insulin strategies in type 2 diabetes. the epidemic of type 2 diabetes and the recognition that...
TRANSCRIPT
INSULIN STRATEGIES IN TYPE 2 INSULIN STRATEGIES IN TYPE 2 DIABETESDIABETES
The epidemic of type 2 diabetes and the recognition that
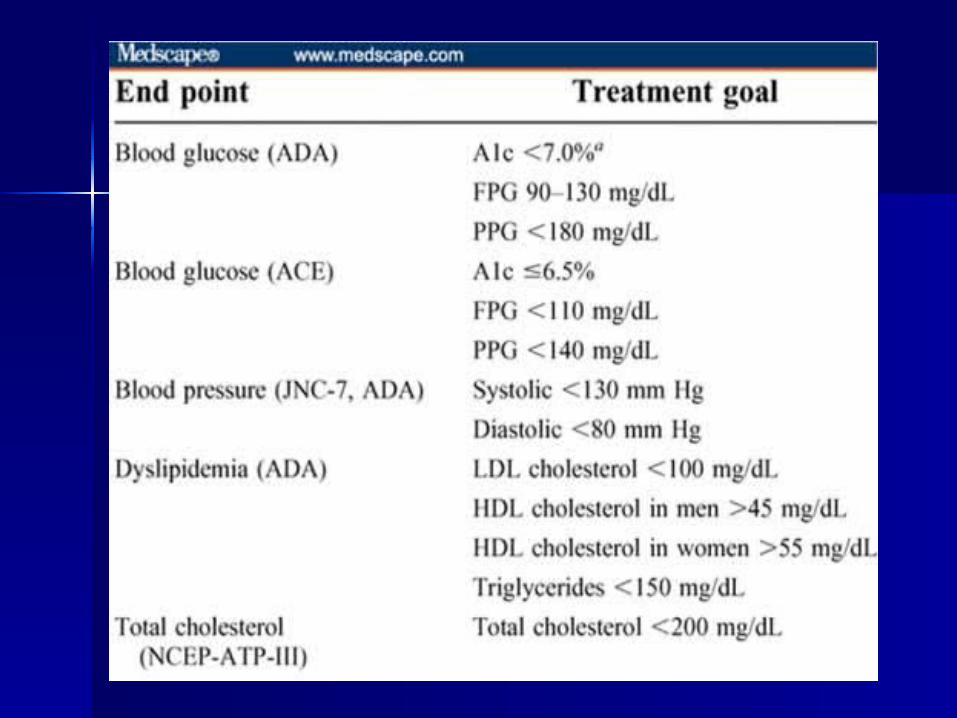
achieving specific glycemic goals can substantially reduce
morbidity have made the effective treatment of
hyperglycemia a top priority
Medical nutrition therapy (MNT), physical activity, blood glucose monitoring and patient education
are the cornerstones of diabetes management for all patients. Pharmacological management should be used in combination with MNT and physical activity
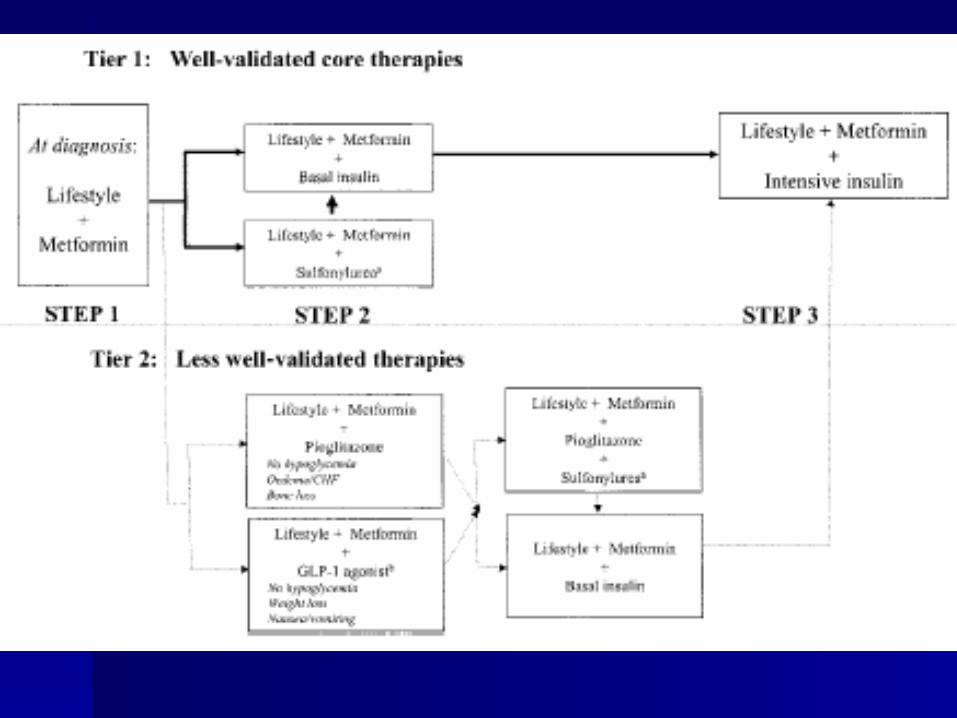
Although the treatment options for Type 2 diabetes have expanded rapidly in recent years with the development of new oral therapies, the abilities of these agents to lower blood glucose to reach and sustain glycemic targets is limited
·Type 2 diabetes is a progressive disease with worsening hyperglycemia due mainly to a relentless decline in insulin secretion.
