interruptions experienced by cardiovascular intensive care...
TRANSCRIPT

1
Interruptions Experienced by Cardiovascular Intensive Care Unit Nurses: An Observational Study Farzan Sasangohara,b, Birsen Donmeza, Anthony Eastyb,c, Helen Storeyd, and Patricia Trbovichb,c
a Department of Mechanical and Industrial Engineering, University of Toronto
b HumanEra, Techna, University Health Network
c Institute of Biomaterials and Biomedical Engineering, University of Toronto
d University Health Network
Acknowledgement for research support: This research was funded by a Natural Sciences and
Engineering Research Council of Canada (NSERC) Postgraduate Scholarship and a Canadian
Institute of Health Research (CIHR) Health Care, Technology, and Place (HCTP) Doctoral
Scholarship.
Word count (including abstract; excluding figures, tables, and references): 3659 Number of tables: 4 Corresponding author: Birsen Donmez, 5 King’s College Rd., Toronto, Ontario, Canada, M5S
3G8, email: [email protected], telephone: +1 (416) 978-7399; fax: +1 (416) 978-7753.

2
Keywords: Interruptions; Nursing; ICU; Task Severity; Cardiovascular
Abstract
Purpose: Intensive Care Unit (ICU) nurses get interrupted frequently. Although interruptions
take cognitive resources from a primary task and may hinder performance, they may also convey
critical information. Effective management of interruptions in ICUs requires the understanding
of interruption characteristics, the context in which interruption happens, and interruption
content. Methods: An observational study was conducted in a Cardiovascular ICU at a Canadian
teaching hospital. Four observers (1 Ph.D. and 3 undergraduate students) trained in human
factors research observed 40 nurses, approximately 1-hour each, over a 3-week period. Data
were recorded by the observers in real time, using touchscreen tablet PCs and special software
designed for this purpose. Results: Although about half of the interruptions (~51%) happened
during high-severity tasks, more than half of these interruptions which happened during high-
severity tasks conveyed either work- or patient-related information. Further, the rate of
interruptions with personal content was significantly higher during low-severity tasks compared
to medium- and high-severity tasks. Conclusions: Mitigation strategies other than blocking
should also be explored. In addition, interrupters might have evaluated primary task severity
before interrupting. Therefore, making task severity more transparent may help others modulate
when and how they interrupt a nurse.

3
1. INTRODUCTION
Intensive Care Units (ICUs) are complex and demanding modern work environments. ICU
nurses perform various procedures, document patient care, interact with medical devices,
respond to the needs of patients and families, and often multi-task (1). Further, ICU nurses are
frequently interrupted (e.g., (2–4)). ICUs are generally known to be error-prone (5) and given the
limitations of human working memory and attentional resources (e.g., (6–9)), it is likely that
interruptions combined with performing multiple concurrent tasks facilitate errors (10). In line
with this expectation, interruptions observed in health care settings are generally considered to
have negative effects on performance, and some of the current mitigation approaches focus on
removing or blocking interruptions by applying the so called “sterile cockpit” approach and “no
interruption” zones (e.g., (11–13)). However, interruptions at times are necessary as they can
convey critical information (14-17); therefore, mitigation strategies should be designed
accordingly.
As a first step to understanding different ICU interruptions with the ultimate goal of
developing situation-specific mitigation approaches, we propose that the following three C’s of
interruptions should be considered:
1) Characteristics (e.g., frequency and duration): Previous research on interruptions
mainly focuses on interruption characteristics and suggests that both interruption frequency and
duration have an impact on performance. Longer interruptions tend to result in a longer period of
task resumption (i.e., time taken to resume the primary task once the interruption is over), which
can hinder performance for time-critical tasks (18,19). Further, more frequent interruptions
decrease decision accuracy and increase decision time (20). In the ICU context, research so far
has mainly focused on the frequency and duration of interruptions to nurses and reported high
4
frequencies (10/hour in Drews (21); 15.3/hour excluding multitasking in Grundgeiger et al. (19);
4.5/hour during documentation in Ballerman et al. (22)) and an increased task resumption time
for longer interruptions (19).
2) Context (e.g., sources of interruption, tasks being interrupted, and conditions
interruptions happen under): Context plays a major role in understanding why interruptions
happen and informs how they should be handled. For example, it may be necessary to block an
interruption if the task-at-hand can lead to a severe outcome in case of an error. Conversely, an
interruption may increase arousal in low workload periods. In this study, we focus on primary
task (or task-at-hand) severity and interruption sources. To our knowledge, an analysis of
interruptions according to primary task severity has not been conducted in ICU settings. In
general, previous ICU-specific studies report other nurse interruptions to be one of the top
sources (24% in pediatric ICU by McGillis Hall et al. (4); 37.3% in adult ICU by Drews (21))
and patient care and documentation as the most commonly interrupted primary tasks (34% and
21% respectively reported by McGillis Hall et al. (4) for pediatric ICU).
3) Content (e.g., information the interruption conveys, purpose of interruption):
Interruption content can guide how the interruption should be handled. For example, an
interruption should potentially be allowed if it conveys time-critical information about the task-
at-hand, or if it is necessary for another time-critical task even if it is unrelated to the task-at-
hand (e.g., another patient having a cardiac arrest). In pediatric care (critical, surgical, and
medical care combined), McGillis Hall et al. (4) reported communications with the nurse related
to patient care to be the most frequent cause of interruptions (35%) as well as the existence of
potentially non-patient-care related interruptions (e.g., socializing: 4% and phone calls: 2.7%).
These latter types of interruptions may have to be blocked based on a given context. In general,

