internship survival guide 2014-2015 - college of...
TRANSCRIPT

50
Internship Survival Guide 2014-2015
University of Florida College of Medicine
Department of Pediatrics

2
Section Page
Important Phone Numbers 3
Patient Safety Report 7
Vitals by age, Top 10 Reading List 8
EPIC/ Home Access, List of Order Sets 10
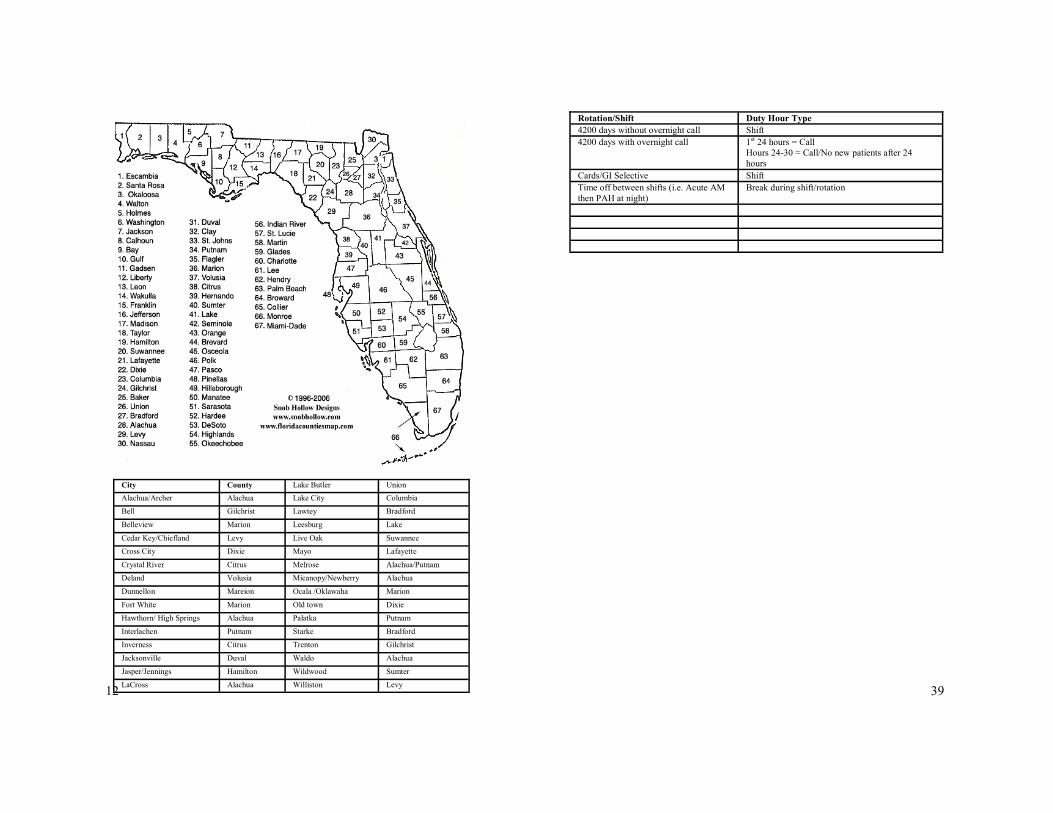
Florida Map 12
Presentations/PBAR 13
I-PASS for Patient Hand Offs 14
PEWS 16
Responding to a Code 18
NICU 19
Newborn Sepsis Guidelines 20
Hyperbilirubinemia 21
PICU 22
Vents and ABG Interpretation 23
Asthma 24
Bronchiolitis Score 26
CF 27
Heme/Onc 28
Transfusion Tips 29
EKG 31
FEN 32
Clinic and immunizations 33-35
Development Chart 36
Duty Hour Logging 37-39
Chain of Command, When to Call ? 40
Procedures 42-44
Important Login Information 45
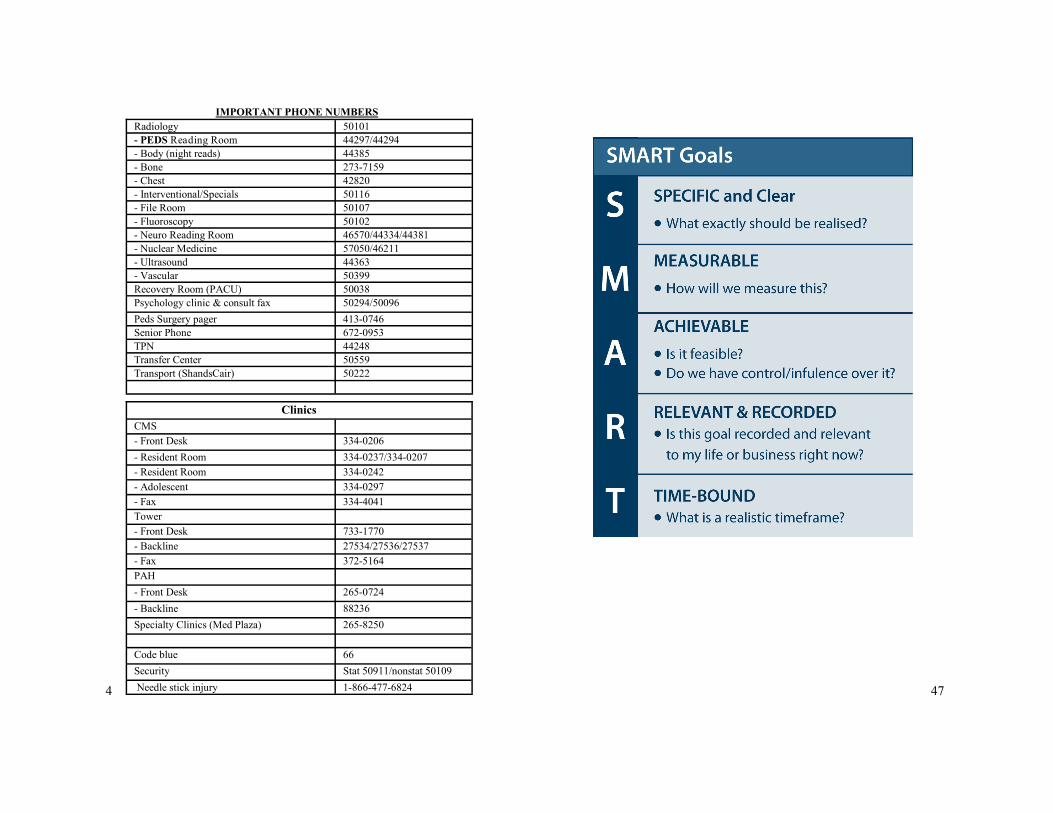
SMART Goals 47
Table of Contents
49

48
3
General Numbers
Admissions 50236
Bed Control 50233
Blood Bank 50377
Cardiology
- ECHO lab (reads) 392-2500
- ECHO 258-1927
- EKG (PICU) 413-0175
- EKG (Floor & NICU) 413-0174
- Heart Station (Holters) 50047
Child Life 46470
- Text pager 413-5068
Dialysis (peds) 50255
EEG 50334
ED Break Room 93517
Hospital (main) 265-0111
iHIRM 59375
Laboratory - Main 47737
- Chemistry 44869
- Hematology 44857
- Immunology 45328
- Microbiology (open 8am-5pm) 50165
- Rocky Point (main) 50172
- Rocky Point (chemistry) 72202
- Send Out 72200
- Virology 44778
Lactation (Brenda) 50317
Medical Records 44796
MRI 50106
MRI anesthesia 49982
OR Front Desk 50023
Pathology 50208
Pharmacy
- Inpatient (PICU) 42754
- Inpatient (Floor & NICU) 43401
- Outpatient (atrium/med plaza) 50405/58270
Pre-op 50076
PFTs (pulmonary) 50275
Poison Control 800-222-1222
Peds ID consults/ outpt scheduling 294-5481/294-5480
4
IMPORTANT PHONE NUMBERS
Radiology 50101
- PEDS Reading Room 44297/44294
- Body (night reads) 44385
- Bone 273-7159
- Chest 42820
- Interventional/Specials 50116
- File Room 50107
- Fluoroscopy 50102
- Neuro Reading Room 46570/44334/44381
- Nuclear Medicine 57050/46211
- Ultrasound 44363
- Vascular 50399
Recovery Room (PACU) 50038
Psychology clinic & consult fax 50294/50096
Peds Surgery pager 413-0746
Senior Phone 672-0953
TPN 44248
Transfer Center 50559
Transport (ShandsCair) 50222
Clinics
CMS
- Front Desk 334-0206
- Resident Room 334-0237/334-0207
- Resident Room 334-0242
- Adolescent 334-0297
- Fax 334-4041
Tower
- Front Desk 733-1770
- Backline 27534/27536/27537
- Fax 372-5164
PAH
- Front Desk 265-0724
- Backline 88236
Specialty Clinics (Med Plaza) 265-8250
Code blue 66
Security Stat 50911/nonstat 50109
Needle stick injury 1-866-477-6824 47

