inmunoterapia en cáncer de pulmón - seom: sociedad espa · 1-yr os: 42% (48 pts at risk) 2-yr os:...
TRANSCRIPT

Inmunoterapia en cáncer de pulmón
Mariano Provencio
Servicio de Oncología Médica
Hospital Universitario Puerta de Hierro

Current Therapeutic Landscape
for NSCLC
• Current treatment strategies in NSCLC
– Various chemotherapy regimens based on histologic diagnosis
– Targeted therapy options available for specific molecular
mutations
• Anti-EGFR–targeted therapy for patients with EGFR mutations
• ALK inhibitors for patients with ALK translocations
• ROS, Her2,…
• Even with various personalized approaches, the 5-yr survival
rate for patients with NSCLC (all stages) is only 17%
• The role of immunotherapy in lung cancer have
historically been associated with disappointing results
1. American Cancer Society. Cancer facts and figures 2013.


Anti-CTLA-4 Blockade
In preclinical mouse models, CTLA4 blockade in combination with various
chemotherapeutic agents was synergistic in inducing tumor regression and
elicited prolonged anti-tumor effects and induction of a memory immune response

Reck M et al. Ann Oncol 2013;24:75-83
ED-SCLC naive
Were randomized 1:1:1
Concurrent regimen:
4 doses of ipilimumab/paclitaxel/carbo followed by 2 doses of carbo/paclitaxel
Phased-ipilimumab regimen:
2 doses placebo/carbo/taxol followed 4 doses of ipilimumab/taxol/carbo
Control regimen:
Up to six doses of placebo/taxol/carbo
Ipilimumab: 10mg/Kg; taxol: 175mg/m2; carbo (AUC:6), every 3 weeks
Primary end point: immune-relatedPFS. Secondary: mWHO-PFS;OS, OPP, iBORR

Reck M et al. Ann Oncol 2013;24:75-83
Efficay
Phased-regimen
improved irPFS compared control
HR, 0.64; p:0.03
Median 5.3 vs 6.4 m

OS: phased: 12.9 m vs 9.9 m (HR:0.75) mWHO-PFS: 5.2 m vs 5.2 m control
Reck M et al. Ann Oncol 2013;24:75-83

Reck M et al. Ann Oncol 2013;24:75-83
Tumor response rates appeared to favor phased ipi,
the differences being greater when assessed by iRC

A phase III clinical trial is currently ongoing to evaluated the efficacy of ipilimumab
in addition to chemotherapy with platinum/etoposide in patients with ES-SCLC
with the primary endpoint of OS (NCT014507661)
Reck M et al. Ann Oncol 2013;24:75-83
Discontinuation were similar across arms: control 9%; concurrent 7% and phased: 5%
Overall incidence
grade 3 / 4 AES
9% control
21% concurrent
17% phased

204 patients chemotherapy-naive NSCLC
were randomly 1:1:1
Primary end point: irPFS
Other end points: PFS, ORR, irORR, OS and safety

Kaplan-Meier plots for progression-free survival
per immune-related response criteria (irPFS).
Lynch T J et al. JCO 2012;30:2046-2054
©2012 by American Society of Clinical Oncology
Phased ipilimumab regimen
improved irPFS significantly
compared with control
HR: 0.72; p: 0.05
Median irPFS: 4.6 m control
5.7 m phased
5.5 m concurrent
Median WHO-PFS: 4.2 m control
5.1 m phased
4.1 concurrent

Kaplan-Meier plots for overall
survival (OS).
Lynch T J et al. JCO 2012;30:2046-2054
Median OS phased ipili was: 12.2 m vs 8.3 m control (> 3.9m) HR: 0.87, p:0.23
in squamous/phased regimen: HR: 0.48 (0.22-1.03) vs nonsquamous HR: 1.17
In phased regimen
irPFS greater in patients with squamous histology: HR: 0.55 (95% CI, 0.27-1.12)
also in WHO-PFS ( HR: 0.40 (95% CI, 0-18-0.87)

