intradialytic hypertension (idh) hta intradialytique · intradialytic hypertension (idh) hta...
TRANSCRIPT
Intradialytic Hypertension (IDH)
HTA intradialytique
Malik Touam
23-24 avril 2012
Malik Touam
AURA & Hôpital Necker Paris
HID
• Definition• Prevalence• Clinical Characteristics• Prognostic significance
Intradialytic Hypertension
• Prognostic significance• Pathophysiologic Mechanisms• Treatment
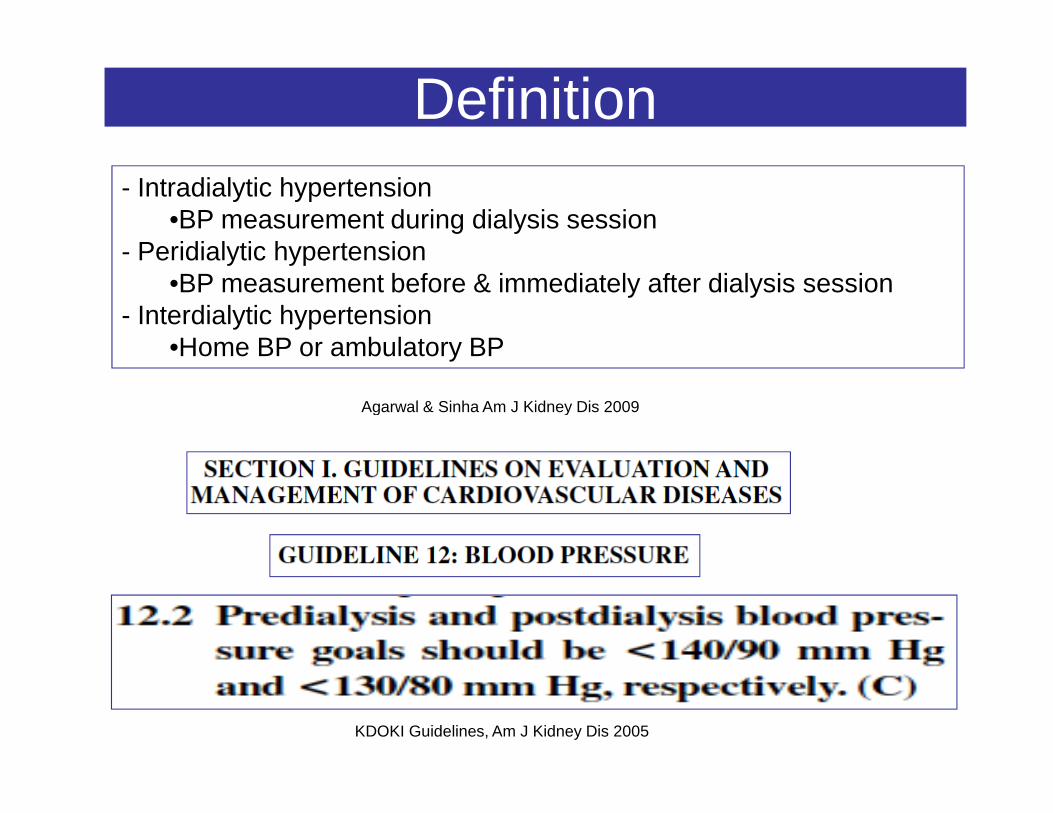
Definition - Intradialytic hypertension
•BP measurement during dialysis session- Peridialytic hypertension
•BP measurement before & immediately after dialysis session- Interdialytic hypertension
•Home BP or ambulatory BP
Agarwal & Sinha Am J Kidney Dis 2009
KDOKI Guidelines, Am J Kidney Dis 2005
Agarwal & Sinha Am J Kidney Dis 2009
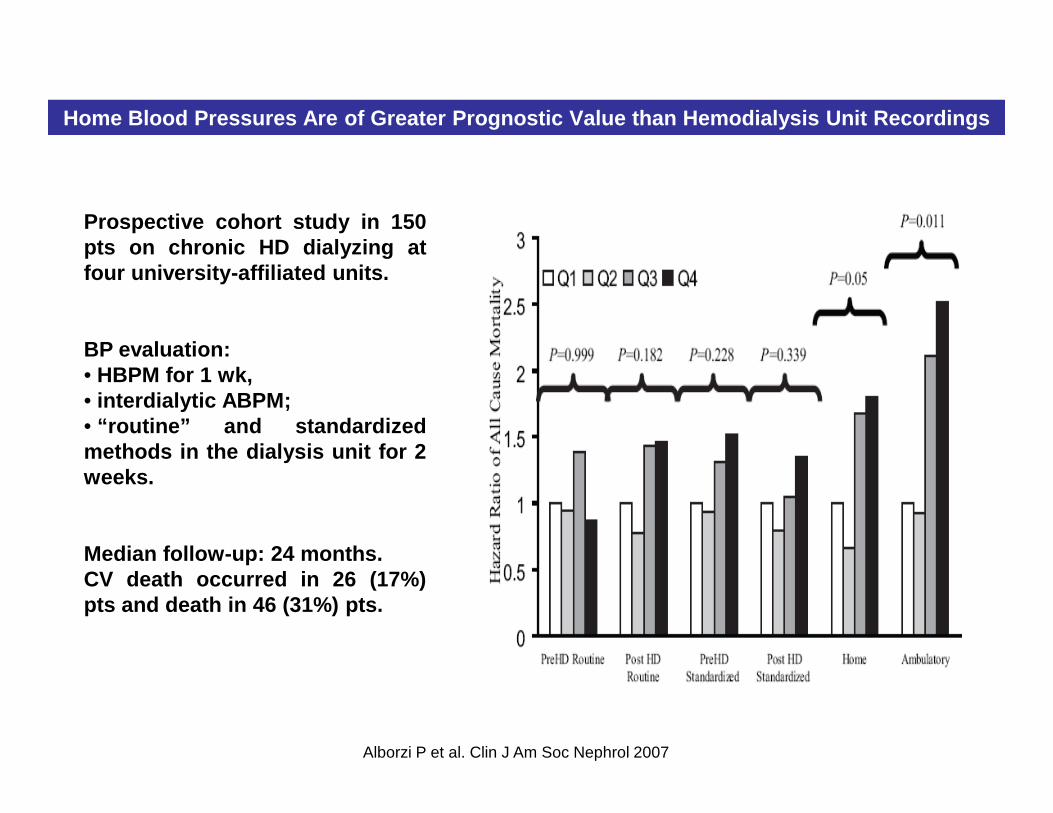
Home Blood Pressures Are of Greater Prognostic Valu e than Hemodialysis Unit Recordings
Prospective cohort study in 150pts on chronic HD dialyzing atfour university-affiliated units.
BP evaluation:• HBPM for 1 wk,• interdialytic ABPM;• interdialytic ABPM;• “routine” and standardizedmethods in the dialysis unit for 2weeks.
