integratingclinicaldecision supportincpoe - ashp · pdf file ·...
TRANSCRIPT
Primary Intended Outcomes1. Improve the efficiency, safety, and accuracy of
ordering electrolyte replacement through anurse-managed protocol,
2. Provide discrete orders in the computerizedprovider order entry (CPOE) system whennurses replace electrolytes, and
3. Improve how CPOE orders interface to thepharmacy system to enhance efficiency andreduce potential dispensing errors.
Relevant PPMI RecommendationC2. The following technology solutions in hospi-
tals and health systems are important enablersin the development of optimal pharmacy prac-tice models:
C2d. Clinical decision support (CDS) integratedwith CPOE.
Situation AnalysisVanderbilt University Medical Center is a compre-hensive health care facility dedicated to patientcare, research, and biomedical education. TheMedical Center has more than 900 licensed bedsdivided between a main hospital campus, theMonroe Carell Jr. Children’s Hospital at Vanderbilt,and the Psychiatric Hospital at Vanderbilt. Com-prehensive outpatient services are also providedin numerous clinics both on and off campus. Phar-macists practice throughout the Medical Centerbut are typically divided between adult, pediatric,and outpatient areas. Pharmacy practice special-ties include oncology, infectious disease, trans-plantation, hemophilia, anticoagulation,cardiology, neonatal intensive care, pediatricintensive care, and adult surgical, medical, andtrauma intensive care. The Vanderbilt system has
Integrating Clinical DecisionSupport in CPOESubmitted by: Fred Hargrove, B.S. Pharm, Informatics Pharmacy Manager, Informatics Center Vanderbilt UniversityMedical Center, 3401 West End Avenue, Suite 630, Nashville, TN 37203, (615) 343-5145, [email protected]
C A S E S T U D Y
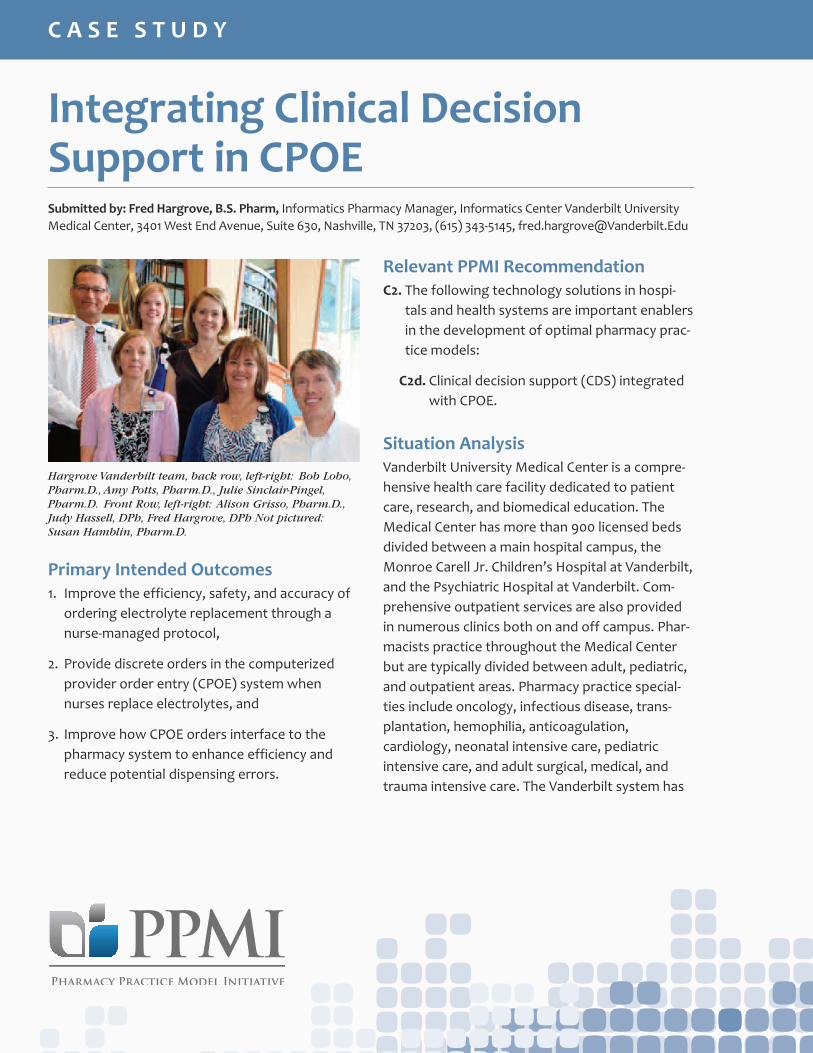
Hargrove Vanderbilt team, back row, left-right: Bob Lobo,Pharm.D., Amy Potts, Pharm.D., Julie Sinclair-Pingel,Pharm.D. Front Row, left-right: Alison Grisso, Pharm.D.,Judy Hassell, DPh, Fred Hargrove, DPh Not pictured:Susan Hamblin, Pharm.D.