46
Important Information
How to Access Log in Name Password
Pedalink
- ILP
- PREP questions
www.pedialink.org or via
www.aap.org AAP ID # Set up yourself
Nelson’s Online http://site.ebrary.com/lib/
univflorida/
docDetail.action?
docID=10567389
None-must be on VPN None-must be on VPN
The Harriet Lane Hand-
book
http://site.ebrary.com/lib/
univflorida/
docDetail.action?
docID=10567408
None-must be on VPN None-must be on VPN
FL Shots www.flshots.com Organization ID: UFPC01 (for CMS) and UFPC02 (for
Tower)
Username: Last name plus
first letter of first name in all caps (i.e. Al Gator would be
GATORA)
Set up yourself
CANVAS Gatorlink username Gatorlink password
Genetics Patient Protocols http://www.peds.ufl.edu/
divisions/genetics/
fellowship.htm
Patient Protocols - then
enter Gatorlink username Gatorlink password
New Innovation Www.new-innov.com First letter of first name
and then last name
Set up yourself
Med student eval Medinfo.ufl.edu Gatorlink username Gatorlink password
5
Outpatient Departments
Allergy 265-8250
Cardiology 273-7770
Child Psychology 413-3338
CPT 334-1300
Dental (peds) 273-7643
- Backline 273-7645
Endocrinology 334-1390
Gastroenterology 273-9350
Genetics 294-5050
Hematology/Oncology 392-5633
Immuno/Rheum/ID 392-2961
Lactation Clinic (Mary’s cell/pager) 219-2335/413-4302
Nephrology 392-4434
Neurology 273-8920
Ortho Clinic 273-7001
- Backline (Teri Rhodes) 273-7379
Pulmonology 392-4458
Inpatient Floors & Workrooms
4200 50042 (fax 265-0946)
4400 50044 (fax 265-0467)
4500 50045 (fax 265-0793)
4433 Conference Room 44013
Blue Workroom (4530) 43450/47325/44057
Green Workroom (4270) 48208/43449/46200
Orange Workroom (4437) 43934/45259
ER 265-5437 (KIDS)
- Charge Nurse 745-8280
- Peds Resident Phone 51256 or 51257
- Peds Attending 745-8278
Mother/Baby (3500) 50035
Newborn Nursery 44097
NI2 50352
NI3 50033
- Fishbowl 44348/44124
PICU 51004/51005
- Fellow phone 494-8383
- Resident phone 745-8027
Housekeeping 50480

6
Housestaff Numbers
Pediatric Chair’s Office 273-9001
Pediatric Med Ed 273-8234
Tammy/Amy 273-8466/273-8594
- Fax 273-8593
Chief Pager 888-980-3608
Chief Office – Nora 50912
Chief Office – Kendall 50919
Clinical pharmacists
- Brian Kelly 45868/413-4054
- Lisa Taylor 413-1892
Dr. Black 50915/413-2048
Peds IT/Shands IT 273-5808/265-0526
PCCP 413-1454
Pediatric Team Phones
Green Team 317-5326
Senior Phone 672-0953
Outside Hospitals
Halifax (Daytona Beach) 386-254-4000
Leesburg Regional Medical Center 352-323-5762
Munroe Regional Medical Center 352-351-7200
N. FL Regional Medical Center (NFRMC) 352-333-4000
Ocala Regional Medical Center 352-401-1000
Putnam Community Medical Center (Palatka) 386-328-5711
Seven Rivers (Crystal River) 352-795-6560
Tallahassee Memorial 850-431-1155
Quest 800-282-6613
45
How to Access Log in Name Password
Peds E-mail
www.mail.ufl.edu Gatorlink username Gatorlink password
Shands Portal my.portal.shands.ufl.edu (Shands homepage)
Home screen for most
computers, otherwise use
link to left
Shands ID
Citrix/EPIC
citrix.shands.org Can access directly on
most computers, via link
to left, or via Portal
Shands ID
Stentor - Radiology On portal page (after
logging in), middle area
under “Clinical Applica-
tions”
Shands ID (to get onto
Portal)
SUF On-Call Schedule
(calling consults) On portal page (after
logging in), middle area
under “Clinical Tools”
Shands ID (to get onto
Portal)
Drug Reference On portal page (before
logging in), bottom left in
“Clinical Links”
No log-in needed
New Innovations
- Call Schedule
- Work Hours
- Evaluations
- Procedure Log
- Schedule
www.new-innov.com
Log-in WEEKLY for
work hrs & MONTHLY
for evals
Institution Login: ufl
Username: first letter of
first name and entire last
name (i.e. Al Gator would
be agator)
Set up yourself
Text Paging www.myairmail.com ufpeds gator
REMOTE (do it from home!)
remote.peds.ufl.edu Gatorlink username Gatorlink password
SHAREPOINT -List -PCP list -Intern guide
www.peds.ufl.edu
-Faculty & Staff
-Faculty & Staff Re-
sources
-Click Housestaff after
logging in for information
ufad\”gatorlink username” Gatorlink password If 3 blanks, put UFAD in
domain
Important Information

44
Procedure Log Remember to update frequently on New Innovations.
Required Procedures: Date Location/Supervisor’s Signature
Bag-mask ventila-
tion
Bladder catheterization
Giving immunizations
Incision and drainage of abscess
Lumbar Puncture
Neonatal endotracheal intubation
Peripheral intravenous catheter placement
Reduction of simple dislocation
Simple laceration repair
Simple removal of foreign body
Temporary splinting of fracture
Umbilical catheter placement
Venipuncture
Simulated placement of intraosseous line
Medical Knowledge
of the following:
Date Location/Supervisor’s Signature
Arterial line place-ment
Arterial puncture
Chest tube placement
Circumcision
Endotracheal intuba-tion of non-neonates
Thoracentesis
7
Patient Safety Report
How to Submit a Patient Safety Report Note: Do not press [enter ], always use [tab] or the
mouse to go to the desired field.
To report a new event, log in to the Shands portal (homepage on
hospital computers):
Click “Patient Safety Report – UF&Shands”
Select “Report an Event”: follow prompts
There is an option to place an ‘Express Report’ or you can
find the category of the incident and report it that way

8
Normal vital signs by age Temperature
36 – 38.5 UNLESS under 3 months, immunocompromised or
HEME/ONC - fever is 38 for them!
Heart Rate
Respiratory Rate
Blood Pressure
Find BP norms by age and height percentile at:
http://www.cc.nih.gov/ccc/pedweb/pedsstaff/bp.html
Age Sleeping Awake
Term -3 mo 80-160 85-205
3 mo-2 yrs 75-160 100-190
2-10 yrs 60-90 60-140
>10 years 50-90 60-100
Age Respiratory rate
Birth-6 weeks 30-60
Infant 24-40
2-6 years 22-34
6-10 years 18-30
Over 10 years 12-20
Age Wt SBP DBP
Preterm 1 40-60 20-36
Term Newborn 2-3 60-70 30-45
1 month 4 70-100 30-62
6 months 7 70-118 50-70
1 year 10 70-126 41-91
2-3 years 12-14 74-124 39-89
4-5 years 16-18 79-119 45-85
6-8 yrs 20-26 80-124 45-85
10-12 yrs 32-42 90-135 55-88
>14 >50 90-140 60-90
1-10 y/o 50thPercentile SBP=90 + (Age x 2)
5th Percentile SBP=70 + (Age x 2)
43
PROCEDURE GUIDE The procedures listed below and levels of ability in performing them are the
minimum requir ed by the Pediatr ic RRC. You will be exposed to and do
many other procedures during residency and you should document them all in
your procedure log on the ACGME website.
RRC training requirement
Patient Care and Procedural Skills: Residents must be able to competent-
ly perform procedures used by a pediatrician in general practice, including
being able to describe the steps in the procedure, indications, contraindica-
tions, complications, pain management, post-procedure care, and interpreta-
tion of applicable results. Residents must demonstrate procedural competence
by performing the following: Bag-mask ventilation Bladder catheterization Giving immunizations Incision and drainage of abscess Lumbar puncture Neonatal endotracheal intubation Peripheral intravenous catheter placement Reduction of simple dislocation Simple laceration repair Simple removal of foreign body Temporary splinting of fracture Umbilical catheter placement Venipuncture Complete training and maintain certification in PALS including
simulated placement of an intraosseous line and Neonatal Resusci-tation
Medical Knowledge: Residents must be competent in the under standing
of the indications, contraindications, and complications for the following: Arterial line placement Arterial puncture Chest tube placement Circumcision Endotracheal intubation of non-neonates Thoracentesis
http://www.acgme.org/acgmeweb/Portals/0/PFAssets/2013-PR-FAQ-PIF/320_pediatrics_07012013.pdf
42
PROCEDURE NOTES:
Lumbar puncture
Date/Time:
Indication:
Consent on chart:
Infant draped and prepped in sterile fashion. 22 g myelonate
spinal needle inserted between L 4-5.
On attempt #; yielded approximately ______ mL clear/ se-
rosanguiness/xanthochromic CSF.
Pt tolerated procedure well with minimal blood loss and no
complications.
Labs sent for:
Tube 1: G-stain, Cult, AFB/fungal stain
Tube 2: Glucose, protein
Tube 3: Special (HSV PCR)
Tube 4: Cell count, diff.
Intubations:
Date/Time:
Infant intubated with ______ETT and _____ blade on _____
attempt. Equal breath sounds heard bilaterally and color change
seen on CO2 detector. ETT taped at _____ cm at lip. CXR
obtained to confirm placement.
Circumcision:
Date/Time:
Indication: Phimosis, unwanted foreskin
Consent: Obtained and on chart
Time out preformed. 1% lidocaine (1.5 ml) used for DPNB.
Infant prepped and draped in sterile fashion. Gomco 1.1/1.3
used to perform circumcision. Estimated blood loss < 5 ml.
Infant tolerated procedure well. Aftercare instructions given to
mother.
9
Top 10 Reading List—Common Pediatric Diagnoses
Pneumonia
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3202323/
Asthma
http://pedsinreview.aappublications.org/content/30/10/375
Acute bronchitis/bronchiolitis
http://pedsinreview.aappublications.org/content/30/10/386
Skin and subcutaneous tissue infections http://www.uptodate.com/
contents/evaluation-and-management-of-suspected-methicillin-
resistant-staphylococcus-aureus-skin-and-soft-tissue-infections-in-
children?
source=search_result&search=soft+tissue+infections&selectedTitl
e=9%7E150
Epilepsy
http://pediatrics.aappublications.org/content/127/2/389.full.html
Urinary tract infections
http://pediatrics.aappublications.org/content/early/2011/08/24/
peds.2011-1330
Otitis Media
http://pediatrics.aappublications.org/content/early/2013/02/20/
peds.2012-3488.abstract
Pharyngitis
http://circ.ahajournals.org/content/119/11/1541.full.pdf
ADHD
http://pediatrics.aappublications.org/
content/128/5/1007.full.pdf+html?sid=f19cb249-15a2-429b-9860-
92f2231d079b

