integrating the latest data and guidelines into...
TRANSCRIPT

Integrating the Latest Data and Guidelines into Practice: How to Reorganize Care to Get the Right Patient to the Right Place Right Away
Lee H. Schwamm, MD, FAHA, FANA Executive Vice Chair of Neurology C Miller Fisher Endowed Chair and Director of Stroke Services Director MGH TeleHealth Massachusetts General Hospital, Professor of Neurology, Harvard Medical School
Disclosures
Presenter Disclosure Information: • Steering and Science Committees of Get With The Guidelines • Target:Stroke Working Group, Chair Stroke Clinical Work Group • International Steering Committee, DIAS 3&4 (Lundbeck) and REACT-
AF/Stroke AF (Medtronic) • PI of MR WITNESS (NINDS/Genentech) • DSMB Separator 3D (Penumbra)

How the Beatles Changed Stroke Care: “Help. I Need Somebody!”
1950’ Cadillac Meteor
Maizlin ZV1, Vos PM. Do we really need to thank the Beatles for the financing of the development of the computed tomography scanner? J Comput Assist Tomogr. 2012 Mar-Apr;36(2):161-4.
1970’s
L R
Electric and Musical Industries (EMI) Ltd was formed in 1931 from the Columbia Graphophone Company. EMI invested in its engineers who went on to develop radar, television transmitters, photomultipliers, transistorized computers and under Houndsfield, the CT scanner
1960’s

Acute stroke triage to improve access to IV tPA
Site of stroke
Patient history, vitals, CT scan
Triage decision: ED physician/
neurologist confirms stroke diagnosis
Negative CT Positive CT ICH
EMS transfer
Prehospital triage
Self-present
Stroke center
Hospital
Unidimensional EMS Triage for Acute Stroke to tPA-Capable Hospitals
Having a Stroke? No worries, we’ll help. We have tPA!

