insert catchy title - c.ymcdn.comc.ymcdn.com/sites/ · 7/26/2013 · intellectual disabilities...
TRANSCRIPT
7/24/2013
1
Robin DuFresne, MA, PC, NCC
Allison Arnekrans, MA, PCC, NCC
July 26, 2013
Updating Your Clinical Toolkit: Understanding and Applying DSM-5
Changes with Children & Adolescents
Objectives
Overview of major DSM-IV to 5
changes.
Review current Neurodevelopmental
Disorders in the DSM-5.
Identify and apply changes to the
Disruptive, Impulse-Control, and
Conduct Disorders chapter.
DSM-IV-TR DSM-5 First DSM published in 1952.
◦ It had 106 diagnoses and 130 pages.
DSM-5 will be the first full revision since 1994.
◦ It has over 340 diagnoses and 947 pages.
◦ More developmental and evidence-based approach.
◦ Represents the contributions of more than 1,500 mental health and medical experts over a 14-year process of discussion and collaboration.
7/24/2013
2
Utilization
You can start using DSM-5 today! ◦ APA encourages utilization by 12/31/13.
Claim: “The new manual represents a step forward in more precisely identifying and diagnosing mental disorders.” ◦ DSM-5 will continue to use statistical
codes in the International Classification of Diseases (ICD).
DSM Code & ICD for most diagnoses (i.e. 313.81 (F91.3).
Changes in Reporting Structure
DSM-5 combines the first three DSM-IV-TR axes into one list that contains: ◦ All Mental Disorders
◦ Personality Disorders
◦ Intellectual Disabilities
◦ Medical Diagnosis
Psychosocial and environmental factors now represented through an expanded selected set of ICD-9-CM: V-codes and from the forthcoming ICD-10-CM: Z-Codes.
GAF is no more. . .
NOS categories replaced with two options:
1.) other specified disorder and 2.) unspecified disorder
Other Noteworthy Changes…
Some different disorders or subtypes share same diagnostic codes.
The diagnostic groups have been deleted or reconfigured. (e.g. PTSD no longer included in Anxiety group;
Disorders of Infancy, Childhood, & Adolescence has been eliminated)
◦ 17 groups in total
Dimensional component. ◦ No more NOS labeling More specificity
through dimensional labeling.
Categories more sensitive to gender and cultural differences.

7/24/2013
3
Neuro-
Developmental
Disorders
Intellectual Disabilities (319.)
Previously Mental Retardation
Diagnosis based on cognitive capabilities and adaptive functioning: ◦ Adaptive functioning level determines severity Mild (F70), Moderate (F71), Severe (F72), and
Profound (F73)
Intellectual Developmental Disorder is ICD title for disorder
Additional Diagnoses of: ◦ 315.8 (F88) Global Developmental Delay
◦ 319 (F79) Unspecified Intellectual Disability
Communication Disorders
Language Disorder 315.39 (F80.9)
◦ Combination of Expressive and Mixed
Receptive Expressive Disorder
Speech Sound Disorder 315.39 (F80.0)
◦ Phonological Disorder
Childhood-Onset Fluency Disorder
315.35 (F80.81)
◦ Stuttering
7/24/2013
4
Communication Disorders (continued)
Social (Pragmatic) Communication Disorder 315.39
(F80.89)
◦ New addition in DSM-5
◦ Persistent difficulties in social use of verbal and
nonverbal communication
◦ Cannot be diagnosed when concurrent with
restrictive repetitive behaviors, interests or
activities (See Autism)
◦ Encompasses some symptoms of Pervasive
Developmental Disorder NOS
Unspecified Communication Disorder 307.9 (F80.9)
◦ No changes
Autism Spectrum Disorder (ASD)
299.00 (F84.0)
Combination of Autism, Asperger’s,
Pervasive Developmental Disorder NOS,
and Childhood Disintegrative Disorder.
Two core domains:
◦ Social communication and social interaction
◦ Restricted repetitive behaviors, interests and
activities
Autism Spectrum Disorder (continued)
Specifiers ◦ Associated with known medical or genetic
condition or environmental factor ◦ Associated with another
neurodevelopmental, mental or behavioral disorder
◦ Severity With very substantial support
With substantial support
With support
◦ Accompanied by intellectual impairment
◦ Accompanied by language impairment
◦ Accompanied by catatonia

7/24/2013
5
Asperger’s Integration into ASD
DSM-IV-TR ◦ Impairment in social interaction ◦ Restricted repetitive and stereotyped patterns
of behavior, interest and activities
◦ No delay in language
◦ No clinically significant delay in cognitive development, age appropriate self-help skills, adaptive behavior and curiosity about the environment
DSM-5 ◦ Autism Spectrum Disorder with no intellectual
impairment, without language impairment, requiring support
Childhood Disintegrative
Disorder into ASD
DSM-IV-TR ◦ Normal development in all areas for at least first
two years of life ◦ Loss of previously acquired skills before the age
of 10 in two areas
◦ Abnormal functioning in two of the three areas of social interaction, communication, or restrictive, repetitive and stereotyped patterns of behavior, interests and activities
DSM-5 ◦ Autism Spectrum Disorder with intellectual
impairment, with or without language impairment, and determine support level.