been using CPOE for approximately 20 years, andintroduced bar code medication administration(BCMA) within the last 5 years. The PharmacyDepartment uses automation technology in drugstorage, preparation, and dispensing.
Nurse-managed electrolyte replacement proto-cols were used in the adult hospital and cliniciansordered discrete doses in the pediatric hospital.To increase efficiency and minimize delays in elec-trolyte replacement, the pediatric hospital alsoelected to implement a nurse-managed protocolif sufficient CDS safeguards were available.Because replacement doses are dependent onpatient and lab result variables, the protocolorders entered into CPOE were essentially per-mission orders without any dose or administra-tion details. The single CPOE electrolytereplacement order was linked to a pharmacy sys-tem protocol containing up to a dozen PRNorders with verbose, lab- dependent, replace-ment instructions in the comment field. Thesepharmacy PRN orders were transmitted to theBCMA system for nurse review. Additionally,these orders could link to electrolytes stored inunit-based automated dispensing cabinets. Whenan electrolyte lab result was reported, the nursefollowed the order instructions in BCMA andcould either obtain the electrolyte from the dis-pensing cabinet or the pharmacy. Errors in rate ordosing had been reported, and follow-up labswere not consistently ordered.
Service DescriptionThe pediatric pharmacy clinical coordinatorapproached the pharmacy informatics team todevelop a nurse-managed electrolyte replace-ment protocol that would use real-time, patient-
specific CDS. The requirements were approved bythe pediatric Pharmacy and Therapeutics Commit-tee (P&T) and nursing leadership. A pediatric clini-cal pharmacist assisted Pharmacy Informaticswith content, behavior, and testing.
The new CPOE procedure allows the clinician tospecify which electrolytes should be replaced andonly permits the nurse to order these defined elec-trolytes (Figure 1). When a lab result is reported,the nurse orders the replacement electrolyte inCPOE, where the suggested replacement dose ishighlighted based on the most recent lab result.Calculations for weight-based dosing along withdilution instructions for peripheral and centraladministration are displayed (Figures 2, 3, and 4).Maximum doses are enforced regardless ofweight-based calculation results. To minimize phar-macy order processing errors, the program selectsthe appropriate dispensing file, which is sent via anintelligent interface to the pharmacy system (Fig-ure 5). Rather than being a PRN order in BCMA sys-tem, the replacement order is now a scheduledmedication that demands that the nurse addressthe order. BCMA information is sent to the phar-macy, electronic medical record (EMR), and CPOEsystems. Appropriately scheduled follow-up laborders are also ordered.
Coincidentally, shortly after the new procedurewas implemented in pediatrics, the adult phar-macy clinical coordinator contacted PharmacyInformatics about minimizing electrolyte replace-ment errors. Pharmacy Informatics suggested anadult version of the program developed for pedi-atrics. This was approved by P&T, adult traumaphysicians, and nursing. Pharmacy Informaticsworked with the trauma clinical pharmacist oncontent and testing (Figures 6 and 7).
