interoperability and health information exchange workgroup march 19, 2015 micky tripathi, chair...
TRANSCRIPT
Interoperability and Health Information Exchange
Workgroup
March 19, 2015
Micky Tripathi, chairChris Lehmann, co-chair
1

Agenda
• Review HITPC Comments• Approach moving forward• Continue reviewing Interoperability Roadmap
2
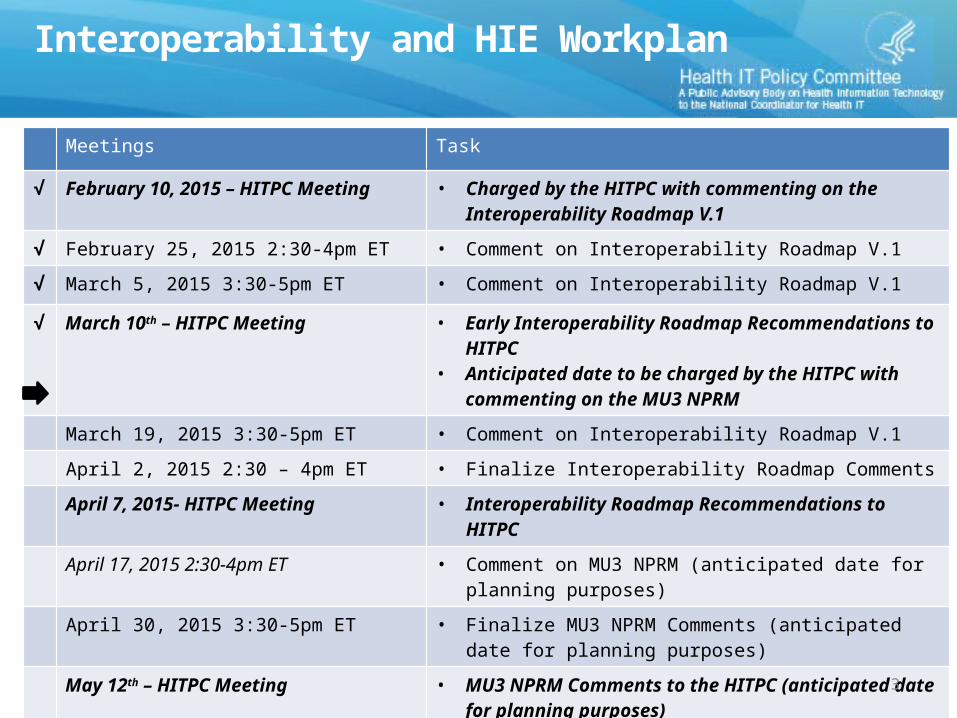
Interoperability and HIE Workplan
Meetings Task
√ February 10, 2015 – HITPC Meeting • Charged by the HITPC with commenting on the Interoperability Roadmap V.1
√ February 25, 2015 2:30-4pm ET • Comment on Interoperability Roadmap V.1
√ March 5, 2015 3:30-5pm ET • Comment on Interoperability Roadmap V.1
√ March 10th – HITPC Meeting • Early Interoperability Roadmap Recommendations to HITPC• Anticipated date to be charged by the HITPC with
commenting on the MU3 NPRMMarch 19, 2015 3:30-5pm ET • Comment on Interoperability Roadmap V.1
April 2, 2015 2:30 – 4pm ET • Finalize Interoperability Roadmap Comments
April 7, 2015- HITPC Meeting • Interoperability Roadmap Recommendations to HITPC
April 17, 2015 2:30-4pm ET • Comment on MU3 NPRM (anticipated date for planning purposes)
April 30, 2015 3:30-5pm ET • Finalize MU3 NPRM Comments (anticipated date for planning purposes)
May 12th – HITPC Meeting • MU3 NPRM Comments to the HITPC (anticipated date for planning purposes)
3
HITPC Comments
4
Approach moving forward
• Based on time remaining and the number of critical action items to review we are proposing to prioritize near term critical action items (2015-2017).– On the last call we discussed 10 of 18 critical action items for accurate
identity matching.– In addition to those 8 remaining items there are 18 reliable resource
location actions to be discussed.– Next call we will discuss the minimum data set for accurate individual
identity matching.• To help provide more actionable recommendations to ONC we
should specify which near term critical actions items we think can be removed based on our comments that there are too many.– Will request member comment on which critical action items can be
removed and then we will discuss during the next call.
5
6
Accurate Individual Identity Matching