PD-1 and PD-L1 Antibodies
Agent
Anti PD-L1
MPDL3280A (Genetech)
MEDI-4736 (Astra)
BMS 936559 (BMS)
MSB0010718C (Merck)
Anti PD 1
Nivolumab (BMS)
MK-3475 Pembrolizumab (Merck)
Pidilizumab (CureTch)
AMP 224 (Glaxo)
AMP 514 (Astra)

PD-L2–mediated
inhibition of TH2 T cells Stromal PD-L1
modulation of T cells
Reprinted from Clinical Cancer Research. 2013;19(5):1021-1034. Sznol M, et al. Antagonist antibodies to PD-1 and B7-H1
(PD-L1) in the treatment of advanced human cancer.
Blockade of PD-1 Binding to PD-L1 (B7-H1) and PD-L2 (B7-DC) Revives T Cells
• PD-L1 expression on tumor cells is induced by γ-interferon
• In other words, activated T cells that could kill tumors are specifically disabled by those tumors
PD-1
PD-L1
PD-L2
T-cell receptor
MHC-1
CD28
Shp-2
B7.1
IFN-γ–mediated
upregulation of
tumor PD-L1 PD-L1/PD-1–mediated
inhibition of tumor cell killing
Priming and
activation of
T cells
Immune cell
modulation of T cells
Tumor cell
IFN-γR
IFN-γ
Tumor-associated
fibroblast M2
macrophage
Treg
cell
Th2
T cell
Other NFκB P13K
CD8+ cytoxic
T lymphocyte
T-cell polarization
TGF-β
IL-4/13
Can you generate
tumor-killing T cells?
Dendritic
cell
Antigen priming
Can the T cells
get to the tumor?
T-cell trafficking
Can the T cells
see the tumor?
Peptide-MHC
expression
Can the T cells
be turned off?
Inhibitory cytokines
Can the T cells
be turned off?
PD-L1 expression
on tumor cells
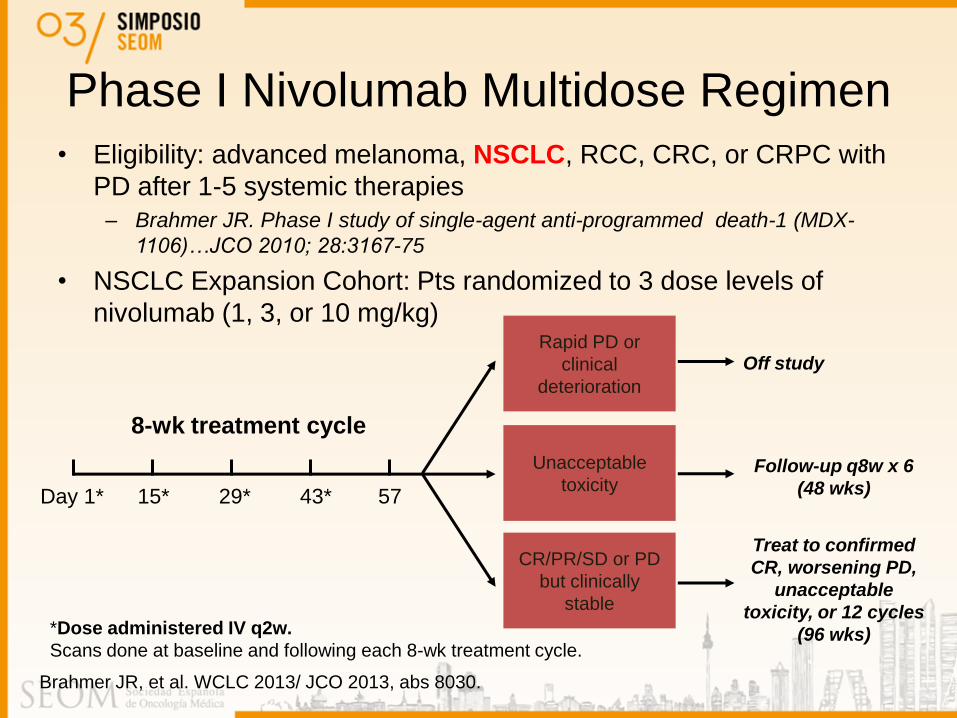
Phase I Nivolumab Multidose Regimen
• Eligibility: advanced melanoma, NSCLC, RCC, CRC, or CRPC with
PD after 1-5 systemic therapies
– Brahmer JR. Phase I study of single-agent anti-programmed death-1 (MDX-
1106)…JCO 2010; 28:3167-75
• NSCLC Expansion Cohort: Pts randomized to 3 dose levels of
nivolumab (1, 3, or 10 mg/kg)
Day 1* 15* 29* 43* 57
Follow-up q8w x 6
(48 wks)
Treat to confirmed
CR, worsening PD,
unacceptable
toxicity, or 12 cycles
(96 wks)
Off study
*Dose administered IV q2w.
Scans done at baseline and following each 8-wk treatment cycle.
Rapid PD or
clinical
deterioration
Unacceptable
toxicity
CR/PR/SD or PD
but clinically
stable
8-wk treatment cycle
Brahmer JR, et al. WCLC 2013/ JCO 2013, abs 8030.

