intravenous dhe and cost saving
TRANSCRIPT

Letters to the Editor
Emergency Department Treatment of Headache
Kusum L. Kumar, MD
Section of General Medicine VA Medical Center
Assistant Professor of Medicine
Oregon Health Sciences University
3710 Southwest US Veterans Hospital Road
Portland, OR 97207
I read, with great interest, the article "Evaluation and Treatment of Headache Patients in the Emergency Department: A Survey" by Dr. Christopher W.Barton.1 I agree with him that therapy of headache patients in the emergency department continues to depend on narcotics, in spite of availability of otherdrugs like sumatriptan, dihydroergotamine, and Toradol.(r)
I believe that the problem exists because most physicians did not have any formal training in diagnosis and management of headache during medicalschool education and residency training. Epidemiologic data has shown that moderate to severely disabling migraine alone affects 8.7 million women and2.6 million men in the U.S.2 In the National Ambulatory Care Medical Survey, headache was the eighth and the thirteenth most common problemencountered by family/general practitioners and internists, respectively.3 In spite of its prevalence, little attention is paid on this topic in medical school andduring residency. To improve the diagnostic and management skills of medical interns, a half-day headache clinic experience for 4 weeks was included inthe Ambulatory Care Block Rotation at the Oregon Health Sciences University Internal Medicine Residency Program, at the Portland Veterans AffairsMedical Center. Each intern completed a questionnaire before and after the rotation. The results showed a significant improvement in diagnostic skills anddecreased use of narcotics in the acute treatment of headache.
I strongly urge the medicine residency program directors to include teaching of headache management in their programs. Medical journals, mostly readby primary care and emergency room physicians, should include periodic reviews on various aspects of headache, especially when a new drug becomesavailable. I think these are the only ways to assure that physicians can make accurate diagnosis and not deprive these patients of specific non-addictivetherapies while preventing headache sufferers from becoming dependent on narcotics.
REFERENCES
1. Barton CW. Evaluation and treatment of headache patients in the emergency department: A survey. Headache. 1994; 34:91-94.
2. Stewart WF, Lipton RB, Celentano DD, Reed ML. Prevalence of migraine headache in the United States. Relation to age, income, race and othersociodemographic factors. JAMA. 1992;267:64-69.
3. Naien J, Frazier T, Altman I, DeLozier J. Ambulatory medical care: a comparison of internists and family-general practitioners. N Engl J Med.1980;302:11-16.
Intravenous DHE and Cost Saving
Lawrence Robbins, MD
Northbrook Court Professional Center
1535 Lake Cook Road, Suite 211
Northbrook, IL 60062
I have recently reviewed the costs attached to treating patients in my office for repetitive intravenous DHE, which I began doing in 19907 I have treatedover 1300 patients in the office with repetitive intravenous DHE and have withdrawn the narcotic, or butalbital, abusers as outpatients since that time.
After calculating the costs of inpatient versus outpatient, I estimate that, in my practice alone, since 1990, I have saved patients and their insurancecompanies $1.3 million. I feel that most of the rationale for inpatient headache treatment is not all that soundly based. My experience with theseend-of-the-line difficult patients is that they can be effectively treated as outpatients. I have worked on an inpatient headache unit and do recognize theadvantages that it can offer to certain patients.
I am writing this letter because I continue to see the values of the inpatient headache unit espoused in books, journals, and at meetings. I believe thatthis approach has hampered physicians in the United States from performing some of the protocols as outpatients when they probably should have beendoing so.
REFERENCES
1. Robbins L, Remmes A. Outpatient repetitive intravenous dihydroergotamine. Headache. 1992;32:455-458.
DHE and Post-concussion Syndrome
Howard Jacobs, MD
500-5255 Yonge Street
North York, Ont M2N 6P4 Canada
The recent article "Use of Dihydroergotamine in Patients With Post-Concussion Syndrome"1 was

of interest to me as further evidence of a central mechanism, possibly secondary to a peripheral nociception for the etiology of posttraumaticheadache. It is suggested by the authors that the post-concussion syndrome was overall affected by the use of dihydroergotamine. I think thepossible explanation for their findings regarding the other symptoms besides the headache are related to the natural progression of chronic painpatients when they have relief of their pain, It is generally accepted, and most of the studies show, that the greatest morbidity for people who sufferposttraumatic injury is related to their headaches and secondarily to their neck pain. It is probably the action of the dihydroergotamine on the H2receptor that inhibits the neurogenic inflammation that causes the head pain.