10
Typing H&Ps/Discharge Summaries/Progress Notes
1) Log into patient’s chart and click on “Note” tab on left side
2) Find appropriate tab for work type (H&P, D/C Summary, etc)
3) Click on either New Note or Notewriter
4) Select appropriate template for work type - most have the
phrase SH IP PED _________(work type). Some services
have their own templates
5) Fill out entire template being sure to not miss any *** or
{bracketed areas}
6) You may use the partial dictation function (see above) at any
point
7) Indicate service team at the top of note, along with co-signing
physician (if you don’t indicate a co-signing physician your
note cannot be finalized)
8) Click “Accept” at bottom of note to finalize - if you click
“Pend” you can return and make changes without having to
create an “Addendum” but your note will remain hidden from
others
9) If you have any questions you may call 265-0526 (50526) at
any time for IT/EPIC assistance
Partial EPIC Dictations
1) Use the headset placed at dictation/PC terminal
2) In New Note or Notewriter, place cursor in area you want to
dictate
3) Click the “Blue microphone” on the toolbar
4) Click the “Record” button the player that appears
5) State and spell the patient’s full name, date of service, and
CSN
6) Dictate the partial dictation (Note: If you rewind and record,
you will overwrite you dictation)
7) Click “Accept” on the player. Dictation link will appear on
the document.
41
Supervision/When to Call?
SUPERB - Guide for Attending Supervision
S - Set expectations for when to be notified
U - Uncertainty is a time to contact
P - Planned communication
E - Easily available
R - Reassure resident not to be afraid to call
B - Balance supervision and autonomy for resident
___________________________________________________________
SAFETY - Resident Guide for Attending Input
S - Seek attending input early (prevents delays, quicker results)
A - Active clinical decisions (surgery, invasive procedure, etc)
F - Feel uncertain about clinical decisions
E - End of life care or family/legal discussions
T - Transitions of care (PICU, discharges, hospital transfers)
Y - You need help with the system/hierarchy (attending to attend-
ing discussions, etc)
Farnan, J.M. et al. Strategies for Effective On-Call Supervision for Internal Medicine Resi-dents: The SUPERB/SAFETY Model. Journal of Graduate Medical Education. 2010 March; 2(1): 46–52

40
Resident Concern Flow sheet
Patient Safety Risk Hotline: (352)538-2635
11
EPIC HELP emr .med.ufl.edu/training
EPIC from Home http://net-services.ufl.edu/provided_services/
vpn/anyconnect/
https://mycitrix.shands.org
EPIC Order sets for Pediatrics:
Failure to Thrive Physician’s Orders IP UF
Pediatric Bronchiolitis Physician's Orders IP UF
Pediatric Acute Gastroenteritis Physicians Orders IP UF
Discharge Pediatrics UF
Pediatric Cellulitis Physicians Orders IP UF
ALTE (Acute Life Threatening Event) Peds
Pediatric Fever without a Source: Infants 0-28 days old and high
risk infants 28-90 days old
Pediatric Pain Intervention Orders (Admission Supplement) IP UF
Pediatric Admission Order Set for Asthma IP UF
Pediatric IMC and Floor Admission Orders IP UF
Pediatric PICC Orders IP UF
Pediatric UTI (Urinary Tract Infection)/Pyelonephritis
Pediatric Pneumonia/Empyema
Pediatric NAT (Nonaccidental Trauma)
Pediatric Hyperbilirubinemia Order Set (for the floor
Failure to Thrive Physician’s Orders IP UF
Pediatric Bronchiolitis Physician's Orders IP UF
Pediatric Acute Gastroenteritis Physicians Orders IP UF
Discharge Pediatrics UF
Pediatric Cellulitis Physicians Orders IP UF
12
City County Lake Butler Union Alachua/Archer Alachua Lake City Columbia Bell Gilchrist Lawtey Bradford Belleview Marion Leesburg Lake Cedar Key/Chiefland Levy Live Oak Suwannee Cross City Dixie Mayo Lafayette Crystal River Citrus Melrose Alachua/Putnam Deland Volusia Micanopy/Newberry Alachua Dunnellon Mareion Ocala /Oklawaha Marion Fort White Marion Old town Dixie Hawthorn/ High Springs Alachua Palatka Putnam Interlachen Putnam Starke Bradford Inverness Citrus Trenton Gilchrist Jacksonville Duval Waldo Alachua Jasper/Jennings Hamilton Wildwood Sumter LaCross Alachua Williston Levy
39
Rotation/Shift Duty Hour Type
4200 days without overnight call Shift
4200 days with overnight call 1st 24 hours = Call
Hours 24-30 = Call/No new patients after 24
hours
Cards/GI Selective Shift
Time off between shifts (i.e. Acute AM
then PAH at night)
Break during shift/rotation

38
Rotation/Shift Duty Hour Type
Wards-Weekday, short Call Shift
Wards-Weekday, no short call Shift
Wards-Weekend, long call 1st 24 hours = Call
Hours 24-30 = Call/No new patients after 24 hours
Wards-Weekend, Sunday NF 1st 24 hours = Call
Hours 24-30 = Call/No new patients after 24 hours
Wards-Weekday Night Float Shift
NICU-Weekday Shift
NICU-Weekday NF Shift
NICU-Weekend (Friday or Saturday) 1st 24 hours = Call
Hours 24-30 = Call/No new patients after 24 hours
NICU-Weekend, Sunday NF 1st 24 hours = Call
Hours 24-30 = Call/No new patients after 24 hours
PICU-Weekday Shift
PICU-Weekday NF Shift
PICU-Weekend (Friday or Saturday) 1st 24 hours = Call
Hours 24-30 = Call/No new patients after 24 hours
PICU-Weekend, Sunday NF 1st 24 hours = Call
Hours 24-30 = Call/No new patients after 24 hours
Newborn Nursery-Weekday or Weekend Shift
Back-up Call, not called in Back-up
Back-up Call, called in Log according to what you were called in for
Annual Leave Vacation/Leave
Sick Leave Sick
Conference Leave Education Leave
Continuity Clinic Continuity Clinic
Acute clinic Shift
PAH, no phone calls Shift
PAH, with phone calls Shift (log only the hours you were in clinic, do not
log phone call hours)
ED Shift
Adolescent Rotation Hours
Development Rotation Hours
Advocacy Rotation Hours
Elective Rotation Hours
Moonlighting (PAH or Abstracting) Moonlighting
Administrative Time (i.e. Time between
adolescent clinic in the AM and AR at
night, etc.)
Rotation Hours
Duty Hour Type by Rotation
13
Daily Presentations
Presentations can be problem-based vs system-based (varies from
attending to attending and from service to service)
For all general patients, please use the PBAR format:
- P = Problem (Chief complaint/problem)
- B = Background (History, overnight events, PE, labs)
- A = Assessment (Assessment of how patient is doing)
- R = Recommendations (Plan)
Each patient can have multiple problems, so go through each one
individually (always include disposition as the last problem)
New admissions will still need more information (what led up to
admission, HPI, etc), compared to those that have been in the hos-
pital for a couple days
This is similar to the SBAR format nurses use to communicate to
one another and should be using to communicate with physicians
(S = Situation instead of Problem)
Medical students are taught the PBAR method, so model this
while they rotate through Pediatrics
The “New” Patient The “Old” Patient
1 line: Identifying information and reason for admission
HPI
PBAR
The last problem is always disposition
1 line: Identifying information and recap of hospitalization
PBAR The last problem is always
disposition
The “new” patient vs. The “old’ patient