Efficacy of Nivolumab Monotherapy in Patients With NSCLC
(N=129)
• Durable responses: responses are ongoing in 45% of patients (10/22)
• Rapid responses: 50% of responding pts had response at first assessment (8 wks)
• 7/16 responders who discontinued for reasons other than disease progression
responded for ≥16 wks; 6/7 remain in response
• Responses in PD-L1 negative
• Similar OS by PDL1 or molecular status (EGFR or KRAS)
Dose, mg/kg ORR, % (n/N)
Median DOR, Wks (Range)
SD Rate 24 Wks, % (n/N)
Median PFS, Mos (95% CI)
Median OS, Mos (95% CI)
All doses 17.1%
(22/129)
74.0 (6.1+, 133.9+)
10.1 (13/129)
2.3 (1.9-3.7)
9.6 (7.8-12.4)
1 mg/Kg 3.0 % (1/33)
63.9 (63.9, 63.9)
15.2 (5/33)
1.9 (1.8-3.6)
9.2 (5.6-11.1)
3 mg/Kg 24.3 % (9/37)
74.0 (16.1+, 133.9+)
8.1 (3/37)
1.9 (1.7-7.3)
14.9 (9.5-NE)
10 mg/Kg 20.3 % (12/59)
83.1 (6.1+, 117.1+)
8.5 (5/59)
3.6 (1.9-3.8)
9.2 (5.2-12.4)
Brahmer JR, et al. WCLC 2013/ JCO 2013, abs 8030.
Heavily preteated (55% had received three or more prior lines of therapy)

Nivolumab: Duration of Response and OS
0 6 12 18 24 30 36 42 48 54
0
0.2
0.4
0.6
0.8
1.0
Mos Since Initiation of Treatment
129 82 48 31 20 4 3 2 1 0 Pts at Risk, n
All Treated Subjects With NSCLC
Died/Treated Median OS (95% CI)
94/129 9.9 (7.8-12.4)
Pro
po
rtio
n S
urv
iva
l
1-yr OS: 42% (48 pts at risk)
2-yr OS: 24% (20 pts at risk)
Brahmer JR, et al. WCLC 2013. Abstract MO18.03/JCO 2013
0 16 32 48 64 80 96 112 128 144 160
Wk
No
ns
qu
am
ou
s
Sq
uam
ou
s
NSCLC Responders by Histology
Duration of response up to discontinuation of therapy Ongoing response Time to response Response duration following discontinuation of therapy
1-yr OS: 44% and 41% squamous and non-squamous histology