Median follow-up: 24 months.CV death occurred in 26 (17%)pts and death in 46 (31%) pts.
Alborzi P et al. Clin J Am Soc Nephrol 2007
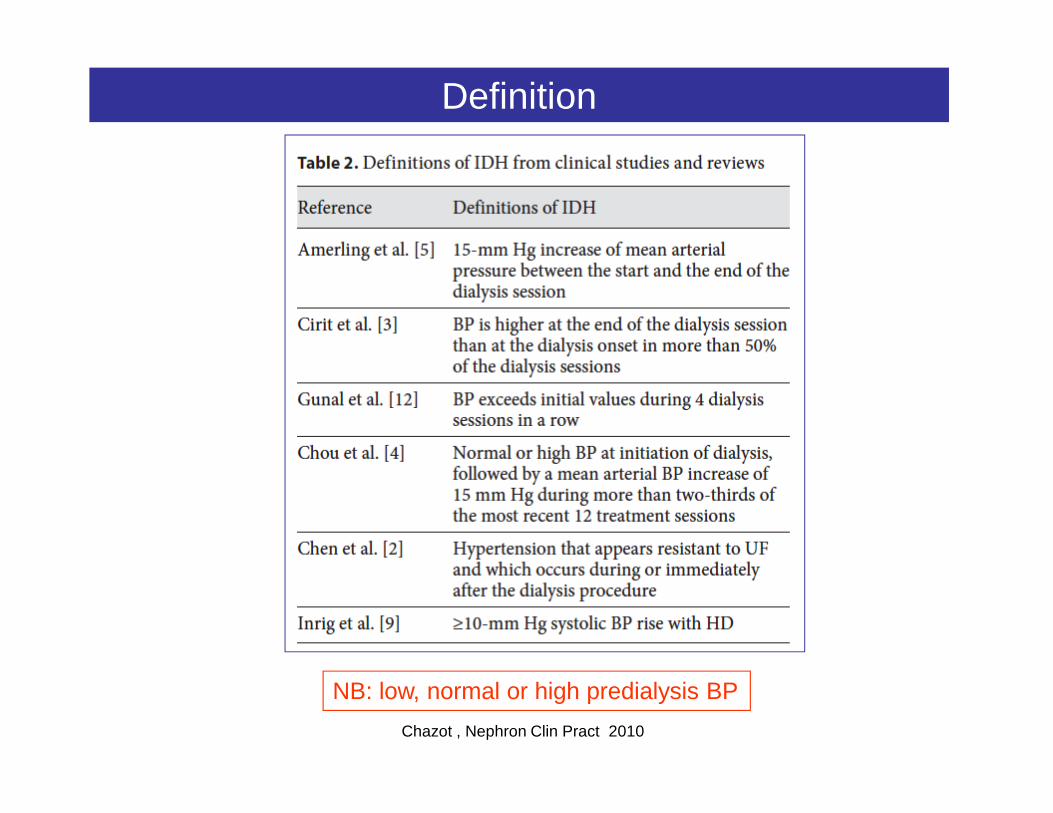
Definition
Chazot , Nephron Clin Pract 2010
NB: low, normal or high predialysis BP
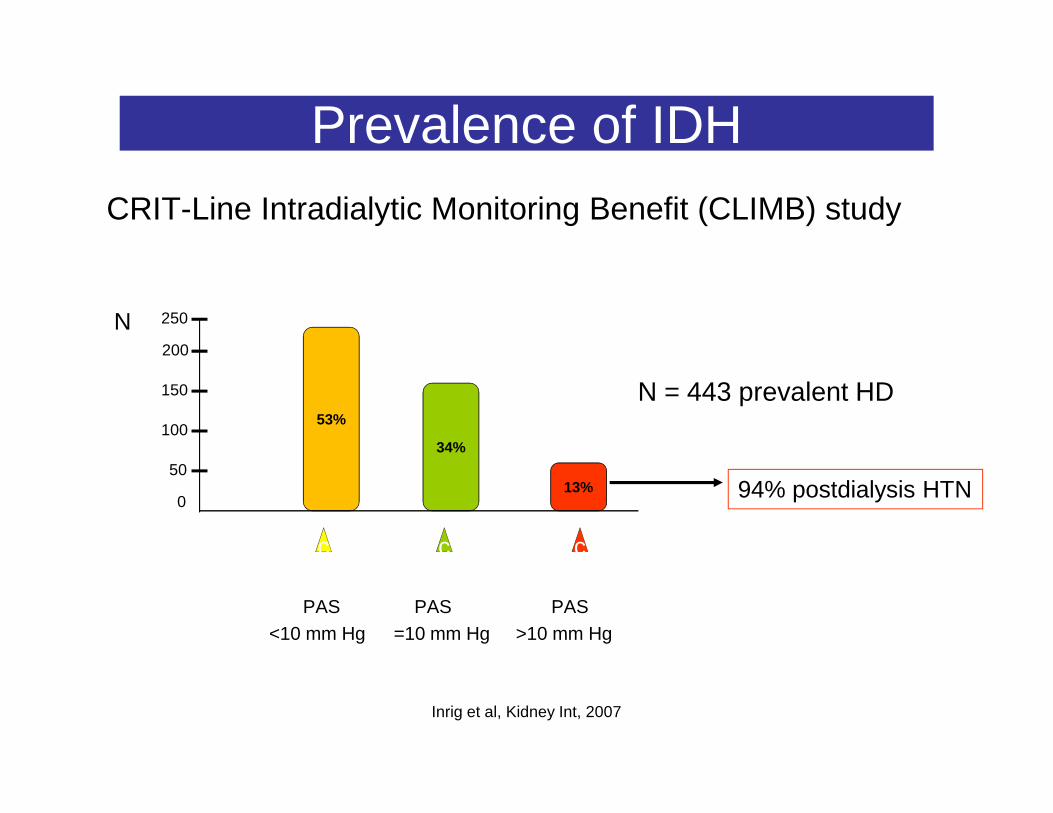
Prevalence of IDHCRIT-Line Intradialytic Monitoring Benefit (CLIMB) study
N = 443 prevalent HD150
200
250N
PAS PAS PAS<10 mm Hg =10 mm Hg >10 mm Hg
Inrig et al, Kidney Int, 2007
53%
34%
13%0
50
100
c c c
94% postdialysis HTN
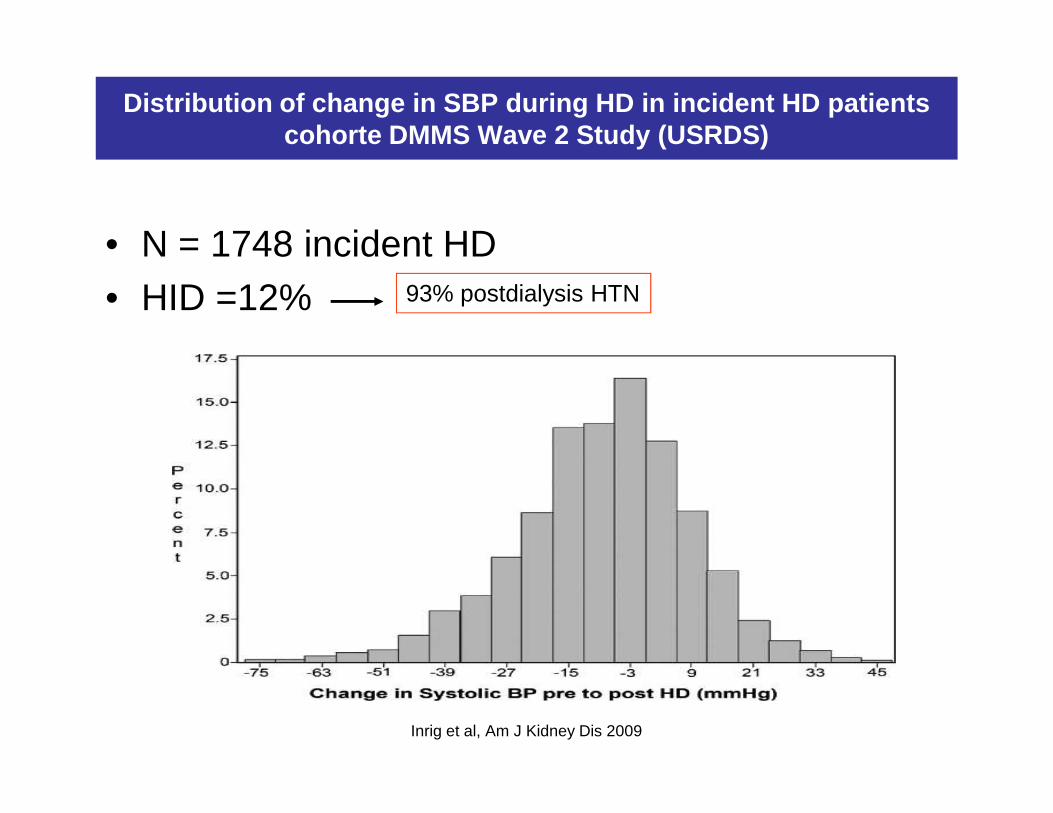
Distribution of change in SBP during HD in incident HD patients cohorte DMMS Wave 2 Study (USRDS)
• N = 1748 incident HD • HID =12% 93% postdialysis HTN
Inrig et al, Am J Kidney Dis 2009

Clinical Characteristics
DMMS Wave 2 Study- SBP >10 mm Hg (N = 744)- Unchanged SBP (N = 791)- SBP >10 mm Hg (N = 213)
• Older patients• Lower BMI, dry weight and interdialytic weight gain• Lower serum creatinine and serum albumin levels• More predialysis HTN • More antihypertensive medications
Inrig et al Am J Kidney Dis 2009