It is interesting to note that other medications were required to maintain the ongoing relief once the initial pain ceased. Their comment on litigationwas also of interest and is backed up by most studies of recent years, that litigation does not play an important part in the ongoing problem.
This article therefore serves as an important study to add to the impressive data that is already available to back up this point. Unfortunately, itdoes not mention whether these patients that were studied had any neck injury or whether any neck pathology was found on examination. It would beinteresting to review these patients and to examine x-rays, and to do diagnostic blocks for positive facet inflammation findings.
Newer medications such as sumatriptan may offer additional avenues of relief for these patients, We did a study which was published inHeadache in 1993.2 This study also showed that sumatriptan was efficacious in abolishing the vascular component of the daily headache whichagain suggests a central mechanism for posttraumatic headache.
REFERENCES
1. McBeath JG, Nanda A. Use of dihydroergotamine in patients with post-concussion syndrome. Headache. 1994; 34:148-151.
2. Gawel MJ, Rothbart P, Jacobs H. Subcutaneous sumatriptan in the treatment of acute episodes of post-traumatic headache. Headache.1993;33:96-97.
Hemodynamic Changes in Cluster Headache
Arthur A. Gage, DDS
12688 Tucano Circle
Boca Raton, FL 33428
Bjorne et al1 refer to hemodynamic changes in extracranial vascular beds and to cluster headache attacks in "susceptible individuals."
In 1988, I presented2 an hypothesis that just might provide a clue for discovering who the susceptible individuals might be. The hypothesis wasnot meant to be a simplistic explanation neglecting the many respected neural-related hypotheses, but rather as a direction sign for future productiveinvestigations. The internal maxillary artery's (IMA) relationships with the two heads of the lateral pterygoid muscle (LPM) usually present one of twoanatomic patterns, possibly genetically related. Reference to the reported familial predisposition of certain individuals to migrainous phenomena mightbe explained by this hypothesis. Those in which the IMA passes between the two heads of the LPM bear a vulnerability to vascular entrapment withaccompanying hemodynamic changes affecting the IMA's branches. Two of the IMA's many branches are the important middle meningeal andaccessory meningeal arteries, main suppliers of the dura, contributor to the ophthalmic artery, and supplier of the semilunar ganglion.3,4Unfortunately, ease of accessibility has caused the temporal artery to be the attention-getter rather than the IMA, the IMA being more difficult tostudy, but probably more important than the temporal artery. Advanced noninvasive vascular visualization techniques should be directed at the veryimportant IMA and its possible role in headache and head pain caused by hemodynamic changes in its branches.
REFERENCES
1. Bjorne A, Hinfelt B, Havelius U. Recurrence of cluster headache after carotid thromboendarterectomy. Headache. 1994;34:230-233.
2. Gage A. Hypothesis: Stress induced vascular entrapment and migraine. Headache. 1988;28:267-268.
3. Gray H; Lewis WH, ed. Anatomy of the Human Body. 24th ed. Philadelphia, Pa: Lea & Febiger; 1944:562-563.
4. Sicher; DuBrul EL, ed. Sicher's Oral Anatomy. 7th ed. St. Louis, Mo: The CV Mosby Co; 1980:362-364.
Verapamil and Cluster Headache
Teresa Catarci, MD
Dipartimento di Neuroscienze
Universita' La Sapienza
00185 - Rome, Italy
Timothy J. Steiner, BSc, PhD, MB, BS, LLM
The Princess Margaret Migraine Clinic
Charing Cross Hospital
London W6 8RF, UK
Verapamil was first reported to be effective in migraine prophylaxis in a preliminary communication in 1983.1 Since then, many studies haveshown good results, not only in migraine,2,3,4 but also in cluster headache.3,5,6 Dosages employed range between 160 and 480 rag/day, Inparticular, Gabai and Spierings6 reported relief after an average of 1.7 weeks in episodic cluster headache patients on a mean dose of 354 rag/day(240 to 600 mg), and after 5 weeks in chronic cluster headache patients on 572 rag/day (120 to 1200 rag). In all cases, treatment was started with120 mg b.i.d.

We wonder whether a higher initial dose and a different prescription regimen might be a more effective therapy. One of our chronic clusterheadache patients, who was no longer responding to any treatment except prednisolone, was advised to take one 80 mg tablet of verapamil threetimes a day. He did not return for follow-up until 4 months later, when he reported that his headaches disappeared 2 days after starting the prescribedmedication and did not recur. He also said that he was taking the three tablets at night, as he used to do when taking lithium. He had no side effectsand his ECG was normal. Verapamil was discontinued and the patient remains headache-free.