5
interruption mitigation strategies should consider the urgency of an interruption and its relevance
to the task-at-hand.
Understanding interruptions in a complex system such as an ICU requires a holistic
approach. We believe that studying context, content, and characteristics of interruptions and their
interaction could be used as a framework to provide insight into why and how interruptions
occur. In this paper, an initial step is taken through an observational study to explore the relations
between the three C’s of interruptions, by identifying interruption content and associated primary
task severity.
2. METHODS
Nurses of the Cardiovascular ICU (CVICU) of a Canadian teaching hospital were asked to
participate in an observational study. Forty nurses participated in the study (response rate of
90%). Observations were conducted on weekdays between 8:00 and 18:00 during day shifts
(07:30 to 19:30) over a 3-week period. The study was approved by the Research Ethics Board of
this hospital. Four observers (1 Ph.D. and 3 undergraduate engineering students) trained in
human factors research conducted 56 observation sessions (1 observer per session), ranging from
26 to 110 minutes, with an average of 56 minutes. The total observation time was 48 hours, a
number that is similar to previous ICU interruption studies (34 hours in Drews (21); 30 hours in
Grundgeiger et al. (19); 60 hours in Ballerman et al. (22)). Each working hour from 8:00 to 18:00
was observed at least three times. Undergraduate students were trained by the Ph.D. student
regarding data collection (5-hours each) and performed two pilot studies (2-hours each) along
with the Ph.D. student. In addition, a codebook was developed to ensure standard adoption of
terminology and to homogenize event coding (Table 1).
Inter-rater reliability was analyzed for the coding of events collected in the pilot studies.

6
Cohen’s Kappa was calculated to compare the coding for each data collection category (i.e.,
interruption source, interrupted task, and interruption content) separately between the Ph.D.
student and each undergraduate observer. Results showed substantial to almost perfect
agreements between observer pairs for the interruption source (Kappa ranged from 0.71 to 0.95),
moderate to almost perfect for the interrupted task (Kappa ranged from 0.59 to 0.95), and
moderate to almost perfect for the interruption content (Kappa ranged from 0.56 to 0.88).
Overall, only one undergraduate observer had moderate agreements with the Ph.D. student (i.e.,
0.55 < Kappa < 0.6 for two categories). This undergraduate observer participated in 3 hours of
additional training. Considering the large number of categories used to establish inter-rater
reliability, the results show an adequate level of agreement between observers (23).
2.1 Apparatus
An observational tool called Remote Analysis of Team Environments (RATE) was used
on two Motion C5t and two Fujitsu Lifebook U810 ultraportable touchscreen tablets. RATE,
developed by University of Virginia researchers (24), was modified for the purposes of this study
to include lists of interruption sources, interrupted tasks, and interruption content (Table 1).
These lists were based on a review of the literature (25) and interviews conducted with three
experienced CVICU nurses before the observational study was undertaken. In order to document
an interruption, the observer interacted with the RATE interface to select the proper categories
from the lists of interruption source, interrupted task, and interruption content, which created a
time-stamped interruption event in a database. These lists were entirely visible at any point in
time (i.e., no drop-down menus were used). Further, 10 most recent events were visible on the
right-side of the screen to facilitate the recording of when an interruption ended. When the
observer clicked an event, it was time stamped and removed from the list. On the interface, there