C A S E S T U D Y
Key Elements for Success1. Experience in demonstrating the power of
incorporating decision support in CPOE,
2. Nursing and pharmacy education in the newprocedure, and
3. Buy-in from the P&T, as most clinical contentchanges in CPOE must have the committee’sapproval.
Resource UtilizationPersonnel: One informatics pharmacist, two clini-cal pharmacists and one clinical coordinator forthe pediatrics program. One informatics pharma-cist, one clinical pharmacist, and one clinical coor-dinator for the adult program. Systems SupportServices assist with nursing education.
IT and other infrastructure: CPOE, barcodeadministration, templates for the electrolytes,regular maintenance of the drug library.
Supply Expense: N/A
Return on Investment: N/A
Recognized Intangible Benefits1. Ordering medications in approved, standard-
ized doses improves patient safety.
2. Improvements in physician orders, guidancefor nurses in managing the electrolyte replace-ment protocol, improved pharmacy order pro-cessing and documentation.
OutcomeMeasures1. Efficiency in responding to low electrolyte lev-
els because clinicians do not need to be con-tacted first,
2. Increased number of follow-up lab tests, and
3. Feedback from physicians and nurses indicat-ing that their workflow has improved.
Lessons Learned1. Programs that pull data from the EMR to assist
clinicians in making decisions about medicationsare worth the investment in time and effort.
2. Nurses tend to appreciate new technologywhen you can demonstrate how it will savethem time and improve patient safety.
Other ConsiderationsPharmacy Informatics is organizationally part ofthe Vanderbilt Informatics Center. This fostersclose cooperation and access to computer sci-ence programmers as well as informatics clini-cians. Pharmacy Informatics is responsible formaintaining drug content and decision support inthe CPOE, pharmacy, and BCMA systems. Phar-macy Informatics is positioned to leverage itsclose working relationships with clinicians andprogrammers to improve the medication-useprocess at the medical center.
C A S E S T U D Y

Suggestions for OtherHospitals/Health SystemsInformatics is a relatively new specialty practicearea for pharmacists. Through their clinicalknowledge and understanding computer andautomation systems, informatics pharmacists arepositioned