There are no reports of the oral administration of 240 mg instant-release verapamil as a single daily dose. The reported side effects of verapamilsustained-release tablets are mainly constipation, dizziness, headache, and peripheral edema.7,8
The postulated mechanism of action of verapamil in cluster headache is to restore a normal inhibitory tone to the pain-modulating pathways fromthe trigeminovascular system.5 Perhaps this can be better achieved with a higher initial dose of verapamil, such as our patient took by mistake.
REFERENCES
1. Solomon GD, Steel JG, Spaccavento LJ. Verapamil pro-phylaxis of migraine: a double blind placebo controlled study. JAMA.1983;250:2500-2502.
2. Markley H, Cheronis J, Pierpho R. Verapamil prophylactic therapy of migraine. Neurology. 1984;34:973-976.
3. Jonsdottir M, Meyer J, Rodgers R. Efficacy, side effects and tolerances compared during headache treatment with three different calciumblockers. Headache. 1987;27:364-369.
4. Prusinski A, Kozubski W. Use of verapamil in the treatment of migraine. Wiad Lek. 1987;40:734-738.
5. Bussone G, Leone M, Peccarisi C, et al. Double blind comparison of lithium and verapamil in cluster headache prophylaxis. Headache.1990;30:411-417.
6. Gabai IJ, Spierings ELH. Prophylactic treatment of cluster headache with verapamil. Headache. 1989;29:187-168.
7. Speders S, Sosna-Heidelberg J, Schumacher A, et al. Efficacy and safety of Isoptin SR 240 mg in essential hypertension - results of a phaseIV study under practice conditions. Hochdrick. 1988;8:25-30.
8. EVEREST'H trial. Multicentre trial of the antihypertensive efficacy and safety of Isoptin SR. Acta Med Int. 1990;2:3-7.
Analgesic Rebound Headaches
Lawrence Robbins, MD
Northbrook Court Professional Center
1535 Lake Cook Road, Suite 211
Northbrook, IL 60062
The rebound headache situation from analgesics is a very real phenomenon.1 However, there have been a number of problems associated withthis backlash that we have seen against analgesics.
I have patients coming to see me who have been refused even five butalbital pills a month by their internists because the internists stated thatthey were told that these medications are bad and should be avoided. Certain patients are being pushed into more expensive and difficult therapies,such as sumatriptan injections, when a number of them would do well with an occasional analgesic oral preparation.
There are a number of patients who, for whatever reason, do well on a very small amount of a daily analgesic, whether it is an aspirin and caffeinemedication, or a butalbital medication, and they limit the amounts. However, they now have physicians advising them that two of these pills per day is"bad" and that they need to get off of even small amounts of daily analgesics. When we look at the side effects of a number of our daily preventives,particularly the beta blockers and antidepressants, versus the side effects of one or two analgesic pills per day, it is not rational to insist that everypatient stop using these analgesics.
Until we have sorted out who gets rebound headaches from which medication and at what dose, I feel that we should swing the pendulum back tosome degree and allow judicious use of analgesics in selected patients. The problem that I see has been that the general medical community hasmisinterpreted our articles and lectures about the dangers of analgesic rebound headache and now is very reluctant to use these medications at all.
REFERENCE
1. Mathew N. Drug induced headache. In: Neurologic Clinics VIII. Philadelphia: WB Saunders Co; 1990;903-912.
Headache Formulary for Managed Care Organizations
Randal Von Seggern, Pharm D
Adelman Headache Center
510 N. Elam Ave, Suite 302
Greensboro, NC 27403
Dr. Klapper1 is quite correct in his call for an established formulary that allows for comprehensive pharmacologic options for the clinician, whilemeeting the cost containment needs of the managed care organizations5 (MCOs).