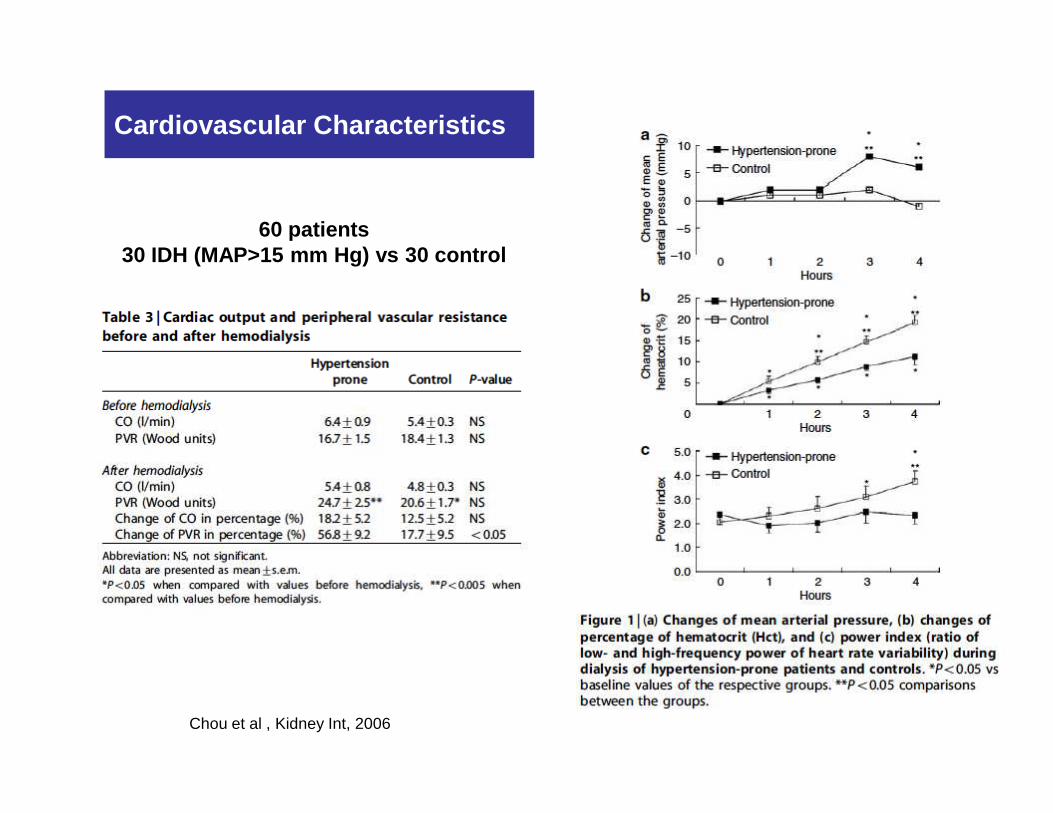
Cardiovascular Characteristics
60 patients30 IDH (MAP>15 mm Hg) vs 30 control
Chou et al , Kidney Int, 2006

Prognostic
N = 5433
Zager et al Kidney Int 1998
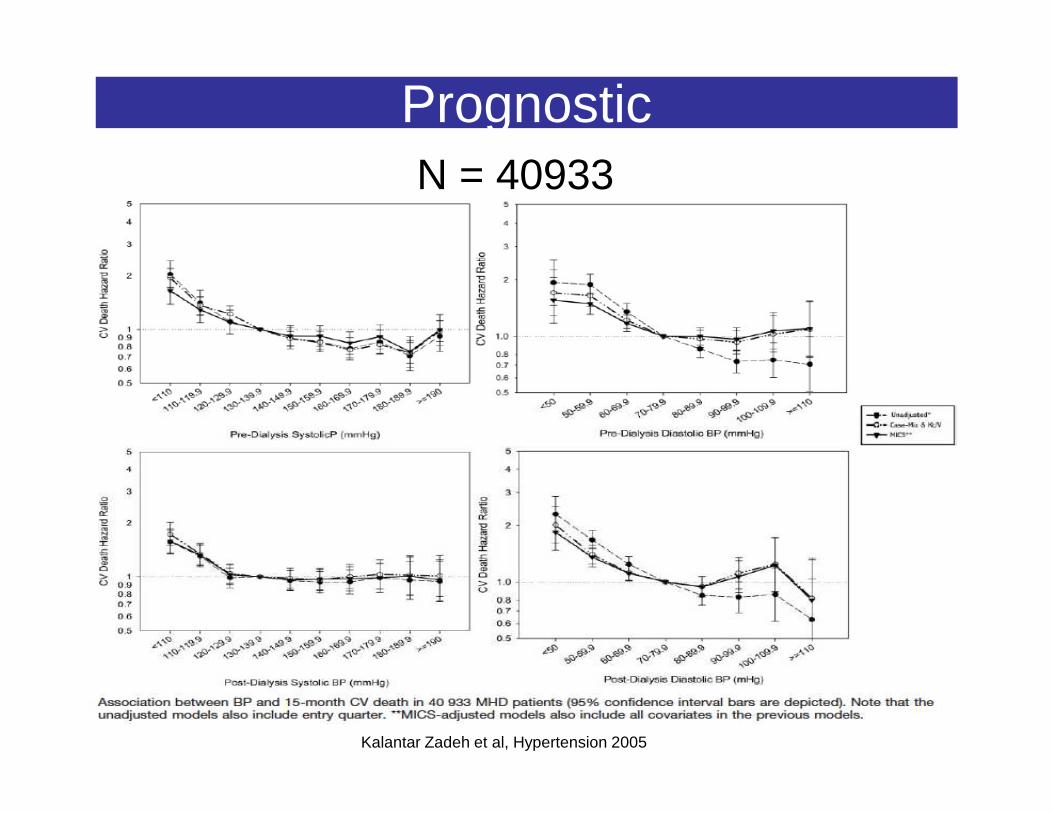
Prognostic N = 40933
Kalantar Zadeh et al, Hypertension 2005
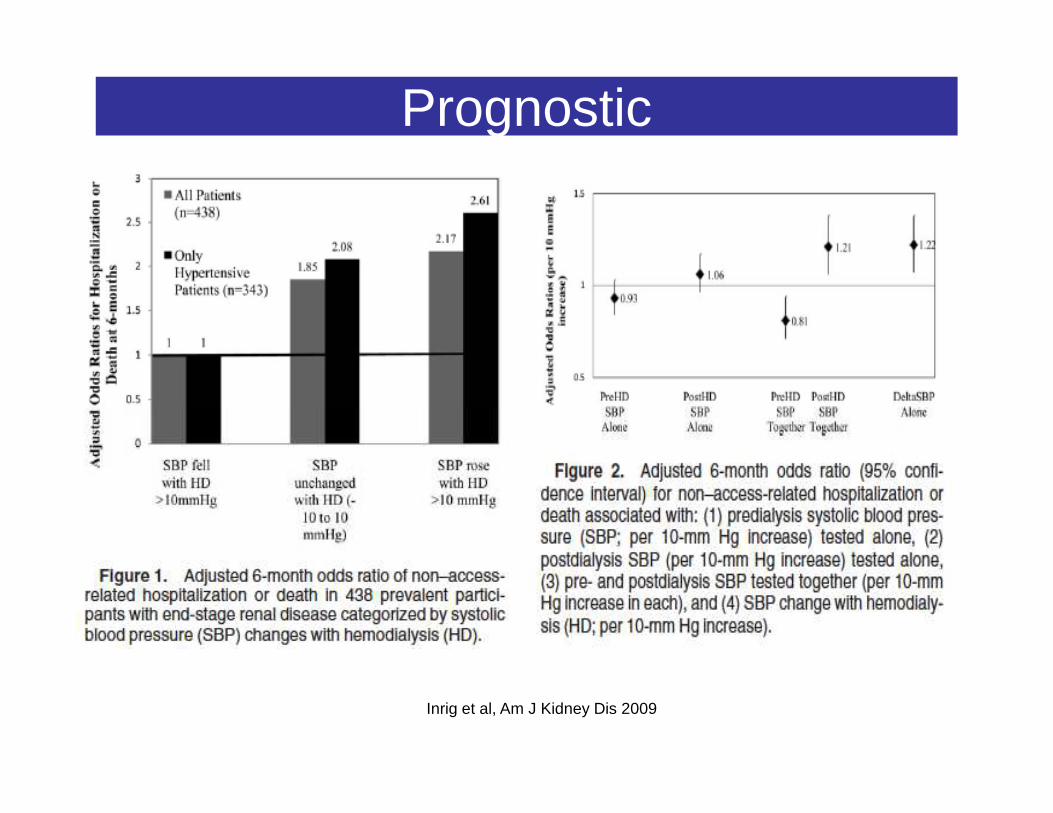
Prognostic
Inrig et al, Am J Kidney Dis 2009
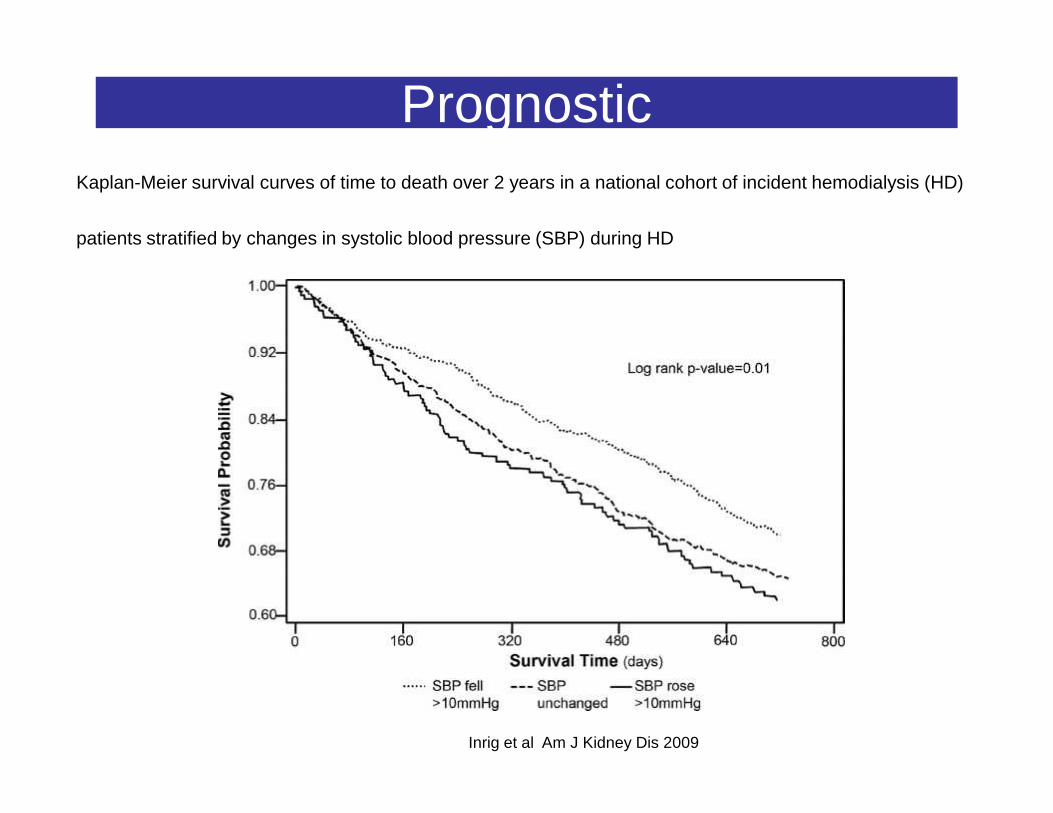
Prognostic Kaplan-Meier survival curves of time to death over 2 years in a national cohort of incident hemodialysis (HD)
patients stratified by changes in systolic blood pressure (SBP) during HD
Inrig et al Am J Kidney Dis 2009
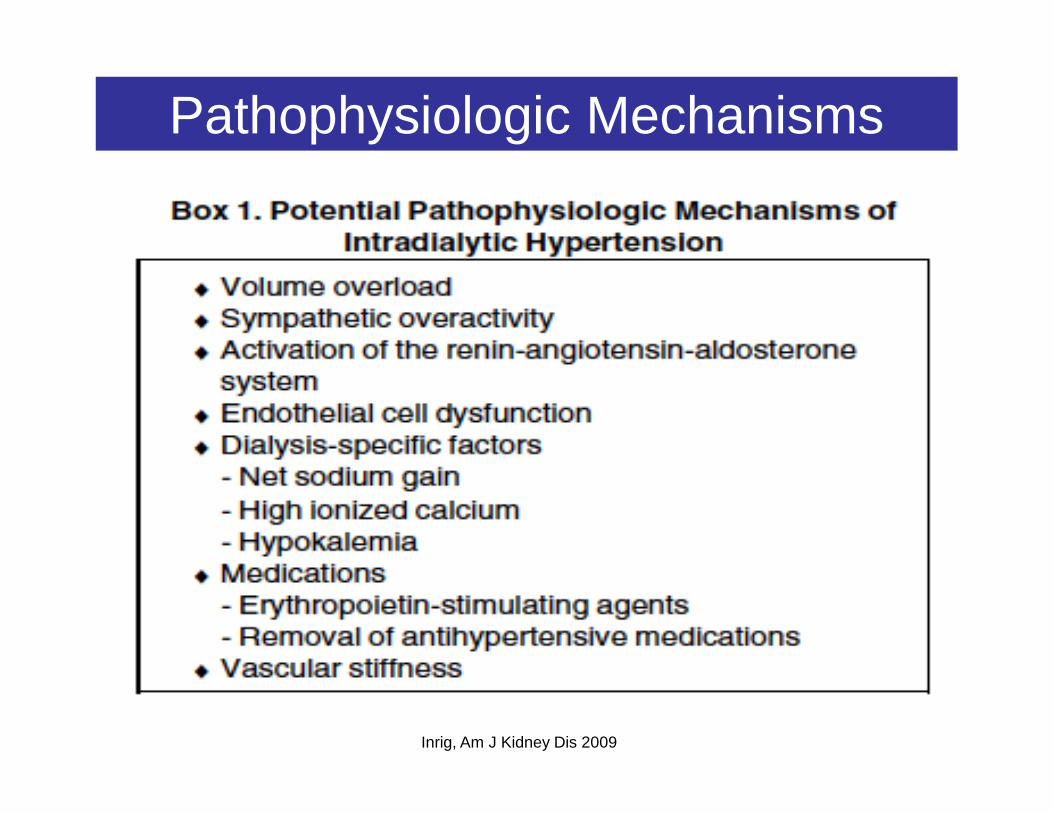
Pathophysiologic Mechanisms
Inrig, Am J Kidney Dis 2009

Volume Overload
6 HD patients
Gunal, J Nephrol 2002
Volume Overload
9 HD patients with postdialysis HTN BPS: 172 204 mm HgPedal edema: only 3 patientsReduction of dry weight (mean -6,7 kg)Reduction of dry weight (mean -6,7 kg)
Reduction of antihypertensive medicationsNormalization of BP
Cirit et al, Nephrol Dial Transplant 1995

