integration of a palliative approach in home, acute ... · analysis methods ... conditions that,...
TRANSCRIPT

BRITISH COLUMBIA PROVINCIAL REPORT
Integration of a Palliative Approach in Home, Acute Medical, and Residential Care Settings: Findings from a Province-Wide Survey
September 25, 2014

i
Acknowledgements iPANEL Survey Leaders:
Richard Sawatzky RN, PhD Associate Professor, School of Nursing Trinity Western University Research Scientist, Centre for Health Evaluation and Outcome Sciences Providence Health Care Research Institute Canada Research Chair – Patient‐Reported Outcomes
Della Roberts RN, MSN, CHPCN (C) Clinical Nurse Specialist, End of Life Fraser Health Authority Sheryl Reimer‐Kirkham RN, PhD Professor, School of Nursing Trinity Western University
iPANEL Leaders:
Kelli Stajduhar RN, PhD Professor, School of Nursing/ Centre on Aging University of Victoria Carolyn Tayler RN, BN, MSA, CON (C) Director, End of Life Care Fraser Health Authority Thank you to the entire iPANEL Team (www.ipanel.ca) for their contributions and leadership
throughout this endeavour. We would also like to thank all the staff at each of the participating
sites that helped with questionnaire distribution and collection.
A special thank you to the staff members who were involved with the various aspects of this
survey along the way: Ami Bitschy, Lara Russell, Melissa Suzuki, and Will Harding.

ii
Table of Contents Acknowledgements .......................................................................................................................... i
List of Tables ................................................................................................................................... iii
List of Figures .................................................................................................................................. iv
Executive Summary .......................................................................................................................... v
Background ..................................................................................................................................... 7
iPANEL & Palliative Approach ..................................................................................................... 7
Provincial Survey ......................................................................................................................... 8
Objectives................................................................................................................................ 8
Sampling strategy ................................................................................................................... 8
Description of sample ............................................................................................................. 9
Questionnaire design ............................................................................................................ 12
Analysis methods .................................................................................................................. 12
Provincial Survey Findings............................................................................................................. 13
Application of a Palliative Approach ......................................................................................... 13
Identification of patients with life‐limiting condition ........................................................... 13
Belief that patients would benefit from a palliative approach ............................................ 15
Application of a palliative approach to the care of patients ................................................ 16
Self‐Perceived Competence in Dimensions of a Palliative Approach ....................................... 18
Acute medical care settings .................................................................................................. 19
Home care settings ............................................................................................................... 20
Residential care settings ....................................................................................................... 21
Application of different dimensions of a palliative approach .............................................. 21
Knowledge and Education for a Palliative Approach ................................................................ 23
Perceived adequacy of knowledge regarding a palliative approach .................................... 23
How are nurses and HCWs learning in practice? .................................................................. 25
Conclusion ..................................................................................................................................... 27
References .................................................................................................................................... 28

iii
List of Tables Table 1 – Number and types of settings within each health authority .......................................... 9
Table 2 – Sample description of settings ...................................................................................... 10
Table 3 – Sample description of participants ............................................................................... 11
Table 4 – Percentages of low self‐competence in acute medical care settings ........................... 19
Table 5 – Percentages of low self‐competence in home care settings ........................................ 20
Table 6 – Percentages of low self‐competence in residential care settings ................................ 21
Table 7 – Application of palliative approach dimensions by nurses and HCWs ........................... 23
Table 8 – Percentage of less than adequate knowledge in a palliative approach ....................... 24

iv
List of Figures Figure 1 – Geographical distribution of surveyed settings throughout the province of BC ........... 9
Figure 2 – Visual of the survey sample description ...................................................................... 10
Figure 3 – Questionnaire content ................................................................................................. 12
Figure 4 – Patients identified as having life‐limiting conditions .................................................. 14
Figure 5 – Patients who would benefit from a palliative approach ............................................. 15
Figure 6 – Application of a palliative approach to the care of patients ....................................... 17
Figure 7 – Application of palliative approach dimensions ............................................................ 22
Figure 8 – Preferred resources for a palliative approach in practice ........................................... 25
Figure 9 – Preferred methods of education for a palliative approach ......................................... 26

v
Executive Summary Supporting people with advancing chronic and life‐limiting1 conditions will be a dominant
challenge for healthcare delivery in the next half‐century. The Initiative for a Palliative
Approach in Nursing: Evidence and Leadership (www.iPANEL.ca) is a practice‐relevant nursing
health services research initiative funded by the Michael Smith Foundation for Health Research
to inform how we can best integrate a palliative approach2 into the care of people with
advancing chronic life‐limiting conditions. This iPANEL report focuses on findings from a mixed‐
methods province‐wide survey designed to obtain baseline descriptive information relevant to
the integration of a palliative approach from Registered Nurses (RNs), Licensed Practical Nurses
(LPNs), and Healthcare Workers (HCWs) in acute medical care units, residential care facilities,
and home care settings.
The survey included 114 randomly selected healthcare settings equally drawn from a listing of
all eligible settings in five regional health authorities. A total of 1,468 RNs, LPNs, and HCWs
across urban and rural settings completed the survey questionnaire. Additionally, 25 nurses
(either RNs or LPNs), and 5 HCWs participated in follow‐up qualitative interviews.
The following summary recommendations are supported by the survey findings and provide
important information for regional health authorities regarding the integration of a palliative
approach. These findings will also inform ongoing iPANEL research into the care delivery
systems, education, and practice supports needed to integrate a palliative approach.
1. Improved recognition of the life‐limiting nature of chronic conditions is needed, most
urgently by nurses in acute medical care units, but also by nurses and HCWs in home care
and residential care settings. On average, RNs, LPNs, and HCWs in acute medical care and
home care settings identified only half of their patients as having life‐limiting conditions. In
residential care settings nurses and HCWs on average identified approximately 70% of the
residents as having life‐limiting conditions. Given the high prevalence of chronic life‐
limiting conditions in the sampled acute medical care units, a higher percentage was
expected. Similarly, given that nearly all people admitted to residential care have chronic
life‐limiting conditions, it was expected that closer to 100% of staff would recognize that
nearly all patients are on a progressive illness trajectory that will end their lives.
1Life‐limiting conditions: Chronic conditions (or illnesses) expected to limit how long a person has to live, including dementia, lung, kidney and heart diseases, and cancer. 2Palliative approach: An approach to care focused on improving the quality of life of people with life‐limiting conditions and their family. It is provided in all healthcare settings. It involves physical, psychological, social and spiritual care. The palliative approach is not delayed until the end stages of an illness but is applied earlier to provide active comfort‐focused care and a positive approach to reducing suffering. It also promotes understanding of loss and bereavement.

vi
2. There is a need for consistent application of a palliative approach for people with chronic
life‐limiting conditions in all settings. A palliative approach is not consistently applied by
all RNs, LPNs and HCWs in acute medical, home, and residential care settings. Infrequent
application of a palliative approach in acute care environments is of particular concern. RNs
and LPNs in acute care reported providing a palliative approach to only 50% of patients
who they identified as having chronic life‐limiting conditions.
3. There is a need for improved confidence and knowledge regarding a palliative approach
focussing on spiritual, psychological, social, loss & grief support needs, and ethical & legal
issues. Nurses and HCWs reported feeling least confident and knowledgeable in areas of
spiritual and social needs and ethical and legal issues. These areas are dimensions of care
addressed through conversation and relationship with patients and families. Nurses and
HCWs feel most confident in the physical care of patients, as well as in personal,
professional and inter‐professional collaboration.
4. Interactional approaches to learning that draws on expertise of colleagues, managers,
clinical coordinators and nurse specialists are foundational to the way that nurses and
HCWs learn about how to apply a palliative approach in their practice. Nurses and HCWs
rely heavily on colleagues to inform their practice of a palliative approach. In addition,
face‐to‐face learning is the most preferred method for receiving education for nurses and
HCWs across settings.