7
was a ‘comments’ text box, which was used by the observer to take opportunistic notes using a
digital keyboard or a stylus. When the observer finished taking a note by clicking the ‘enter’
button, the note was time-stamped and saved. It should be noted that although an attempt to
collect data on interruption length was made, these data are not reported in this paper due to data
collection limitations.
<< Insert Table 1 about here>>
2.2 CVICU Staff
The CVICU observed in the present study has approximately 20 registered nurses (RNs)
present during the day shifts, including 1 clinical resource RN and 1 nurse manager. Overall,
there are about 100 nurses working in this CVICU. Other personnel generally available during
day shifts on weekdays are: 1 patient-care coordinator (PCC), 2 staff medical doctors (MDs), 2
vascular fellows, 2 unit clerks, 3 patient care assistants (PCAs), and 3-4 cardiovascular surgeons.
Each day, there are two rounds (at 07:30 and 15:00) in which the CVICU team including 1-2
staff anesthesiologists, 1 cardiovascular surgeon, 2-3 cardiovascular and anesthesia fellows, 1 in-
charge nurse, and primary and neighboring nurses participate. There are also vascular team
rounds at 08:00 in which 1 vascular surgeon, 2 fellows, 3 residents, 1 patient-care coordinator,
and primary and neighboring nurses participate.
2.3 Procedure
At the beginning of the study, the observer explained the study procedures and told the
participants that the focus of the study was not to collect data on their performance but to collect
data on the events that resulted in an interruption to their tasks. After obtaining participant
consent, one observer shadowed one registered nurse for about an hour. To obtain a more
representative sample, a large number of nurses were observed for an hour each rather than fewer

8
nurses for longer time periods. Further, we wanted to limit the observation period to minimize
observer fatigue. When an interruption occurred, the observer marked the relevant information
on the RATE software. If time allowed, he also typed in additional comments (e.g., MD entered
the room to discuss lab results).
The definition of interruption adopted for this paper is an external intrusion of a
secondary task, which leads to a discontinuity in primary task. This definition is similar to the
one given by Grundgeiger et al. (26) but does not consider the secondary task to be unplanned or
unexpected as these two stipulations were hard to assess during observation. Further, the
definition we adopted also does not consider a “discontinuity in task performance” as suggested
by Grundgeiger et al. (26) since we were not able to assess primary task performance. Although
the observers attempted to record data on potential distractions as well (e.g., noise from the
hallway), due to reliability issues associated with the identification of distractions, this paper
focuses only on interruptions as defined above.
3. RESULTS
3.1 Characteristics
In 48 hours of total observation time, 1007 interruptions were observed. That is, on
average, one interruption occurred per about 3 minutes of observation.
3.2 Context
Of the 1007 interruptions observed, other nurses were the most common source
(43.38%), followed by equipment (12.04%) and MDs (12.04%), and then patients (8.46%),
visitors (6.47%), and phone (4.38%). The rest of interruption sources accounted for less than
15% of all interruptions.
Almost half of all interruptions happened during documentation (26.91%) and procedures

9
(21.45%) (Table 2). Once the observations were complete, four experienced nurses were asked to
categorize CVICU tasks as having high, medium, or low severity outcomes in case of an error.
The nurses responded individually and the mode response was chosen for task severity. Based on
this breakdown, about half of the interruptions (50.65%) were found to have happened during
high-severity tasks (Table 2). It should be noted that about 6% of the interruptions could not be
assigned a task-severity category due to missing information.
<< Insert Table 2 about here>>
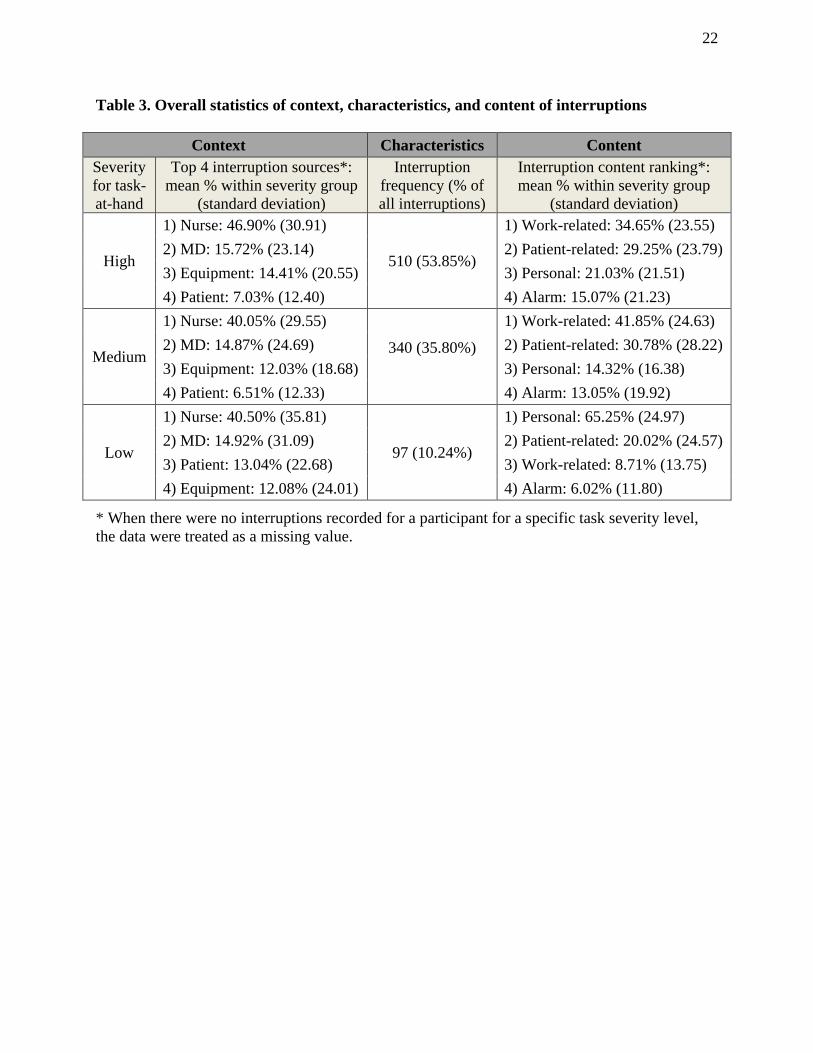
Table 3 reports the frequency percentage (mean and standard deviation) of different
interruption sources and contents within the three task severities. To obtain this table, we first
calculated the frequency percentages within each task severity for each participant; we then
calculated the means and standard deviations of these values. When there were no interruptions
recorded for a specific task severity level, the datum for that task-severity level was treated as a
missing value. For low-severity tasks, there were 17 participants whose data were treated as
missing as opposed to one participant each for high- and medium-severity tasks.
<< Insert Table 3 about here>>
A 3 (task severity: high, medium, or low) x 4 (source: nurse, MD, equipment, or patient)
mixed linear model was built with participant included as a random factor. The main effect of
source was significant (F(3,357) = 43.30, p < .0001). In particular, rate of nurse interruptions
were significantly higher than that of MDs (t(357) = 8.35, p < .0001), patients (t(357) = 10.17, p
< .0001), and equipment (t(357) = 9.03, p < .0001). The main effect of task severity (F(2,357) =
0.13, p = .88) and its interaction with source were not significant (F(6,357) = 0.38, p = .89).