The effect of dry-weight reduction on interdialytic ambulatory systolic (A) and diastolic BP (B) in hypertensive hemodialysis patients
DRIP studyPrevalent HD
Agarwal et al, Hypertension 2009
Prevalent HD
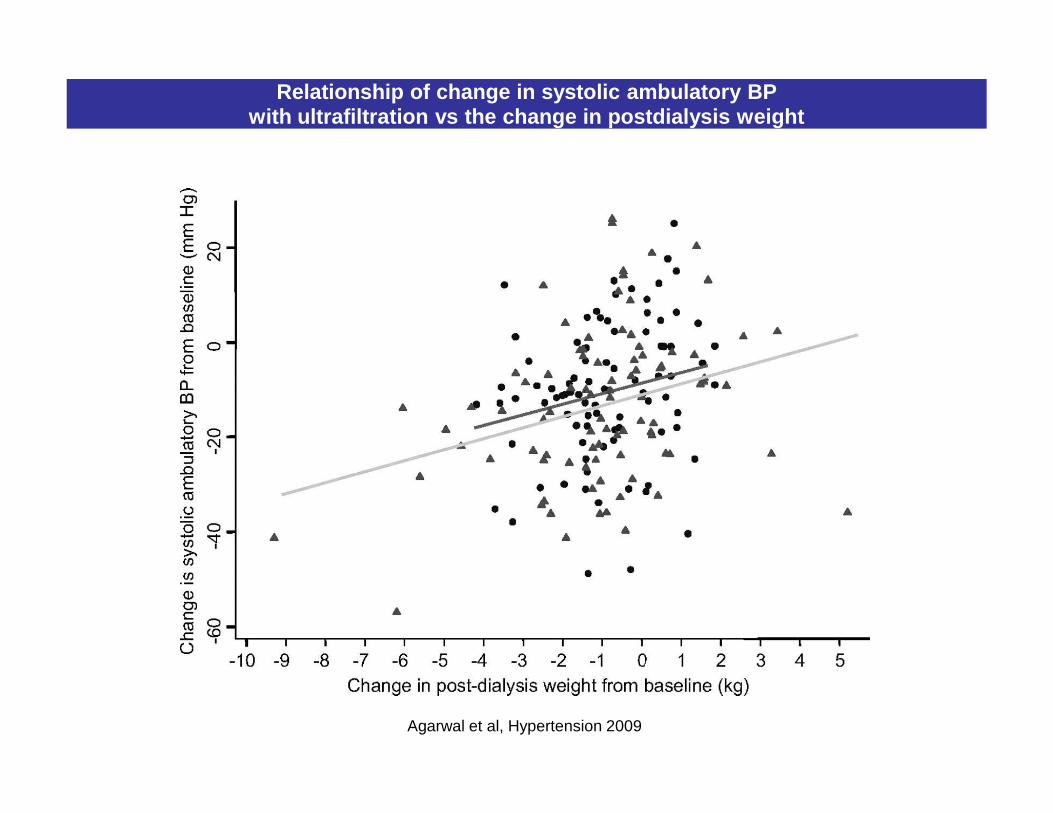
Relationship of change in systolic ambulatory BP with ultrafiltration vs the change in postdialysis weight
Agarwal et al, Hypertension 2009
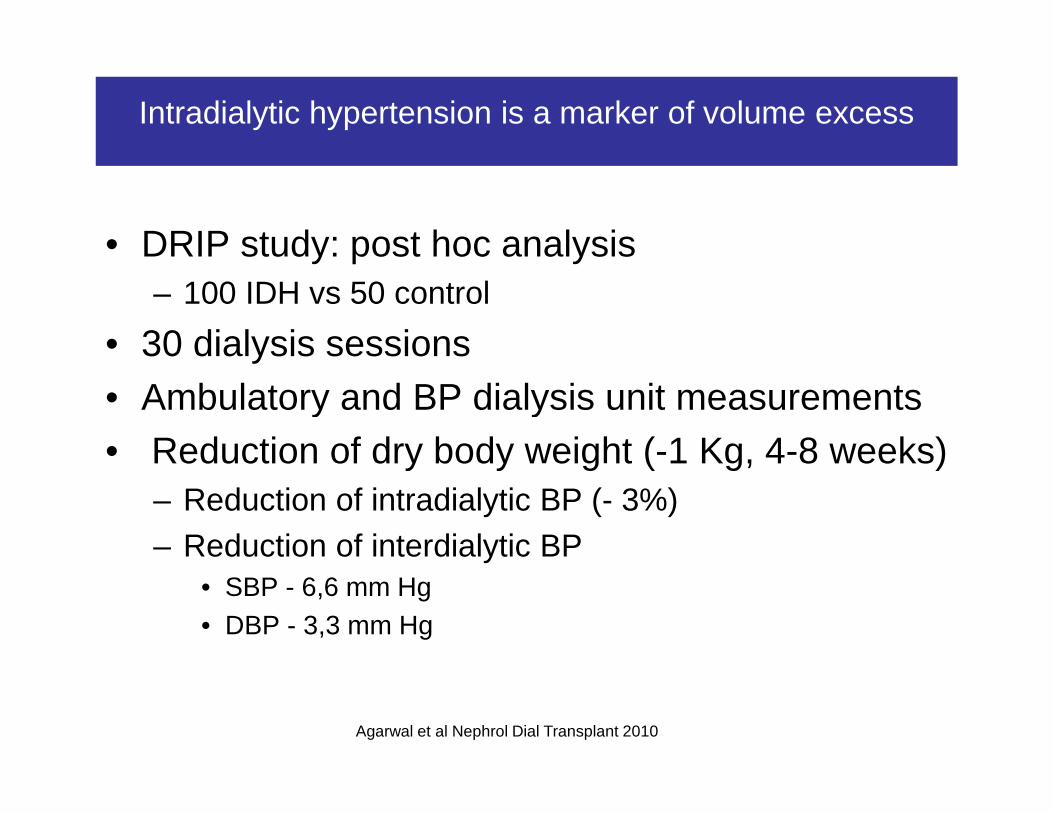
Intradialytic hypertension is a marker of volume excess
• DRIP study: post hoc analysis– 100 IDH vs 50 control
• 30 dialysis sessions• Ambulatory and BP dialysis unit measurements• Ambulatory and BP dialysis unit measurements• Reduction of dry body weight (-1 Kg, 4-8 weeks)
– Reduction of intradialytic BP (- 3%)– Reduction of interdialytic BP
• SBP - 6,6 mm Hg• DBP - 3,3 mm Hg
Agarwal et al Nephrol Dial Transplant 2010

Dialysis Specific factorsSodium
Song et al J Am Soc Nephrol 2005
Sodium
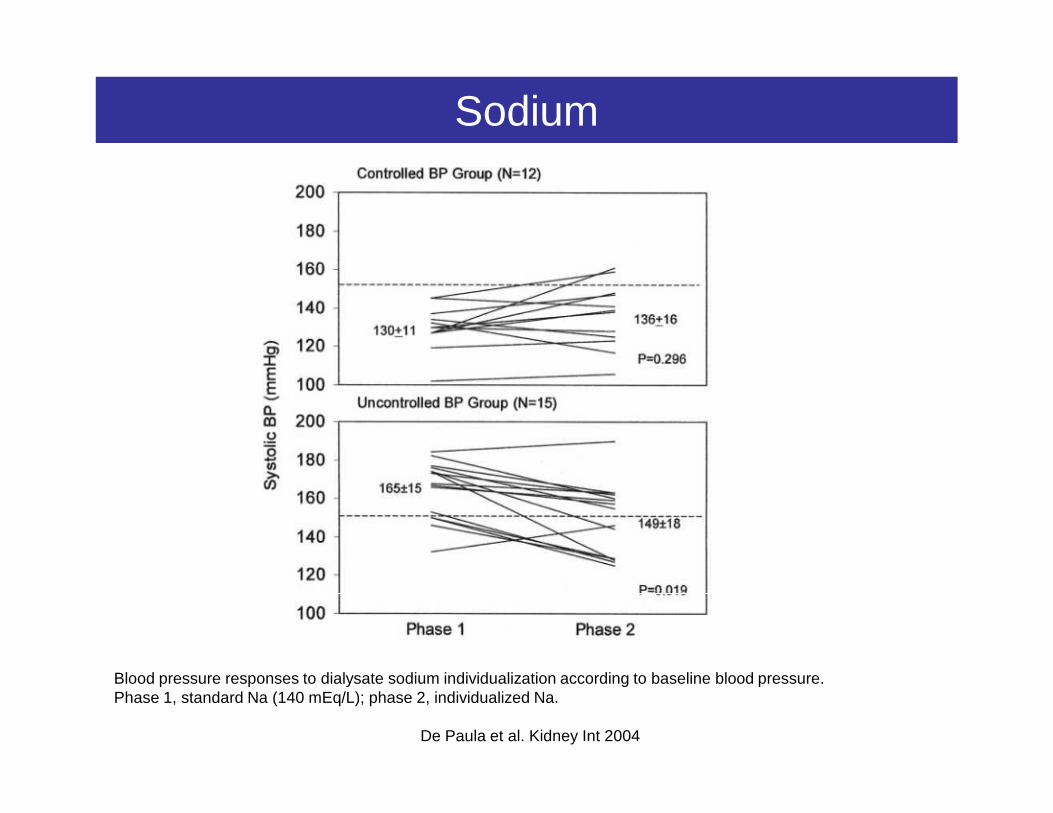
Blood pressure responses to dialysate sodium individualization according to baseline blood pressure. Phase 1, standard Na (140 mEq/L); phase 2, individualized Na.