7
Background
iPANEL & Palliative Approach Although modern medicine has extended life by years, it
is still true that, inevitably, each of us lives with a set of
conditions that, taken together, are progressively
worsening and eventually fatal [2]. The rising number of
people facing old age makes it likely that supporting
persons with serious chronic and life‐limiting conditions
will be a dominant challenge for healthcare delivery in
the next half‐century [3]. The End of Life (EOL) Action
Plan for the province of BC highlights redesign of health
services to deliver timely coordinated EOL care as a
priority. The plan specifically recommends a population
approach that includes earlier identification of
individuals with life‐limiting conditions who would
benefit from a palliative approach [4].
People with life‐limiting conditions are everywhere in
our health care system. Yet, it seems that healthcare
providers are often not identifying people who are on a
dying trajectory until the last days of life [5]. Most
people with advancing chronic conditions will not have a
predictable time frame before death and may not need
specialized palliative care. The 2008 Canadian Institute
for Health Information (CIHI) report on end‐of‐life care
in BC notes that of all those who die, only 27% received
palliative care at end of life [5]. However, those living
with life‐limiting conditions such as heart, lung and
kidney disease, dementia, and cancer, along with their
families, would benefit from the application of palliative
care principles regardless of their context of care and stage in the disease trajectory. This
palliative approach to care would maximize their ability to live well while concurrently
preparing and supporting transitions that eventually will result in death. Registered nurses
(RNs), licensed practical nurses (LPNs), and healthcare workers (HCWs) are amongst those who
frequently encounter and care for patients with life‐limiting conditions in every sector of the
health care system.
WHAT IS A PALLIATIVE
APPROACH?
This is an approach that applies the principles of palliative care to the care of those living with life‐limiting conditions. This approach is congruent with disease modifying care in that they both strive to meet the physical, psychological, social, and practical needs of the ill person. However, a palliative approach considers these needs through the lens of the disease being progressive and life‐limiting.
A palliative approach recognizes that, although not all people with life‐limiting conditions require specialized palliative care services, they do require care that is aimed at improving their quality of life, by preventing and relieving suffering through early identification, assessment and treatment of physical, psychosocial and spiritual concerns [1].

8
The Initiative for a Palliative Approach in Nursing: Evidence and Leadership (www.iPANEL.ca) is
a practice‐relevant nursing health services research initiative, composed of leading
practitioners, administrators, and academics in nursing throughout the province of BC. iPANEL
is funded by the Michael Smith Foundation for Health Research BC Nursing Research Initiative.
Members of iPANEL conduct research to inform how we can best integrate a palliative
approach into the care of people with advancing chronic life‐limiting conditions.
Provincial Survey As part of the iPANEL research initiative, the team completed a mixed‐methods province‐wide
survey. The survey was designed to obtain baseline descriptive information relevant to
integration of a palliative approach from nurses (RNs and LPNs) and HCWs working in acute
medical care units, residential care facilities, and home care settings across BC. Respondents
were also given the opportunity to participate in follow‐up qualitative interviews or focus
groups regarding a palliative approach in their workplace.
Objectives
In addition to providing descriptive information, this report addresses the following questions:
1. To what extent is a palliative approach applied in different types of nursing care settings?
2. How confident are nurses and HCWs in applying palliative dimensions of care to address the
needs of people with advancing chronic life‐limiting conditions and their families?
3. To what extent do nurses and HCWs view their knowledge regarding important palliative
dimensions of care as adequate for integrating a palliative approach in practice?
4. What educational resources do nurses and HCWs rely upon to inform their practice of a
palliative approach?
Sampling strategy
A sampling frame of all relevant settings was developed in collaboration with the BC Ministry of
Health, Health Authorities and HealthLinkBC. These settings include: (a) hospital‐based medical
services, including general acute medical care units and specialized renal, respiratory, cardiac,
oncology and geriatric care units; (b) home care nursing services; and (c) residential care
facilities, excluding assisted living and non‐contracted private facilities. No specialized palliative
care units were included.
A two‐stage clustered and stratified sampling strategy was used to identify 114 randomly
selected sites from the following five health authorities in BC; Vancouver Island Health
Authority (VIHA), Fraser Health Authority (FHA), Interior Health Authority (IHA), Northern
Health Authority (NHA), and Vancouver Coastal Health Authority (VCH). The sampling strategy
ensured geographical representation of sites within each of the five regional health authorities.