10
3.3 Content
The majority of interruptions were either work-related (but not about the patient-in-care,
34.79%) or patient-related (33.26%). Interruptions with personal content constituted 17.88%; and
one-third (20.18%) of interruptions by other nurses were about personal matters. Furthermore,
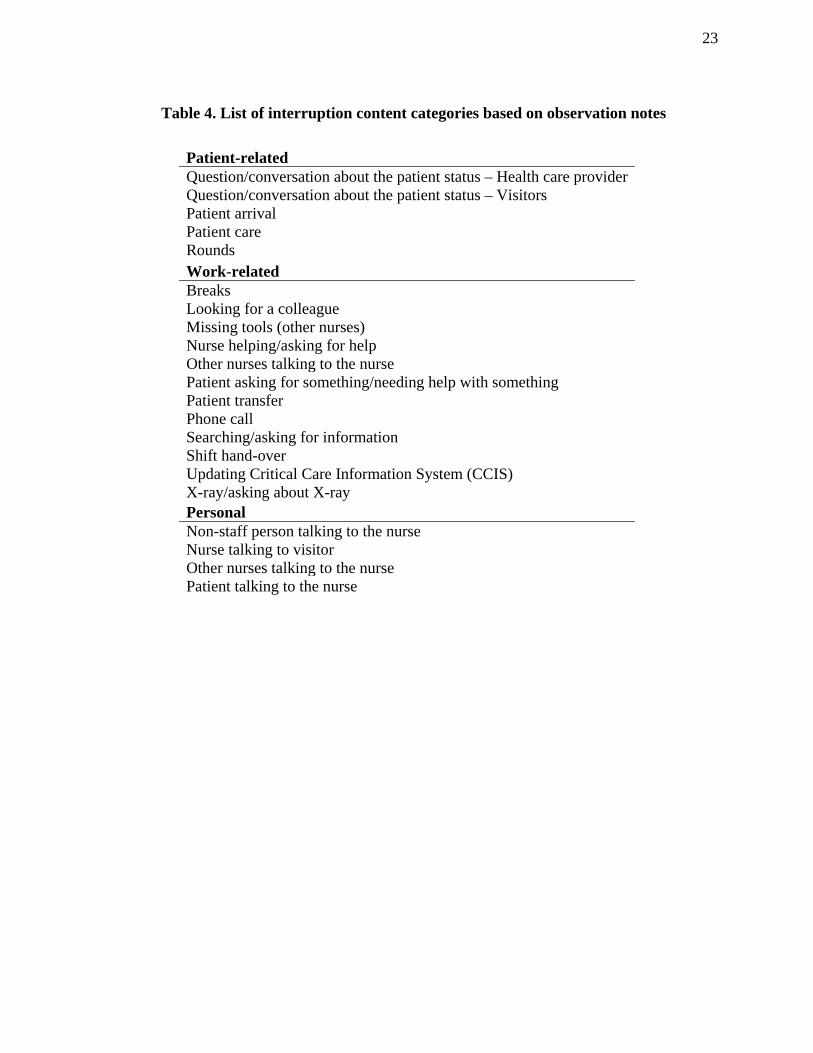
alarms constituted 14.07% of all interruptions. Table 4 presents a list of interruption contents that
were recorded through opportunistic notes. Although it may not be a comprehensive list of
contents, it is provided here to inform future observational studies.
<< Insert Table 4 about here>>
A 3 (task severity: high, medium, or low) x 4 (content: patient-related, work-related,
personal, or alarm) mixed linear model with participant included as a random factor revealed
significant effects for content (F(3, 349) = 17.40, p < .0001) and its interaction with task severity
(F(6, 349) = p < .0001). Follow-up comparisons of content across different task severity levels
revealed that, the rate of interruptions with personal content observed during low-severity tasks
was higher than that observed during both medium- (t(349) = 8.67, p < .0001) and high-severity
tasks (t(349) = 7.52, p < .0001). Further, the rate of work-related interruptions to low-severity
tasks was smaller than that to both medium- (t(349) = -5.64, p < .0001) and high-severity tasks
(t(349) = -4.41, p < .0001). Other comparisons were not significant (p > .05).
Comparisons of task-severity level across different contents were also conducted. During
low-severity tasks, the rate of personal interruptions was higher than the rate of alarms (t(349) =
8.91, p < .0001), work-related interruptions (t(349) = 8.51, p < .0001), and patient-related
interruptions (t(349) = 6.80, p < .0001). During high-severity tasks, the rate of alarms was lower
than the rate of interruptions with patient-related content (t(349) = -2.84, p = .005) as well as
work-related-content (t(349) = -3.92, p < .0001). In addition, interruptions with work-related