Select AEs (≥ 1%) Occurring in Pts With NSCLC
Treated With Nivolumab (N = 129)
• Drug-related pneumonitis (any grade) occurred in 8 NSCLC pts (6%) vs 12
pts (4%) in the overall study population
– 3 pts (2%) with NSCLC had grade 3/4 pneumonitis
*AE severity was graded based on the Common Terminology Criteria for Adverse Events, v3.0.
Treatment-Related Select AE, % (n) Any Grade* Grade 3/4*
Any treatment-related select AE 41 (53) 5 (6)
Skin 16 (20) 0
Gastrointestinal 12 (15) 1 (1)
Pulmonary 7 (9) 2 (3)
Endocrinopathies 6 (8) 0
Hepatic 5 (6) 1 (1)
Infusion reaction 4 (5) 1 (1)
Renal 3 (4) 0
Brahmer JR, et al. ASCO 2013. Abstract 8030. Brahmer JR, et al. WCLC 2013. Abstract MO18.03.

1st-line nivolumab monotherapy (3mg/kg q 2 wks): Safety, efficacy, and correlation with PD-L1 status (n=20)
• Key results
– Overall ORR 30% (2 CR ,1 SCC, 1 non-SCC)
• Response at first assessment (11 weeks) in 83% (5/6 pts)
• PD-L1 expression status correlate with response (50% in PD-L1+; 0 PD-L1-) – PFS rate at 24 weeks was 60%, 1-year OS 75% – Grade 3–4 treatment-related AEs 20%
ASCO 2014 Gettinger 14, poster, abstr 8024
Responders by histology Responders by PDL-1
ORR 30% 22% SCC, 36% Non-SCC

Unprecedented RR seen in patients with heavily pretreated
NSCLC
Ongoing Nivolumab Clinical Trials in Patients With NSCLC
Line of therapy Phase PD-L1 Selection Comparator
Single agent Nivolumab
1st line[1] III Yes Chemotherapy maintenance
2nd line, squamous[2] III No Docetaxel
2nd line, adeno[3] III Yes Docetaxel
≥ 2nd line, squamous[4] II No NA
Combination Nivolumab
≥ 2nd line[5] I No + LAG3
≥ 2nd line[6] I No + lirilumab (KIR)
1st line[7] I No Single agent; + chemotherapy;
+ bevacizumab; + erlotinib; + ipilimumab
1. ClinicalTrials.gov. NCT02041533. 2. ClinicalTrials.gov. NCT01642004. 3. ClinicalTrials.gov. NCT01673867.
4. ClinicalTrials.gov. NCT01721759. 5. ClinicalTrials.gov. NCT01968109. 6. ClinicalTrials.gov. NCT01714739.
7. ClinicalTrials.gov. NCT01454102.

KEYNOTE-001: MK-3475 for Patients With NSCLC
• Treatment: administered IV 2 mg/kg q3w, 10 mg/kg q3w, or 10 mg/kg q2w
• Tumor assessment:
– Imaging q9w
– Primary: RECIST v1.1 (independent central review)
– Secondary: immune-related response criteria (investigator assessed)
• Tumor biopsy
– A new tumor biopsy within 60 days prior to the first dose of MK-3475 was required
Screening
-28 Days
MK-3475
C1D1 CR or PR,
SD
PD, unacceptable
toxicity, or
investigator decision
Continue dosing &
assessments q9w*
Off study Mandatory Biopsy
*Until progression, unacceptable toxicity, or investigator decision.
Garon EB, et al. WCLC 2013. Abstract MO18.02. Reprinted with permission.

4/49
PD-L1 Identifies Pts With NSCLC Most
Likely to Benefit From MK-3475
Strong PD-L1 positive staining was considered ≥ 50% of tumor cells, and weak was
defined as staining between 1% to 49% of positively staining tumor cells. Negative had
no tumor staining for PD-L1.
Re
sp
on
se
Ra
te (
%)
3/42 7/46 15/41 25/129
Gandhi L, et al. AACR 2014. Abstract CT105.
RR-RECIST 1.1
50
40
30
20
10
0
19
37
15
7
Total
1%-49% PD-L1 staining
≥ 50% PD-L1 staining
PD-L1 negative
Re
sp
on
se
Ra
te (
%)
4/53 20/44 28/146
RR-irRC
50
40
30
20
10
0
19
46
8 8
n/N: n/N:

Examples of PD-L1 NSCLC Sample
Immunohistochemical Staining*
PD-L1 Negative PD-L1 Positive
*Clinical trial assay.
Staining
Intensity 0+ 1+ 2+ 3+
PD-L1
Positivity, % 0 2 100 100
Gandhi L, et al. AACR 2014. Abstract CT105

KEYNOTE-001: MK-3475 AEs in Patients
With NSCLC
• 20 patients (53%) experienced ≥1 drug-related AE of any grade
• Drug-related AEs of interest: grade 2 hyperthyroidism (n = 1), grade 2 hypothyroidism (n
= 1), grade 2 pneumonitis (n = 1), and grade 3 pulmonary edema (n = 1)
• No patient experienced treatment-related death
Adverse Event All Grades, n (%) Grades 3-5, n (%)
Rash 8 (21) 0 (0)
Pruritis 7 (18) 0 (0)
Fatigue 6 (16) 0 (0)
Diarrhea 5 (13) 0 (0)
Arthralgia 4 (11) 0 (0)
Back pain 2 (5) 0 (0)
Cough 2 (5) 0 (0)
Decreased appetite 2 (5) 0 (0)
Garon EB, et al. WCLC 2013. Abstract MO18.02.

Ongoing MK-3475 Clinical Trials in
Patients With NSCLC
Line of Therapy Phase PD-L1
Selection
Comparator
Single-agent MK-3475
1st line; ≥ 2nd line[1,2] I/II Both NA
2nd line[3] III Yes Docetaxel
1st line[4] III Yes Chemotherapy
Combination MK-3475
NA[5] I/II No Single agent; + chemotherapy;
+ pemetrexed; + gefitinib; + erlotinib;
+ ipilimumab
1. ClinicalTrials.gov. NCT02085070. 2. ClinicalTrials.gov. NCT02129556. 3. ClinicalTrials.gov. NCT01905657.
4. ClinicalTrials.gov. NCT02142738. 5. ClinicalTrials.gov. NCT02039674.

BMS 936559: PD-L1 antibody
• 207 patients with advanced solid organ malignancies
– was given every 2 weeks
– 75 p with NSCLC
• 49 evaluable for response
• 5 objective responses (4 non-squamous and 1 squamous)
Brahmer JR NEJM 2012; 366: 2455-65

Phase I Study of MPDL3280A in NSCLC • MPDL3280A: anti–PD-L1 antibody engineered for enhanced safety and efficacy
• Specifically engineered to block the PD1/PD-L1 interaction
• Patients with metastatic solid tumors
– EGFR and KRAS status assessed at baseline
• Study design: MPDL3280A IV every 3 wks x 16 cycles (≈ 1 yr)
• Primary endpoint: safety
• Secondary endpoint: ORR by RECIST v1.1
Characteristics n = 85*
Median age, yrs (range) 60 (24-84)
Sex, male/female, n (%) 48 (56)/37 (44)
ECOG PS, 0 / 1, n (%) 27 (32)/58 (68)
Histology, n (%)
Squamous 20 (24)
Nonsquamouss 65 (76)
*Safety evaluable patients (n = 85) with NSCLC. Data cutoff April 30, 2013. †Systemic regimens administered in the metastatic, adjuvant or neoadjuvant setting. 3% of patients had no previous systemic regimens.
Characteristics, n (%) n = 85*
Previous systemic regimens†
1 or 2 36 (42)
≥ 3 47 (55)
Smoking status
Current/previous 68 (80)
Never 17 (20)
Horn L, et al. WCLC 2013. Abstract MO18.