Pervasive Developmental
Disorder NOS into ASD
DSM-IV-TR
◦ Used when severe and pervasive impairment in development of reciprocal social interaction with either Impairment in verbal or non-verbal communication
OR
Presence of stereotyped behavior, interests and activities
DSM-5
◦ Autism Spectrum Disorder without intellectual disorder, with or without language impairment, and specify support level
7/24/2013
6
Attention-Deficit/Hyperactivity
Disorder (ADHD) 314.00/.01
Moved to Neurodevelopmental chapter when chapter addressing diagnosis usually first made in infancy, childhood or adolescents was eliminated.
Application across the lifespan
Cross-situational requirement necessities several symptoms in each setting
Onset changed from before 7-years to symptoms were present prior to age 12
Subtypes replaced by presentation specifiers
Can be diagnosed co-morbid with Autism
Addition of symptom threshold for adults
Specific Learning Disorder
Combination of reading disorder, mathematics disorder, disorder of written expression and learning disorder NOS
Specifiers: ◦ 315.00 (F81.0) Impairment in reading
◦ 315.2 (F81.81) Impairment in written expression
◦ 315.1 (F81.2) Impairment in mathematics
◦ Severity (Mild, Moderate, Severe)
Motor Disorders
Developmental Coordination Disorder 315.4 (F82)
Stereotypic Movement Disorder 307.3 (F98.4)
Tourette’s Disorder 307.23 (F95.2)
Tic Disorders ◦ Persistent Motor or Vocal Tic Disorder 307.22
(F95.1)
◦ Provisional Tic Disorder 307.21 (F95.0)
◦ Other Specified Tic Disorder 307.2 (F95.8)
◦ Unspecified Tic Disorder 307.2 (F95.9)

7/24/2013
7
Other Neurodevelopmental
Disorders
Other Specified Neurodevelopmental
Disorders 315.8 (F88)
Unspecified Neurodevelopmental
Disorder 315.9 (F89)
Disruptive,
Impulse-Control,
and Conduct
Disorders
New Chapter in DSM-5
Brings together disorders that were
previously included in two others chapters.
Disorders all characterized by problems in
emotional and behavioral self-control.
◦ Because of its close association with Conduct
Disorder, Antisocial Personality Disorder has
dual listing in this chapter.
◦ ADHD often co-morbid with the disorders in this
chapter but its listed with Neurodevelopmental
disorders.

7/24/2013
8
Oppositional Defiant Disorder
313.81 (F91.3) Symptoms now grouped into three types: ◦ Angry/irritable mood ◦ Argumentative/defiant behavior, and
◦ Vindictiveness
Exclusion criterion for Conduct Disorder has been removed.
A note has been added to the criteria to provide guidance on the frequency typically needed for a behavior to be considered symptomatic of the disorder.
Severity Rating has been added.
Oppositional Defiant Disorder
313.81 (F91.3) Specifiers:
◦ MILD: Symptoms are confined to
only one setting (e.g. at home, at
school, at work, with peers.)
◦ MODERATE: Some symptoms are
present in at least 2 settings.
◦ SEVERE: Some symptoms are
present in three or more settings.
Intermittent Explosive Disorder
312.32 (F63.81) Type of aggressive outbursts that should
be considered: ◦ Physical aggression was required in DSM-IV,
whereas verbal aggression and non-destructive/noninjurious physical aggression also meet criteria in DSM-5.
More specific symptomology defining the frequency needed to meet criteria added.
Minimum age of 6-years (or equivalent developmental level) now required.
Relationship of this disorder to other disorders has been clarified.
7/24/2013
9
Conduct Disorder
Largely unchanged from IV 5
Conduct disorder is characterized by behavior that violates either the rights of others or major societal norms. ◦ Symptoms must be present for at least three
months with one symptom having been present in the past six months.
◦ The symptoms must cause significant impairment in social, academic or occupational functioning.
◦ Typically diagnosed prior to adulthood.
Conduct Disorder Specifiers
◦ Specify whether:
312.81 (F91.1)- Childhood-onset type: at least
one symptom prior to age 10.
312.82 (F91.2)- Adolescent-onset type: no
symptom characteristic of conduct disorder
prior to age 10 years.
312.089 (F91.9)- Unspecified onset: Criteria for
CD are met, but there is not enough
information available to determine whether
onset was before or after age 10.