9
The sampling was stratified by type of site (acute medical care units, residential care facilities,
and home care settings), size of site (based on a median split of the sizes of sites within each
health authority), and, for acute medical care units, whether the site was a specialized or
general medical unit. This approach ensured that different types of sites were represented in
the sample.
Description of sample
Sample of surveyed settings: The provincial survey was completed in 2 phases – in Figure 1 the
blue dots represent the 59 sites surveyed in phase I and the orange dots represent the 55 sites
surveyed in phase II. A breakdown of selected sites per setting and health authority can be
seen in Table 1. Descriptive information about the sample of settings is provided in Table 2.
Figure 1 – Geographical distribution of surveyed settings throughout the province of BC
Table 1 – Number and types of settings within each health authority
TYPE OF SETTING
FHA IHA NHA VCHA VIHA TOTAL
Home Care 8 8 6 7 8 37Acute Medical 8 8 7 8 8 39
Residential 8 8 7 7 8 38
Total 24 24 20 22 24 114
10
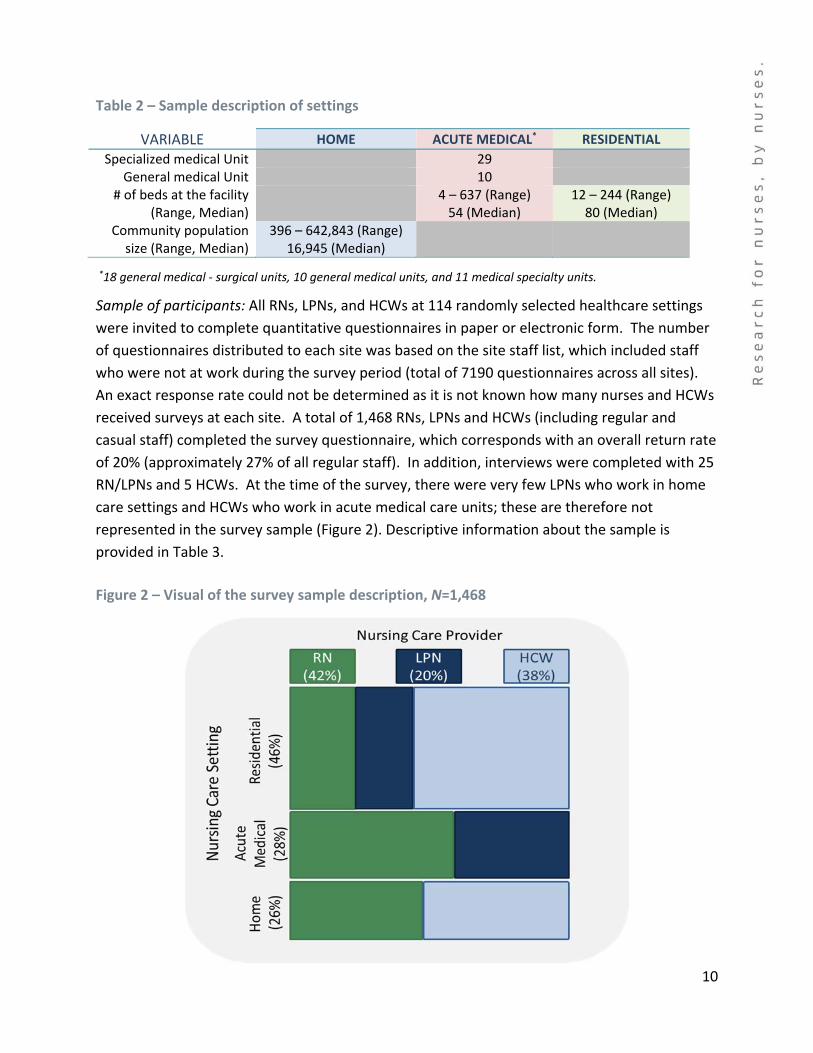
Table 2 – Sample description of settings
VARIABLE HOME ACUTE MEDICAL* RESIDENTIAL
Specialized medical Unit 29 General medical Unit 10
# of beds at the facility (Range, Median)
4 – 637 (Range) 54 (Median)
12 – 244 (Range) 80 (Median)
Community population size (Range, Median)
396 – 642,843 (Range) 16,945 (Median)
*18 general medical ‐ surgical units, 10 general medical units, and 11 medical specialty units.
Sample of participants: All RNs, LPNs, and HCWs at 114 randomly selected healthcare settings
were invited to complete quantitative questionnaires in paper or electronic form. The number
of questionnaires distributed to each site was based on the site staff list, which included staff
who were not at work during the survey period (total of 7190 questionnaires across all sites).
An exact response rate could not be determined as it is not known how many nurses and HCWs
received surveys at each site. A total of 1,468 RNs, LPNs and HCWs (including regular and
casual staff) completed the survey questionnaire, which corresponds with an overall return rate
of 20% (approximately 27% of all regular staff). In addition, interviews were completed with 25
RN/LPNs and 5 HCWs. At the time of the survey, there were very few LPNs who work in home
care settings and HCWs who work in acute medical care units; these are therefore not
represented in the survey sample (Figure 2). Descriptive information about the sample is
provided in Table 3.
Figure 2 – Visual of the survey sample description, N=1,468

11
Table 3 – Participant demographic information1
VARIABLE HOME2
ACUTE MEDICAL3
RESIDENTIAL TOTAL* (%)
HCW RN LPN RN HCW LPN RN
Distribution across settings (%)
6 6 6 20 32 15 16 100
Gender (%)
Male 5 2 9 15 13 9 7 10
Female 95 98 91 85 87 90 93 90
Highest level of education (%)High school 5 6 2 Certificate 67 3 5 75 1 29
Licensed practical nurse 3 88 1 92 19 Registered nurse 2 49 4 30 2 45 16 Bachelor's degree 1 42 57 1 50 21 Master's in nursing 2 1 1 1 1
Other 23 5 3 13 16 2 5 11
Employment status (%)
Full‐time 29 19 34 13 18 22 19 19 Part‐time 23 36 13 24 21 11 24 21
Casual 49 45 53 64 60 68 58 60
Age (in years)
Mean (standard deviation) 50 (10) 50 (9) 44 (10) 38 (12) 46 (11) 40 (11) 51 (11) 45 (12)Range 22 – 67 26 – 65 22 – 62 20 – 66 20 – 68 20 – 64 24 – 75 20 – 75
Note. The percentages represent “weighted” population estimates based on the information provided by the provincial sample of 1,433 participants. 1 Missing sample data were 9% for gender, 10% for education, 1% for employment status, and 12% for age. 2,3 There were few LPNs in home care, and HCWs in acute medical care units at the time of this survey. These provider groups/setting are therefore not included in the analysis. * Numbers may not necessarily sum to 100 due to rounding.

12
Questionnaire design
The questionnaire was designed to obtain information about the perspectives of nurses and
HCWs regarding their confidence, knowledge, and application of a palliative approach, as well
as information about their work environment and demographics (Figure 3).
Figure 3 – Questionnaire content
1 Some questions were modified for Healthcare Workers 2 Adapted from the 2005 National Survey of the Work and Health of Nurses 3 Data on work environment is not provided in this report.
Analysis methods
Herein, we report the descriptive analyses that address the objective questions outlined on
page 8. All statistical analyses have been proportionally weighted to accommodate the
stratified and clustered sampling design. These statistics therefore describe the overall
province. Qualitative methods of analysis were used to identify common themes arising from
the transcribed interviews and focus group data.

13
Provincial Survey Findings The following provides key information relevant to the application of a palliative approach. The findings are reported for the provincial nurses and HCWs in acute medical care, residential care, and home care settings.
Application of a Palliative Approach This section of the report addresses the question: To what extent is a palliative approach
applied in different types of nursing care settings? Participants were asked the following 3
questions:
1. In your practice setting, how many patients out of ten have life‐limiting conditions?
2. In your practice setting, how many out of ten of the patients with life‐limiting conditions
would benefit from a palliative approach to care?
3. How often do you apply a palliative approach to your care of persons with life‐limiting
conditions?
Identification of patients with life‐limiting condition/s
On average across the BC settings, nurses and HCWs in Acute medical care units and Home care
settings indicate that 5 of ten (or 50%) of their patients have life‐limiting conditions. A greater
proportion, 7 of 10 (70%), of patients in Residential care settings are identified as having life‐
limiting conditions. Across the province, RNs, LPNs, and HCWs were relatively similar within
each setting type (i.e., home, acute medical, residential).
These findings indicate the need for improvement in recognition of the life‐limiting nature of
chronic conditions by nurses and HCWs. It was expected that a greater percentage of patients
would have been identified as having life‐limiting chronic conditions. For example, nearly all
people admitted to residential care have chronic life‐limiting conditions, and it would therefore
be expected that closer to 100% would have been identified as such.