As our understanding of the natural history and progressive course of Type 2 diabetes increases so does the need for more effective blood glucose lowering therapies
Insulin has been viewed traditionally as a last resort, to be used only when all other treatment options have been exhausted
·However, significant improvements in insulin therapy are beginning to remove the barriers to initiation of insulin replacement in Type 2 diabetes
·Insulin should now be viewed as a valuable therapeutic tool for early intervention, to attain and maintain target levels of blood glucose control
Early Insulin Replacement in Type 2 diabetesEarly Insulin Replacement in Type 2 diabetes
There are two defects that, together, cause Type 2 diabetes:impaired insulin secretion with progression towards insulin deficiencyand insulinn resistance
Impaired insulin secretion is a result of initial beta
cell dysfunction and subsequent insulin deficiency,
while insulin resistance results in increased hepatic glucose
production and reduced peripheral glucose uptake
.There is evidence that beta cell dysfunction begins prior to the onset of Type 2 diabetes and, indeed, can predict the progression from normal glucose tolerance (NGT) to impaired glucose tolerance (IGT) to Type 2 diabetes
Short-term intensive therapy has been shown to improve insulin resistance, possibly bycorrecting glucotoxicity and lipotoxicity
· The reduced strain on the beta cell by insulin therapy can potentially induce ‘beta cell
rest’,which results in increased insulin secretion
· Clinical support for this ‘beta cell rest’ hypothesis One could speculate from this
observation that earlier initiation of insulin therapy – perhaps even from disease onset –