Accurate Individual Identity Matching
• Review summary comments and add any missing thoughts.
7
Accurate Individual Identity Matching – Preliminary Thoughts (1 of 2)
• Technical standards are necessary but not sufficient to establishing accurate and reliable patient-matching – Requires a combination of technical standards and aligned business processes
• Establishment of a best practice minimum set of data for identify-matching would be beneficial– Certification could ensure that EHR technology is capable of capturing and storing this
minimum data set– Should not restrict approaches to only this set– Should not require that “every transaction” include the minimum set – such data is often
not available at all, or not available with sufficient quality, or not appropriate to the specific exchange use case
– WG will make recommendation on minimum data set for next meeting
• ONC can play a valuable role in convening implementers to identify and share best practices and lessons learned– Work done under S&I framework and in specific transaction areas (e.g., PDMPs) should
be shared and leveraged where possible8

Accurate Individual Identity Matching – Preliminary Thoughts (1 of 2)
• Locally driven data governance, such as data-sharing arrangements as defined by the JTF, will motivate use of the minimum data set and address technical and business requirements beyond the minimum set– Too much local variation in capabilities and clinical/business needs to allow a
single national approach– Data assurance – which source is the source of truth? – Data quality – how are emerging issues resolved and maintained?– Voluntary data elements – highly dynamic and dependent on local capabilities– Clinical, business, and legal accountability – who is responsible for what?
• Patient-matching by itself may be setting the bar too low– May want to include record location based on identity-matching as a longer-
term goal in the roadmap to address query-retrieve use cases– Some private data-sharing arrangements are already deploying such services
today (Commonwell, MA HIway, etc)– Opportunity for CMS to launch Medicare-focused RLS based on existing claims
and HITECH data?9