11
content were observed to have a significantly higher rate than personal interruptions (t(349) =
2.73, p = 0.007). Same differences were observed during medium-severity tasks, where the rate
of alarms was lower than the rate of interruptions with patient-related content (t(349) = -3.55, p =
.0004) as well as work-related-content (t(349) = -5.77, p < .0001). Further, again for medium-
severity tasks, interruptions with work-related content had a significantly higher rate than
personal interruptions (t(349) = 5.52, p < 0.001). Other comparisons were not significant (p >
.05).
4. INTERPRETATION
Summary: The ICU nurses got interrupted frequently (~20/hour). Other nurses (~43%) accounted
for almost half of all interruptions, followed by equipment (~12%) and MDs (~12%). Almost
half of all interruptions (~51%) happened during high-severity tasks and in particular during
procedures (~21%). Although majority of interruptions were either work- or patient-related,
about 18% of interruptions were due to personal reasons. Moreover, based on opportunistic
notes, it was found that some of the work-related interruptions were initiated by nurses who were
missing medical supplies or equipment. Finally, looking across task-severity levels, the rate of
work-related interruptions were significantly higher during medium- and high-severity tasks
compared to low-severity tasks, whereas rate of interruptions with personal content was
significantly higher for low-severity tasks compared to medium- and high-severity tasks.
Explanation of findings: We observed 19.7 interruptions per hour, slightly larger than
other observational studies in ICU settings which reported 4.5 to 15.3 per hour, a range that itself
represents large variability (19, 21–22). The differences among these numbers might be due to
differences in interruption definitions adopted or due to the characteristics of the specific ICUs
observed. Also in line with other studies (24% in a pediatric ICU in McGillis Hall et al. (4);

12
37.3% in adult ICU in Drews (21)), we observed other nurses to be the most common source of
interruption (~43%).
Similar to Trbovich et al. (27) who investigated interruptions in chemotherapy settings,
interrupted ICU tasks were categorized in terms of potential severity in case of an error.
Although the majority of observed ICU tasks were categorized as high-severity tasks, the fact
that more than half of the interruptions happened during high-severity tasks might be of concern.
However, a large percentage of interruptions were found to be either work- or patient-related,
which can convey information that is necessary for the completion of the task-at-hand. Ideally,
the non-urgent, non-task-relevant interruptions should be delayed or blocked during high-
severity tasks. It should be noted that such mitigation techniques would depend on the awareness
of the task-at-hand which may sometimes be difficult to achieve. For example, a clinician may
enter a room without knowing the tasks that are being performed and the mere act of entering a
room may cause an interruption. Conversely, interruptions with personal content ranked highest
during low-severity tasks, which may indicate that interrupters might have evaluated the task
severity before interrupting. Although not statistically significant, higher average rate of
interruptions by patients during low-severity tasks (Table 3) may also support this argument.
Therefore, making task severity more transparent may help others modulate when and how they
interrupt a nurse. Work is underway to evaluate technological interventions to improve task-
severity awareness by enabling nurses to inform other personnel of the severity of task-at-hand.
Limitations: One of the limitations of this study was that only the day shifts were
observed. Interruptions may in fact have different characteristics during night shifts where no
admissions or rounds happen and communication is minimized. In addition, other ICU
environments (e.g., pediatric) may generate different patterns due to variations in workflow,