14
Figure 4 – Patients identified as having life‐limiting conditions1,2
1Participants were asked, “In your practice setting, how many patients out of ten have life‐limiting conditions?” 2Missing data for the BC sample across all providers and settings was 7%.
Qualitative findings shed light on the factors that influence how patients are identified with life‐
limiting conditions or as “palliative” by nurses in particular settings. One factor revolves around
how the term “palliative” is understood and/or used within each practice setting. Several home
care participants indicated the term “palliative” is reserved for people referred for services (i.e.,
a physician has indicated their prognosis is last months of life and has enrolled the patient in
the BC Palliative Benefits Program). Some acute medical participants noted the term
“palliative” is a designation assigned by the physician indicating a change in the goals of care to
supportive or “comfort care”, whereas those in residential care indicated that the term
“palliative” typically refers to the last days of life or the actively dying time. Another factor was
related to how the person was viewed within the different clinical contexts. A clinical context in
which treatment is paramount makes it more difficult for nurses to recognize a chronic
condition as life‐limiting.
# of patients out of 10

15
Belief that patients with life‐limiting conditions would benefit from a palliative approach
There is substantial variability in the extent to which nurses and HCWs believe that a palliative
approach would be beneficial for their patients with life‐limiting conditions. On average, nurses
and HCWs in BC reported that between 50% and 74% of their patients with life‐limiting
conditions would benefit from a palliative approach (Figure 5). RNs and LPNs in acute medical
care units are relatively less likely to do so.
Figure 5 – Patients with life‐limiting conditions who would benefit from a palliative approach1,2
1Participants were asked, “In your practice setting, how many out of ten patients with life‐limiting conditions would
benefit from a palliative approach to care?” 2Missing data for the BC sample across all providers and settings was 9%.
The finding that not all nurses and HCWs believe that a palliative approach would be beneficial
to patients with chronic life‐limiting conditions is important and requires further exploration.
# of patients out of 10

16
The expectation had been that participants would indicate that all of their patients with life‐
limiting conditions could benefit from a palliative approach.
Qualitative findings provide some additional insight. The importance of the inter‐professional
team context in relation to identifying individuals who would benefit from a palliative approach
was highlighted in the interviews. For example, some HCWs expressed that they do not have a
strong voice within the inter‐professional team regarding palliative needs or care planning.
One HCW described not being part of the formalized care planning despite working closely with
the residents: “even when they do annual reviews for the residents, we are not present”.
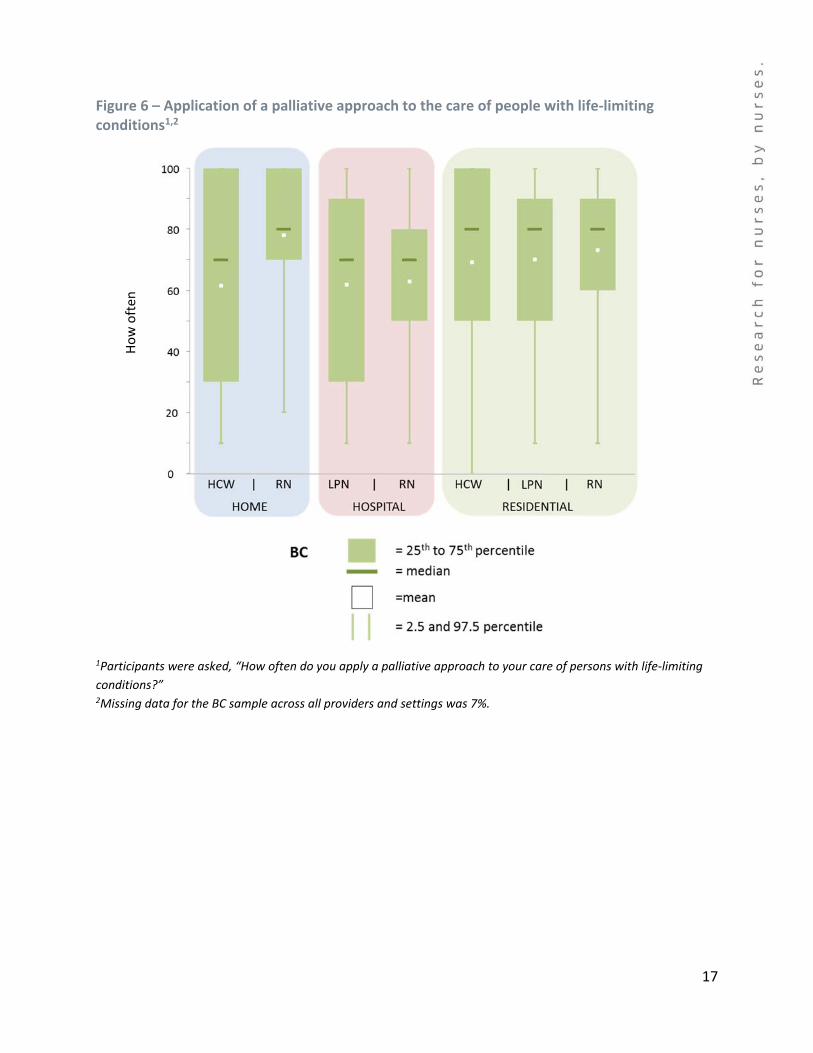
Application of a palliative approach to the care of patients with life‐limiting conditions
On average across all settings, nurses and HCWs apply a palliative approach in the care of
people with chronic life‐limiting conditions most of the time. However, relative to LPNs and
HCWs, RNs are more likely to apply a palliative approach in all settings (72% of RNs apply a
palliative approach most of the time). RNs, as a group, are also most consistent in applying a
palliative approach (this variability is demonstrated in the size of the boxes – Figure 6). HCWs in
home care and LPNs in acute medical care units are least likely to apply a palliative approach
most of the time (55% and 57%, respectively). Similarly, there is substantially more variability
among HCWs and LPNs in these two settings in how often they apply a palliative approach.
Overall, it was expected that all nurses and HCWs would apply a palliative approach most of the
time in the care of people with chronic life‐limiting conditions. The findings, however, reveal
substantial variation across and within the different care provider groups and settings. From a
staffing and skill mix perspective, it is important to note the RNs are consistently more likely to
apply a palliative approach in their care settings.
In the qualitative interviews, divergent views within the inter‐professional team about the goals
of care, limited team knowledge about what information has been shared with the patient, and
limited time, were all identified as affecting integration of a palliative approach in nursing care.
An RN in acute care explained: “Sometimes you don’t have time to communicate well with the
family or to look into referrals or talk to the doctor about this issue”.
17
Figure 6 – Application of a palliative approach to the care of people with life‐limiting conditions1,2
1Participants were asked, “How often do you apply a palliative approach to your care of persons with life‐limiting
conditions?” 2Missing data for the BC sample across all providers and settings was 7%.
How often