could preserve beta cell function and, thus, insulin secretion, which could prevent disease
progression and/or improve glycemic responses to supplemental oral treatment if needed
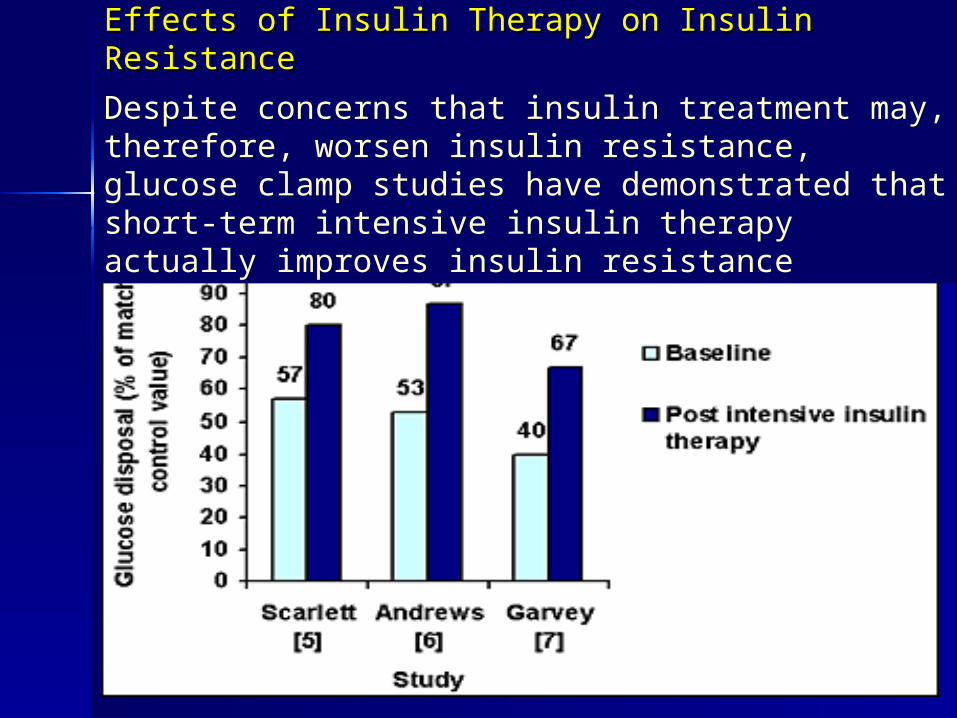
Effects of Insulin Therapy on Insulin ResistanceEffects of Insulin Therapy on Insulin Resistance
Despite concerns that insulin treatment may, therefore, worsen insulin resistance, glucose clamp studies have demonstrated that short-term intensive insulin therapy actually improves insulin resistance
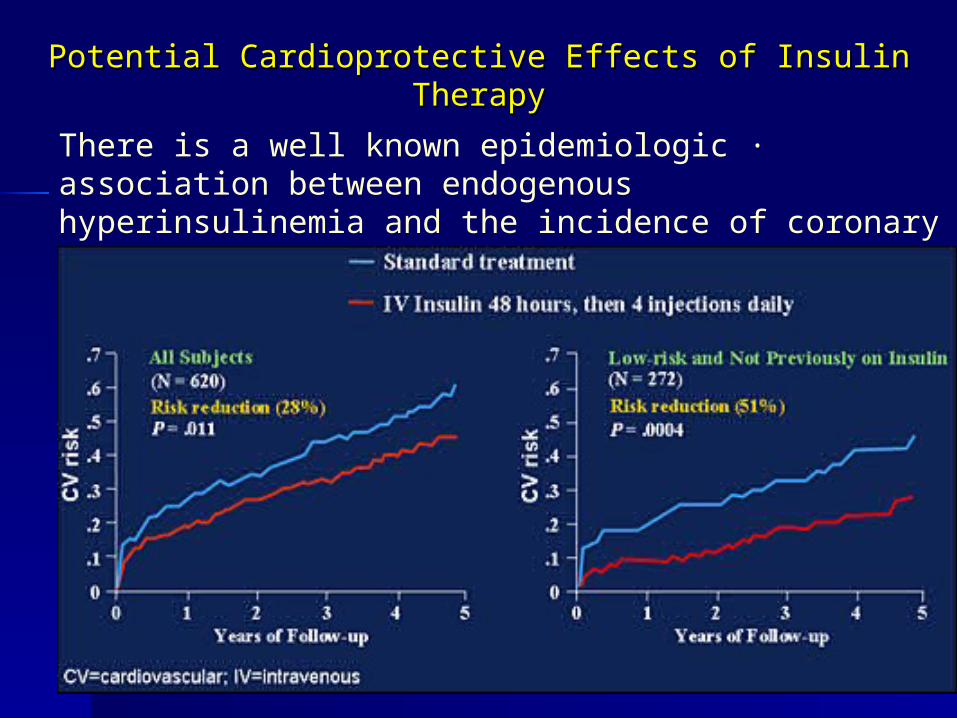
Potential Cardioprotective Effects of Insulin TherapyPotential Cardioprotective Effects of Insulin Therapy
·There is a well known epidemiologic association between endogenous hyperinsulinemia and the incidence of coronary heart disease in non-diabetic individuals
Barriers to Insulin TherapyBarriers to Insulin Therapy