A New Era Dawns
6

mechanistic basis for superiority relates to…? - retention of structural integrity of the clot and vessel wall - reduced outward radial pressure on the vessel wall
Gorelick P, Lancet 2012
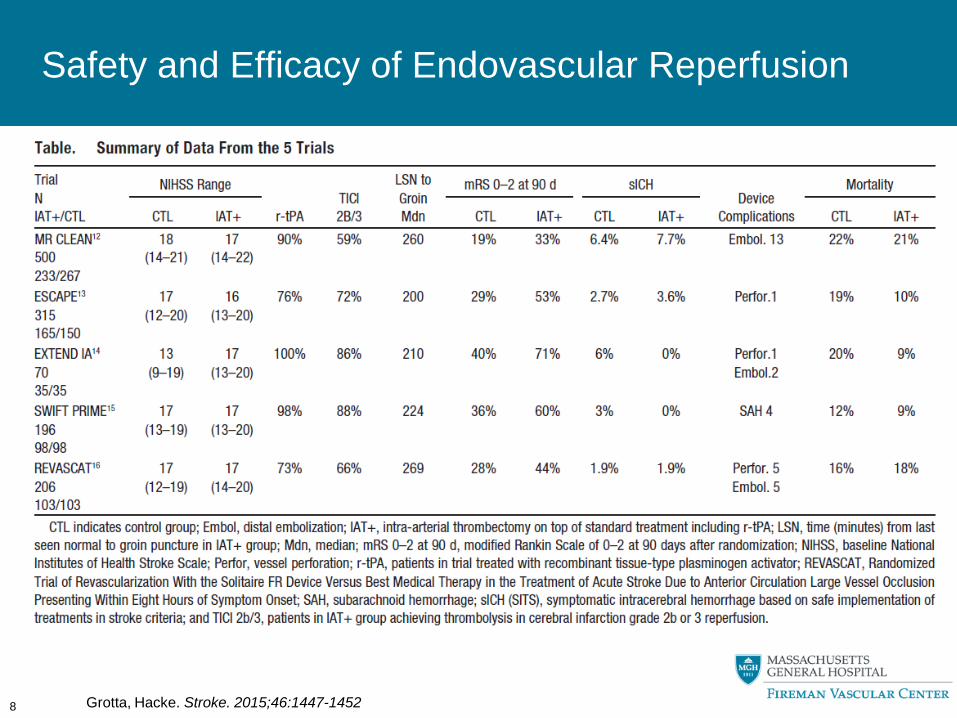
Safety and Efficacy of Endovascular Reperfusion
8 Grotta, Hacke. Stroke. 2015;46:1447-1452
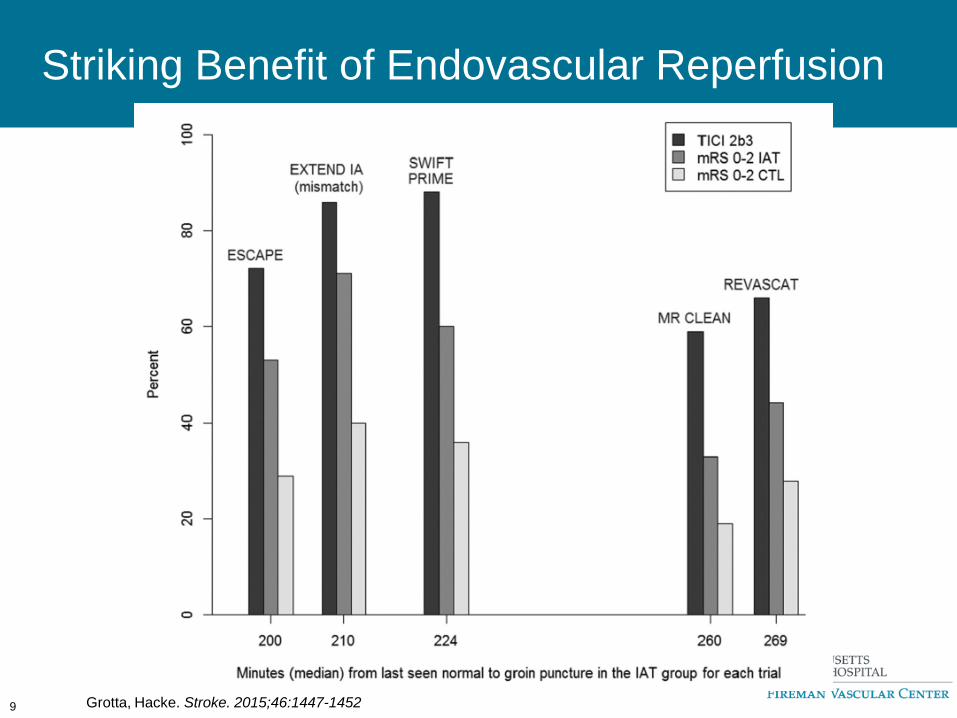
Striking Benefit of Endovascular Reperfusion
9 Grotta, Hacke. Stroke. 2015;46:1447-1452
10

2015: Pre-Hospital Triage Pathways for Acute Stroke
Acute Stroke Ready Hospital
BLS transport
ALS transport
Air transport
Mobile Stroke Unit Rx Onsite
Basic Receiving Hospital
-Primary
-Comprehensive
Factors: • tPA candidate? • EVT candidate? • Distance • Run Times • Designation Tiers • Availability of Services • Diversion Status • Medical Control • ABC stable • Dispatch Criteria • Public vs. Private EMS • Patient Preference
Regional Prehospital
Triage Algorithms: based on
stroke duration and
patient severity

How Must We Change in Light of the Compelling EVT Evidence of Benefit?
• Who are the Right Patients?
– How Can We Detect them Reliably?
• What are the Right Places?
• How Soon is the Right Amount of Time?
• How Should we Accomplish this?
12