De Paula et al. Kidney Int 2004
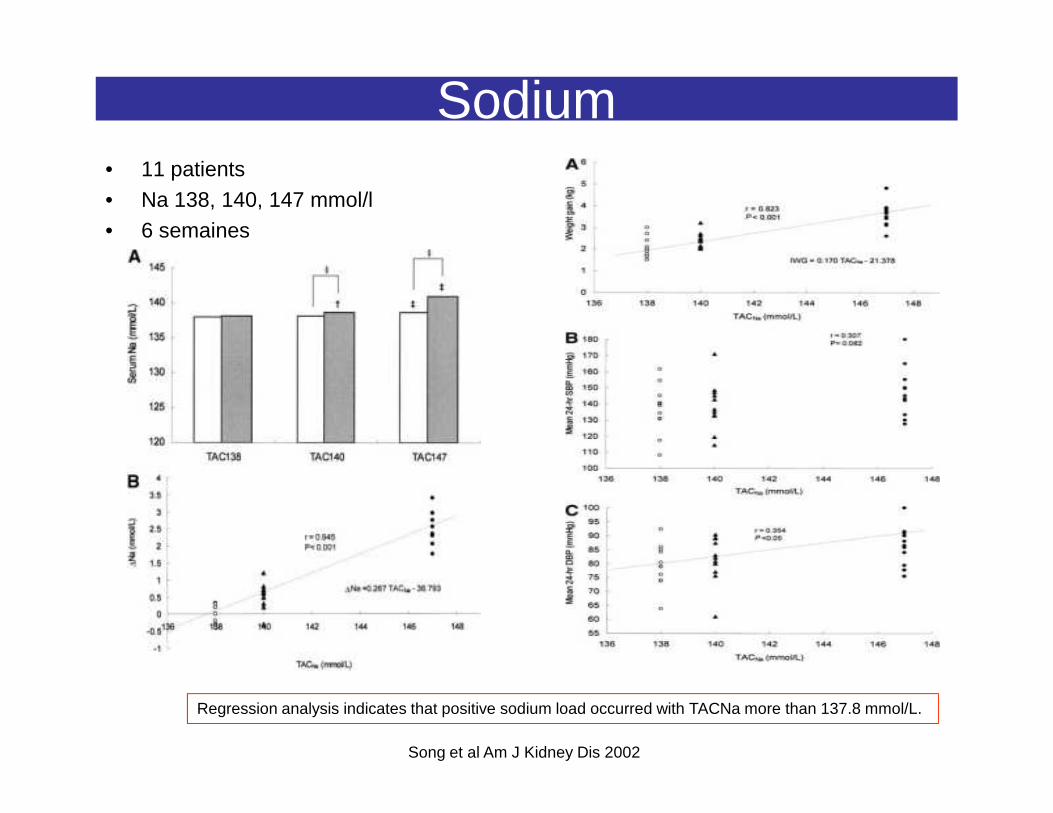
Sodium • 11 patients• Na 138, 140, 147 mmol/l• 6 semaines
Song et al Am J Kidney Dis 2002
Regression analysis indicates that positive sodium load occurred with TACNa more than 137.8 mmol/L.

• Hypokaliemia: direct vasoconstrictor effect• Acute increase Ca++: increases myocardial contractility and cardiac output
Potassium – Calcium
Chou et al Kidney int 2006
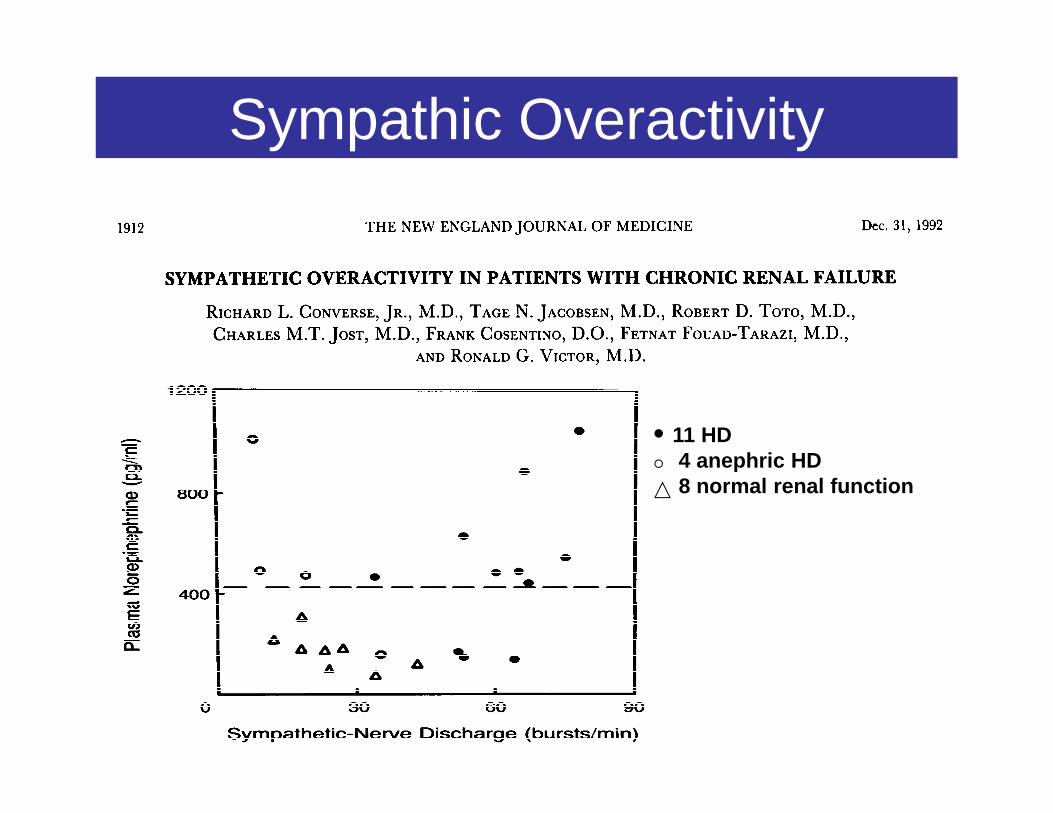
Sympathic Overactivity
11 HD4 anephric HD8 normal renal function
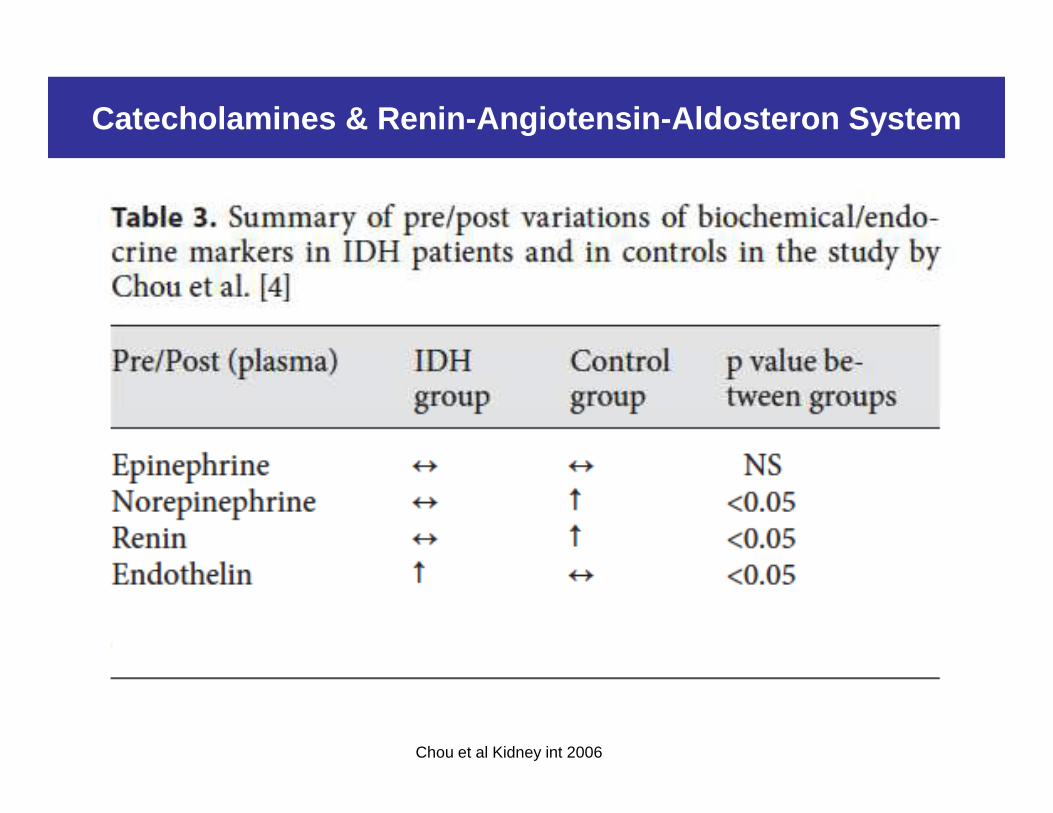
Catecholamines & Renin-Angiotensin-Aldosteron Syste m
Chou et al Kidney int 2006
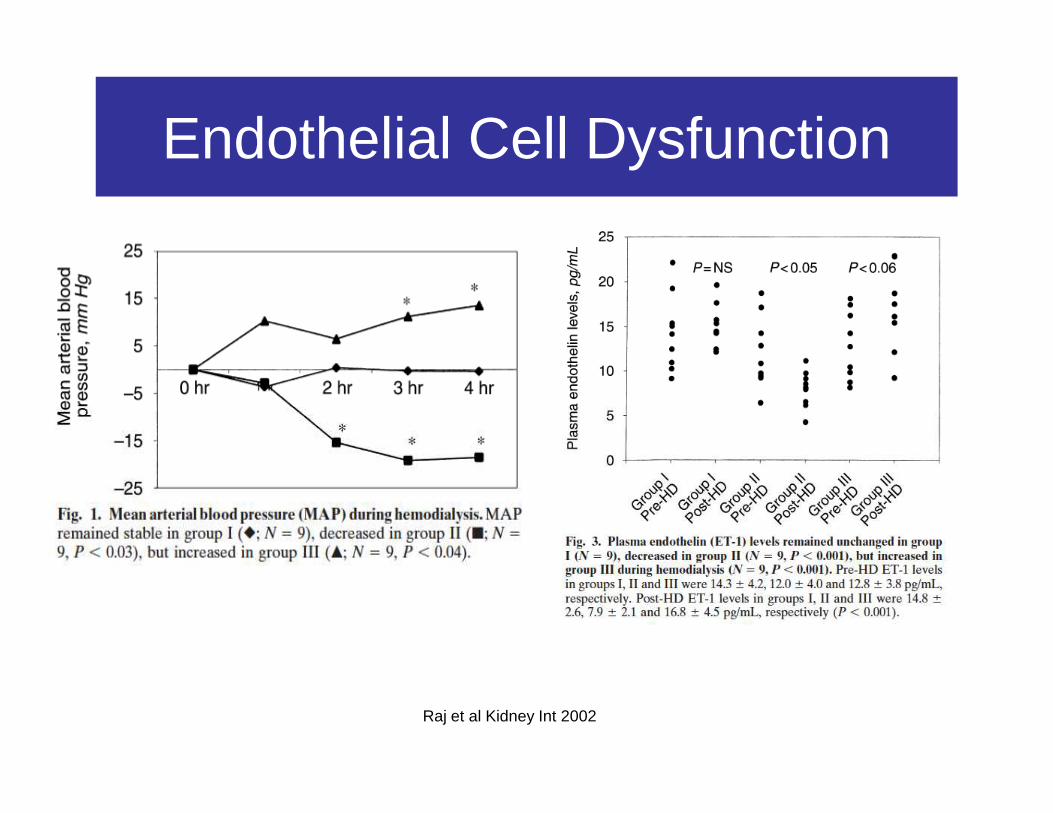
Endothelial Cell Dysfunction
Raj et al Kidney Int 2002
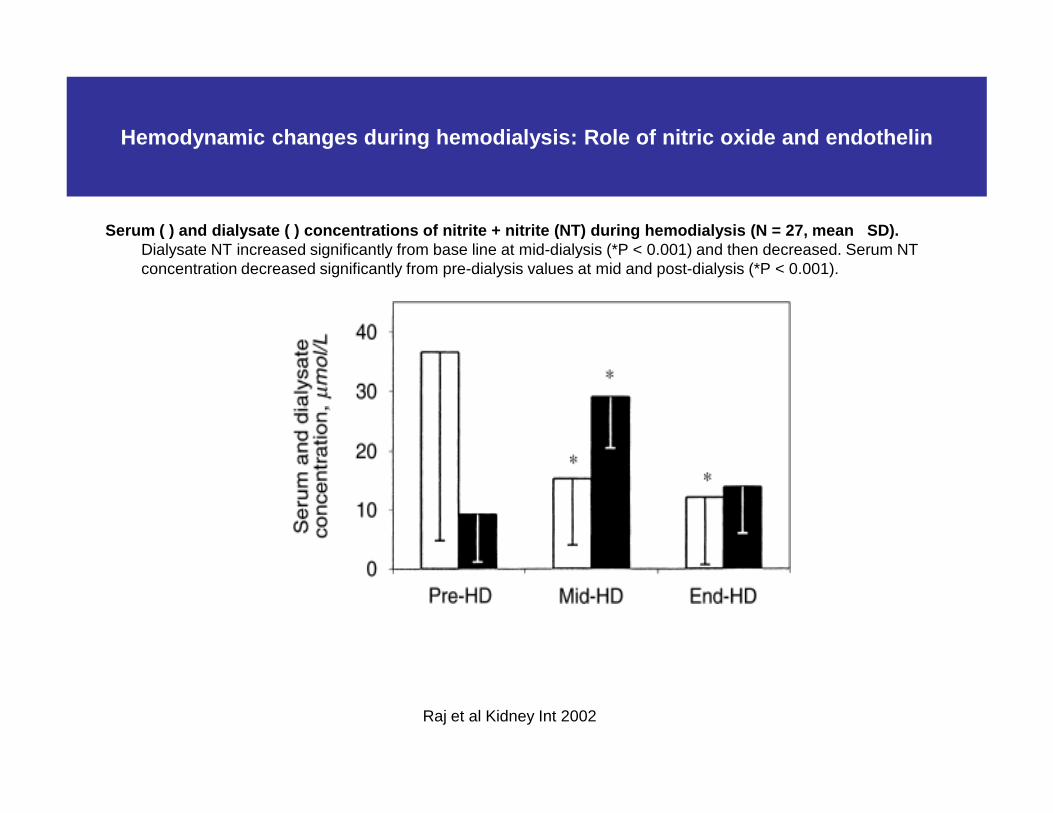
Serum ( ) and dialysate ( ) concentrations of nitri te + nitrite (NT) during hemodialysis ( N = 27, mean SD).Dialysate NT increased significantly from base line at mid-dialysis (*P < 0.001) and then decreased. Serum NT concentration decreased significantly from pre-dialysis values at mid and post-dialysis (*P < 0.001).