·Despite evidence that insulin therapy may be most beneficial in patients with Type 2 diabetes physicians also have numerous barriers to insulin
therapy including:
–Exaggerated concern that insulin therapy may cause significant weight gain in patients with Type 2 diabetes
–Valid concerns that the risk of hypoglycemia will be increased
–Misconceptions from the epidemiologic non-interventional studies about endogenous insulin as a factor that may increase cardiovascular risk
–Limited resources and time constraints to instruct patients with Type 2 diabetes how to inject and adjust insulin therapy
–patients will not accept insulin
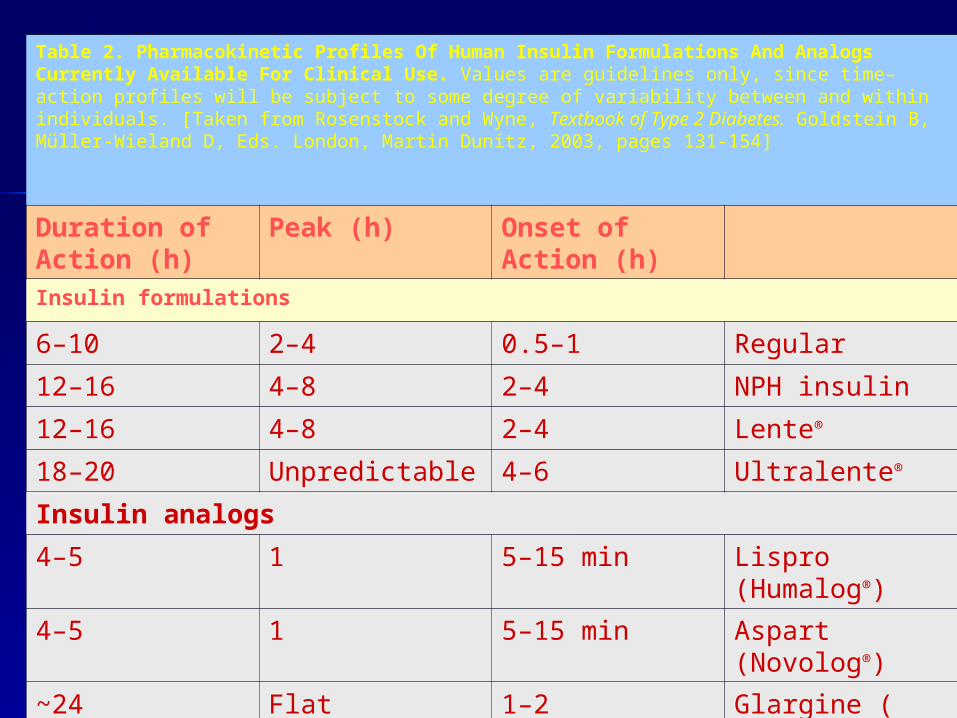
Table 2. Pharmacokinetic Profiles Of Human Insulin Formulations And Analogs Currently Available For Clinical Use. Values are guidelines only, since time–action profiles