"Sy says — When having a stroke, get to the hospital as soon as possible — within the first six hours. Ask for a T.P.A”
http://www.theatlantic.com/health/archive/2009/12/about-my-father/32221/
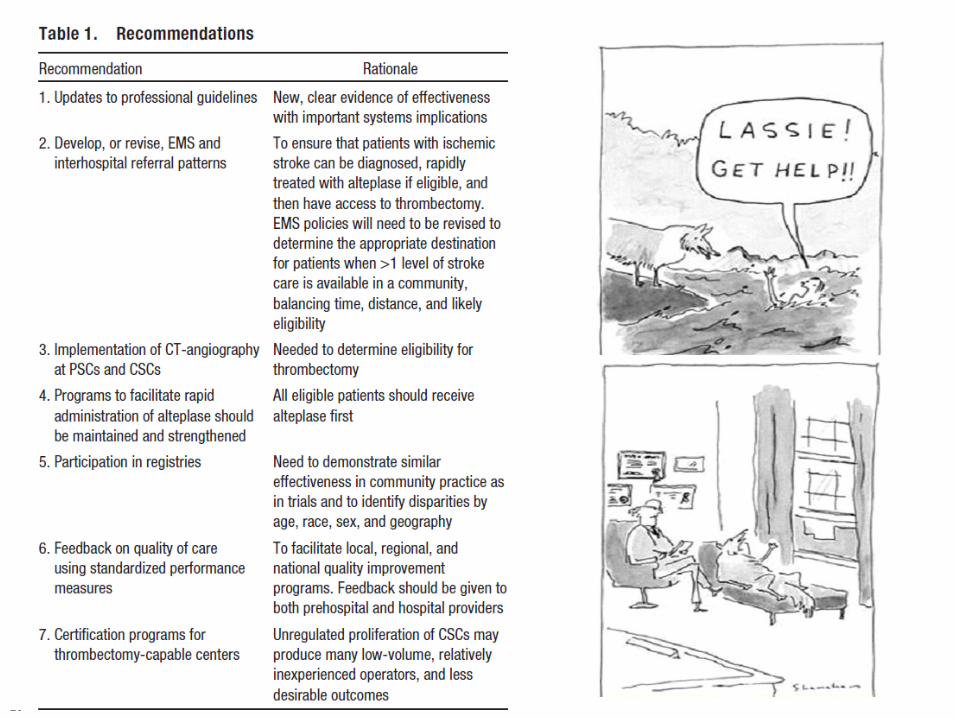
Most Patients Don’t Come with a Note Pinned to their Chest that says “Get me a thrombectomy!”

Treatable Patients at High Risk with Major Stroke Syndromes of Relatively Short Duration

Penumbra (at risk)
Core (irreversibly damaged)
Major Strokes: How to define?