to make contributions to improvingmedication management and patient care. Hospi-tals should be encouraged to nurture an infor-matics pharmacist program and evaluate howtheir systems can support improvements inpatient care and mitigate potential errors.
Other key individuals involved in this project were:
• Judy H. Hassell, B.S.Pharm, Informatics Phar-macist, Informatics Center, Vanderbilt Univer-sity Medical Center
• Julie Sinclair-Pingel, Pharm.D., Clinical Pharma-cist, Monroe Carell Jr. Children's Hospital atVanderbilt
• Amy L. Potts, Pharm.D, BCPS, Assistant Direc-tor, Monroe Carell Jr. Children’s Hospital atVanderbilt
• Alison Grisso, Pharm.D., Clinical Pharmacist,Monroe Carell Jr. Children's Hospital at Vander-bilt
• Susan Hamblin, Pharm.D, BCPS, Trauma CriticalCare Clinical Pharmacist, Vanderbilt UniversityMedical Center
• Bob Lobo, Pharm.D., FCCP, BCPS, Manager,Drug Policy and Clinical Services, Departmentof Pharmaceutical Services
C A S E S T U D Y
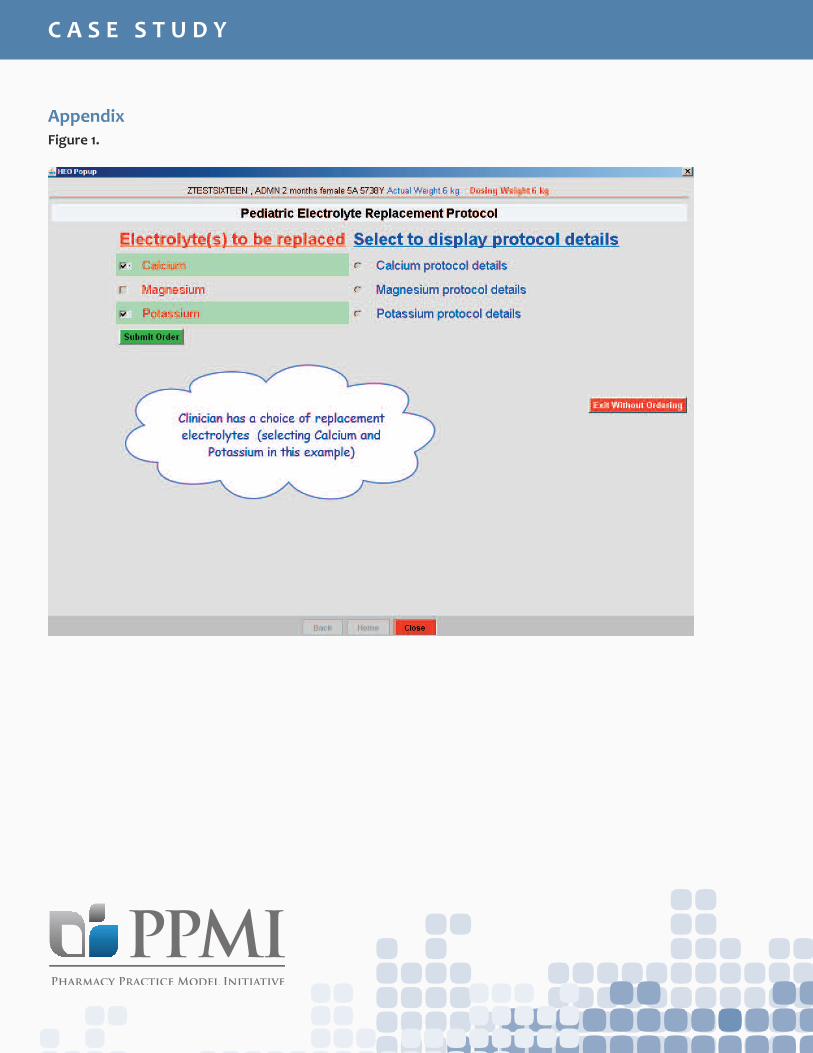
AppendixFigure 1.
C A S E S T U D Y
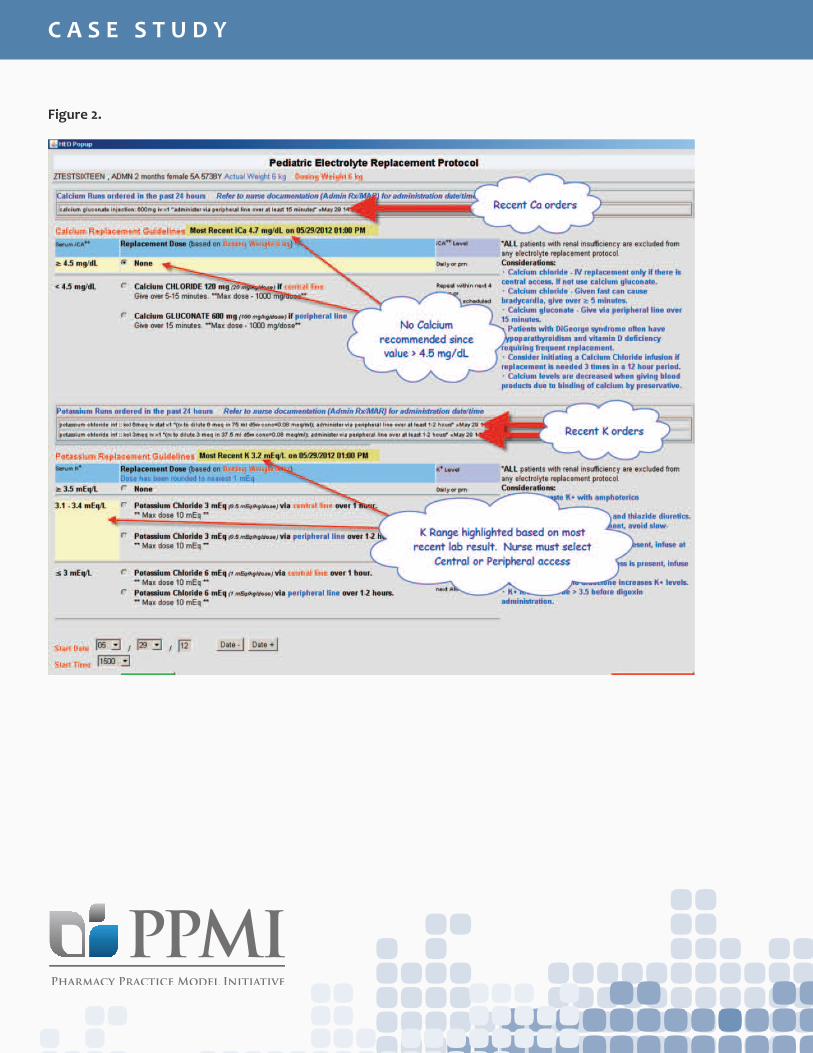
Figure 2.
C A S E S T U D Y
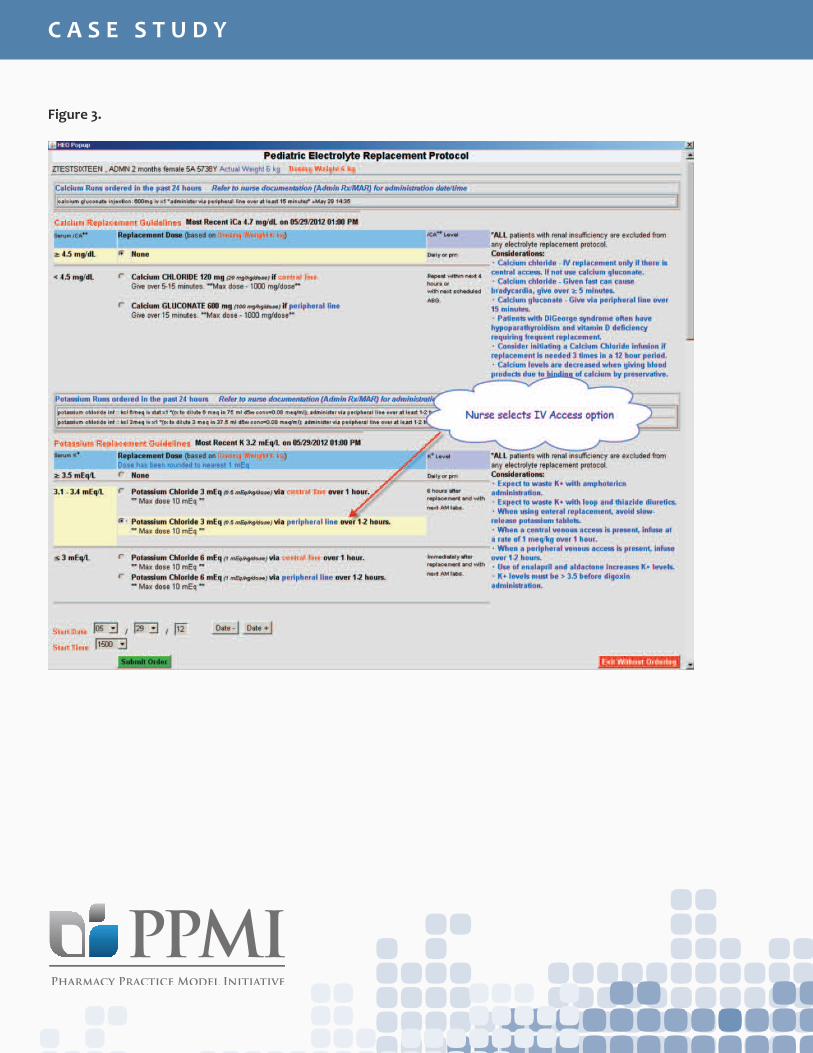
Figure 3.