18
Self‐Perceived Competence in Dimensions of a Palliative Approach This section of the report addresses the question: How confident are nurses and HCWs in
applying palliative dimensions of care to address the needs of people with advancing chronic
life‐limiting conditions and their families?
The survey questionnaire included the Palliative Care Nursing Self‐Competence3 instrument
developed by Jean‐François Desbiens [6]. This scale is composed of 50 questions measuring
nurses’ self‐perceived competence in 10 dimensions of palliative care: physical needs in
regards to pain management, physical needs in regards to other symptoms, psychological
needs, social needs, spiritual needs, needs related to functional status, ethical and legal issues,
inter‐professional collaboration and communication, personal and professional issues related to
nursing care, and last hours of life. There were five questions for each dimension. Participants
were asked to rate their confidence on a scale of 0 (not at all confident) to 5 (very confident).
In this report we provide summaries of each dimension based on the averages of the five
corresponding questions. The scores for each individual question are available upon request
The tables in this section (Tables 4‐6) demonstrate the percentage (%) of RNs, LPNs, and HCWs
who view themselves as having low confidence (i.e., an average rating of less than 2.5 on a
scale of 0 – 5) in each of the dimensions of a palliative approach. Therefore, the higher the
percentages illustrated in the tables, the less confident nurses and HCWs see themselves in
those dimensions. The findings are presented separately for each setting and are compared
side‐by‐side with the overall province.
3 Perceived nursing self‐competence refers to nurses' judgment about their own capabilities to offer quality care. This self‐assessment process may promote professional practice and competence development.

19
Acute medical care settings
In acute medical care settings across the province, most RNs and LPNs feel confident in all
dimensions. The dimensions of lowest confidence are spiritual needs, social needs, and ethical
and legal issues. Areas of greater confidence are physical needs – pain, and care during last
hours of life.
Table 4 – Percentage of nurses and HCWs who feel low self‐competence in the dimensions of a palliative approach in acute medical care settings1
DIMENSIONS OF A PALLIATIVE APPROACH
RN LPN HCW2
BC BC
% provider with low confidence*
% provider with low confidence*
Physical needs: pain 2 1Physical needs: other symptoms 6 3Psychological needs 13 10Social needs 25 23Spiritual needs 28 27Needs related to functional status 9 0Ethical & legal issues 18 15Inter‐professional collaboration 5 6Personal & professional issues 3 3Last hours of life 4 2
1Missing data for the BC sample across all providers in acute medical care settings ranged from 3‐8% across the 10 dimensions. 2There were few HCWs in acute medical care units at the time of this survey, therefore this provider group/setting pair were not included in the analysis. *The dimensions where nurses and HCWs feel the least confident are highlighted in rust, and bordered. The
dimensions where nurses and HCWs feel the most confident are highlighted in green. In general, the two highest and lowest have been highlighted.
In the qualitative interviews, one acute care nurse explained feeling relatively less confident
addressing social needs, especially those of family members: “And as a nurse, we’re going in,
we’re offering care, we’re turning a patient, we’re offering pain control so that they’re
comfortable. And then I’m at a loss of what to do for the family. What can I do for them when
the person actually passes?”