By Imaging Criteria? Preserved Parenchyma & Good Collaterals if CTA Available and Reliable
16
Collaterals: From Rags ………………………………………………………to Riches
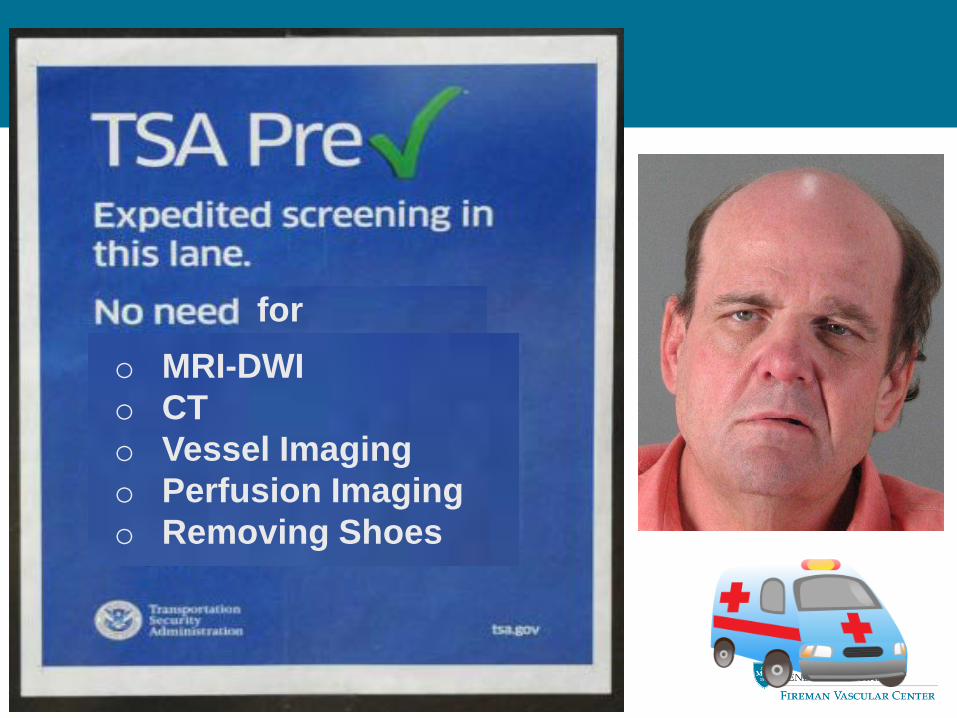
for undergo o MRI-DWI o CT o Vessel Imaging o Perfusion Imaging o Removing Shoes
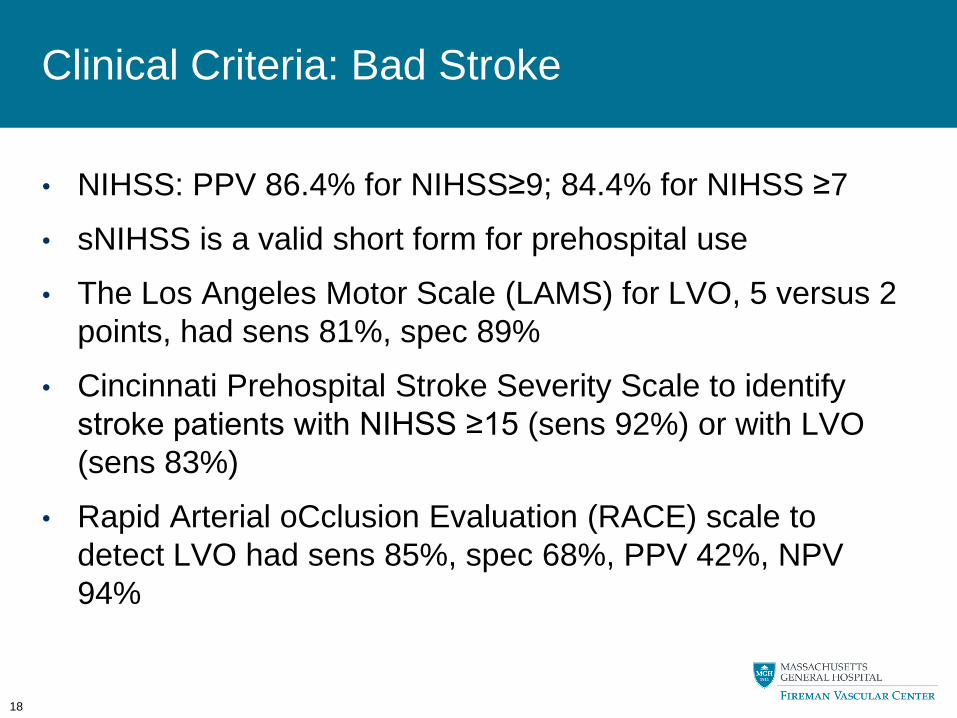
Clinical Criteria: Bad Stroke
• NIHSS: PPV 86.4% for NIHSS≥9; 84.4% for NIHSS ≥7
• sNIHSS is a valid short form for prehospital use
• The Los Angeles Motor Scale (LAMS) for LVO, 5 versus 2 points, had sens 81%, spec 89%
• Cincinnati Prehospital Stroke Severity Scale to identify stroke patients with NIHSS ≥15 (sens 92%) or with LVO (sens 83%)
• Rapid Arterial oCclusion Evaluation (RACE) scale to detect LVO had sens 85%, spec 68%, PPV 42%, NPV 94%
18