10
Reliable Resource Location
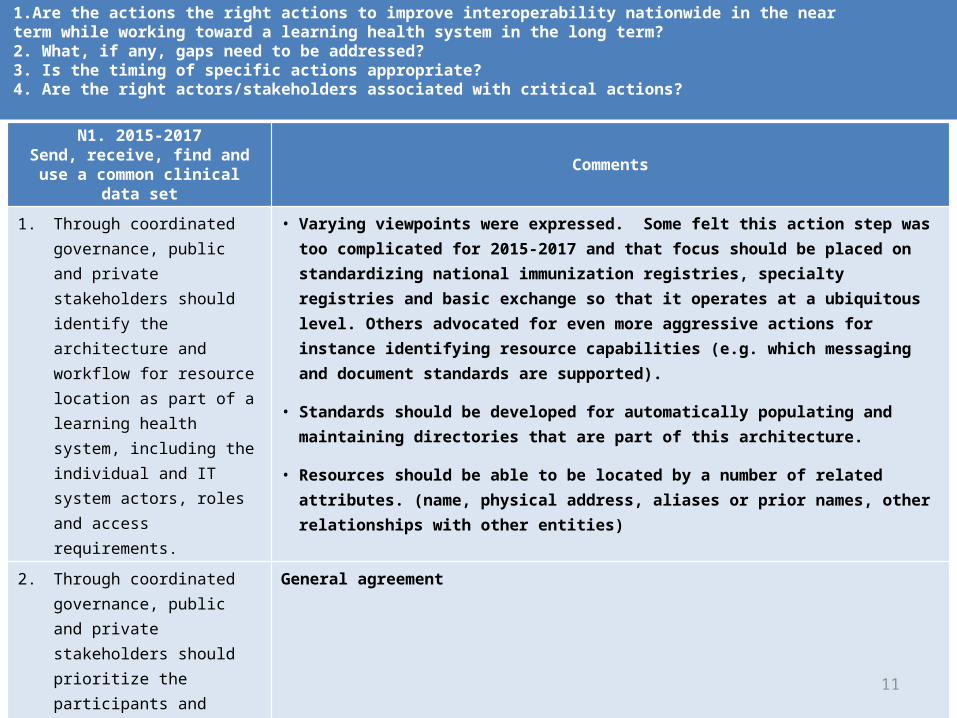
1.Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N1. 2015-2017Send, receive, find and use a
common clinical data setComments
1. Through coordinated governance, public and private stakeholders should identify the architecture and workflow for resource location as part of a learning health system, including the individual and IT system actors, roles and access requirements.
• Varying viewpoints were expressed. Some felt this action step was too complicated for 2015-2017 and that focus should be placed on standardizing national immunization registries, specialty registries and basic exchange so that it operates at a ubiquitous level. Others advocated for even more aggressive actions for instance identifying resource capabilities (e.g. which messaging and document standards are supported).
• Standards should be developed for automatically populating and maintaining directories that are part of this architecture.
• Resources should be able to be located by a number of related attributes. (name, physical address, aliases or prior names, other relationships with other entities)
2. Through coordinated governance, public and private stakeholders should prioritize the participants and services that are to be discoverable using resource location and identify a near-term goal for the first small set of resources to be included in an initial implementation.
General agreement
11
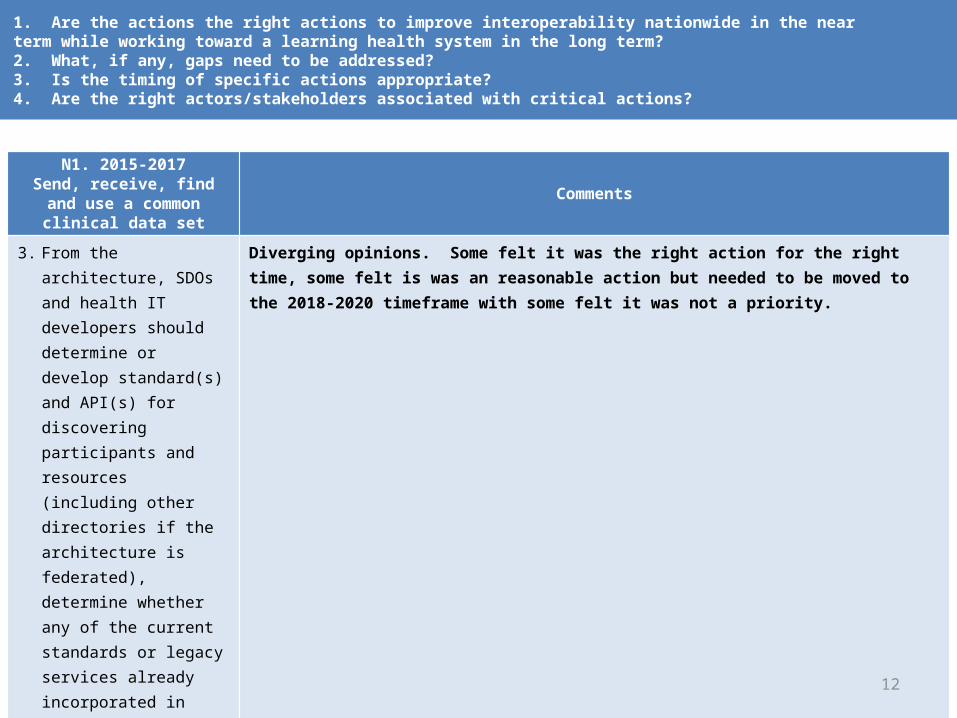
1. Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N1. 2015-2017Send, receive, find and use a
common clinical data setComments
3. From the architecture, SDOs and health IT developers should determine or develop standard(s) and API(s) for discovering participants and resources (including other directories if the architecture is federated), determine whether any of the current standards or legacy services already incorporated in products can be used or extended and develop a Roadmap to implementation of new standard(s) and API(s), if necessary.
Diverging opinions. Some felt it was the right action for the right time, some felt is was an reasonable action but needed to be moved to the 2018-2020 timeframe with some felt it was not a priority.
12