14
© 2011 I-PASS Study Group/Children’s Hospital Boston
All Rights Reserved. For Permissions contact [email protected]
I Illness Severity Stable, “watcher,” unstable
P Patient Summary Summary statement
Events leading up to admission Hospital course Ongoing assessment Plan
A Action List To do list Timeline and ownership
S Situation Aware-ness & Contin-gency Planning
Know what’s going on
Plan for what might happen
S Synthesis by Re-ceiver
Receiver summarizes what was heard
Asks questions
Restates key action/to do items
37
How to Log Duty Hours?
Log-on to www.new-innov.com and click Client Login
Enter ‘ufl’ for Institution, username and password are same
as your Gatorlink
Select either Log My Hours on the middle-right side of the
screen or from the drop-down menu (under Main), select Du-
ty Hours
Enter Duty Hours corresponding to the rotation/shift you
worked (see key on next page)
Enter Duty Hours on a daily basis
If there are any work hour violations, residents must leave a
comment explaining why the violation occur red (it will
then be reviewed by Chief Residents and Program Director)
Residents not entering their duty hours by Tuesday of each
week, will start to receive reminder emails that will also be
sent to the Chief Residents and Program Directors
Please be truthful when entering duty hours - we all must
abide by the ACGME Work Hours and want to know if there
are rotations/areas where residents aren’t meeting the require-
ments

36
Ag
e
La
ng
ua
ge
F
ine
mo
tor
Gro
ss
mo
tor
Ps
yc
ho
so
cia
l
1
mo
Ale
rts to
so
un
d,
cri
es
Han
ds tig
htly fis
ted
H
ea
d u
p in
pro
ne
R
eg
ard
s f
ace
, fo
llow
s
2
mo
Sm
ile
s s
ocia
lly
Reta
ins r
attle
(b
riefly)
if p
laced
in
ha
nd
Che
st
up
in
pro
ne
, H
old
s h
ead
m
idline
sm
ile
s s
ocia
lly,
tra
cks p
ast
mid
line
, re
ga
rds h
an
ds
3
mo
Coo
s
Hold
s h
an
ds o
pe
n a
t re
st
Su
pp
ort
s o
n fo
rearm
s in
pro
ne
p
ositio
n,
hold
s h
ea
d u
p s
tea
dily
Rea
ch
es f
or
ob
jects
, a
ntici-
pa
tes f
ee
din
g
4
mo
La
ug
hs,
ori
en
ts t
o v
oic
e
Gra
sp
s &
re
tain
s,
bri
ng
s h
an
ds
to m
idlin
e
No h
ea
d la
g, ro
lls f
ron
t to
ba
ck,
rolls
ba
ck t
o fro
nt b
y 5
mo
En
joys lo
okin
g a
rou
nd
, sm
iles
sp
on
t. b
y 5
mo
6
mo
Ba
bb
les, a
h-g
oo
, ra
zz, la
tera
l o
rien
tatio
n t
o b
ell
Tra
nsfe
rs o
bje
ct
ha
nd
to
ha
nd
, im
ma
ture
ra
ke
Sits-p
rop
s o
n h
an
ds, p
uts
fee
t in
m
ou
th,
sits w
ith
ou
t h
elp
by 7
mo
Reco
gniz
es m
oth
er,
loo
ks t
o
flo
or
wh
en
ob
ject
dro
ps
9
mo
Ma
ma
/Da
da
no
nsp
ecific
, G
estu
res, u
nd
ers
tan
ds "
no
" C
ub
e h
eld
with
th
um
b &
fin
ge
r tip
s, im
ma
ture
pin
ce
r gra
sp
, h
old
s b
ottle
, th
row
s o
bje
cts
Pu
lls t
o s
tan
d,
cre
ep
s o
n h
an
ds
& k
ne
es,
piv
ots
wh
en
sittin
g,
cru
ise
s a
t 10
mo
, sta
nd
s a
t 1
1
Str
an
ge
r a
nxie
ty,
take
s s
olid
s,
wa
ve
s b
y-b
ye
by 1
0 m
o,
pe
ek
-a-b
oo
12
mo
2 w
ord
s (
no
t m
a/d
ad
a),
one-
ste
p c
om
ma
nd
with
ge
stu
re
Fin
e p
incer
gra
sp
, m
ark
s w
ith
cra
yo
n,
rele
ase
s v
olu
nta
rily
Walk
s
Se
pa
ratio
n a
nxie
ty,
dri
nks
fro
m c
up
with
help
15
mo
3-5
wo
rds,
ma
ture
ja
rgo
nin
g,
po
ints
to
bod
y p
art
2 c
ub
e t
ow
er
at
14
mo
& 3
cu
be
s a
t 1
6 m
o
Walk
s w
ell
at 1
4 m
o a
nd
ba
ck-
wa
rd/r
un
s a
t 1
6 m
o
So
lita
ry p
lay,
dri
nks f
rom
cu
p
co
op
era
tes w
ith
dre
ssin
g
18
mo
10
-25
wo
rds,
po
ints
to
3 b
od
y
pa
rts
4 c
ub
e t
ow
er,
scri
bb
les,
turn
s
2-3
pa
ge
s a
t a
tim
e
Th
row
s b
all,
ha
nde
dn
ess d
evel-
op
s
Hug
s p
are
nts
, u
se
s s
po
on
2
yrs
1/2
of
sp
ee
ch
is in
telli
gib
le, 2
w
ord
se
nte
nce
s,
2 s
tep
co
m-
ma
nd
s,
50
+ w
ord
s
6 c
ub
e t
ow
er,
ca
n d
raw
, u
nzip
s
zip
per
Kic
ks b
all,
thro
ws o
ve
rha
nd
, w
alk
s d
ow
n s
tair
s
Kis
se
s w
ith
pu
cke
r, r
em
ove
s
ga
rme
nt,
pa
ralle
l pla
y,
op
en
s
do
or,
cop
ies p
are
nts
in
ta
sks
3
yrs
3/4
sp
ee
ch
is inte
lligib
le,
3
wo
rd s
en
ten
ce
s,
na
me
s 1
co
lor,
25
0+
wo
rds
10
cu
be
to
we
r, c
an d
raw
cir
cle
, d
ries h
an
ds if
rem
ind
ed
Bro
ad
ju
mp
, ri
de
s tri
cycle
, b
ala
nce
s o
n o
ne
foo
t fo
r 1
-2 s
ec,
up
sta
irs w
ith
rail/
alt.
fee
t
Pu
ts o
n s
om
e c
loth
ing
, gro
up
p
lay, ta
ke
s t
urn
s,
un
dre
sse
s,
kn
ow
s f
ull
na
me
, g
en
de
r, a
ge
4
yrs
10
0%
in
telli
gib
le s
pe
ech,
4
wo
rd s
en
ten
ce
s,
kn
ow
s c
olo
rs,
kn
ow
s 4
pre
po
sitio
ns
Can
dra
w +
, d
raw
s a
pe
rso
n
with
3 p
art
s
Walk
up
& d
ow
n s
tair
s w
ith
rail
&
altern
atin
g f
ee
t, b
ala
nce
1 f
oo
t fo
r 3-4
se
c,
hop
, ca
tch
ball
Dre
sse
s w
ith
ou
t h
elp
, pla
ys
co
op
era
tive g
am
es,
bu
tto
ns,
tells
a s
tory
5
yrs
5 w
ord
se
nte
nce
s,
cou
nts
5-1
0
blo
cks, d
efin
es 5
fa
mili
ar
wo
rds,
kn
ow
s o
pp
osite
s
dra
w t
ria
ngle
/pers
on
(5-6
p
art
s),
pri
nts
a f
ew
le
tters
/ firs
t n
am
e,
tie
s s
ho
es
Walk
s u
p &
do
wn
sta
irs w
ith
ou
t ra
il, b
ala
nce
s o
n o
ne
fo
ot
for
5-
10
se
c,
skip
s
Pla
ys b
oard
ga
me
s,
follo
w
rule
s, lik
es t
o h
elp
in
hou
se
-h
old
ch
ore
s
Development Chart
15
I-PASS Handoff Essentials Better handoffs. Safer Care
Structured Verbal Handoff Begin with overview of entire service Need proper environment – limit interruptions Use IPASS mnemonic Employ closed loop communication
Printed Handoff Document Supplements verbal handoff May import elements from EMR Keeps information current with updates
High Level Skills Patient Summary Be concise and focused Establish working diagnosis Include semantic qualifiers Ensure check-back with receiver
Contingency Plans – “If this happens, then…” Problem solve before things go wrong Know potential therapies or interventions Identify most worrisome patients Articulate chain of command
© 2011 I-PASS Study Group/Children’s Hospital Boston
All Rights Reserved. For Permissions contact [email protected]