How Must We Change in Light of the Compelling EVT Evidence of Benefit?
• Who are the Right Patients?
• What are the Right Places?
– First Stop vs. Transfer
• How Soon is the Right Amount of Time?
• How Should we Accomplish this?
19
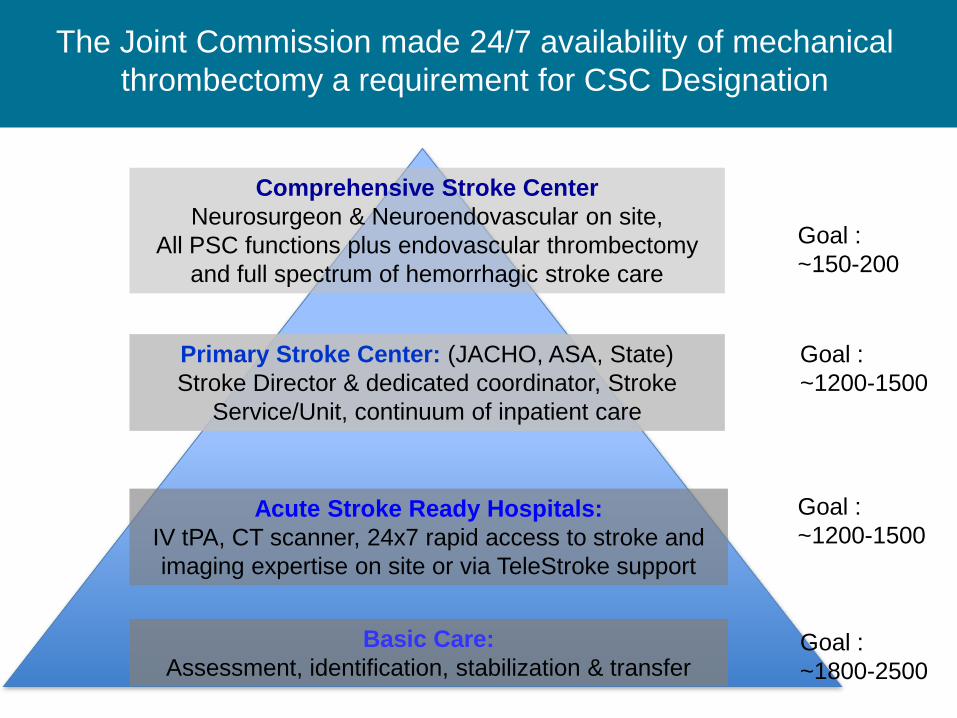
The Joint Commission made 24/7 availability of mechanical thrombectomy a requirement for CSC Designation
Basic Care: Assessment, identification, stabilization & transfer
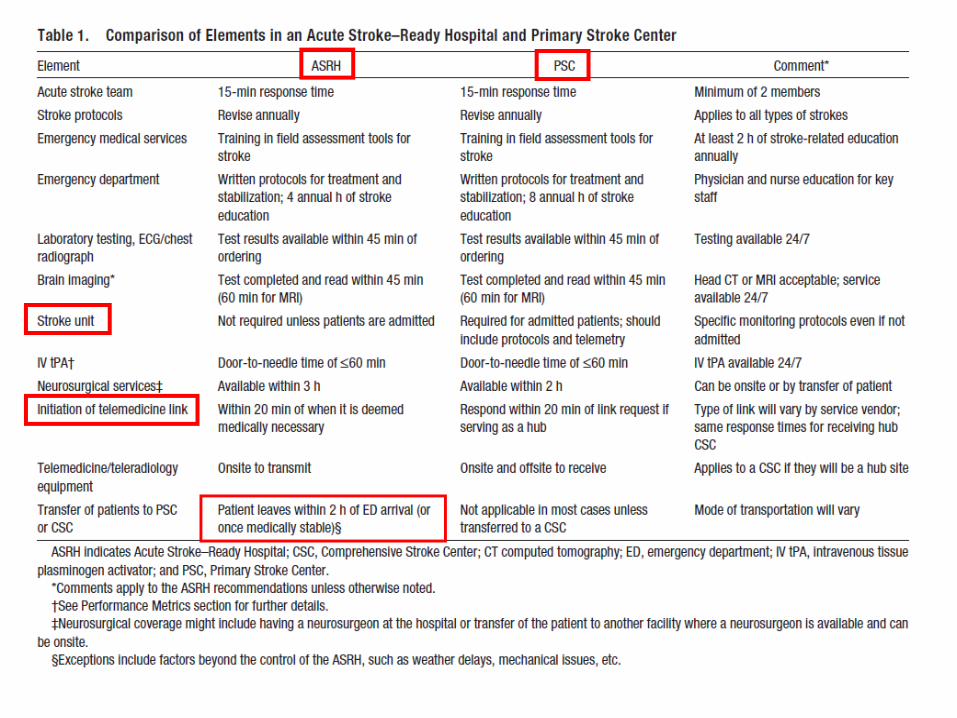
Acute Stroke Ready Hospitals: IV tPA, CT scanner, 24x7 rapid access to stroke and imaging expertise on site or via TeleStroke support
Primary Stroke Center: (JACHO, ASA, State) Stroke Director & dedicated coordinator, Stroke
Service/Unit, continuum of inpatient care
Comprehensive Stroke Center Neurosurgeon & Neuroendovascular on site,
All PSC functions plus endovascular thrombectomy and full spectrum of hemorrhagic stroke care
Goal : ~150-200
Goal : ~1200-1500
Goal : ~1200-1500
Goal : ~1800-2500