20
Home care settings
In home care settings, RNs reported relatively more confidence than HCWs in all dimensions of
care. Inter‐professional collaboration is one of the dimensions of greatest confidence, as is
exemplified in the following quote: “when the nurse and the doctor can work together in a
collegial, respectful relationship, it honors the patient and you are doing the best care possible
for that client. You’re working as a team”.
The dimensions of least confidence include those pertaining to spiritual needs, social needs,
psychological issues and ethical and legal issues. One participant commented: “Ethical is the
most difficult…that’s one I’ve struggled with in my nursing…”
Table 5 – Percentage of nurses and HCWs who feel low self‐competence in the dimensions of a palliative approach in home care settings1
DIMENSIONS OF A PALLIATIVE APPROACH
RN LPN2 HCW
BC BC
% provider with low confidence*
% provider with low confidence*
Physical needs: pain 4 13 Physical needs: other symptoms 1 10 Psychological needs 6 10
Social needs 7 19 Spiritual needs 19 23
Needs related to functional status 1 6 Ethical & legal issues 9 12 Inter‐professional collaboration 1 14 Personal & professional issues 4 6 Last hours of life 1 15
1Missing data for the BC sample across all providers in home care settings ranged from 1‐6% across the 10 dimensions. 2There were few LPNs in home care at the time of this survey, therefore this provider group/setting pair were not included in the analysis. *The dimensions where nurses and HCWs feel the least confident are highlighted in rust, and bordered. The
dimensions where nurses and HCWs feel the most confident are highlighted in green. In general, the two highest and lowest have been highlighted.
21
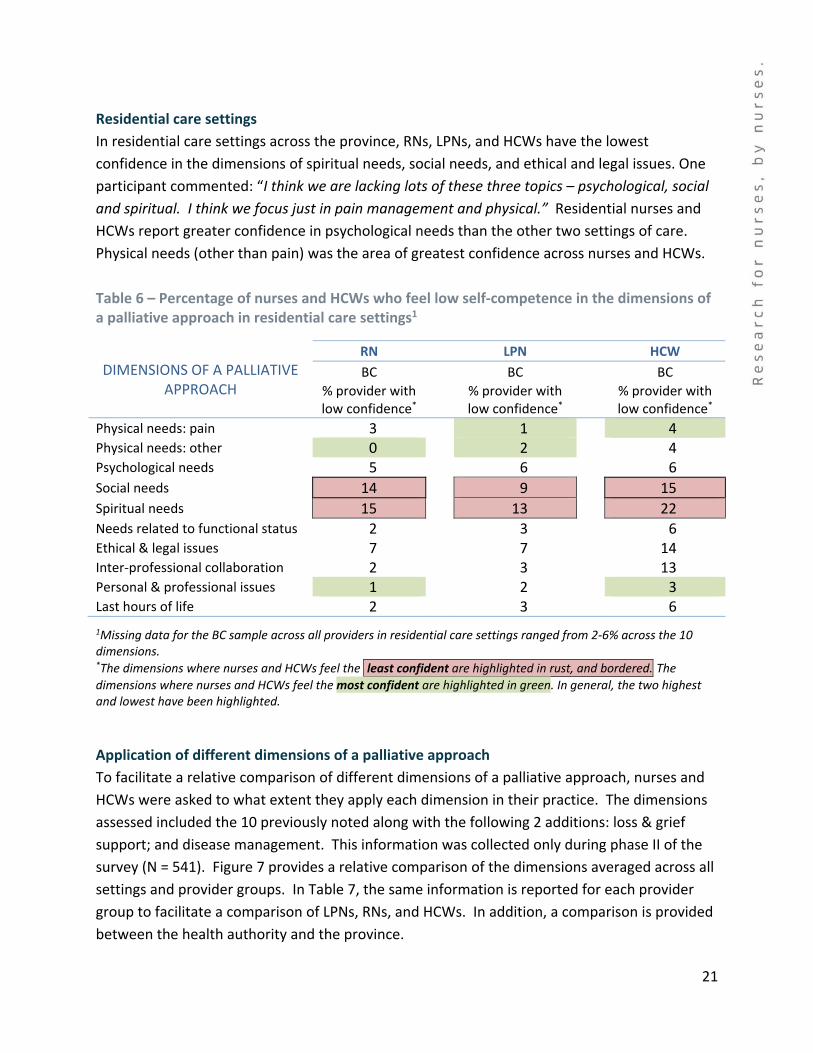
Residential care settings
In residential care settings across the province, RNs, LPNs, and HCWs have the lowest
confidence in the dimensions of spiritual needs, social needs, and ethical and legal issues. One
participant commented: “I think we are lacking lots of these three topics – psychological, social
and spiritual. I think we focus just in pain management and physical.” Residential nurses and
HCWs report greater confidence in psychological needs than the other two settings of care.
Physical needs (other than pain) was the area of greatest confidence across nurses and HCWs.
Table 6 – Percentage of nurses and HCWs who feel low self‐competence in the dimensions of a palliative approach in residential care settings1
DIMENSIONS OF A PALLIATIVE APPROACH
RN LPN HCW
BC BC BC
% provider with low confidence*
% provider with low confidence*
% provider with low confidence*
Physical needs: pain 3 1 4 Physical needs: other 0 2 4 Psychological needs 5 6 6
Social needs 14 9 15
Spiritual needs 15 13 22 Needs related to functional status 2 3 6 Ethical & legal issues 7 7 14 Inter‐professional collaboration 2 3 13 Personal & professional issues 1 2 3 Last hours of life 2 3 6
1Missing data for the BC sample across all providers in residential care settings ranged from 2‐6% across the 10 dimensions. *The dimensions where nurses and HCWs feel the least confident are highlighted in rust, and bordered. The
dimensions where nurses and HCWs feel the most confident are highlighted in green. In general, the two highest and lowest have been highlighted.
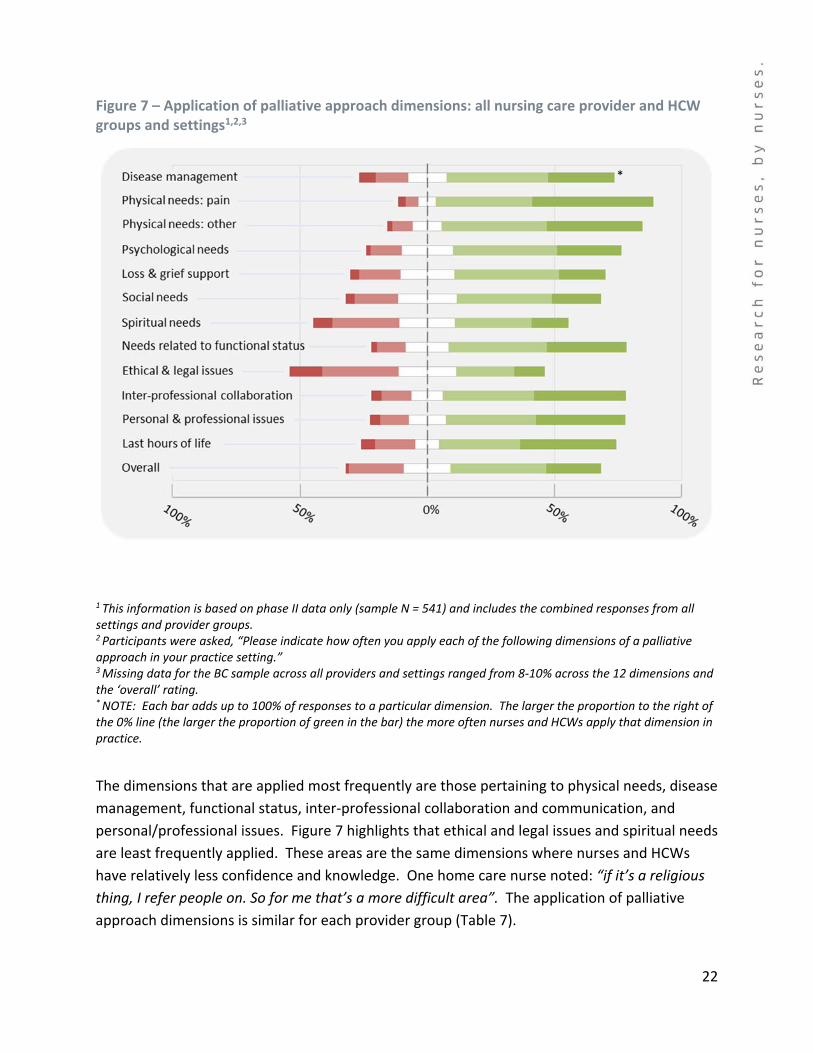
Application of different dimensions of a palliative approach
To facilitate a relative comparison of different dimensions of a palliative approach, nurses and
HCWs were asked to what extent they apply each dimension in their practice. The dimensions
assessed included the 10 previously noted along with the following 2 additions: loss & grief
support; and disease management. This information was collected only during phase II of the
survey (N = 541). Figure 7 provides a relative comparison of the dimensions averaged across all
settings and provider groups. In Table 7, the same information is reported for each provider
group to facilitate a comparison of LPNs, RNs, and HCWs. In addition, a comparison is provided
between the health authority and the province.
22
Figure 7 – Application of palliative approach dimensions: all nursing care provider and HCW groups and settings1,2,3
1 This information is based on phase II data only (sample N = 541) and includes the combined responses from all settings and provider groups. 2 Participants were asked, “Please indicate how often you apply each of the following dimensions of a palliative approach in your practice setting.” 3 Missing data for the BC sample across all providers and settings ranged from 8‐10% across the 12 dimensions and the ‘overall’ rating. * NOTE: Each bar adds up to 100% of responses to a particular dimension. The larger the proportion to the right ofthe 0% line (the larger the proportion of green in the bar) the more often nurses and HCWs apply that dimension in practice.
The dimensions that are applied most frequently are those pertaining to physical needs, disease