16
Ca
teg
ory
0
po
ints
1
po
int
2 p
oin
ts
3 p
oin
ts
Beh
avio
r
•Pla
yin
g
•Ap
pro
pri
ate
for
pat
ient
•Sle
epin
g
•Irr
itab
le &
con
sola
ble
•Irr
itab
le o
r ag
itat
ed &
is
not
con
sola
ble
•Let
har
gic
or
con
fuse
d
•Red
uce
d p
ain
re
spon
se
Ca
rd
iova
scu
lar
•Pin
k
•Cap
illa
ry r
efil
l 1
-2
seco
nd
s
•Pal
e
•Cap
illa
ry r
efil
l 3
sec
ond
s
•Gre
y
•Cap
illa
ry r
efil
l 4
sec
-on
ds
•Tac
hyca
rdia
of
20
above
norm
al r
ate
•Gre
y &
mott
-le
d
•Cap
illa
ry r
efil
l
≥ 5
sec
ond
s
•Tac
hyca
rdia
30 a
bove
nor-
mal
rat
e
•Bra
dyca
rdia
for
age
Resp
ira
tory
•Wit
hin
norm
al
par
amet
ers
•No r
etra
ctio
ns
•>1
0 a
bove
norm
al p
aram
e-te
rs
•Usi
ng a
cces
sory
mu
scle
s
•24-4
0%
FIO
2 o
r ≥
2 L
/min
O2
•An
y i
nit
iati
on o
f O
2
•> 2
0 a
bove
norm
al
par
amet
ers
•R
etra
ctio
ns
•>4
0%
FIO
2 o
r ≥
3 L
/min
O
2
•5 b
elow
nor-
mal
par
amet
ers
wit
h r
etra
ctio
ns
•G
run
tin
g
•≥ 5
0%
FIO
2 o
r
≥ 8
L/m
in O
2
Pediatric Early Warning Score (PEWS) System
35
Synagis Guidelines
(non-CLD)
34
20
14
-1
5 U
F P
ED
IAT
RIC
CL
INIC
VA
CC
INE
SC
HE
DU
LE
Bir
th/
Nu
rse
ry
2 m
o
4 m
o
6 m
o
12
mo
1
5 m
o
18
mo
2
yrs
4
-6 y
rs
11
-12
yrs
1
5 y
rs
18
yrs
HB
V
Pe
dia
rix
(DT
aP
+IP
V+
HB
V)
Pe
dia
rix
(DT
aP
+IP
V+
HB
V)
Pe
dia
rix
(DT
aP
+IP
V+
H
BV
)
DT
aP
Kin
rix
(DT
ap
+IP
V)
Td
ap
Ad
ace
l (>
11
yrs
) B
oo
str
ix
(> 1
0 y
rs)
Td
ap
ca
tch
up
>
12
yrs
H
ib w
ith
Pe
dia
rix
Hib
wit
h
Pe
dia
rix
Hib
wit
h
Pe
dia
rix
(N
ot
ne
ed
ed
if
P
ed
va
xH
IB a
t
2 a
nd
4 m
on
th)
Hib
M
MR
Pro
qu
ad
(M
MR
+V
ari
v
ax)
P
revn
ar
(PC
V1
3)
Pre
vn
ar
(PC
V1
3)
Pre
vn
ar
(PC
V1
3)
Pre
vn
ar
(PC
V1
3)
Va
riva
x
Va
riva
x C
atc
h u
p >
6 y
r o
f a
ge
(3
mth
s a
pa
rt till
ag
e 1
3 y
rs t
he
n 4
wks
ap
art
)
Ro
tari
x 1
/ R
ota
teq
1
(6 w
k -
14
wks
6 d
ys)
Ro
tari
x 2
/
Ro
tate
q 2
Ro
tate
q 3
(< 8
mo
nth
s 0
da
ys)
Hep
A
Hep
A
(6 m
ths a
fte
r
1st
do
se
)
H
ep
A c
atc
h u
p >
2 y
rs
M
en
actr
a
(MC
V4
)
Me
na
ctr
a (
MC
V4
) B
oo
ste
r
- a
t 1
6 y
rs, if fir
st d
ose
be
-tw
ee
n 1
1-1
2 y
rs
- a
t 1
6-
18
yrs
, if fir
st
do
se
be
twe
en
13
-15
yrs
Ga
rda
sil
[Gir
ls &
B
oys]
(H
PV
) 0
-2-6
m
ths
(24
wks
be
twe
en
d
ose
1 a
nd
3)
F
lu-M
ist:
IN
, 2
- 4
9 y
rs h
ealth
y,
Ju
ly -
Ma
y,
0.1
ml e
ach
no
str
il
F
lu-S
ho
t: I
M >
6 m
ths,
Se
p -
Ma
y,
0.2
5 m
l fo
r 6
mth
s
Flu
-Sh
ot:
Se
p -
Ma
y,
0.5
ml fo
r >
3 y
ea
rs
Flu
va
ccin
e: 2
do
se
s a
t le
ast
4 w
ks a
pa
rt f
or
ch
ildre
n <
9 y
rs r
eceiv
ing
fo
r th
e fir
st tim
e.
On
e d
ose
if
(re
ceiv
ed
2 d
ose
s o
f se
aso
nal flu
la
st ye
ar/
1 d
ose
of
se
aso
nal flu
in
tw
o p
revio
us s
ea
son
s)
and
an
y 2
00
9 H
1N
1 m
on
ova
len
t va
ccin
e
17
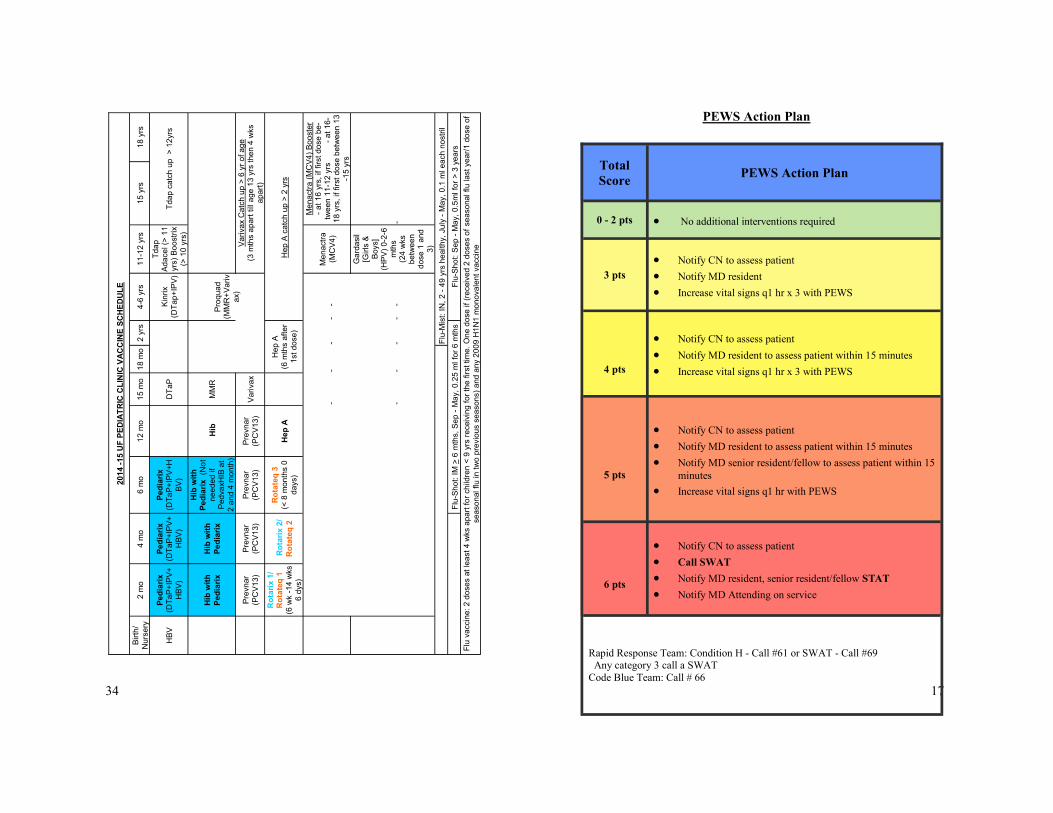
Total
Score PEWS Action Plan
0 - 2 pts No additional interventions required
3 pts
Notify CN to assess patient
Notify MD resident
Increase vital signs q1 hr x 3 with PEWS
4 pts
Notify CN to assess patient
Notify MD resident to assess patient within 15 minutes
Increase vital signs q1 hr x 3 with PEWS
5 pts
Notify CN to assess patient
Notify MD resident to assess patient within 15 minutes
Notify MD senior resident/fellow to assess patient within 15
minutes
Increase vital signs q1 hr with PEWS
6 pts
Notify CN to assess patient
Call SWAT
Notify MD resident, senior resident/fellow STAT
Notify MD Attending on service
Rapid Response Team: Condition H - Call #61 or SWAT - Call #69 Any category 3 call a SWAT
Code Blue Team: Call # 66
PEWS Action Plan