High Impact, Low Frequency, Widely Dispersed
Menon. Stroke. 2015 Apr;46(4): 989-95
Proportion of GWTG hospitals providing endovascular therapy 2003-2013 Proportion of patients receiving endovascular therapy at GWTG Hospitals

“Harry, which hospital will the Sorting Hat put us in? Comprehensive, Primary or Acute Stroke Ready?”
Stroke Centers
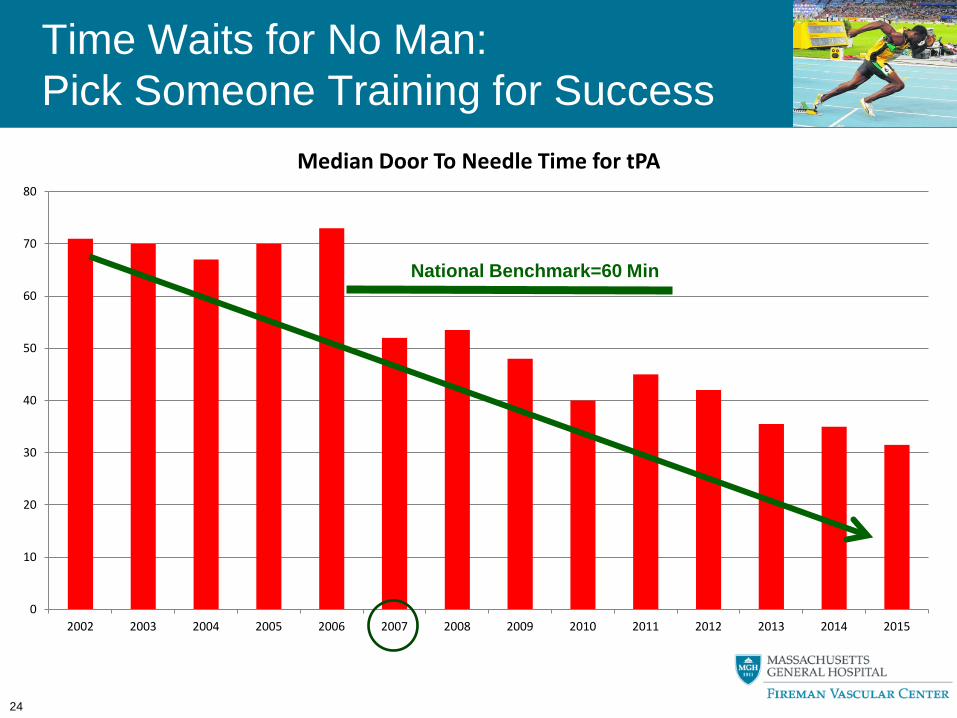
Time Waits for No Man: Pick Someone Training for Success
24
0
10
20
30
40
50
60
70
80
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Median Door To Needle Time for tPA
National Benchmark=60 Min

High Volume Centers That are Not Too Far Away and Focused on Short DTB for EVT
Process map for time intervals from patient assessed for intervention, clinical exam, evidence of occlusion on CTA to arrival in Endovascular Suite
Mehta BP et al. Reducing door-to-puncture times for intra-arterial stroke therapy: a pilot quality improvement project. J Am Heart Assoc. 2014 Nov 11;3(6):e000963