management, functional status, inter‐professional collaboration and communication, and
personal/professional issues. Figure 7 highlights that ethical and legal issues and spiritual needs
are least frequently applied. These areas are the same dimensions where nurses and HCWs
have relatively less confidence and knowledge. One home care nurse noted: “if it’s a religious
thing, I refer people on. So for me that’s a more difficult area”. The application of palliative
approach dimensions is similar for each provider group (Table 7).
*
23
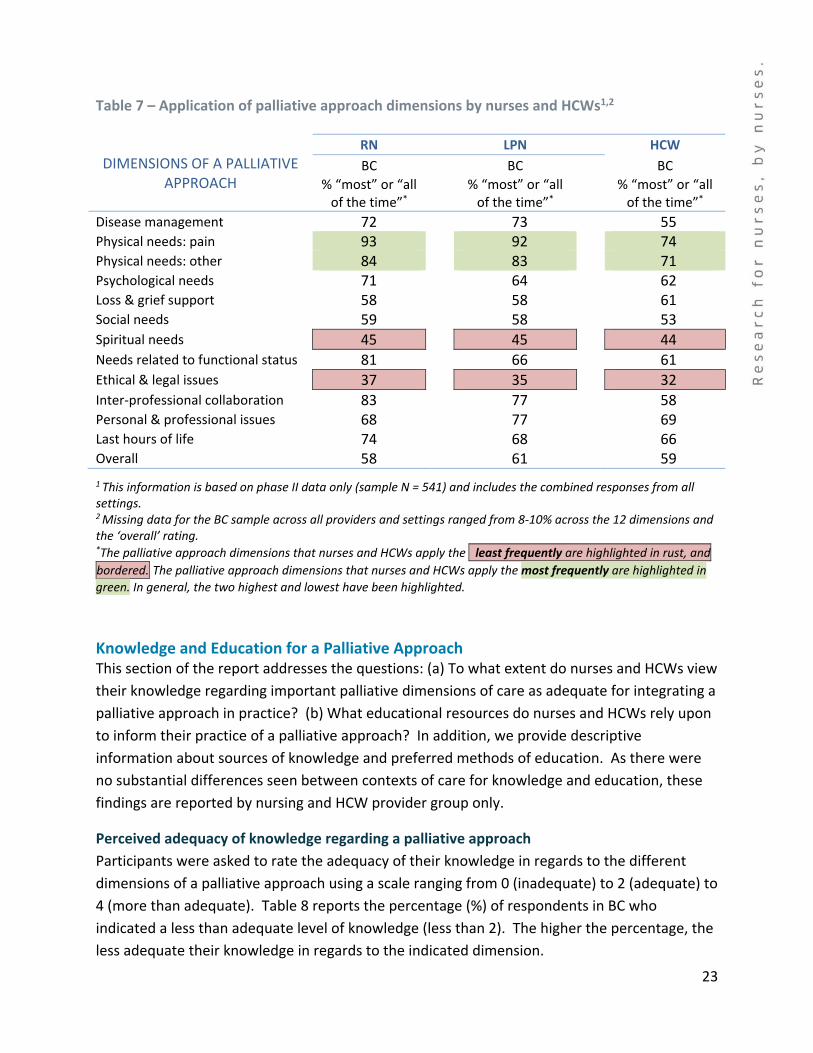
Table 7 – Application of palliative approach dimensions by nurses and HCWs1,2
DIMENSIONS OF A PALLIATIVE APPROACH
RN LPN HCW
BC BC BC
% “most” or “all of the time”*
% “most” or “all of the time”*
% “most” or “all of the time”*
Disease management 72 73 55 Physical needs: pain 93 92 74 Physical needs: other 84 83 71 Psychological needs 71 64 62 Loss & grief support 58 58 61 Social needs 59 58 53 Spiritual needs 45 45 44 Needs related to functional status 81 66 61 Ethical & legal issues 37 35 32 Inter‐professional collaboration 83 77 58 Personal & professional issues 68 77 69 Last hours of life 74 68 66 Overall 58 61 59
1 This information is based on phase II data only (sample N = 541) and includes the combined responses from all settings. 2 Missing data for the BC sample across all providers and settings ranged from 8‐10% across the 12 dimensions and the ‘overall’ rating. *The palliative approach dimensions that nurses and HCWs apply the least frequently are highlighted in rust, and
bordered. The palliative approach dimensions that nurses and HCWs apply the most frequently are highlighted in
green. In general, the two highest and lowest have been highlighted.
Knowledge and Education for a Palliative Approach This section of the report addresses the questions: (a) To what extent do nurses and HCWs view
their knowledge regarding important palliative dimensions of care as adequate for integrating a
palliative approach in practice? (b) What educational resources do nurses and HCWs rely upon
to inform their practice of a palliative approach? In addition, we provide descriptive
information about sources of knowledge and preferred methods of education. As there were
no substantial differences seen between contexts of care for knowledge and education, these
findings are reported by nursing and HCW provider group only.
Perceived adequacy of knowledge regarding a palliative approach
Participants were asked to rate the adequacy of their knowledge in regards to the different
dimensions of a palliative approach using a scale ranging from 0 (inadequate) to 2 (adequate) to
4 (more than adequate). Table 8 reports the percentage (%) of respondents in BC who
indicated a less than adequate level of knowledge (less than 2). The higher the percentage, the
less adequate their knowledge in regards to the indicated dimension.
24
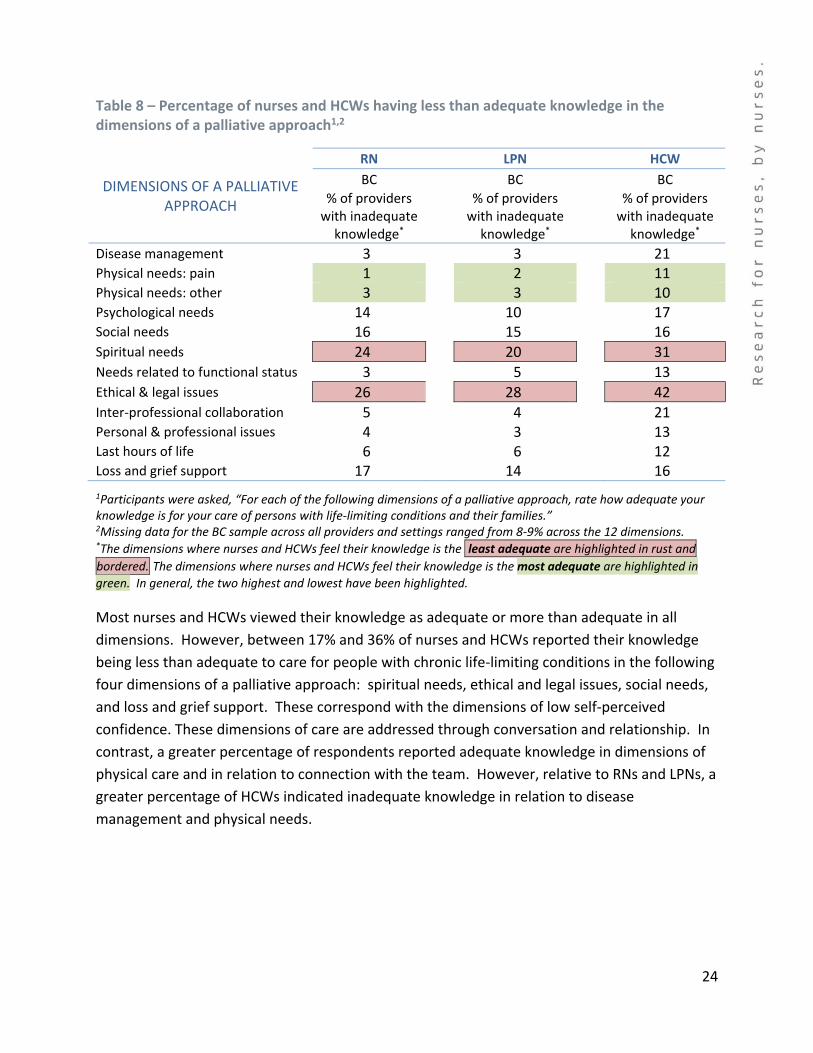
Table 8 – Percentage of nurses and HCWs having less than adequate knowledge in the dimensions of a palliative approach1,2
DIMENSIONS OF A PALLIATIVE APPROACH
RN LPN HCW
BC BC BC
% of providers with inadequate knowledge*
% of providers with inadequate knowledge*
% of providers with inadequate knowledge*
Disease management 3 3 21 Physical needs: pain 1 2 11 Physical needs: other 3 3 10 Psychological needs 14 10 17 Social needs 16 15 16 Spiritual needs 24 20 31 Needs related to functional status 3 5 13 Ethical & legal issues 26 28 42 Inter‐professional collaboration 5 4 21 Personal & professional issues 4 3 13 Last hours of life 6 6 12 Loss and grief support 17 14 16
1Participants were asked, “For each of the following dimensions of a palliative approach, rate how adequate your knowledge is for your care of persons with life‐limiting conditions and their families.” 2Missing data for the BC sample across all providers and settings ranged from 8‐9% across the 12 dimensions. *The dimensions where nurses and HCWs feel their knowledge is the least adequate are highlighted in rust and
bordered. The dimensions where nurses and HCWs feel their knowledge is the most adequate are highlighted in
green. In general, the two highest and lowest have been highlighted.
Most nurses and HCWs viewed their knowledge as adequate or more than adequate in all
dimensions. However, between 17% and 36% of nurses and HCWs reported their knowledge
being less than adequate to care for people with chronic life‐limiting conditions in the following
four dimensions of a palliative approach: spiritual needs, ethical and legal issues, social needs,
and loss and grief support. These correspond with the dimensions of low self‐perceived
confidence. These dimensions of care are addressed through conversation and relationship. In
contrast, a greater percentage of respondents reported adequate knowledge in dimensions of
physical care and in relation to connection with the team. However, relative to RNs and LPNs, a
greater percentage of HCWs indicated inadequate knowledge in relation to disease
management and physical needs.