18
33
Clinic Tips Car seats:
Infants - Rear-facing seats until 2 years of age (or until
highest weight/height allowed by car seat manufacturer
reached)
Toddlers/Preschoolers - Forward-facing seats (5-point
harness) until outgrows (typically around age 4)
School-aged children - Booster seats (belt-positioning)
until 4’9” tall and between 8-12 years old
Older children - Seat belts (lap and shoulder); children
younger than 13 years old should ride in the back seat
FLSHOTS.com (keep log-in in your email!)
___________________________________________________
Anemia
Eyes: refer if >10 difference between eyes or worse than
Age 4 = 20/40
Age 5 = 20/30
Age 6 = 20/20
Age Anemia = Hgb 2 SD below
mean Mean
6mo-6yr 10.5 12
7-12yo 11 12.5
>12 ♀ 12 14
>12 ♂ 13 16

32
FEN:
Fluids- (General rules, does not always apply)
4ml/kg for each kg between 1-10kg +
2ml/kg for each kg between 11-20kg +
1ml/kg for each kg over 20kg or
Quick version for over 20 kg- just add 40 to weight
Most of time use D5 ½ NS + 10-20 meq KCl/L
- Exceptions: NS for brain tumors; no KCl for Onc pts
- ¼ NS for neonates
- NS is 154 meq/L Na and Cl
Maintenance Electrolytes-
Na+: 3meq/kg/day K+: 2meq/kg/day
Important Formulas
Anion Gap: Na – (Cl + HCO3)
Corrected Na : Na + [(glucose – 100) x 0.016]
Osmolality: 2x Na + glucose/18 + BUN/2.8
FE Na: Cr clearance:
Urine Na x serum Cr Urine Cr x urine Vol (ml)
Serum Na x urine Cr Serum Cr x time (min)
GFR estimated: PC x height (cm)/ serum Cr
(Proportionality Constant = 0.33 in LBW infants < 1 yo, 0.45 in
term infants < 1 yo, 0.55 in children 2-12, 0.55 in girls 13-21,
0.70 in boys 13-21)
GIR (glucose infusion rate): % dextrose x 10 x rate in ml/hr
60 x weight (kg)
19
NICU/NBN
Intubations:
Blade Size: 1 for term, 0 Term-30 wks, 00 < 30wks
Tape at: 6+ weight (kg)
Lines:
FEN:
Kcal/kg/day calculations:
Dextrose: ml/kg/day x % dextrose x 0.034
Lipids: ml/kg/day x 2
AA: g/kg x 4
Formulas:
GIR (glucose infusion rate): % dextrose x 10 x rate in ml/hr
60 x weight (kg)
Acid correction: For pH<7.2 OR Base deficit >10
NaHCO3 2mEq/kg/dose or ½ correction:
Base Deficit x 0.6xWt (kg)/2 Given over 30-60 minutes
Na Correction: Give ½ over 12-24 hours
[Na deficit – Na value] x weight(kg) x 0.6
ROP Guidelines: At 6 weeks. <30wks or <1500g
Car Seat Guidelines: <4 lbs= carbed, <37 wks Car seat test
HUS/MRI Guidelines: HUS 1 wk, MRI PTD. <30wks or <1250g
Synagis Guidelines: See next page
<1kg 1-2 kg 2-3 kg 3+ kg
ETT size 2.5 cm 3.0 cm 3.5 cm 3.5-4cm
UAC (Weight(kg) x 3) + 9 for T6-T9
Weight + 7 for L3-4
UVC UAC length /2 + 1
(Weight(kg) x 1.5) +5.5
20 kcal/oz 0.67 kcal/ml
22 kcal/oz 0.73 kcal/ml
24 kcal/oz 0.80 kcal/ml
20
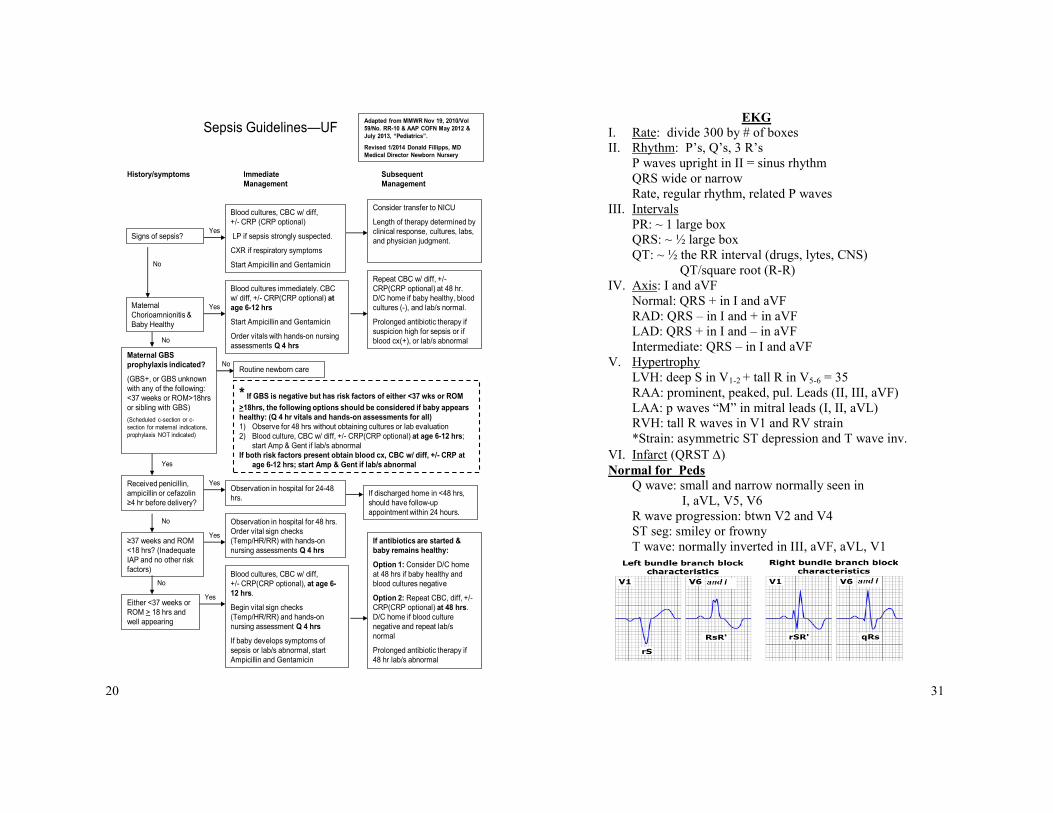
Sepsis Guidelines—UFAdapted from MMWR Nov 19, 2010/Vol
59/No. RR-10 & AAP COFN May 2012 &
July 2013, “Pediatrics”.
Revised 1/2014 Donald Fillipps, MD
Medical Director Newborn Nursery
Signs of sepsis?Yes
Blood cultures, CBC w/ diff,
+/- CRP (CRP optional)
LP if sepsis strongly suspected.
CXR if respiratory symptoms
Start Ampicillin and Gentamicin
Maternal
Chorioamnionitis &
Baby Healthy
No
Yes
Blood cultures immediately. CBC
w/ diff, +/- CRP(CRP optional) at
age 6-12 hrs
Start Ampicillin and Gentamicin
Order vitals with hands-on nursing
assessments Q 4 hrs
History/symptoms Immediate
Management
Subsequent
Management
Consider transfer to NICU
Length of therapy determined by
clinical response, cultures, labs,
and physician judgment.
Repeat CBC w/ diff, +/-
CRP(CRP optional) at 48 hr.
D/C home if baby healthy, blood
cultures (-), and lab/s normal.
Prolonged antibiotic therapy if
suspicion high for sepsis or if
blood cx(+), or lab/s abnormal
Maternal GBS
prophylaxis indicated?
(GBS+, or GBS unknown
with any of the following:
<37 weeks or ROM>18hrs
or sibling with GBS)
(Scheduled c-section or c-
section for maternal indications,
prophylaxis NOT indicated)
No
NoRoutine newborn care
Yes
Received penicillin,
ampicillin or cefazolin
≥4 hr before delivery?
YesObservation in hospital for 24-48
hrs.If discharged home in <48 hrs,
should have follow-up
appointment within 24 hours.No
≥37 weeks and ROM
<18 hrs? (Inadequate
IAP and no other risk
factors)
Yes
Observation in hospital for 48 hrs.
Order vital sign checks
(Temp/HR/RR) with hands-on
nursing assessments Q 4 hrs
Either <37 weeks or
ROM > 18 hrs and
well appearing
No
Yes
Blood cultures, CBC w/ diff,
+/- CRP(CRP optional), at age 6-
12 hrs.
Begin vital sign checks
(Temp/HR/RR) and hands-on
nursing assessment Q 4 hrs
If baby develops symptoms of
sepsis or lab/s abnormal, start
Ampicillin and Gentamicin
If antibiotics are started &
baby remains healthy:
Option 1: Consider D/C home
at 48 hrs if baby healthy and
blood cultures negative
Option 2: Repeat CBC, diff, +/-
CRP(CRP optional) at 48 hrs.
D/C home if blood culture
negative and repeat lab/s
normal
Prolonged antibiotic therapy if
48 hr lab/s abnormal
* If GBS is negative but has risk factors of either <37 wks or ROM
>18hrs, the following options should be considered if baby appears
healthy: (Q 4 hr vitals and hands-on assessments for all)
1) Observe for 48 hrs without obtaining cultures or lab evaluation
2) Blood culture, CBC w/ diff, +/- CRP(CRP optional) at age 6-12 hrs;
start Amp & Gent if lab/s abnormal
If both risk factors present obtain blood cx, CBC w/ diff, +/- CRP at
age 6-12 hrs; start Amp & Gent if lab/s abnormal
31
EKG I. Rate: divide 300 by # of boxes
II. Rhythm: P’s, Q’s, 3 R’s
P waves upright in II = sinus rhythm
QRS wide or narrow
Rate, regular rhythm, related P waves
III. Intervals
PR: ~ 1 large box
QRS: ~ ½ large box
QT: ~ ½ the RR interval (drugs, lytes, CNS)
QT/square root (R-R)
IV. Axis: I and aVF
Normal: QRS + in I and aVF
RAD: QRS – in I and + in aVF
LAD: QRS + in I and – in aVF
Intermediate: QRS – in I and aVF
V. Hypertrophy
LVH: deep S in V1-2 + tall R in V5-6 = 35
RAA: prominent, peaked, pul. Leads (II, III, aVF)
LAA: p waves “M” in mitral leads (I, II, aVL)
RVH: tall R waves in V1 and RV strain
*Strain: asymmetric ST depression and T wave inv.
VI. Infarct (QRST )
Normal for Peds Q wave: small and narrow normally seen in
I, aVL, V5, V6
R wave progression: btwn V2 and V4
ST seg: smiley or frowny
T wave: normally inverted in III, aVF, aVL, V1