Triage to 1st Site then Transfer vs. Admission of AIS <4.5 h when EMS Considers Potentially Eligible for tPA or Thrombectomy
1st Entry MSU Basic ASRH PSC CSC Mimic? Opp cost Not Good* ? ? Opp Cost
V. Mild sx Opp cost Not Good* OK Ideal Opp Cost
Mod sx Ideal Not Good* Ideal Ideal Opp Cost
Severe sx Ideal Not Good* OK OK Ideal
Mod-Sev HS Ideal Not Good* OK OK Ideal
26
Admission MSU Basic ASRH PSC CSC Benign Mimic - ? OK? Prob Ideal Opp Cost
V. Mild sx - Not Good Maybe Ideal Opp Cost
Mod sx - Not Good Not Good Ideal Maybe
Severe sx - Not Good Not Good Maybe Ideal
Mod-Sev HS - Not Good Not Good Maybe Ideal
* Unless airway compromise or unstable in BLS care
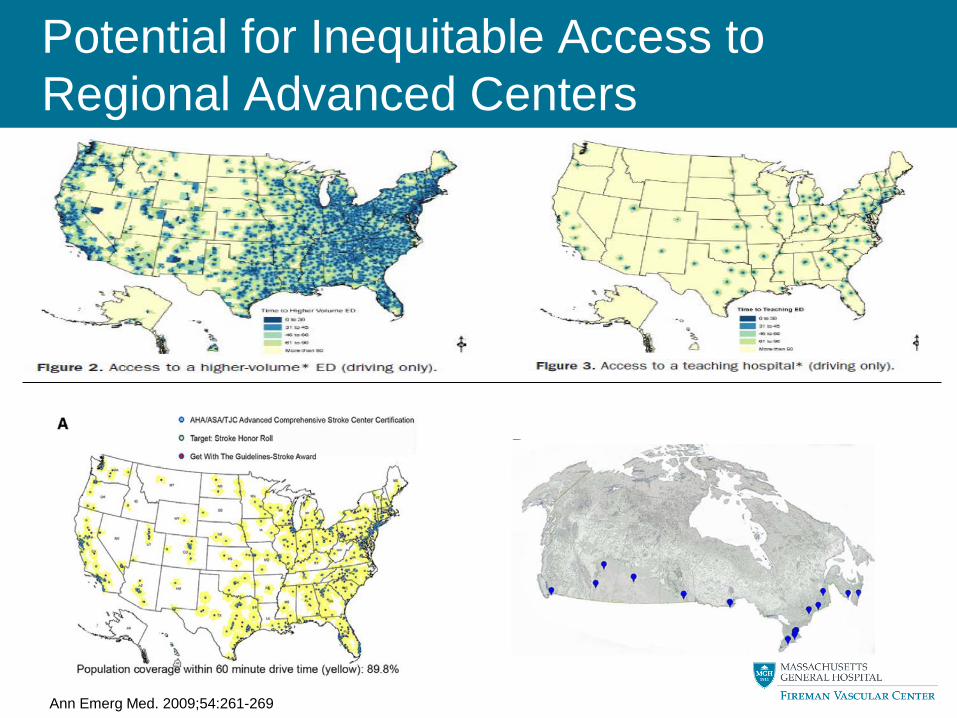
Potential for Inequitable Access to Regional Advanced Centers
Ann Emerg Med. 2009;54:261-269

Drip and Ship: Turning tPA Treatment Online in Community Hospitals
28 Sheth. Stroke. 2015;46:732-739

How Must We Change in Light of the Compelling EVT Evidence of Benefit?
• Who are the Right Patients?
• What are the Right Places?
• How Soon is the Right Amount of Time?
– 6 v. 8 v. 12 hr?
– Is Time Relevant if Imaging is Favorable?
• How Should we Accomplish this?
29

Pick Your First Dance Partner Carefully
Hard to get out of..
Herrin. Arch Intern Med. 2011 Nov 28;171(21):1879-86. Prabhakaran. Stroke. 2011; 42:1626-1630
Median DIDO for PPCI: 64 (43,104) min Goal <30 min
For EVT in Stroke: Median hospital-to-hospital distance was 14.7 (IQR 8.5–21.9) miles and median transfer time was 104 (IQR 80 –135) min. odds of treatment decrease by 2.5% for every min of transfer time.
Easy to get into..

It’s Boogie Time: Time is Still Brain
31 Khatri. Neurology. 2009 Sep 29; 73(13): 1066–1072.