13
culture, and policies. Moreover, the high prevalence of interruptions during certain primary tasks
might be due to the fact that these tasks constitute a majority of nurses’ work.
As it is not known what percentage of time nurses spend performing different primary
tasks, inferences cannot be made connecting primary task characteristics to the occurrence of
interruptions. Further, as pointed out in the results section, when there were no interruptions
recorded for a specific task severity level, the data for that task-severity level was treated as a
missing value. However, when we did not record interruptions for a certain task-severity level,
there could have been two underlying reasons: (1) the participant did not perform tasks at that
severity level during the observation period; (2) the participant did perform tasks at that severity
level, but no interruptions happened during these tasks. Lack of data collection on primary tasks
when interruptions were not present is a general limitation of this study.
Participants were aware of the study’s objective of investigating interruptions. This
awareness might have influenced their behavior. However, if there were an influence, one would
expect the frequency of interruptions to decrease, leading to an underestimation. Further, due to
the complexity of data collection, time constraints, and observers’ limited clinical knowledge,
clinical errors were not documented and the effect of different types of interruptions on task
performance cannot be inferred from the data. Finally, the inter-rater reliability analysis should
include a comparison with an ICU health care professional.
Future work: An important future direction is to differentiate between negative and
positive interruptions. Intuitively, interruptions with personal content are likely to have only
negative effects. However, negative effects would be minimal (and may even become positive) if
these interruptions occur at opportune times, such as during low-risk tasks. On the other hand,
patient- and work-related interruptions may contain important information necessary for the task-

14
at-hand and the overall patient safety (15-17, 28). Similarly, alarms usually convey important
information about an off-nominal situation. Based on this broad reasoning, the majority of
observed interruptions in CVICU were potentially positive. Future work should investigate
interruption management approaches that minimize the negative effects of necessary
interruptions while removing unnecessary ones. Thus, future studies should consider
categorizing interruption importance along with primary task severity. In addition, work is
needed to investigate the effects of varying levels of interruption contexts, contents, and
characteristics on performance.
5. ACKNOWLEDGMENTS
This research was funded by a Natural Sciences and Engineering Research Council of Canada
(NSERC) Postgraduate Scholarship and a Canadian Institute of Health Research (CIHR) Health
Care, Technology, and Place (HCTP) Doctoral Scholarship awarded to Farzan Sasangohar. We
gratefully thank Dr, Mark Chignell, and Dr. Linda McGillis Hall for their insightful feedback,
and Parya Noban, Sahar Ameri, Jaquelyn Monis Rodriguez, and Mohd Asher for their help in
data collection and analysis. The study sponsors were not involved in the conduct of this
research. Further, the authors have no conflicts of interest regarding this research.

15
6. REFERENCES
1. Carayon P, Gürses AP: A human factors engineering conceptual framework of nursing
workload and patient safety in intensive care units. Intensive Crit Care Nurs 2005;21(5):284–301
2. Ebright PR, Patterson ES, Chalko BA, et al: Understanding the complexity of registered
nurse work in acute care settings. J Nurs Adm 2003;33(12):630–8
3. Potter P, Wolf L, Boxerman S, et al: Understanding the cognitive work of nursing in the
acute care environment. J Nurs Adm 2005;35(7-8):327–35
4. McGillis Hall L, Pedersen C, Fairley L: Losing the moment: understanding interruptions to
nurses’ work. J Nurs Adm 2010;40(4):169–76
5. Rothschild JM, Landrigan CP, Cronin JW, et al: The critical care safety study: The
incidence and nature of adverse events and serious medical errors in intensive care. Crit Care
Med 2005;33(8):1694–700
6. Miller GA: The magical number seven, plus or minus two: some limits on our capacity for
processing information. Psychol Rev 1956;63(2):81–97
7. Fuster J: The Prefrontal Cortex. London, UK, Academic Press, 2008
8. Shallice T. From Neuropsychology to Mental Structure. Cambridge, UK, Cambridge
University Press, 1988
9. Just MA, Carpenter PA: A capacity theory of comprehension: Individual differences in
working memory. Psychol Rev 1992;99(1):122–49