PD-L1
Status*
(N = 53)
ORR,†
%
(n/N)
Pts With PD,
% (n/N)
IHC 3
(n = 6)
83
(5/6)
17
(1/6)
IHC 2 and 3
(n = 13)
46
(6/13)
23
(3/13)
IHC 1/2/3
(n = 26)
31
(8/26)
38
(10/26)
All patients
(IHC 0/1/2/3
and 7
patients with
diagnostic
unknown;
N = 53)
23
(12/53)
40
(21/53)
Duration of Treatment and Response
Wk
Histology IHC
NS IHC 0
S IHC 3
NS IHC 0
NS IHC 1
NS IHC 0
S IHC 2
NS IHC 3
S IHC 3
NS IHC 3
NS IHC 0
NS IHC 3
NS IHC 1
*PD-LI status determined using proprietary Genentech Roche IHC. †ORR includes investigator-assessed unconfirmed and confirmed (u/c) PR per RECIST 1.1.
Patients first dosed at 1-20 mg/kg by October 1, 2012. Data cutoff April 30, 2013.
MPDL3280A in NSCLC: Best Response by PD-L1
Status and DOT/DOR
Horn L, et al. WCLC 2013. Abstract MO18/Spigel DR. JCO abstract 8080.
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
On study, on treatment
On study, post treatment
Treatment discontinued
Ongoing response
First response
First PD

*ORR includes investigator-assessed u/c PR by RECIST 1.1. Patients first dosed at 1-20 mg/kg by October 1, 2012. Data cutoff April 30, 2013.
Former/
Current Smokers
Never
Smokers
Response by Smoking Status (ORR*) Smoking Status (NSCLC; n = 53)
Pts
Wit
h P
R (
%)
EGFR
Mutant
EGFR Status (NSCLC; n = 53)
Unknown
Response by EGFR Status (ORR*)
Pts
Wit
h P
R (
%)
KRAS Status (NSCLC; n = 53) Response by KRAS Status (ORR*)
Pts
Wit
h P
R (
%)
KRAS
Mutant
Unknown
EGFR WT EGFR Mutant
KRAS WT KRAS Mutant
11/43 1/10
9/40 1/6
8/27 1/10
MPDL3280A Phase Ia: Response by Smoking
and Mutational Status
Horn L, et al. WCLC 2013. Abstract MO18. ASCO/JCO
50
40
30
20
10
0
50
40
30
20
10
0
50
40
30
20
10
0
Former/Current Smokers Never Smokers
26%
10%
23% 17%
30%
10% 51%
30%
19%
76% 13%
11%
81%
19%
KRAS WT
EGFR WT
Current/Former: 20/75: 27% ORR
Never: 0/13
ESMO 2014

[TITLE]
Calles ESMO 2014

MPDL3280A: Treatment-Related Adverse
Events in Patients With NSCLC
• Majority of AEs were grade 1/2 and did
not require intervention
• No MTD or dose-limiting toxicities
• No grade 3-5 pneumonitis observed
• Treatment-related death (cardio-
respiratory arrest) in 1 patient with
sinus thrombosis and large tumor
mass invading the heart at baseline
• Immune-related grade 3.4 AEs: 1
patient with large-cell neuroendocrine
NSCLC (diabetes mellitus, 1%)
*AEs occurring in ≥ 5% of patients. †Grade 3/4 treatment-related AEs listed include treatment-
related AEs for which the any grade occurrence was ≥ 5%
of patients.
Data cutoff April 30, 2013.
Adverse Event
(n = 85)
Treatment Related, % (n)
Any Grade* Grade 3/4†
Any AE 66 (56) 11 (9)
Fatigue 20 (17) 2 (2)
Nausea 14 (12) 1 (1)
Decreased appetite 12 (10) 0
Dyspnea 9 (8) 1 (1)
Diarrhea 8 (7) 0
Asthenia 7 (6) 0
Headache 7 (6) 0
Rash 7 (6) 0
Pyrexia 6 (5) 0
Vomiting 6 (5) 1 (1)
Upper respiratory tract
infection
5 (4) 0
Horn L, et al. WCLC 2013. Abstract MO18. Reprinted with permission.