Hemodynamic changes during hemodialysis: Role of ni tric oxide and endothelin
Raj et al Kidney Int 2002
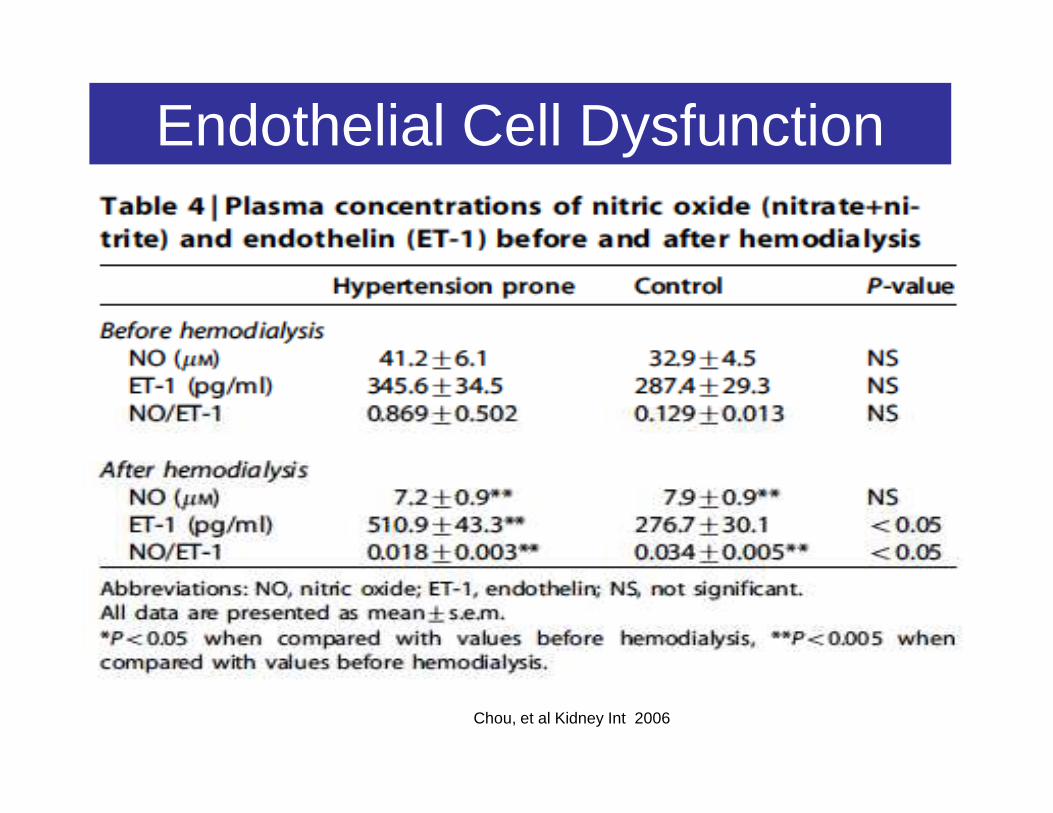
Endothelial Cell Dysfunction
Chou, et al Kidney Int 2006
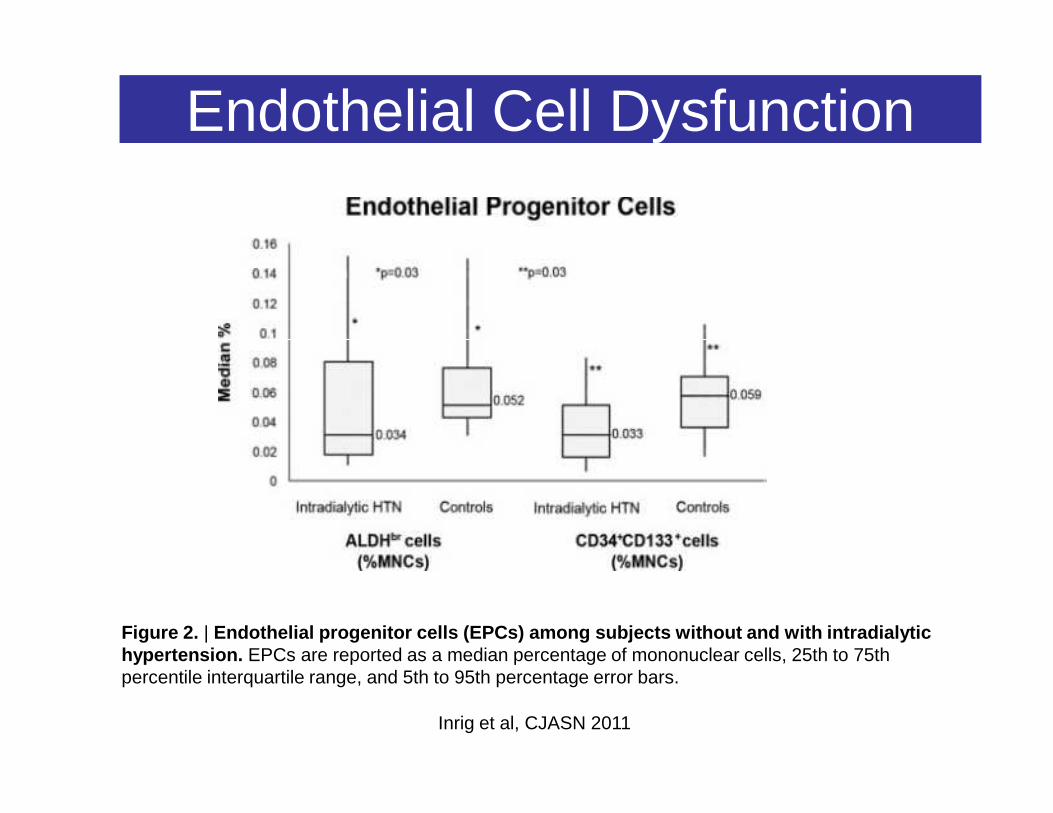
Endothelial Cell Dysfunction
Figure 2. | Endothelial progenitor cells (EPCs) among subjects without and with intradialytic hypertension. EPCs are reported as a median percentage of mononuclear cells, 25th to 75th percentile interquartile range, and 5th to 95th percentage error bars.
Inrig et al, CJASN 2011
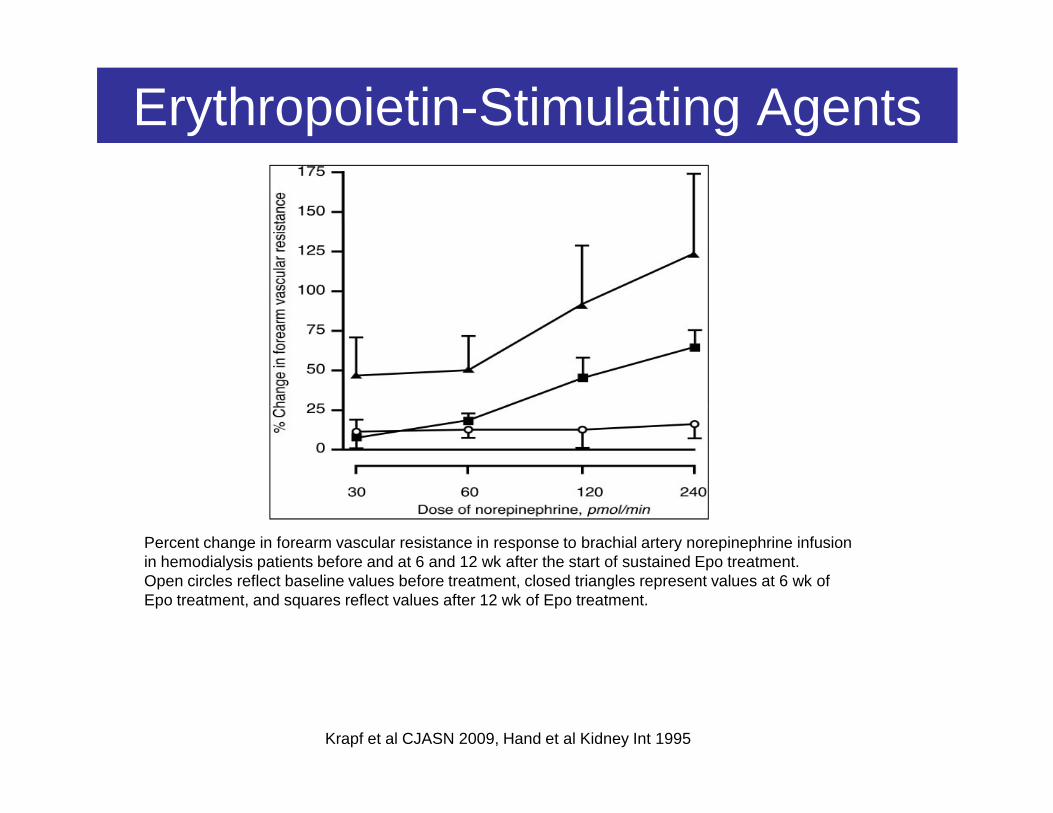
Erythropoietin-Stimulating Agents
Krapf et al CJASN 2009, Hand et al Kidney Int 1995
Percent change in forearm vascular resistance in response to brachial artery norepinephrine infusion in hemodialysis patients before and at 6 and 12 wk after the start of sustained Epo treatment. Open circles reflect baseline values before treatment, closed triangles represent values at 6 wk ofEpo treatment, and squares reflect values after 12 wk of Epo treatment.