25
How are nurses and HCWs learning in practice?
Participants were asked to indicate how often they accessed certain kinds of knowledge while
working in their practice setting (Figure 8). Almost all RNs, LPNs, and HCWs rely on colleagues
to inform their practice of a palliative approach; overall, 97% rely on colleagues “sometimes” or
“often”. An acute care nurse says: “Just ask for help. It’s open communication with colleagues
in terms of what’s needed and what should be done for a patient. That’s invaluable!”
Figure 8 – Preferred resources for a palliative approach in practice1,2
1Participants were asked, “If in your practice there was something that you did not know about a palliative approach, which of the following would you use to find the knowledge that you require?” 2Missing data for the BC sample across all providers and settings ranged from 10‐30% across resources. *NOTE: Each bar adds up to 100% of responses to a particular resource. The larger the proportion to the right of the 0% line (the larger the proportion of green in the bar) the more likely the provider is to access that resource in practice.
*

26
The preference for resources differs substantially across different provider groups and settings.
Interestingly, 89% of RNs across settings reported relying “sometimes” or “often” on clinical
nurse specialists, whereas only 74% of LPNs and HCWs (combined) reported relying on clinical
nurse specialists to the same extent. LPNs and HCWs instead reported relying more frequently
on their nurse manager or coordinator (91%). As described by this residential care aide: “Our
team leaders are fabulous. They give us total, 100% support and any questions we have, they’re
right there.”
Figure 9 – Preferred methods of education1,2,3
1 Data only available for Phase I of the Survey (N=892) 2 Participants were asked, “What are your preferred methods for receiving education in a palliative approach?’”
3 Missing data for the BC sample across all providers and settings ranged from 10‐17% across methods (missing data for
‘Other’ is excluded). *NOTE: Each bar adds up to 100% of all provider group responses to a particular education method. The larger the proportion to the right of the 0% line (the larger the proportion of green in the bar) the more providers preferred that method of education.
*

27
In addition to preferred resources for a palliative approach in practice, participants were also
queried about their preferred methods of receiving education (Figure 9). Face‐to‐face learning
was notably the most preferred method for receiving education for nurses and HCWs across
settings. Although online and self‐study are accessed, education in a palliative approach would
be best received given a face‐to‐face format. When interviewed, nurses said they benefitted
from “just in time” strategies such as huddles, care rounds, and mentorship.
Conclusion
The finding from our survey provide an overview of BC nurses’ and HCWs’ perspectives of their
confidence, knowledge and application regarding a palliative approach in acute medical,
residential and home care settings. Additional analyses, not reported herein, have been
conducted to improve our understanding of the differences in self‐perceived competence,
knowledge, professional experience, work place characteristics, and other differences among
nurses and HCWs related to the integration of a palliative approach.
An important finding from these analyses is that identification of people with chronic life‐
limiting conditions is not enough to ensure the integration of a palliative approach. Other
factors, including nurses’ and HCWs’ beliefs regarding the benefits of a palliative approach,
must also be considered. Processes are needed to support clear understanding of the benefit
of a palliative approach for particular patient groups. This includes: advance care planning
conversations; assessment of symptom burden; incorporating interventions beyond disease
modifying treatments to relieve symptom distress; creation of shared care plans that
acknowledge ongoing disease advancement; and addressing the unique perspectives of the
patients and their families’.
iPANEL is using the results of the survey to inform a more extensive program of research that
seeks to address the question: How and in which contexts can a palliative approach better meet
the needs of patients with an advancing chronic life‐limiting illness and their family members
and guide the development of innovations in health care delivery systems to better support
nursing practice and the health system in British Columbia (BC)? This includes knowledge
synthesis, knowledge translation, and primary research to investigate approaches to nursing
care delivery that best facilitate the integration of a palliative approach.
28
References
1. Kristjanson, L.J., C. Toye, and S. Dawson, New dimensions in palliative care: a palliative
approach to neurodegenerative diseases and final illness in older people. The Medical
journal of Australia, 2003. 179(6 Suppl): p. S41‐3.
2. Lynn, J., Living long in fragile health: The new demographics shape end of life care.
Supplement to Improving End of Life Care: Why has it been so difficult. Hastings Center
Report Special Report. 35(6), S14‐S18. Retrieved June 1, 2014 from
http://www.thehastingscenter.org/pdf/living‐long‐in‐fragile‐health.pdf.
3. Stajduhar, K.I., Chronic illness, palliative care, and the problematic nature of dying. The
Canadian journal of nursing research = Revue canadienne de recherche en sciences
infirmieres, 2011. 43(3): p. 7‐15.
4. British Columbia Ministry of Health, The Provincial End‐of‐Life Action Plan for British
Columbia, 2013. Retrieved June 1, 2013, from
http://www.health.gov.bc.ca/library/publications/year/2013/end‐of‐life‐care‐action‐
plan.pdf
5. Canadian Institute for Health Information, Health care use at the end of life in British
Columbia, 2008. Retrieved June 1, 2014, from
https://secure.cihi.ca/free_products/end_of_life_report_aug07_e.pdf
6. Desbiens, J.F. and L. Fillion, Development of the Palliative Care Nursing Self‐competence
Scale. Journal of Hospice & Palliative Nursing, 2011. 13(4): p. 230‐241.