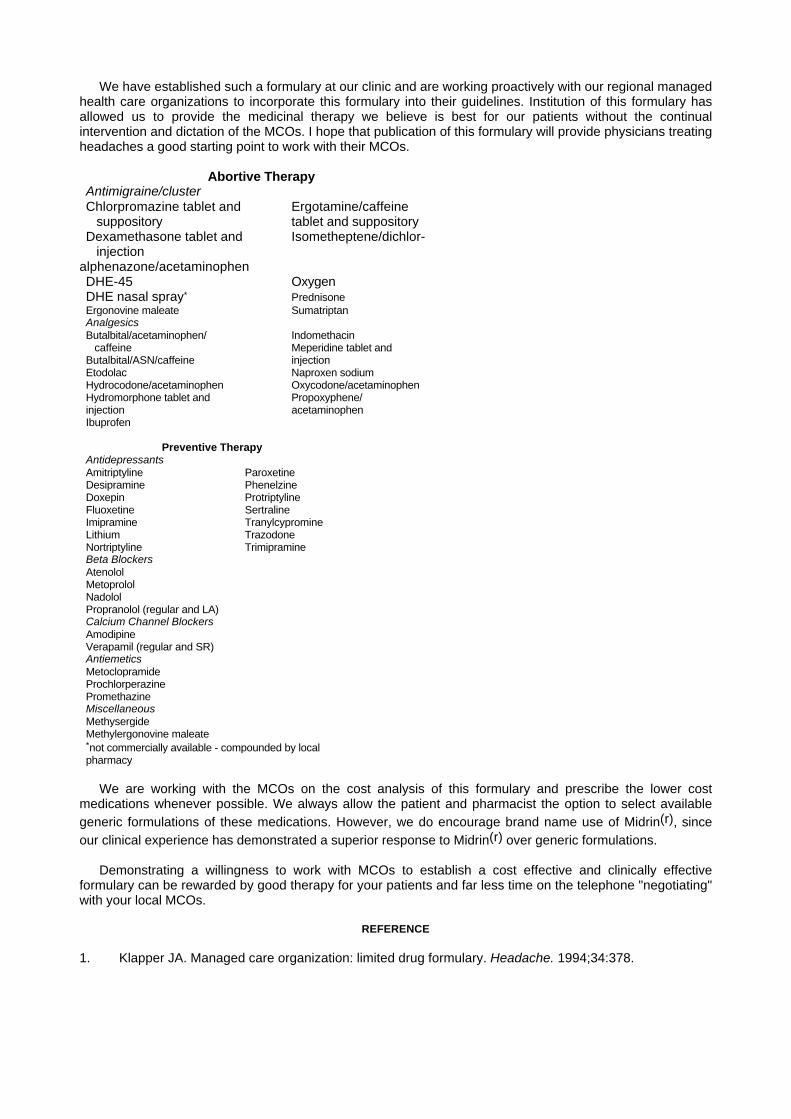
We have established such a formulary at our clinic and are working proactively with our regional managedhealth care organizations to incorporate this formulary into their guidelines. Institution of this formulary hasallowed us to provide the medicinal therapy we believe is best for our patients without the continualintervention and dictation of the MCOs. I hope that publication of this formulary will provide physicians treatingheadaches a good starting point to work with their MCOs.
Abortive TherapyAntimigraine/clusterChlorpromazine tablet and Ergotamine/caffeine suppository tablet and suppositoryDexamethasone tablet and Isometheptene/dichlor- injection
alphenazone/acetaminophenDHE-45 OxygenDHE nasal spray* PrednisoneErgonovine maleate SumatriptanAnalgesicsButalbital/acetaminophen/ Indomethacin caffeine Meperidine tablet andButalbital/ASN/caffeine injectionEtodolac Naproxen sodiumHydrocodone/acetaminophen Oxycodone/acetaminophenHydromorphone tablet and Propoxyphene/injection acetaminophenIbuprofen
Preventive TherapyAntidepressantsAmitriptyline ParoxetineDesipramine PhenelzineDoxepin ProtriptylineFluoxetine SertralineImipramine TranylcypromineLithium TrazodoneNortriptyline TrimipramineBeta BlockersAtenololMetoprololNadololPropranolol (regular and LA)Calcium Channel BlockersAmodipineVerapamil (regular and SR)AntiemeticsMetoclopramideProchlorperazinePromethazineMiscellaneousMethysergideMethylergonovine maleate*not commercially available - compounded by localpharmacy
We are working with the MCOs on the cost analysis of this formulary and prescribe the lower costmedications whenever possible. We always allow the patient and pharmacist the option to select availablegeneric formulations of these medications. However, we do encourage brand name use of Midrin(r), sinceour clinical experience has demonstrated a superior response to Midrin(r) over generic formulations.
Demonstrating a willingness to work with MCOs to establish a cost effective and clinically effectiveformulary can be rewarded by good therapy for your patients and far less time on the telephone "negotiating"with your local MCOs.
REFERENCE
1. Klapper JA. Managed care organization: limited drug formulary. Headache. 1994;34:378.