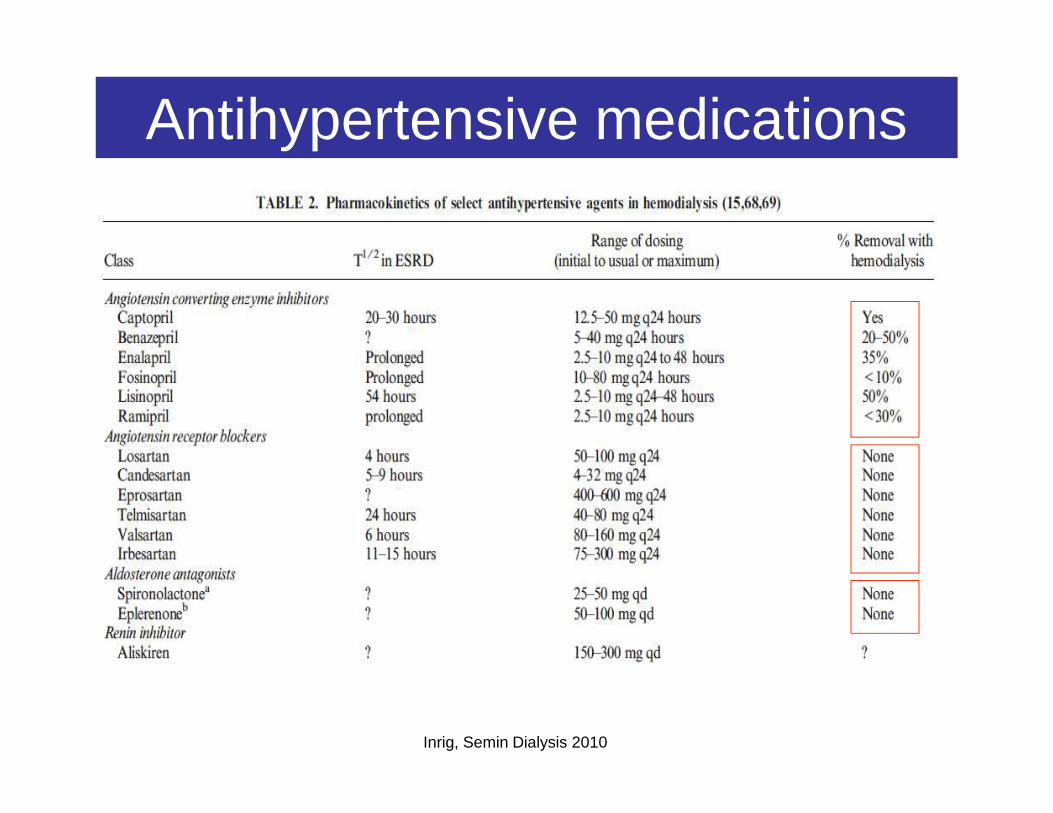
Antihypertensive medications
Inrig, Semin Dialysis 2010
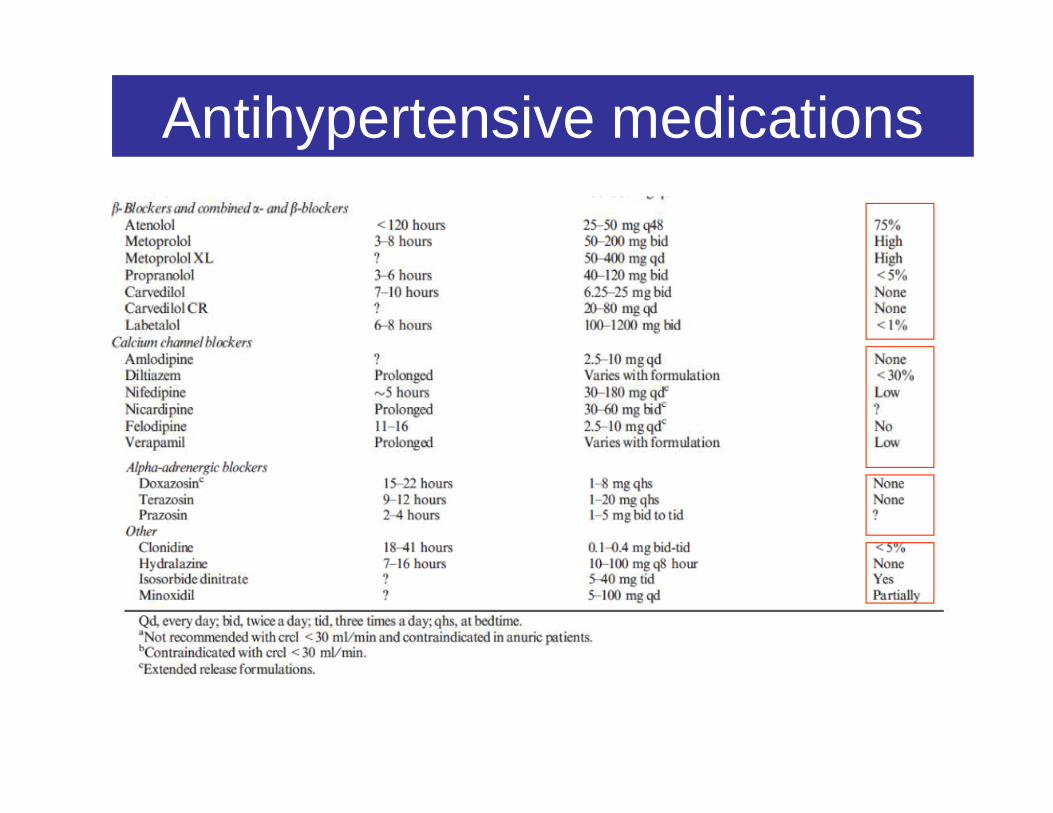
Antihypertensive medications
Antihypertensive medications
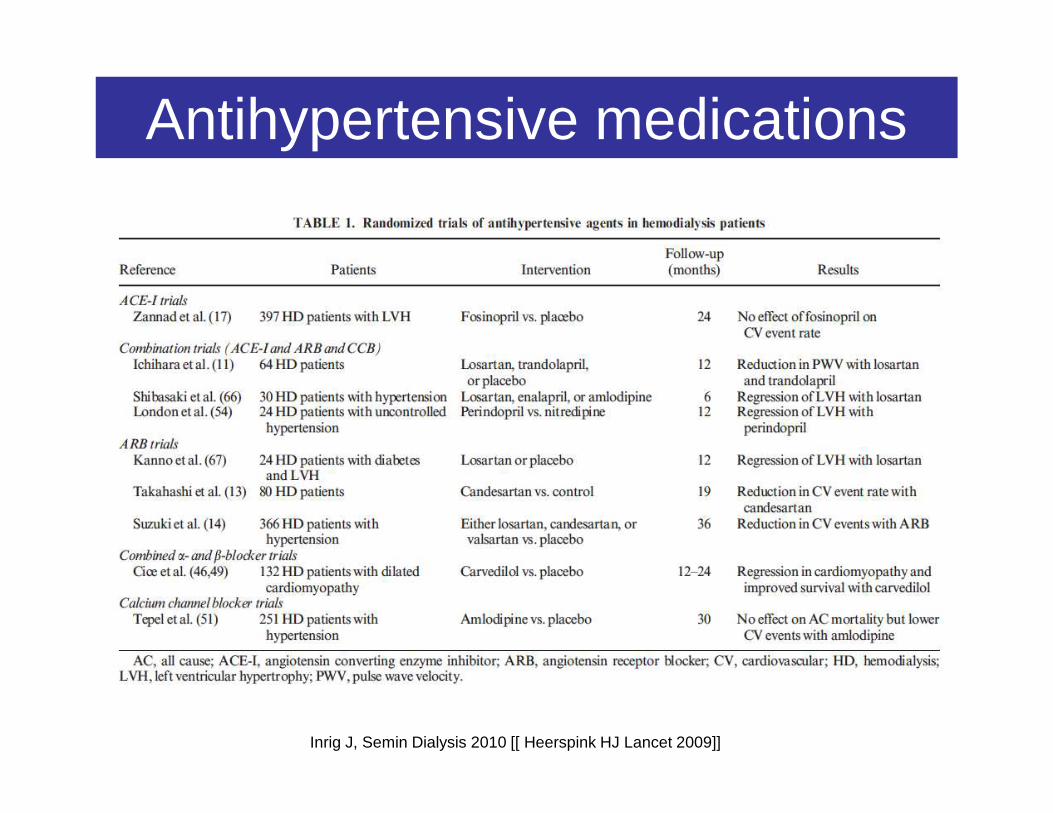
Inrig J, Semin Dialysis 2010 [[ Heerspink HJ Lancet 2009]]
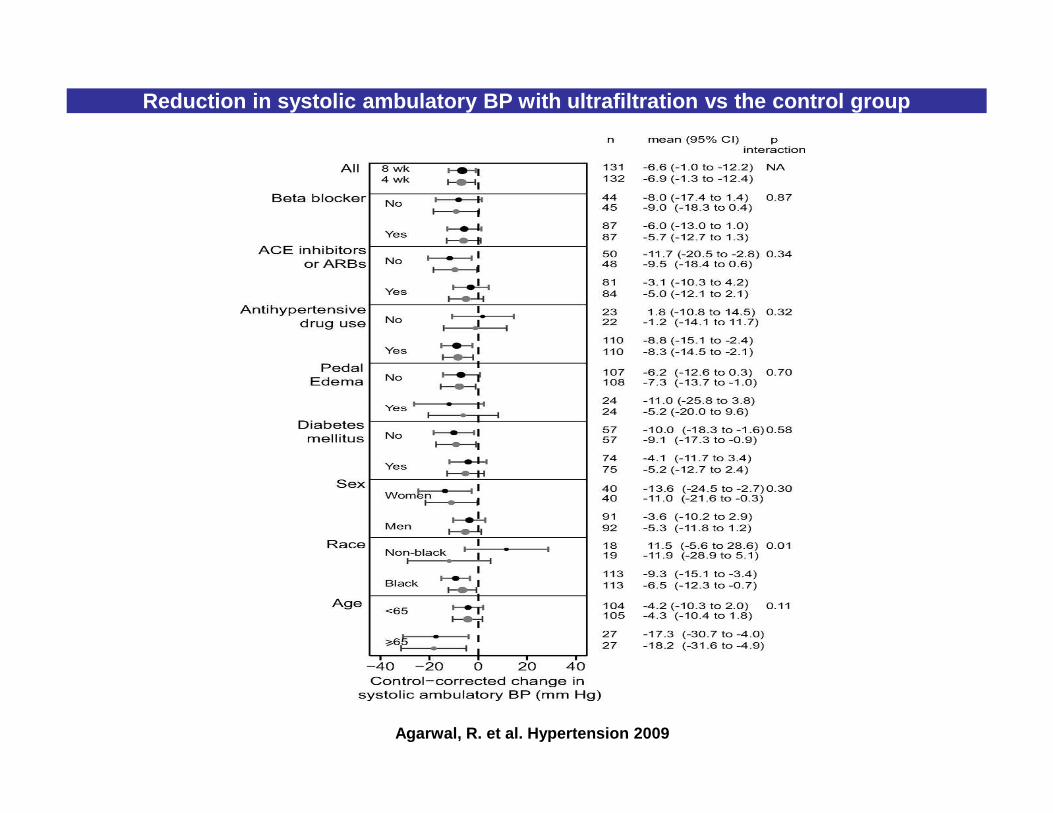
Reduction in systolic ambulatory BP with ultrafiltr ation vs the control group
Agarwal, R. et al. Hypertension 2009

Potential strategies for the treatment of intradialytic hypertension
Locatelli et al Nat. Rev. Nephrol. 2009
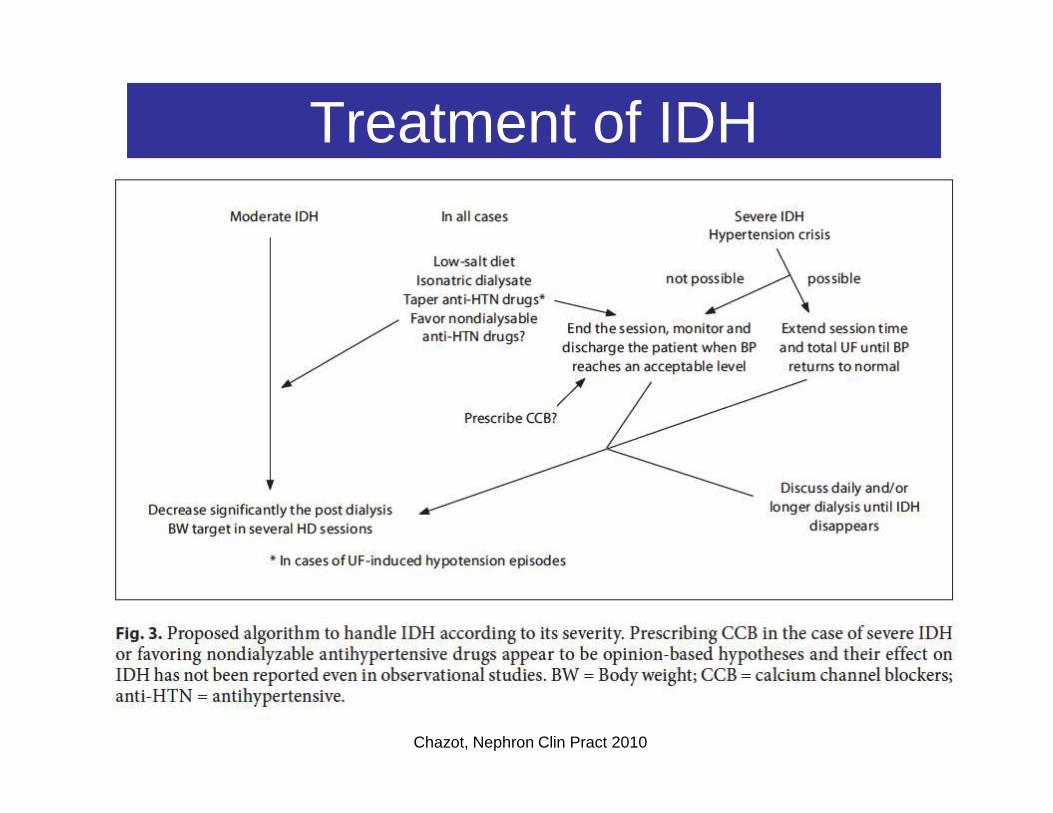
Treatment of IDH
Chazot, Nephron Clin Pract 2010
Conclusion
• IDH present in 5-15% of HD patients• More common in patients who are older , have lower dry
weights and are prescribed more antihypertensive drugs• IDH is associated with a increased risk of hospitalization
or death at 6 months• Important role of endothelial cell dysfuntion• Important role of endothelial cell dysfuntion• Treatment should be individualized
– Decreasing dry weight +++ (sodium balance neutral or negative)– Altering the dialysis prescription– Select antihypertensive medications according to the elimination
profile – Suspend ESA or switch from intravenous to subcutaneous ESA
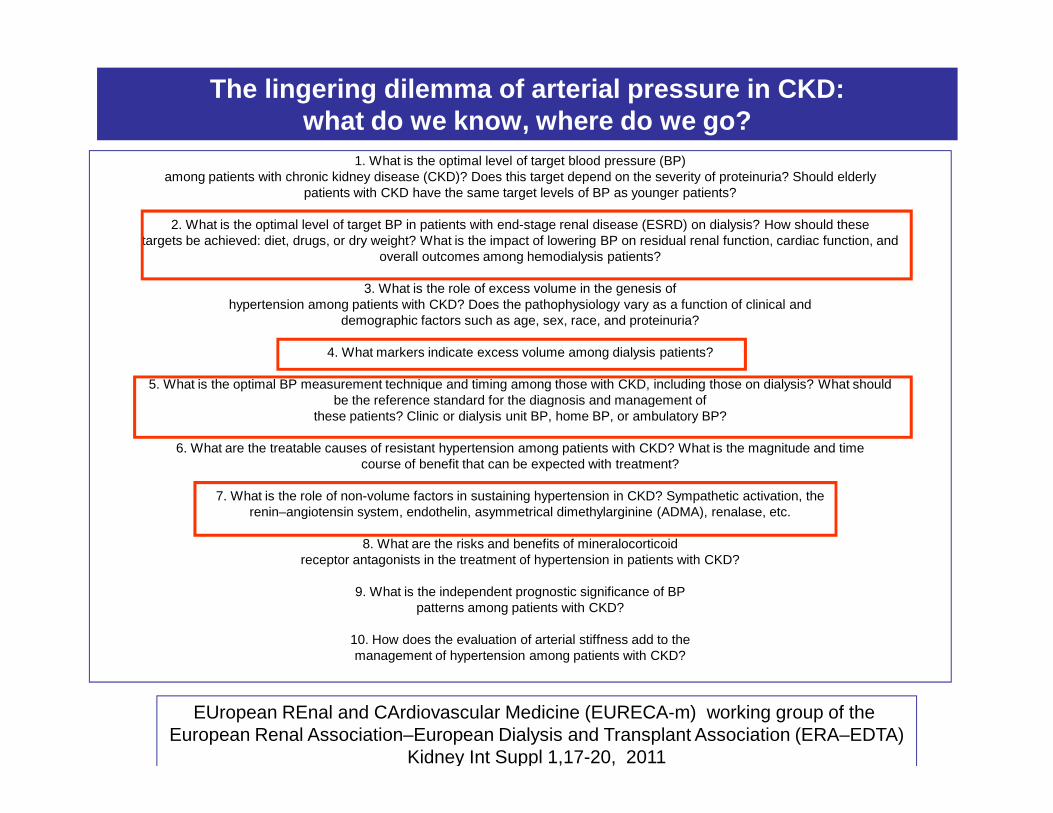
The lingering dilemma of arterial pressure in CKD:what do we know, where do we go?
1. What is the optimal level of target blood pressure (BP)among patients with chronic kidney disease (CKD)? Does this target depend on the severity of proteinuria? Should elderly
patients with CKD have the same target levels of BP as younger patients?