C A S E S T U D Y
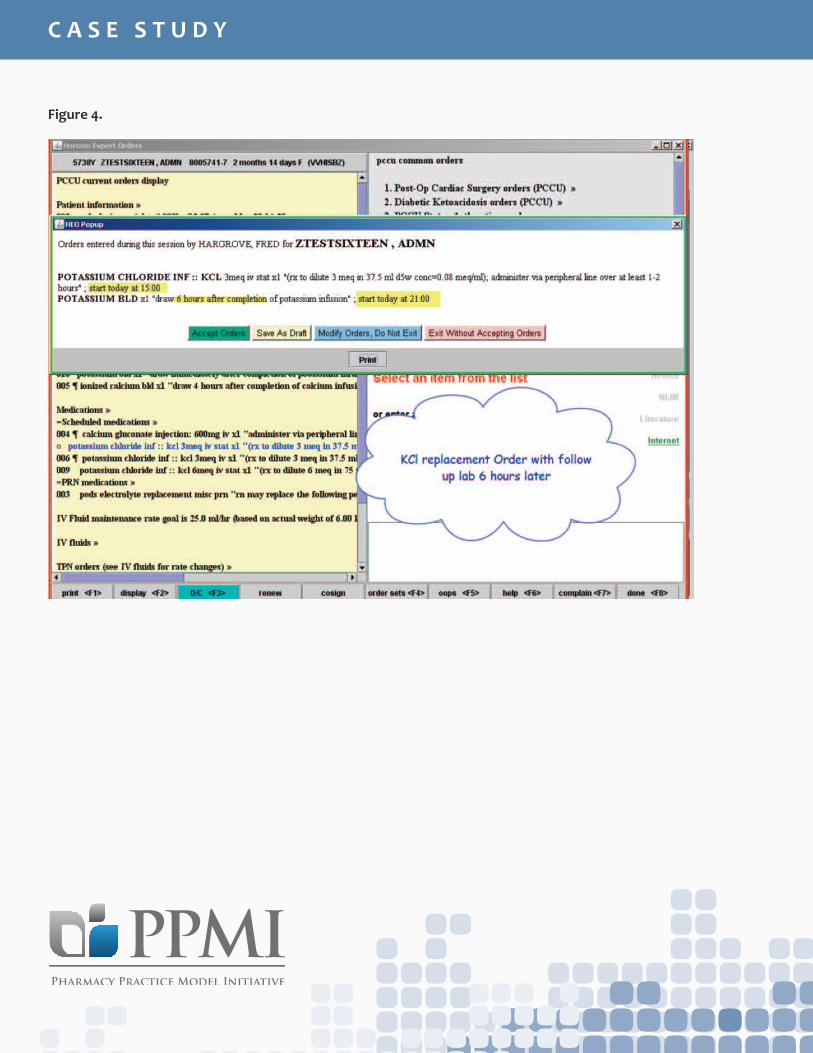
Figure 4.