will be subject to some degree of variability between and within individuals. [Taken from Rosenstock and Wyne, Textbook of Type 2 Diabetes. Goldstein B, Müller-Wieland D, Eds. London, Martin Dunitz, 2003, pages 131-154]
Onset of Action (h)
Peak (h)Duration of Action (h)Insulin formulations
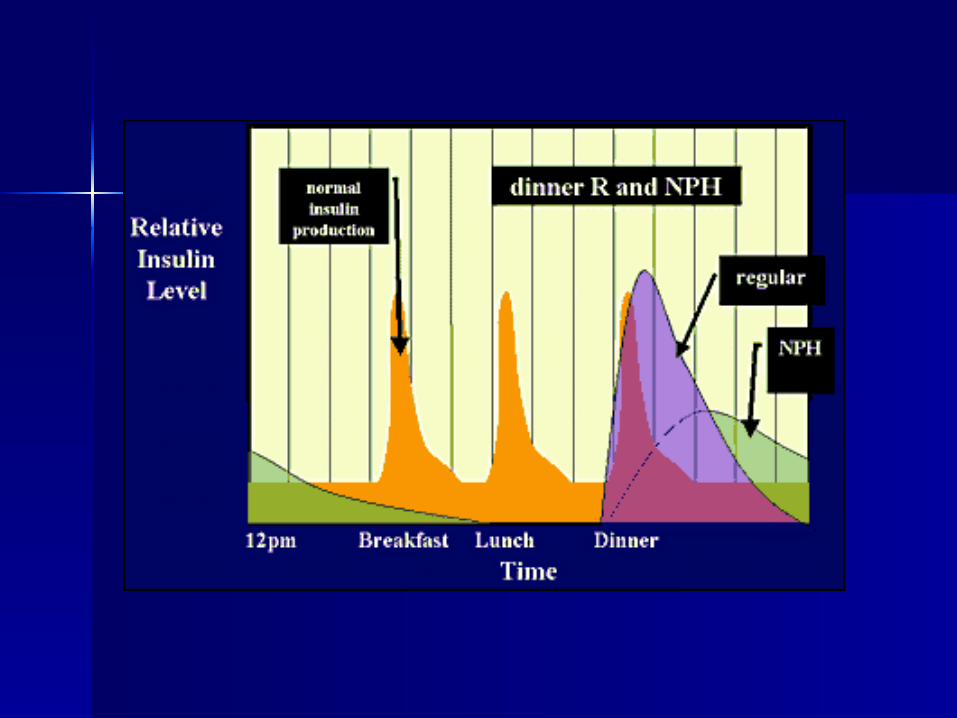
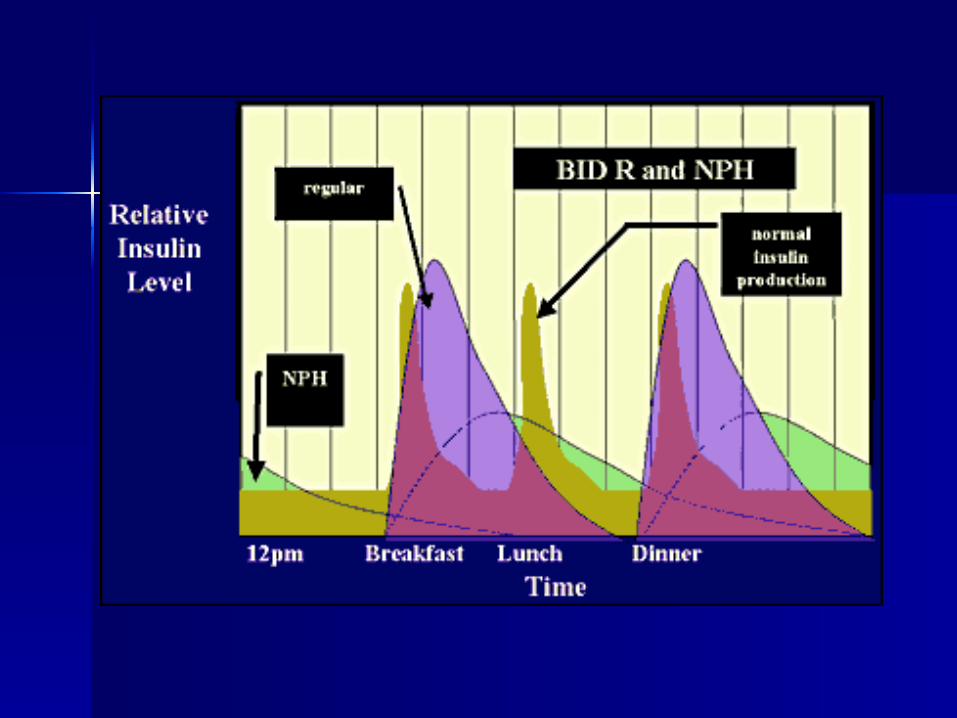
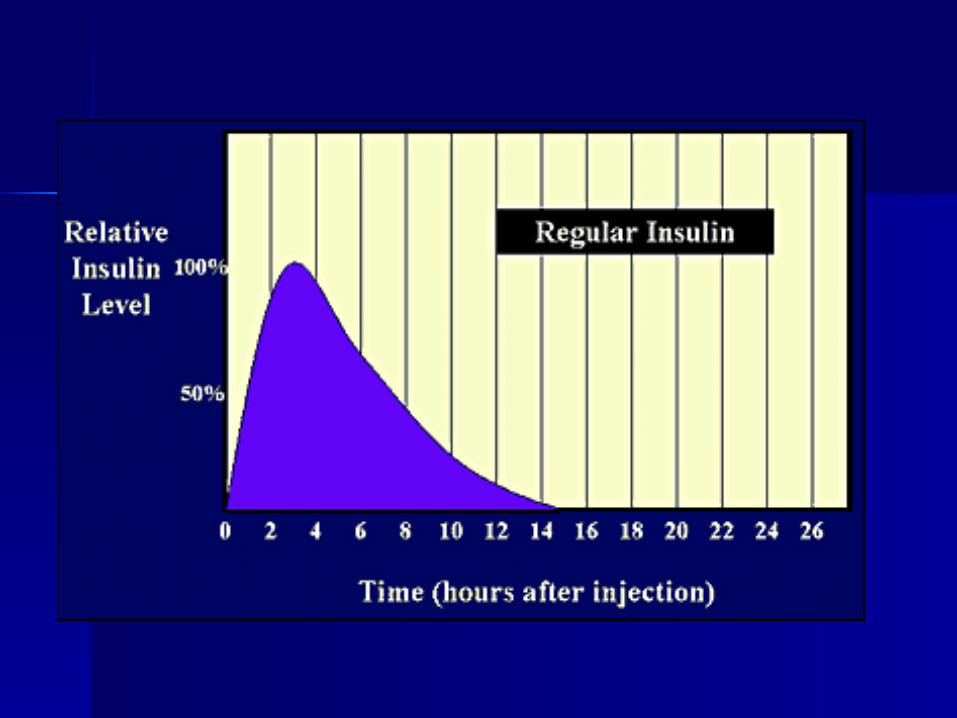
Regular0.5–12–46–10
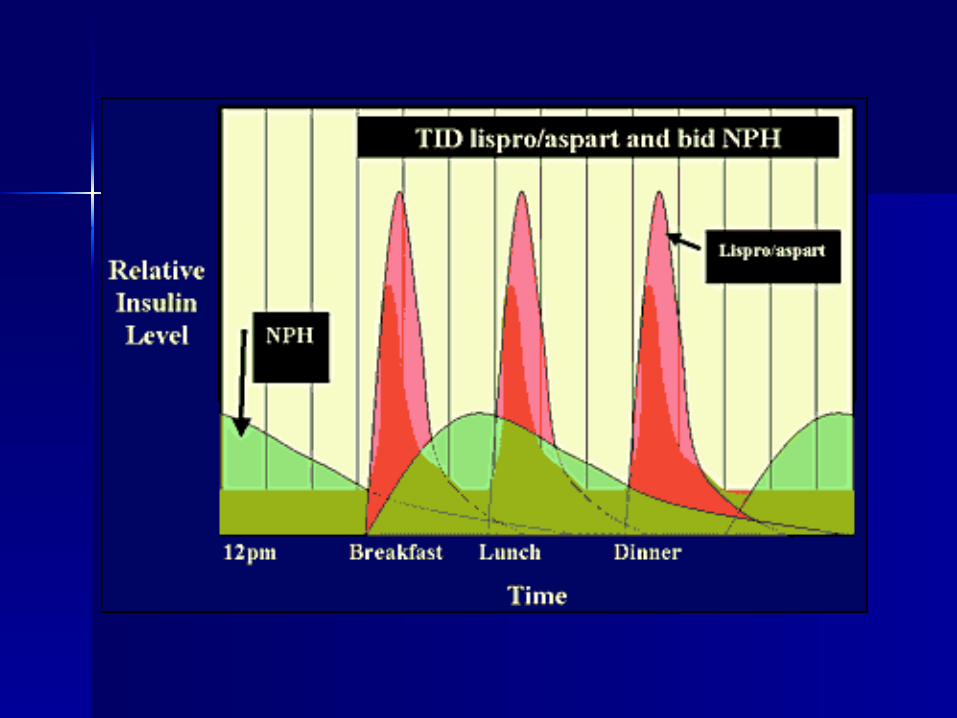
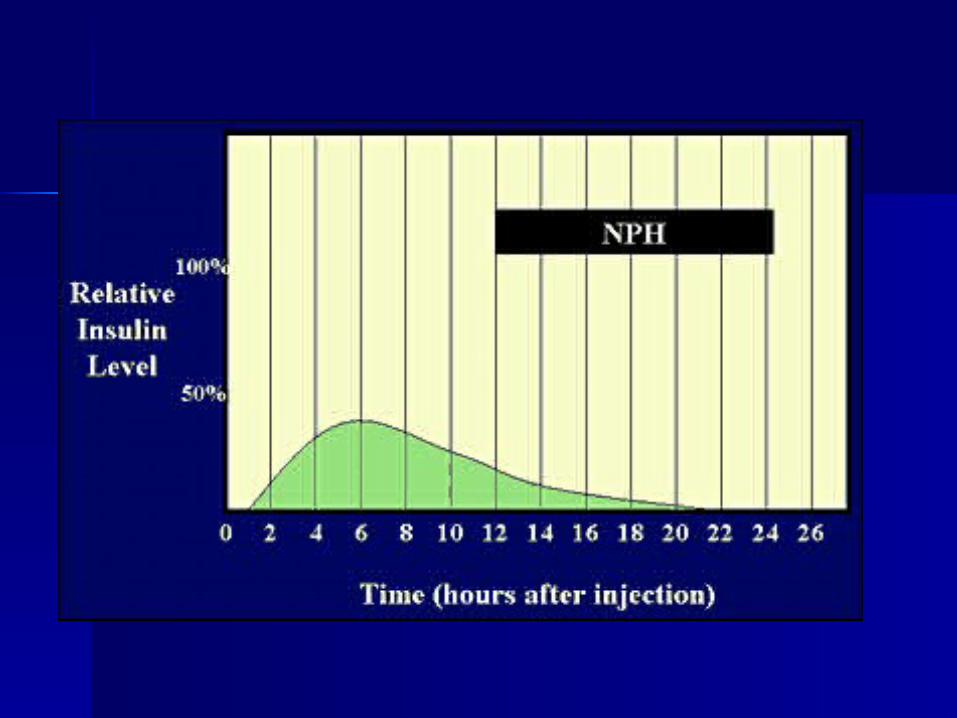
NPH insulin2–44–812–16
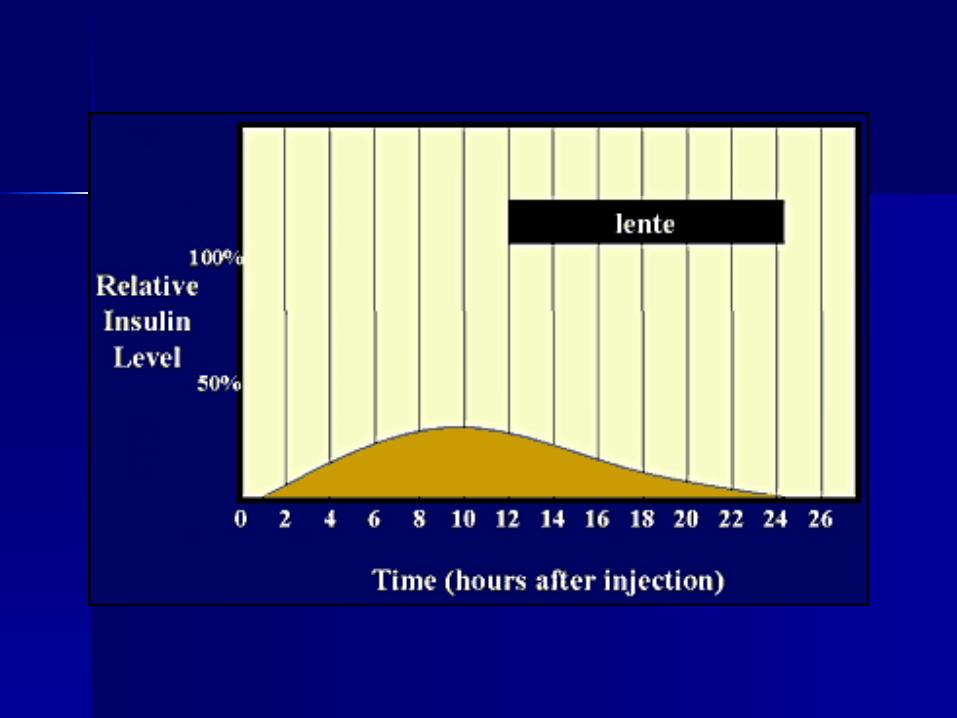
Lente®2–44–812–16
Ultralente®4–6Unpredictable18–20
Insulin analogs
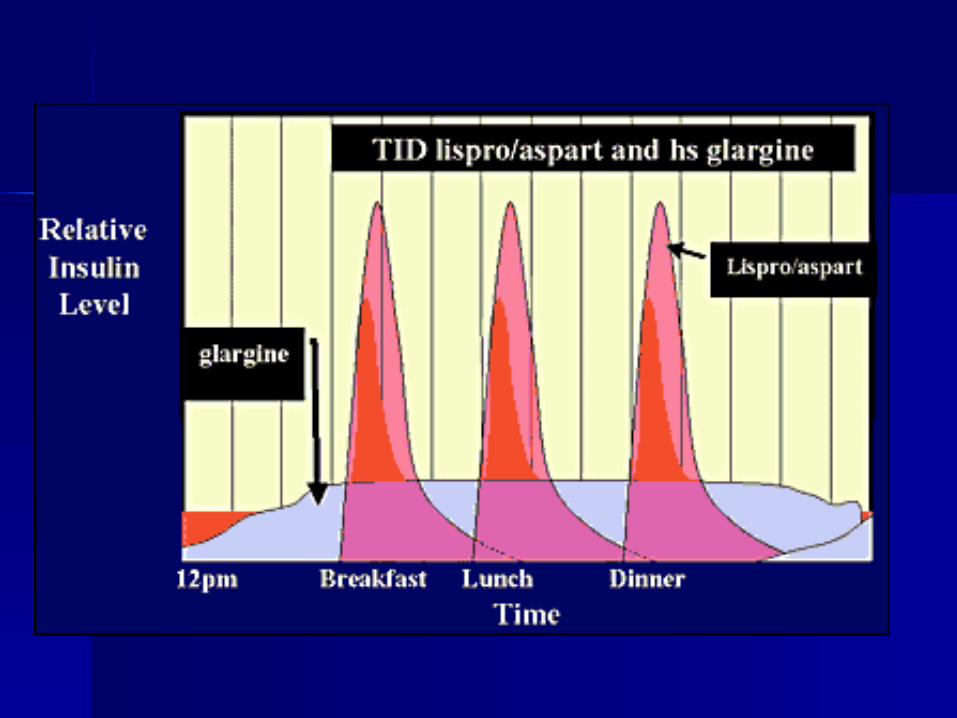
Lispro (Humalog®)5–15 min14–5
Aspart (Novolog®)5–15 min14–5
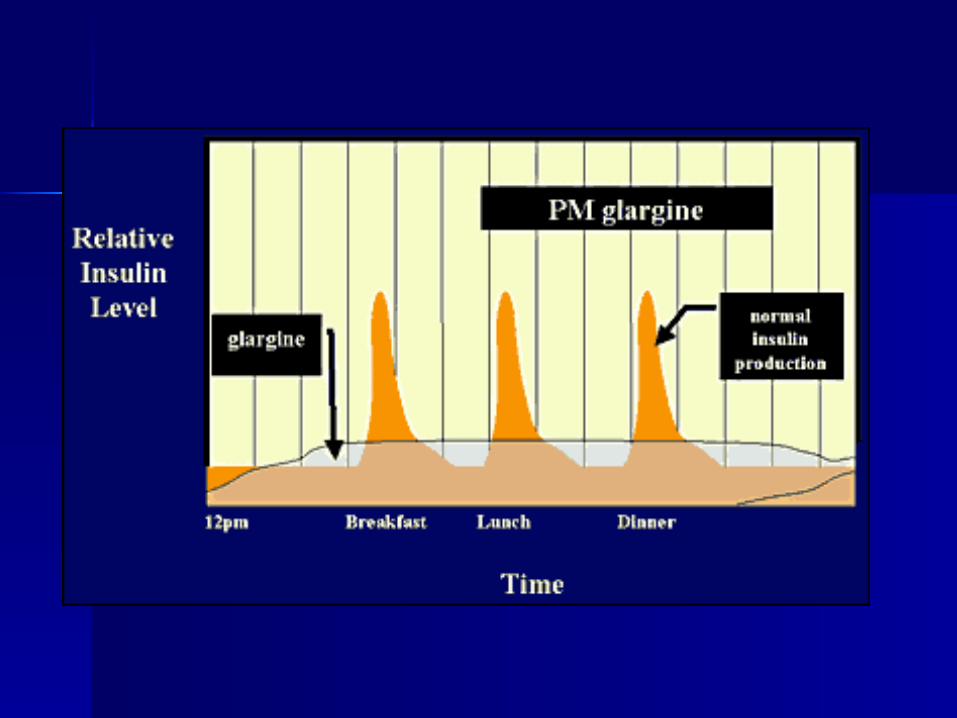
Glargine (Lantus®)1–2Flat~24
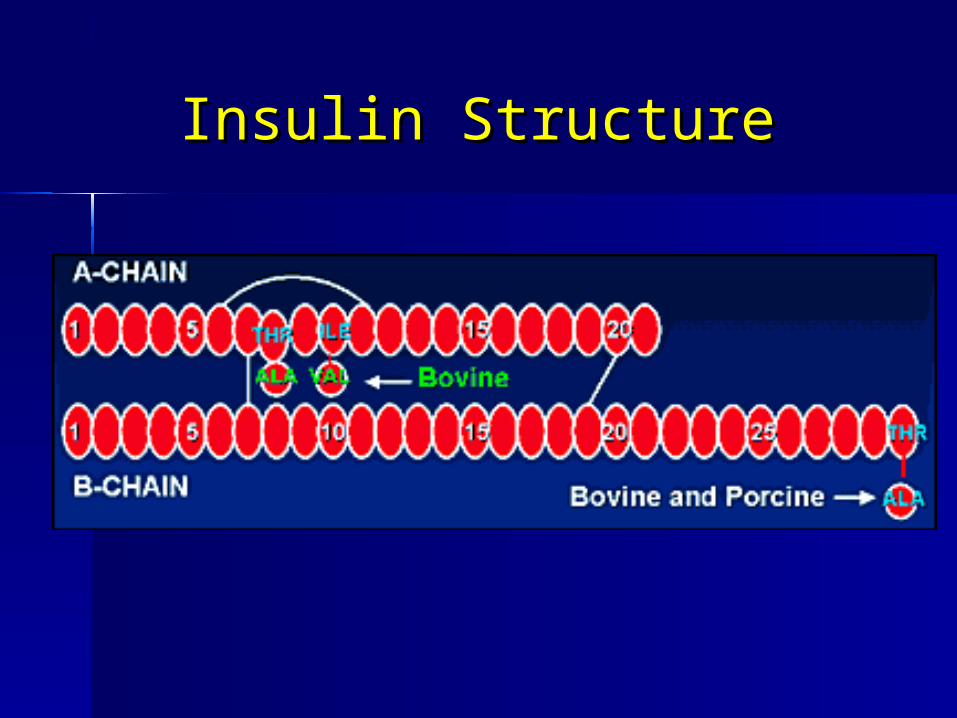