How Must We Change in Light of the Compelling EVT Evidence of Benefit?
• Who are the Right Patients?
• What are the Right Places?
• How Soon is the Right Amount of Time?
• How Should we Accomplish this?
– What Changes to the Stroke System of Care?
– Focus on STEEEP, the 6 IOM Domains of Quality
• Safe, Timely, Effective, Efficient, Equitable and Patient-centered
32

An Educated Consumer is our Best Customer, …In Any Language!

Primary Stroke Centers
Comp Stroke
Centers
Acute Stroke Ready Hospitals
Basic Receiving Hospitals
Field Response and Triage
Paradigm for Regionalization of Stroke Care
Limited ? Advanced


Radical Redesign: London Hyperacute Stroke Unit Reorganization
• Before HASU Redesign, all potential patients went to nearest hospital • After Redesign in Gr. Manchester, AIS patients <4 hr go to PSC/CSC, and all
others to a nearby “District Stroke Center”. Once stable, they are repatriated to a DSC, nursing home, or home for community-based rehabilitation (~USA model)
• After Redesign in London, all AIS patients go to first to a HASU for assessment and treatment up to 72 hr, then repatriated to an Stroke Unit, nursing home, or home for community-based rehabilitation (Radical Change)
• HASU is staffed by rotating Acute Stroke Faculty from the London Stroke Units
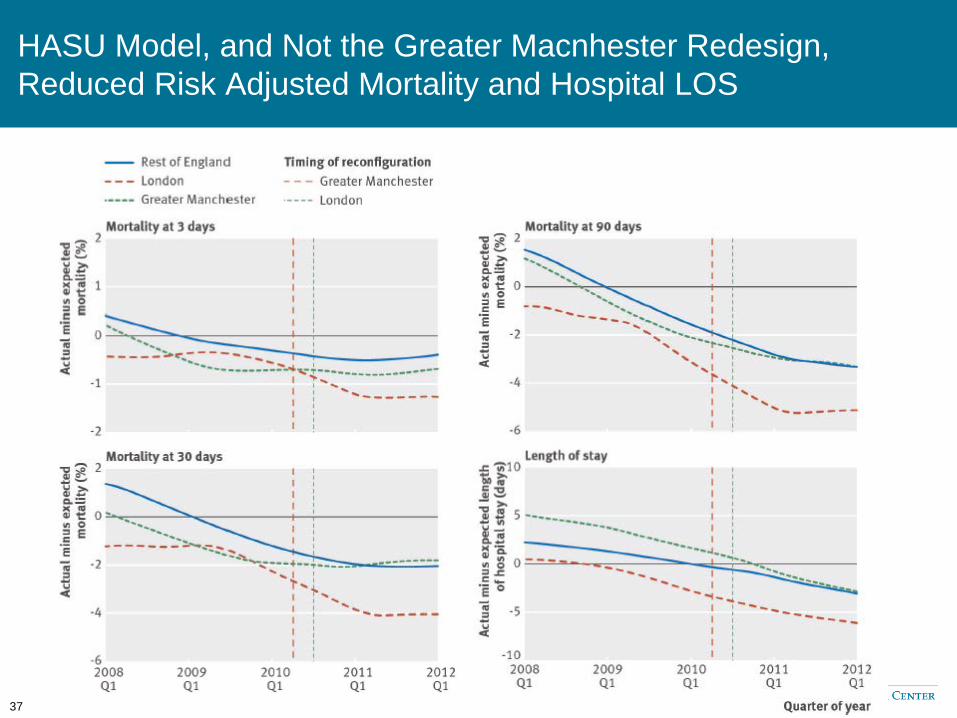
HASU Model, and Not the Greater Macnhester Redesign, Reduced Risk Adjusted Mortality and Hospital LOS
37

“Siri, I am having a stroke. Where should I go?”
Based on your estimated stroke severity, real-time traffic updates, publicly reported door to needle times and rates of thrombectomy in all hospitals reachable within 4.5 or 6 hours from your time last known well: Siri recommends:
• Immediate transport to Tiny Hospital • TeleStroke for IV tPA with DIDO <60 • Transfer to Giant Medical Center for
EVT and NeuroICU care • Activating EMS Dispatch • Performing pre-arrival notification and
requesting tPA dispensing

Going Beyond the mRS: The ICHOM Stroke Standard Set

40
Scorecard
Specificity Delay, Risk