C A S E S T U D Y
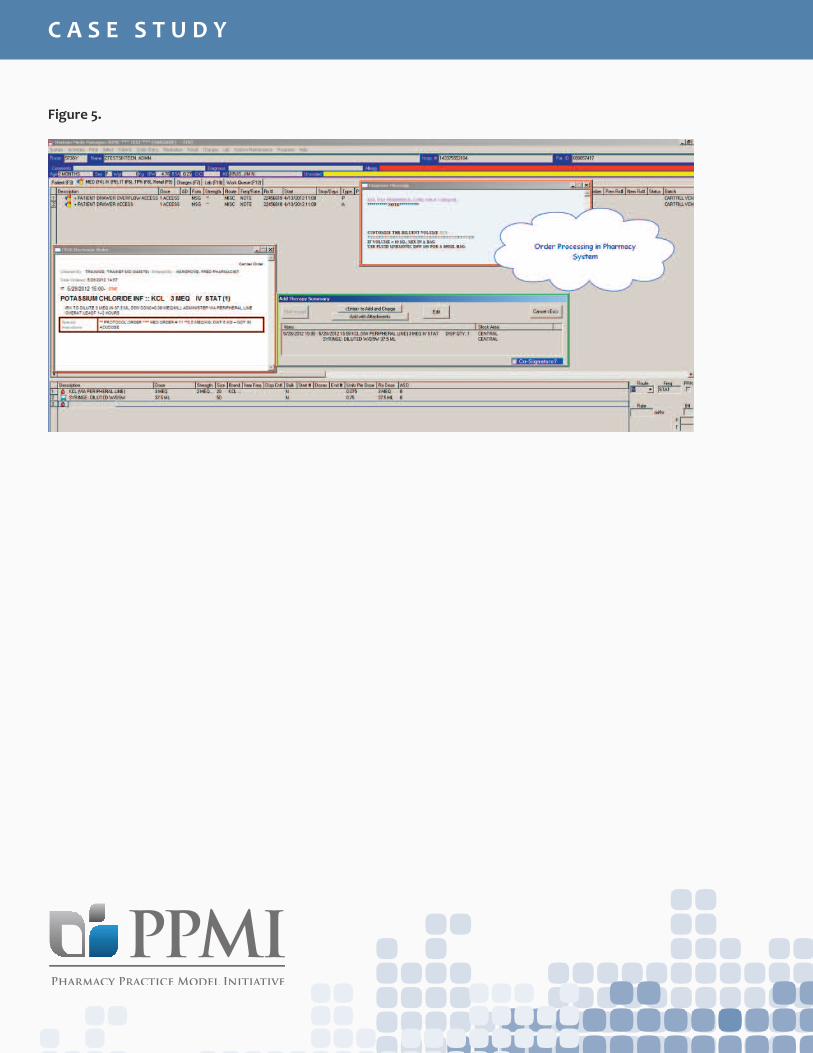
Figure 5.
C A S E S T U D Y
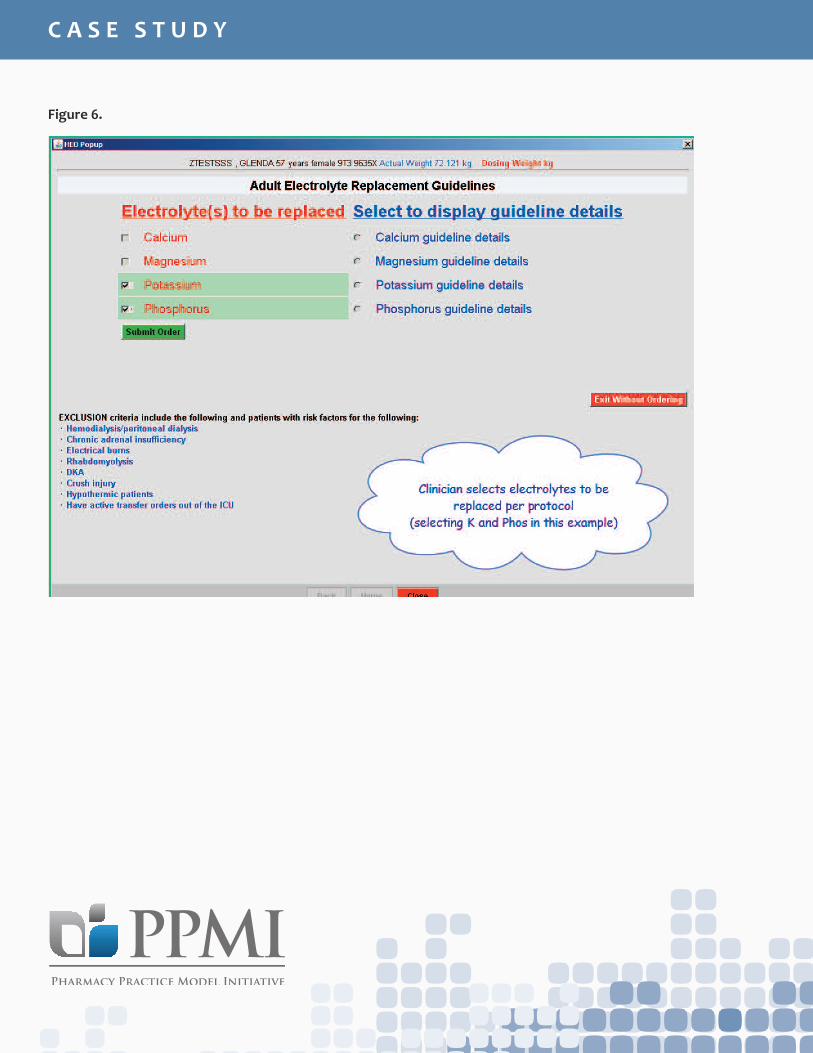
Figure 6.