Conduct Disorder Specifiers
Specify if: ◦ With limited prosocial emotions:
Individual must have displayed at least 2 characteristics over at least 12 months and in multiple relationships/settings. Reflect typical behavior versus occasional functioning.
Lack of remorse or guilt
Callous- lack of empathy
Unconcerned about performance
Shallow or deficient affect
7/24/2013
10
Conduct Disorder Specifiers
MILD
• Few problems in excess are present.
• Problems cause minor harm.
MODERATE
• Number and effect are intermediate
SEVERE
• Many problems in excess are present.
• Cause considerable harm to others.
Other Disorders
No Significant Changes to:
◦ Pyromania
312.33 (F63.1)
◦ Kleptomania
312.32 (F63.2)
Other Disorders
Previous Disruptive Behavior Disorder
NOS broken down into two disorders…
Other Specified Disruptive,
Impulse-Control, and Conduct
Disorder 312.89 (F91.8)
•Symptoms are present, but not
enough to diagnose.
•Clinician should designate
reason.
Example: Recurrent behavioral
outbursts of insufficient
frequency
Unspecified Disruptive,
Impulse-Control, and
Conduct Disorder 312.0
(F91.9) •Used in situations in which
the clinician chooses NOT to
specify the reason that the
criteria are not met, AND
•includes presentations
where there is insufficient
information to make a more
specific diagnosis.
7/24/2013
11
Other Important
Changes with
Child and
Adolescent
Disorders
Disruptive Mood Regulation
Disorder From Depressive Disorders Group
Characterized by severe and recurrent temper outbursts that are out of proportion in intensity or duration to the situation. ◦ Occur three or more times each week for one year or
more.
Between outbursts, children with DMDD display a persistently irritable or angry mood, most of the day and nearly every day, observable by parents, teachers, or peers.
A diagnosis requires the above symptoms to be present in at least two settings (at home, at school, or with peers) for 12 or more months, and symptoms must be severe in at least one of these settings. ◦ During this period, the child must not have gone three or
more consecutive months without symptoms.
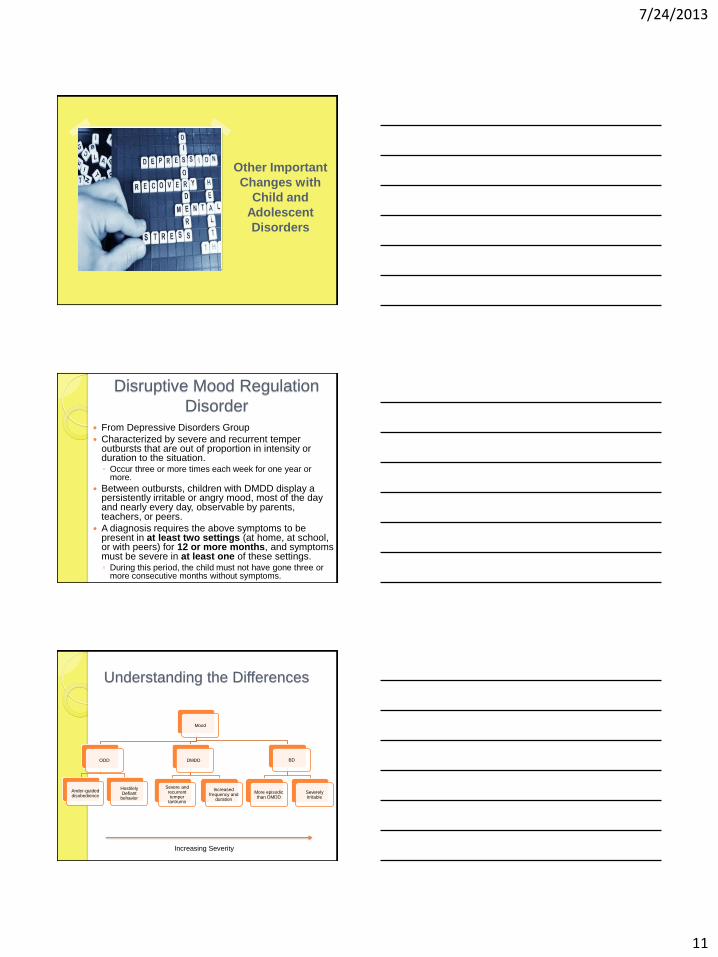
Understanding the Differences
Mood
DMDD
Severe and recurrent temper
tantrums
Increased frequency and
duration
ODD
Ander-guided disobedience
Hostilely Defiant
behavior
BD
More episodic than DMDD
Severely Irritable
Increasing Severity
7/24/2013
12
Posttraumatic Stress Disorder
New addition: Separate criteria for
Children ages 6 and younger.
See provided chart for more information.
PRESENTER CONTACT INFORMATION:
ROBIN DUFRESNE- [email protected]
ALLISON ARNEKRANS-
Questions??