1.Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N1. 2015-2017Send, receive, find and use a
common clinical data setComments
4. Through coordinated governance, public and private stakeholders should identify rules of the road for participating in distributed management of resource location, if appropriate for the architecture and actors. This includes establishing policies and procedures for operation of resource location services, including curation of directory information to maintain data quality.
Diverging opinions some felt it was the right action while others felt it wasn’t a priority.
5. Through coordinated governance, public and private stakeholders should work with SDOs and health IT developers to demonstrate standard(s) and API(s) in a trial implementation, beginning with the prioritized set of resources.
Diverging opinions. Some felt it was the right action for the right time, some felt is was an reasonable action but needed to be moved to the 2018-2020 timeframe with some felt it was not a priority.
13
1.Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N1. 2015-2017Send, receive, find and use a
common clinical data setComments
6. Through coordinated governance, public and private stakeholders should develop a glide path for moving from current provider directories to future resource location techniques.
Diverging opinions. Some felt it was the right action for the right time, some felt is was an reasonable action but needed to be moved to the 2018-2020 timeframe with some felt it was not a priority.
14

1.Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N2. 2015-2017Send, receive, find and use a
common clinical data setComments
1. As an interim step, ONC will work with others to encourage initial uptake of current provider directory activities
General agreement
2. ONC will recommend to CMS that NPPES implement support for the provider directory information query API and data model as specified in the IHE HPD Profile. CMS should maintain Direct addresses and ESI in NPPES
General agreement. Suggestions to improve the action included:
• Should be a similar expectation for private sector care providers• Ensure ESI concept is flexible and extensible• NPPES should be able to handle multiple names, aliases, prior names, physical addresses (payment
address, treating address, ROI address), relationships to other entities along with workflow or profile information.
3. CMS/HRSA/OIG should advance the proposed effort to consolidate/synchronize national credentialing support systems
General agreement
15
1.Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N2. 2015-2017Send, receive, find and use a
common clinical data setComments
4. ONC and other certification bodies will determine how to support provider directories through certification processes
General agreement, though some concern about timing and the readiness of standards and testing tools.
5. ONC will lead the effort to coordinate across federal agencies on the use of existing standards (e.g. provider directory standards)
General agreement
6. ONC will support testing through its Standards Implementation and Testing Environment (www.sitenv.org)
General agreement
16
Next Steps
• Provide comments on near term items to remove
• Next call we will discuss the minimum data set for accurate identity matching and finalize recommendations.
17

Appendix A: Reliable Resource Location Critical Action Items for 2018-2020 and 2021-2024
18

1.Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N1. 2018-2020Expand interoperable health IT
and users
Comments
7. Stakeholder input requested As this work matures, goals/actions need to extend beyond clinical health resources and broadened to address social determinants of health.
N1. 2021-2024Achieve nationwide LHS
Comments
8. Stakeholder input requested
19

1.Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N2. 2018-2020Expand interoperable health IT and
usersComments
7. Through coordinated governance, public and private stakeholders should adopt national standards for locating participants and resources.
General agreement
8. Through coordinated governance, public and private stakeholders should adopt guidance on data quality, maintenance and update processes.
General agreement
9. Through coordinated governance, public and private stakeholders should work with health IT developers to identify and publish best practices for resource location operational issues that could include data quality, maintenance and update processes
General agreement
20
1. Are the actions the right actions to improve interoperability nationwide in the near term while working toward a learning health system in the long term? 2. What, if any, gaps need to be addressed? 3. Is the timing of specific actions appropriate? 4. Are the right actors/stakeholders associated with critical actions?
N2. 2021-2024Achieve nationwide LHS Comments
10. Stakeholder input requested
21