C A S E S T U D Y
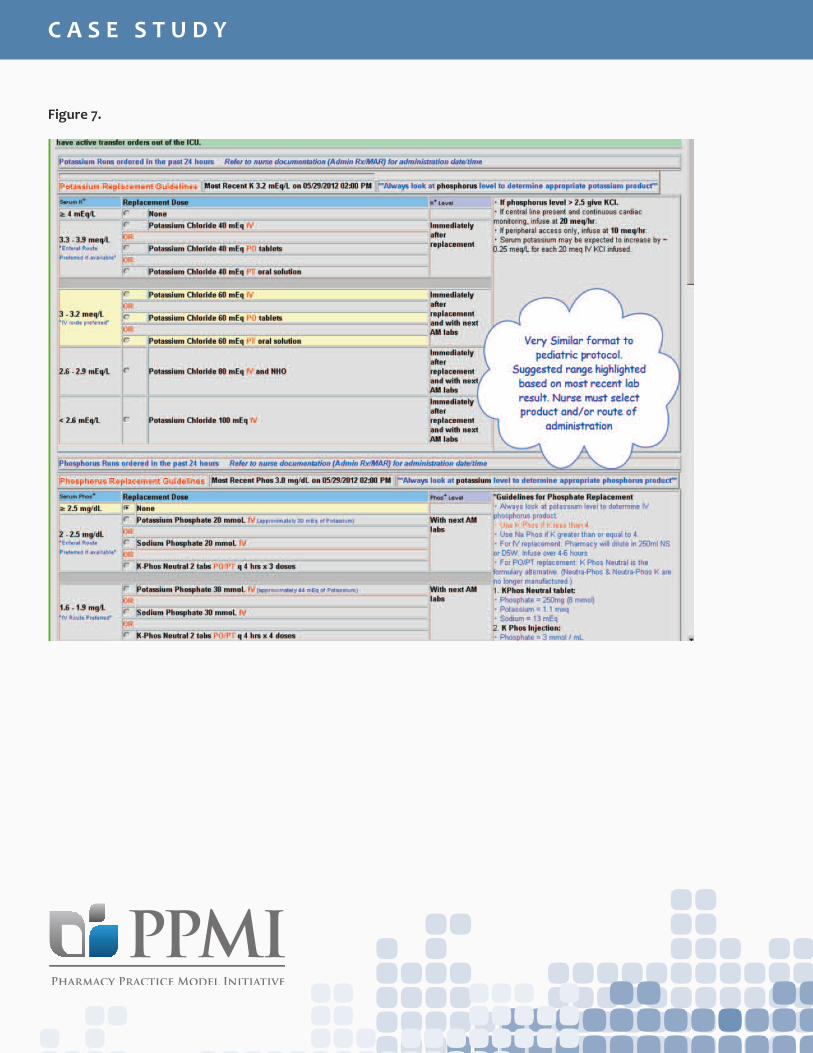
Figure 7.
C A S E S T U D Y