30
Transfusion Guidelines
Pre-Meds:
Only if history of reaction to blood products
Most febrile reactions occur with platelets
Blood (PRBC) Transfusion:
10 – 15 mL/kg
In a stable patient with normal cardiac function, 10 mL/kg can be
transfused over 2 hours
For patients with Hct less than 15 or Hgb less than 5 and stable, rule
of thumb is to give blood slowly. The transfusion volume is
patient’s Hgb x wt in kg over 2-3 hours. Wait a few hours and
reevaluate Hct and Hgb and cardiac status; base next transfu-
sion on new data.
For patients with Hct less than 15 or Hgb less than 5 and unstable
contact Heme/Onc before transfusing
For volume depleted patients who are unstable secondary to blood
loss, infuse as rapidly as possible.
This patient should be in PICU!
1 unit PRBCs = 250 mL (at least, sometimes as much as 500ml)
1 unit PRBCs ~ 3 pedisplit units
1 pedisplit = ~80 mL
Platelets:
10mL per kg
1-2 apheresis units is the maximum
Single donor (apheresis unit) = ~ 8 random donor units
Pre-pooled platelets are the equivalent of 6-8 different donors. For
infants and toddlers random donor units are acceptable. Once
patient is getting equivalent of 4 or more random donors, ½
apheresis unit should be ordered.
Average volume of apheresis unit = ~200-250 mL
Platelets are normally hung by gravity over ~15-20 min
21
Nomogram for designation of risk >36 weeks gestation
Hyperbilirubinemia
Guidelines for therapy >35 weeks gestation
Risk of hyperbilirubinemia: Bilitool.org
22
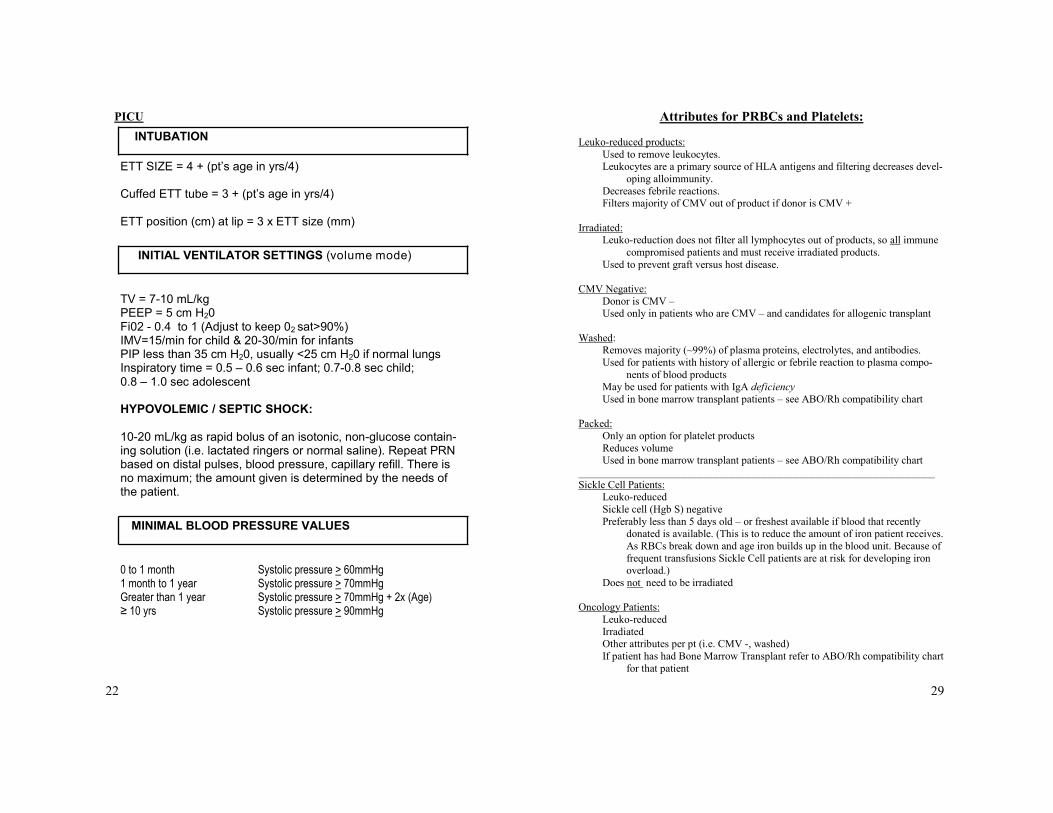
PICU
ETT SIZE = 4 + (pt’s age in yrs/4) Cuffed ETT tube = 3 + (pt’s age in yrs/4) ETT position (cm) at lip = 3 x ETT size (mm)
TV = 7-10 mL/kg PEEP = 5 cm H20 Fi02 - 0.4 to 1 (Adjust to keep 02 sat>90%) IMV=15/min for child & 20-30/min for infants PIP less than 35 cm H20, usually <25 cm H20 if normal lungs Inspiratory time = 0.5 – 0.6 sec infant; 0.7-0.8 sec child; 0.8 – 1.0 sec adolescent HYPOVOLEMIC / SEPTIC SHOCK: 10-20 mL/kg as rapid bolus of an isotonic, non-glucose contain-ing solution (i.e. lactated ringers or normal saline). Repeat PRN based on distal pulses, blood pressure, capillary refill. There is no maximum; the amount given is determined by the needs of the patient.
0 to 1 month Systolic pressure > 60mmHg 1 month to 1 year Systolic pressure > 70mmHg Greater than 1 year Systolic pressure > 70mmHg + 2x (Age) ≥ 10 yrs Systolic pressure > 90mmHg
INTUBATION
INITIAL VENTILATOR SETTINGS (volume mode)
MINIMAL BLOOD PRESSURE VALUES
29
Attributes for PRBCs and Platelets:
Leuko-reduced products:
Used to remove leukocytes. Leukocytes are a primary source of HLA antigens and filtering decreases devel-
oping alloimmunity.
Decreases febrile reactions. Filters majority of CMV out of product if donor is CMV +
Irradiated: Leuko-reduction does not filter all lymphocytes out of products, so all immune
compromised patients and must receive irradiated products.
Used to prevent graft versus host disease.
CMV Negative:
Donor is CMV – Used only in patients who are CMV – and candidates for allogenic transplant
Washed: Removes majority (~99%) of plasma proteins, electrolytes, and antibodies.
Used for patients with history of allergic or febrile reaction to plasma compo-
nents of blood products May be used for patients with IgA deficiency
Used in bone marrow transplant patients – see ABO/Rh compatibility chart
Packed:
Only an option for platelet products
Reduces volume Used in bone marrow transplant patients – see ABO/Rh compatibility chart
___________________________________________________________________
Sickle Cell Patients: Leuko-reduced
Sickle cell (Hgb S) negative
Preferably less than 5 days old – or freshest available if blood that recently donated is available. (This is to reduce the amount of iron patient receives.
As RBCs break down and age iron builds up in the blood unit. Because of
frequent transfusions Sickle Cell patients are at risk for developing iron overload.)
Does not need to be irradiated
Oncology Patients:
Leuko-reduced
Irradiated Other attributes per pt (i.e. CMV -, washed)
If patient has had Bone Marrow Transplant refer to ABO/Rh compatibility chart
for that patient
28
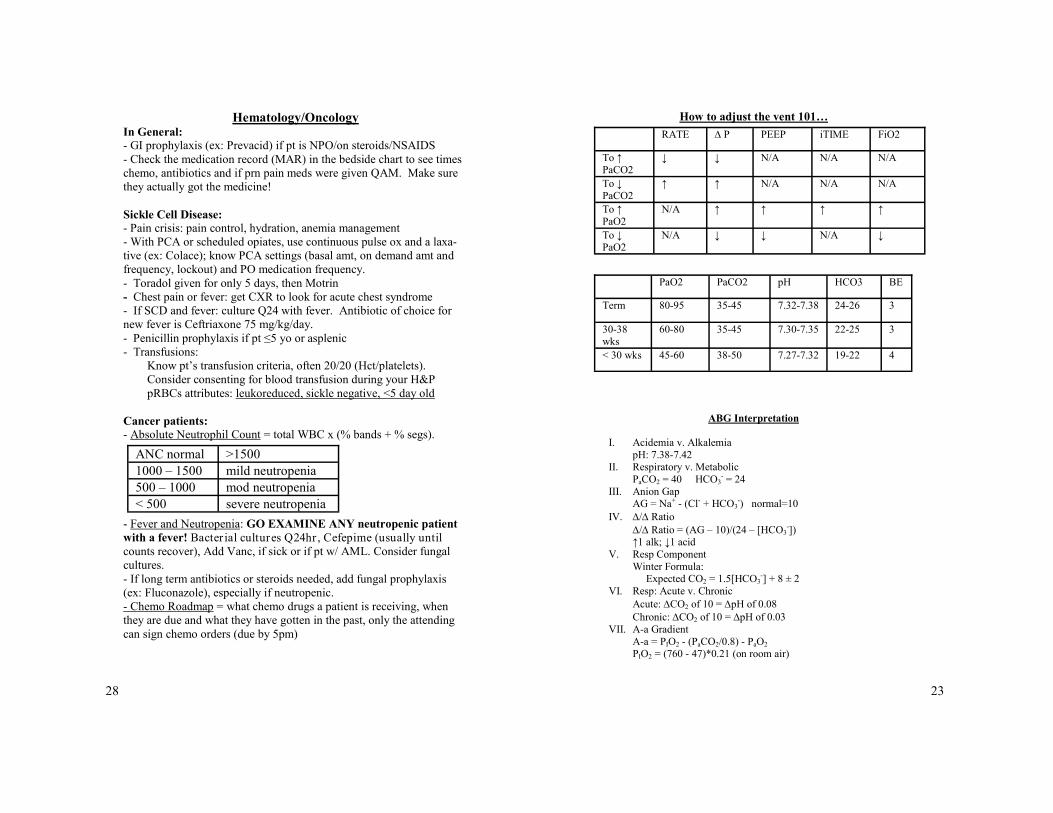
Hematology/Oncology In General:
- GI prophylaxis (ex: Prevacid) if pt is NPO/on steroids/NSAIDS
- Check the medication record (MAR) in the bedside chart to see times
chemo, antibiotics and if prn pain meds were given QAM. Make sure
they actually got the medicine!
Sickle Cell Disease:
- Pain crisis: pain control, hydration, anemia management
- With PCA or scheduled opiates, use continuous pulse ox and a laxa-
tive (ex: Colace); know PCA settings (basal amt, on demand amt and
frequency, lockout) and PO medication frequency.
- Toradol given for only 5 days, then Motrin
- Chest pain or fever: get CXR to look for acute chest syndrome
- If SCD and fever: culture Q24 with fever. Antibiotic of choice for
new fever is Ceftriaxone 75 mg/kg/day.
- Penicillin prophylaxis if pt ≤5 yo or asplenic
- Transfusions:
Know pt’s transfusion criteria, often 20/20 (Hct/platelets).
Consider consenting for blood transfusion during your H&P
pRBCs attributes: leukoreduced, sickle negative, <5 day old
Cancer patients:
- Absolute Neutrophil Count = total WBC x (% bands + % segs).
- Fever and Neutropenia: GO EXAMINE ANY neutropenic patient
with a fever! Bacter ial cultures Q24hr , Cefepime (usually until
counts recover), Add Vanc, if sick or if pt w/ AML. Consider fungal
cultures.
- If long term antibiotics or steroids needed, add fungal prophylaxis
(ex: Fluconazole), especially if neutropenic.
- Chemo Roadmap = what chemo drugs a patient is receiving, when
they are due and what they have gotten in the past, only the attending
can sign chemo orders (due by 5pm)
ANC normal >1500
1000 – 1500 mild neutropenia
500 – 1000 mod neutropenia
< 500 severe neutropenia
23
How to adjust the vent 101…
RATE ∆ P PEEP iTIME FiO2
To ↑ PaCO2
↓ ↓ N/A N/A N/A
To ↓ PaCO2
↑ ↑ N/A N/A N/A
To ↑ PaO2
N/A ↑ ↑ ↑ ↑
To ↓ PaO2
N/A ↓ ↓ N/A ↓
PaO2 PaCO2 pH HCO3 BE
Term 80-95 35-45 7.32-7.38 24-26 3
30-38 wks
60-80 35-45 7.30-7.35 22-25 3
< 30 wks 45-60 38-50 7.27-7.32 19-22 4
ABG Interpretation
I. Acidemia v. Alkalemia
pH: 7.38-7.42 II. Respiratory v. Metabolic
PaCO2 = 40 HCO3- = 24
III. Anion Gap AG = Na+ - (Cl- + HCO3
-) normal=10
IV. / Ratio
/ Ratio = (AG – 10)/(24 – [HCO3-])
↑1 alk; ↓1 acid
V. Resp Component
Winter Formula: Expected CO2 = 1.5[HCO3
-] + 8 ± 2
VI. Resp: Acute v. Chronic
Acute: CO2 of 10 = pH of 0.08
Chronic: CO2 of 10 = pH of 0.03
VII. A-a Gradient
A-a = PIO2 - (PaCO2/0.8) - PaO2 PIO2 = (760 - 47)*0.21 (on room air)