Vaccine therapy
Vaccine Antigen Specific
Phase trial stage/pop
Nº Trial design Results
MAGE 3 present in numerous tumors
JCO 2013
Proof-of-concept MAGE A3 positive Stage IB Phase II vaccine vs placebo
122 Recurrence 35% MAGE A3 arm vs 43% placebo Disease Free Interval: HR: 0.75; p:0.25 Disease Free Survival: HR: 0.76; p:0.24 OS: HR: 0.81; p:0.45
MAGE-A3 ESMO 2014
MAGRIT Stage IB, II and IIIA + MAGE-3 gene placebo vs vaccine
2312 Stopped Did not meet primary end points, including DFS

Vaccine Phase trial stage/pop
Nº Results
MUC-1 Membrane-associated Glycoprotein MUC-1 is increased in cancer cell 60% NSCLC Role not clear Peptide based vaccine- Liposomal BLP-25 (L-BLP25) Butts C. JCO 2005
Phase II IIIB and IV stable after ChT or RT
171 Eight weekly sc imm L-BLP25 vs BSC Median Survival: 17.4 m vs 13 m (HR: 0.73; p: 0.11) 3-year survival rate was: 31% L-BLP25 vs 17% (p:0.035) A post hoc analysis: benefit in stage IIIB (3-y: 49% vs 27%; p: 0.07)
MUC-1 L-BLP-25
START Stage III unresectable vaccine vs ctx vs placebo
1513 After ChemoRT; placebo vs Vaccine Did not meet primary end point OS: 0.88; median OS: 25.6 vs 22.3; p:0.123

Vaccine Phase trial stage/pop
Nº Results
TG 4010 glycoprotein based pox virus Encoding for MUC-1 and IL-2 Ramlau R. JTO 2008
Phase II Stage IIIB/IV 1st line with CDDP-VNR
67 Concurrent arm: 35% and OS: 12.7
TG4010 MUC positive Lancet Oncol 2011
Phase IIB IIIB/IV cis-gem alone vs Cht + vaccine
148 PFS: TG40101: 43.2% ChT: 35.1% (p:0.307) OS: TG4010: 10.7 m ChT: 10.3 m
TG 4010 glycoprotein MUC-1
Stage IV ongoing
placebo vs vaccine Primary end point: OS

Vaccine Phase trial stage/pop
Nº Results
CIMAvax EGF Recombinat Human Epidermal Growth Factor Neninger E. JCO 2008
Phase II Stage IIIB/IV 1st line following BSC vs vaccine
80 Median OS: 11.7m with good EGFR antibody response
Bec2 combined with BCG anti-idiotypic antibody GD3 JCO 2005
Phase III SCLC after induction
551 No improvement in OS, PFS or QoL OS median 16.4 vs 14.3 m
Belagenpumatucel antisense gene –TGF-B2 AACR 2013
Phase II Stage IV
75 OS: 44.4 m


Immunocompetent Mice Reject Tumors Originating in Immunodeficient Mice
Shankaran V, et al. Nature. 2001;410:1107-1111.
In other words, competent immune
systems force the tumors to figure
out how to survive in hostile
environments

Conclusions
Next frontier of treatment of lung cancer

The cytotoxic T-lymphocyte antigen-4 (CTLA-4) inhibitory checkpoint pathway is important in
regulating early T-cell activation.
Brahmer J R JCO 2013;31:1021-1028
©2013 by American Society of Clinical Oncology

Safety and response with nivolumab/erlotinib in p with advanced mutant EGFR (NCT01454102)
Rizvi 14, poster, abstr 8022
PD
Key patient inclusion criteria
•Stage IIIB/IV NSCLC
•Non-squamous
•EGFR+
•CT naïve
(n=21)
nivolumab 3 mg/kg q2w
+ erlotinib 150 mg/day
• Key results:
– 21 p (20 prior treatment with erlotinib)
– Grade 3 AEs occurred in 24% of p (no grade 4 reported)
– ORR 19% / 45% SD
– PFS 29.4 weeks (4.6-81.7), OS NR (10.7-86.9)