16
10. Westbrook JI, Woods A, Rob MI, et al: Association of interruptions with an increased risk
and severity of medication administration errors. Arch Inter med 2010;170(8):683–90
11. Hughes RG, Blegen MA: Medication administration safety. In: Hughes RG, editor. Patient
safety and quality: An evidence-based handbook for nurses. Rockville (MD): Agency for
Healthcare and Quality; 2008
12. Hohenhaus SM, Powell SM: Distractions and interruptions: Development of a healthcare
sterile cockpit. Newborn Infant Nurs Rev 2008;8(2):108–10
13. Anthony K, Wiencek C, Bauer C, et al: No interruptions please: Impact of a no interruption
zone on medication safety in intensive care units. Crit Care Nurse 2010;30(3):21–9
14. Coiera E, Tombs V: Communication behaviours in a hospital setting: an observational
study. BMJ 1998;316(7132):673–6
15. Grundgeiger T, Sanderson P: Interruptions in healthcare: theoretical views. Int J Med Info
2009;78(5): 293-307
16. Rivera-Rodriguez A J, Karsh BT: Interruptions and distractions in healthcare: review and
reappraisal. Qual Safe Health Care 2010;19(4):304-312
17. Walji M, Brixey J, Johnson-Throop K, et al: A theoretical framework to understand and
engineer persuasive interruptions. Proc Hum Factors Ergon Soc Annu Meet 2004, Chicago
18. Monk CA, Gregory J, Boehm-Davis DA: The effect of interruption duration and demand on
resuming suspended goals. J Exp Psychol Appl 2008;14(4):299–313

17
19. Grundgeiger T, Sanderson P, MacDougall HG, et al: Interruption management in the
intensive care unit: Predicting resumption times and assessing distributed support. J Exp Psychol
Appl 2010;16(4):317–34
20. Speier C, Valacich JS, Vessey I: The influence of task interruption on individual decision
making: An information overload perspective. Decis Sci 1999;30(2):337–60
21. Drews FA: The frequency and impact of task interruptions in the ICU. Proc Hum Factors
Ergon Soc Annu Meet 2007;51(11):683–6
22. Ballermann MA, Shaw NT, Arbeau KJ, et al: Impact of a critical care clinical information
system on interruption rates during intensive care nurse and physician documentation tasks. Stud
Health Technol Inform 2010;160(Pt 1):274–8
23. Sim J, Wright CC: The kappa statistic in reliability studies: Use, interpretation, and sample
size requirements. Phys Ther 2005;85(3):257–68
24. Guerlain S, Shin T, Guo H, et al: The RATE tool: multimedia observation and analysis of
teams. Proc Hum Factors Ergon Soc Annu Meet 2002; 46(7):755
25. Sasangohar F, Donmez B, Trbovich P, et al: Not all interruptions are created equal: Positive
interruptions in healthcare. Proc Hum Factors Ergon Soc Annu Meet 2012;56(1):824–8
26. Grundgeiger T, Liu D, Sanderson P, et al: Effects of interruptions on prospective memory
performance in anesthesiology. Proc Hum Factors Ergon Soc Annu Meet 2008; 52(12):808–12
27. Trbovich P, Prakash V, Stewart J, et al: Interruptions during the delivery of high-risk
medications. J Nurs Adm 2010;40(5):211–18
18
28. Henneman EA, Blank FS, Gawlinski A, et al: Strategies used by nurses to recover medical
errors in an academic emergency department setting. Appl Nurs Res 2006;19(2):70–7
19
LIST OF TABLES
Table 1. List of sources of interruption, interrupted tasks, and interruption content used in data
collection
Table 2. Frequency of interrupted tasks grouped by severity
Table 3. Overall statistics of context, characteristics, and content of interruptions
Table 4. List of interruption content categories based on observation notes