24
ASTHMA
Asthma Score 6-12:
Continuous neb Q 1h assessment
Asthma Score 2-5:
Q2h neb Q2h Assessment
Asthma Score 0-1: Hold therapy Q2h assessment
assessment
Discharge Home if:
Asthma Education Asthma Action Plan Follow up
Hold therapy Q 1h assessment Move if score is still
low X 2 Notify MD
Hold therapy Q 2h assessment Move if score is still
low X 2 Notify MD
Move if patient did not require albuterol For 4 hours
Notify MD
Give albuterol Q1hour assessment Move if score is still
highX2 Notify MD
Give albuterol Q 2h assessment Move if score is still
high X 2 Notify MD
Continue protocol if discharge criteria not fulfilled
Escalate Descalate Stable
Flowsheets available in EPIC:
Asthma Scoring System
ED PACE Asthma History
ED PACE Asthma Scoring System
27
Cystic Fibrosis
Print CF patient care form (on the portal)
Look at past H&P, D/C summaries for medication history, sputum
culture results
Airway clearance QID (Vest, CPT, IPV – ask pt what they use or
look at past hospital course/clinic notes)
Sputum culture labeled “CF sputum, extended sensitivities”
Remember annual labs (prealbumin, LFTs, PT/PTT, vitamin lev-
els) and monitoring labs (BMP if pt on Vanc, Vanc trough,
Tobra 2/8 hr levels)
Spirometry (pre- and post-bronchodilator) usually at the time of
admission (sometimes done in clinic) and then usually every
1-2 weeks until improvement seen
Consults to the appropriate services (Endo if pt has CFRD, GI/
Liver if pt has CF liver disease, Nutrition for help with nutri-
tional supplementation, and Pharmacokinetics if pt has drug
levels that will need adjusting)
PICC line consent at the time of admission (1-2 weeks of IV Abx)
ànd then fax PICC consult sheet and call PICC team (don’t
fax consult sheet w/o obtaining consent)
CXR following PICC line placement, if placement is delayed con-
sider earlier CXR
Everyday: ask pt to cough as par t of lung exam (productive?),
if CPT is in progress STOP IT with “pause” button to do exam.

26
Bronchiolitis Score
25
ASTHMA Out-patient: New Diagnosis: determine if it is asthma (if they respond to bronchodila-
tor treatment), and what type of asthma it is (intermittent or persistent)
Classification:
Treatment:
Mild Intermittent-
No daily medication
Only short acting beta agonist (Albuterol)
Mild Persistent
Low-dose inhaled corticosteroid daily (Flovent)
Short acting beta agonist (Albuterol) as needed
Moderate Persistent:
Low-dose inhaled corticosteroid (Flovent) AND long acting beta
agonist (Advair)
OR Medium dose inhaled corticosteroid
Short acting beta agonist (Albuterol) as needed
Severe Persistent
High dose inhaled corticosteroid
Long acting inhaled beta agonist
**If pt has ever been in the PICU for an asthma exacerbation
they should be followed by Pulmonary**
Mild
Intermittent Mild
Persistent Moderate
Persistent Severe
Persistent
Day ≤ 2 days/wk >2/week
but
<1/day
Daily Continual
Night ≤ 2 nights/
month >2 nights/
month >1 night/
wk Frequent
FEV1 ≥ 80% ≥ 80% 60-80% ≤ 60%