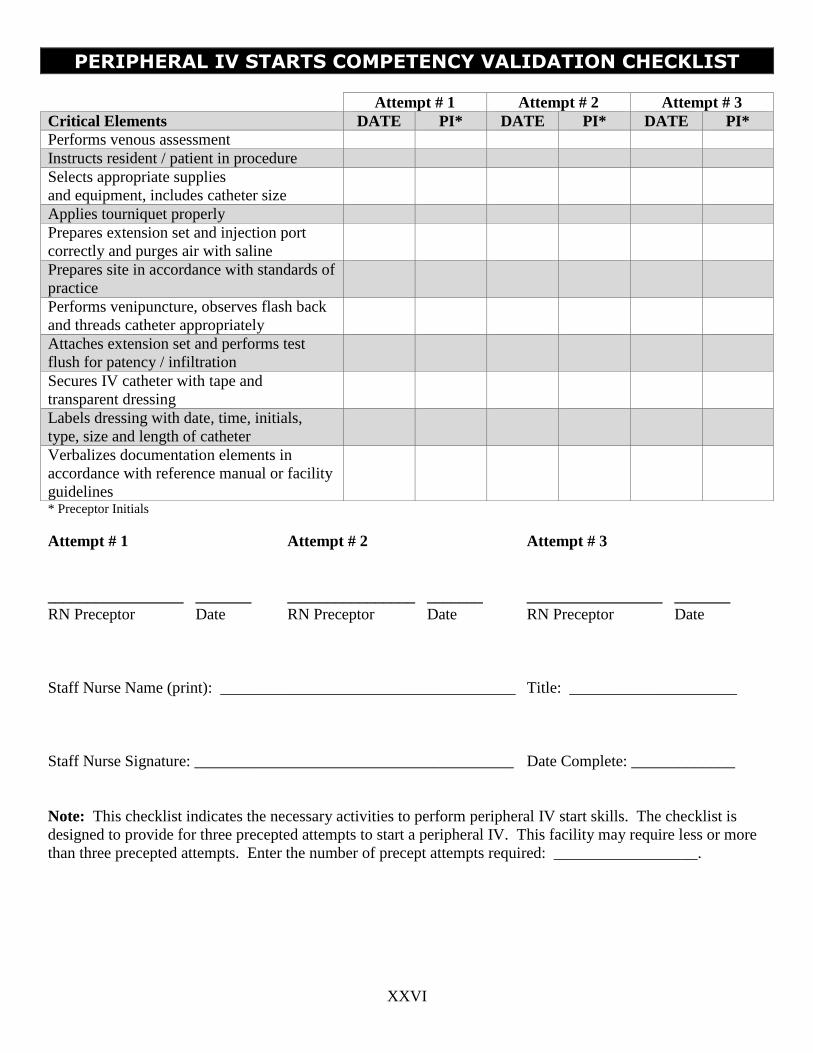
XXVI
PERIPHERAL IV STARTS COMPETENCY VALIDATION CHECKLIST
Attempt # 1 Attempt # 2 Attempt # 3
Critical Elements DATE PI* DATE PI* DATE PI*
Performs venous assessment
Instructs resident / patient in procedure
Selects appropriate supplies
and equipment, includes catheter size
Applies tourniquet properly
Prepares extension set and injection port
correctly and purges air with saline
Prepares site in accordance with standards of
practice
Performs venipuncture, observes flash back
and threads catheter appropriately
Attaches extension set and performs test
flush for patency / infiltration
Secures IV catheter with tape and
transparent dressing
Labels dressing with date, time, initials,
type, size and length of catheter
Verbalizes documentation elements in
accordance with reference manual or facility
guidelines
* Preceptor Initials
Attempt # 1 Attempt # 2 Attempt # 3
_________________ _______ ________________ _______ _________________ _______
RN Preceptor Date RN Preceptor Date RN Preceptor Date
Staff Nurse Name (print): _____________________________________ Title: _____________________
Staff Nurse Signature: ________________________________________ Date Complete: _____________
Note: This checklist indicates the necessary activities to perform peripheral IV start skills. The checklist is
designed to provide for three precepted attempts to start a peripheral IV. This facility may require less or more
than three precepted attempts. Enter the number of precept attempts required: __________________.

XXVII
PHYSICIAN’S PROTOCOL FOR ANAPHYLAXIS
(Adult Protocol)
Patient Name ________________________ Room Number __________ Medical Record Number __________
Assessment Parameters
1. Loss of consciousness
2. Rapid rise or fall in blood pressure, pulse or respiratory rate (from baseline values)
3. Rapid onset of chest, or back pain or general discomfort within five minutes of initiating infusion.
4. Acute, rapid onset of respiratory distress
Planning Parameters
1. Rapidly evaluate vital signs and signs and symptoms
2. Positive assessment finding for Anaphylaxis Reaction
Implementation Parameters
1. Stop IV Infusion
2. Do not leave resident-have another licensed nurse stay with resident
3. Start infusion of Normal Saline 0.9% 500 cc to infuse at 100 cc/hour
4. Immediately have another staff notify EMS & PCP, nurse to remain with patient
5. Administer Epi-Pen (epinephrine) sub-q, may repeat in 15-20 minutes
6. Administer Diphenhydramine (Benadryl) 50 mg IVP or sub-q, one time dose
7. If respiratory distress present, Oxygen at 4-6 L/min. via mask/cannula
Evaluation Parameters
1. Re-assess vital signs every 5 minutes or until stable
2. Assess airway, respirations, and heart rate
3. Start CPR, if cardiopulmonary arrest occurs
4. Assess need for supplemental Oxygen
Documentation Parameters
1. Document course of events in detail
2. Document implementation of protocol and specific actions taken, medications administered
3. Residents response/disposition
Physician’s Signature _________________________________________ Date __________________