Insulin StructureInsulin Structure
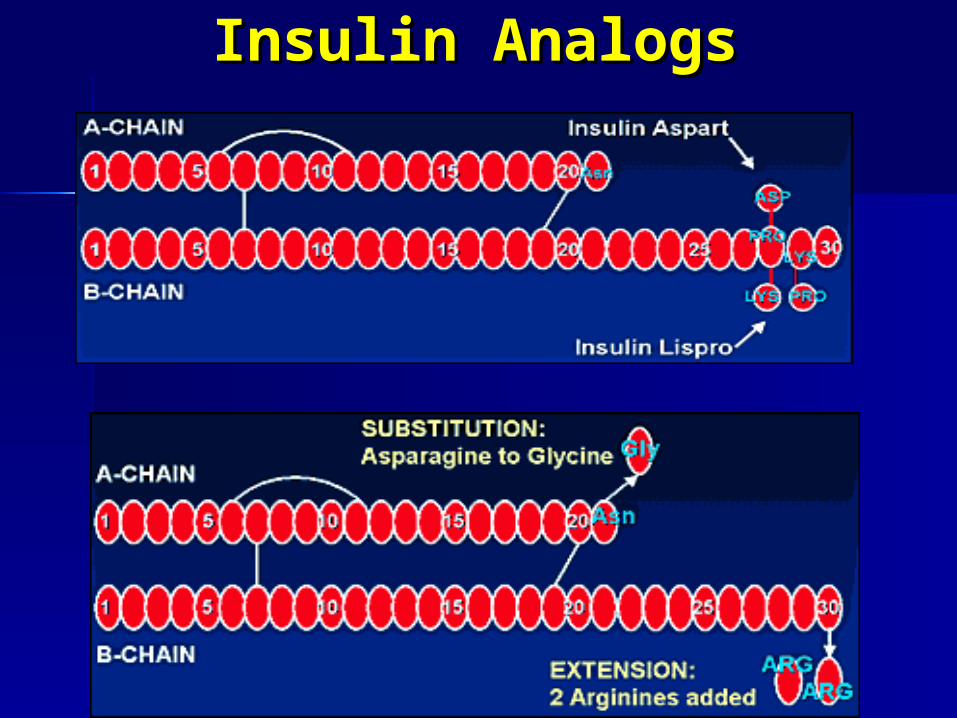
Insulin AnalogsInsulin Analogs
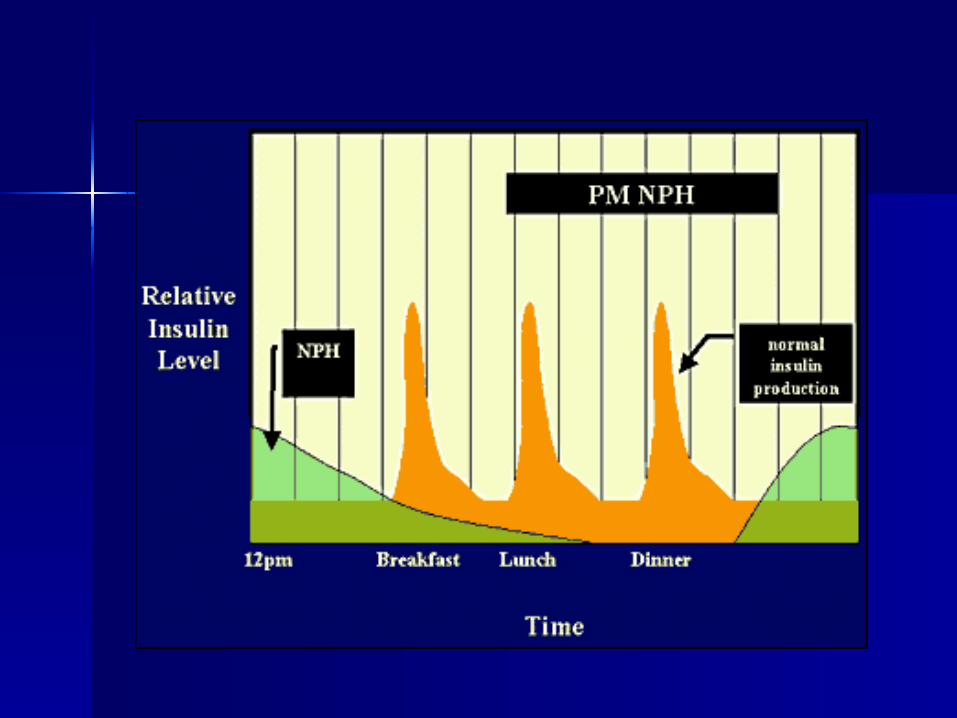
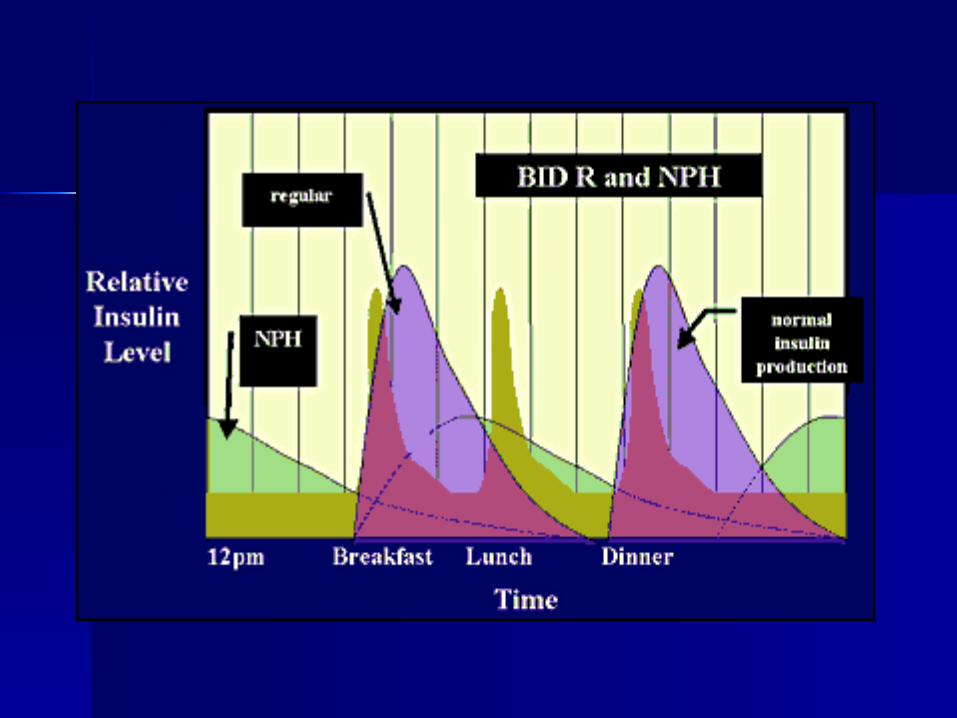
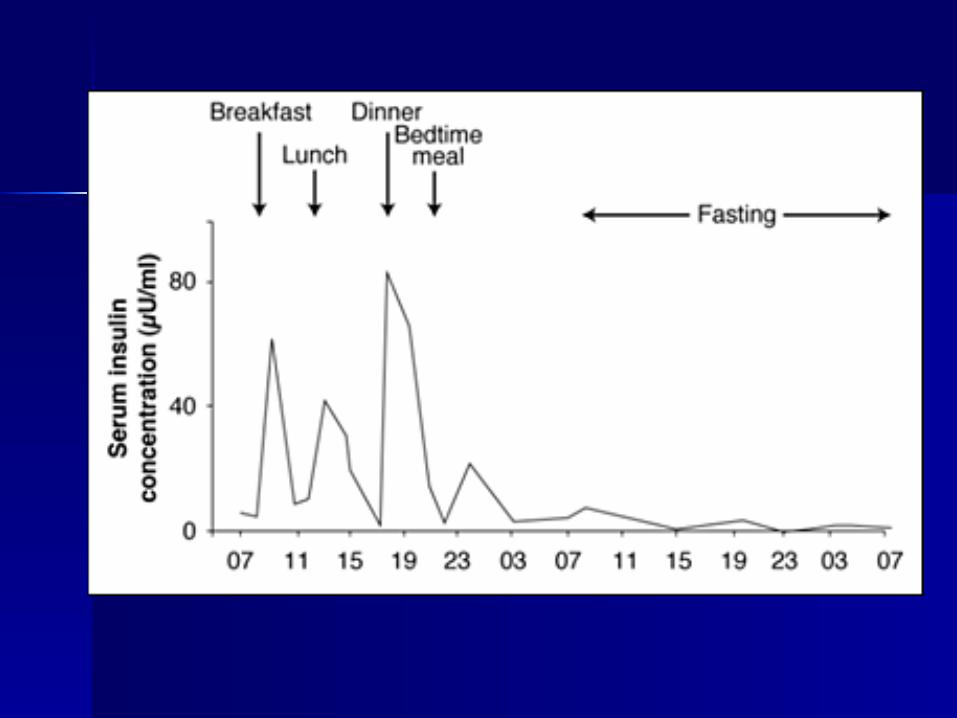
Physiologic Insulin Replacement
A functioning pancreas releases insulin continuously, to supply a basal amount to suppress hepatic glucose output between meals and overnight, and also releases a bolus of insulin prandially to promote glucose utilization after
eating
. Replacing insulin in a manner that attempts to mimic physiologic insulin release is often referred to as the basal/bolus concept
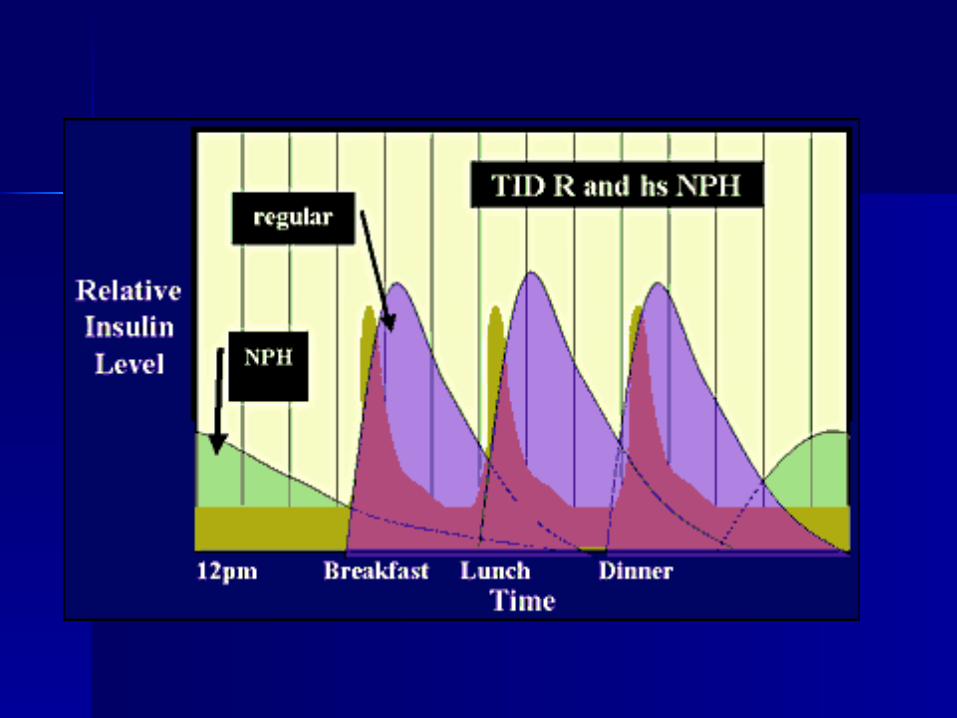
This physiologic replacement requires multiple daily
injections (3 or more) or use of an insulin pump.
Basal insulin requirements are approximately 50% of
the total daily amount
Prandial insulin is ~10-20% of the total daily
insulin requirement at each meal
Limitations of Traditional Human Insulin FormulationsLimitations of Traditional Human Insulin Formulations
·Regular human insulin is less than ideal for post-prandial glucose control:
–The slow onset of action necessitates administration 20–40 minutes before meals, putting patients at risk of pre-meal hypoglycemia if the meal is delayed
–The duration of action extends beyond the duration of endogenous insulin activity, therefore, the risk of hypoglycemia is increased; this encourages between-meal snacking, which promotes weight gain in Type 2 diabetes
·Insulin lispro and aspart are two short-acting insulin analogs with increased rate of dissociation into insulin monomers resulting in rapid absorption profiles that allow for more physiologic replacement of mealtime insulin requirements