20
Table 1. List of sources of interruption, interrupted tasks, and interruption content used in data collection
Interruption Source Interrupted Task Interruption Content Anesthesiologist: CVICU medical anesthesia Clerk: CVICU staff in charge of documentation and communication Equipment: Any noise or alarm related to medical equipment MD: CVICU medical fellows Nurse: Other nurses in the unit Patient: Patient under care PCA: Patient-care assistants are in charge of helping the medical team in tasks such as moving the patient, bed setup, walking the patients. PCC: Patient-care coordinator works directly with CVICU Manager and entire health care team facilitating flow of patients while ensuring all patients and family needs are met. Pharmacist: Hospital personnel in charge of supply of medications to CVICU staff Phone: Any phone that is answered Physiologist: Hospital personnel in charge of post-surgical patient rehabilitation Psychologist: Hospital personnel in charge of providing psychological consultation to patients and family members Surgeon: Hospital personnel who performed the surgery Visitor: Visitors or family members X-ray technician: Hospital personnel who perform in-room x-ray imaging
Connecting equipment: Connecting medical equipment to patient (e.g., defibrillator, dialysis, ventilator) Discussion: Conversations with other health care providers about the status of the patient Documentation: Bedside clinical documentation of patient care such as vital signs, medications, and procedures General care: Routine ICU tasks such as feeding, bathing, and comforting the patient Infusion setup: Setting up the intravenous (IV) infusion such as priming, line insertion, and pump preparation Line change: Process of changing the IV tubing Medication administration: Process of administering medication orally, through infusion, or injection (e.g., connecting syringe to the IV access device and injecting the medication directly into the vein) Medication order: Process of ordering medication for the patient using the medication electronic system Medication preparation: Preparing medication for injection, infusion, or oral administration (e.g., priming IV lines or syringe, preparing the medication cup, connecting IV lines to patients) Patient assessment: Assessing patient status by manual measurement of vital signs, etc. Procedure: Medical procedures performed on the patient (e.g., taking blood sample, intubation) Pump programming: Setting the IV medication dosage and volume to be infused by the pump Using the computer station: Using the in-room computer station for any reason other than medication order (e.g., research, email) Vitals monitoring: Acquiring patient vital signs visually from the displays of the various monitoring devices to which the patient is connected Other: Any other task not categorized above
Patient-related: Interruptions that convey information about patient the observed nurse was treating (e.g., MD orders a new medication, phone call from the lab to discuss blood test) Work-related: Interruptions that are related to CVICU tasks but not about the patient-in-care (e.g., PCC discusses a new transfer, other nurses request help for their patients) Personal: Personal communications that are not about the patient or CVICU tasks (e.g., greetings, personal conversations about vacations) Alarm: Medical equipment or emergency alarms

21
Table 2. Frequency of interrupted tasks grouped by severity
Severity Task Frequency Percentage of all interruptions
High
Procedure 216 21.45% Vitals monitoring 122 12.12% Medication order 51 5.06% Medication preparation 48 4.77% Medication administration 36 3.57% Infusion setup 19 1.89% Pump programming 12 1.19% Patient assessment 6 0.60%
Medium
Documentation 271 26.91% Discussion 64 6.36% Connecting equipment 5 0.50% Line change 0 0.00%
Low General care 96 9.54% Using the computer station 1 0.10%
Other: context data unavailable 60 5.96% Total: 1007 100%
22
Table 3. Overall statistics of context, characteristics, and content of interruptions
Context Characteristics Content Severity for task-at-hand
Top 4 interruption sources*: mean % within severity group
(standard deviation)
Interruption frequency (% of all interruptions)
Interruption content ranking*: mean % within severity group
(standard deviation)
High
1) Nurse: 46.90% (30.91)
510 (53.85%)
1) Work-related: 34.65% (23.55) 2) MD: 15.72% (23.14) 2) Patient-related: 29.25% (23.79) 3) Equipment: 14.41% (20.55) 3) Personal: 21.03% (21.51) 4) Patient: 7.03% (12.40) 4) Alarm: 15.07% (21.23)
Medium
1) Nurse: 40.05% (29.55)
340 (35.80%)
1) Work-related: 41.85% (24.63) 2) MD: 14.87% (24.69) 2) Patient-related: 30.78% (28.22) 3) Equipment: 12.03% (18.68) 3) Personal: 14.32% (16.38) 4) Patient: 6.51% (12.33) 4) Alarm: 13.05% (19.92)
Low
1) Nurse: 40.50% (35.81)
97 (10.24%)
1) Personal: 65.25% (24.97) 2) MD: 14.92% (31.09) 2) Patient-related: 20.02% (24.57) 3) Patient: 13.04% (22.68) 3) Work-related: 8.71% (13.75) 4) Equipment: 12.08% (24.01) 4) Alarm: 6.02% (11.80)
* When there were no interruptions recorded for a participant for a specific task severity level, the data were treated as a missing value.
23
Table 4. List of interruption content categories based on observation notes
Patient-related Question/conversation about the patient status – Health care provider Question/conversation about the patient status – Visitors Patient arrival Patient care Rounds Work-related Breaks Looking for a colleague Missing tools (other nurses) Nurse helping/asking for help Other nurses talking to the nurse Patient asking for something/needing help with something Patient transfer Phone call Searching/asking for information Shift hand-over Updating Critical Care Information System (CCIS) X-ray/asking about X-ray Personal Non-staff person talking to the nurse Nurse talking to visitor Other nurses talking to the nurse Patient talking to the nurse