2. What is the optimal level of target BP in patients with end-stage renal disease (ESRD) on dialysis? How should thesetargets be achieved: diet, drugs, or dry weight? What is the impact of lowering BP on residual renal function, cardiac function, and
overall outcomes among hemodialysis patients?
3. What is the role of excess volume in the genesis ofhypertension among patients with CKD? Does the pathophysiology vary as a function of clinical and
demographic factors such as age, sex, race, and proteinuria?
4. What markers indicate excess volume among dialysis patients?
5. What is the optimal BP measurement technique and timing among those with CKD, including those on dialysis? What shouldbe the reference standard for the diagnosis and management ofbe the reference standard for the diagnosis and management of
these patients? Clinic or dialysis unit BP, home BP, or ambulatory BP?
6. What are the treatable causes of resistant hypertension among patients with CKD? What is the magnitude and timecourse of benefit that can be expected with treatment?
7. What is the role of non-volume factors in sustaining hypertension in CKD? Sympathetic activation, therenin–angiotensin system, endothelin, asymmetrical dimethylarginine (ADMA), renalase, etc.
8. What are the risks and benefits of mineralocorticoidreceptor antagonists in the treatment of hypertension in patients with CKD?
9. What is the independent prognostic significance of BPpatterns among patients with CKD?
10. How does the evaluation of arterial stiffness add to themanagement of hypertension among patients with CKD?
EUropean REnal and CArdiovascular Medicine (EURECA-m) working group of the European Renal Association–European Dialysis and Transplant Association (ERA–EDTA)
Kidney Int Suppl 1,17-20, 2011
