initial experience with a new compression device for hemostasis after femoral arterial puncture
TRANSCRIPT

Catheterization and Cardiovascular Diagnosis 26:241-244 (1992)
Preliminary Reporf
Initial Experience With a Compression Device for
New
Hemostasis After Femoral Arterial Puncture Robert Roth, RN, Karen Modrosic, Matt Brown, and Morton J. Kern, MD
We evaluated a new hemostasis device to maintain focused pressure over the femoral artery puncture site for 2 6 hours in 330 cases after diagnostic catheterization or coronary angim plasty. No patient developed later hematoma or vascular com- plications. The initial favorable experience suggests that this hemostasis device has advantageous features of stability and site visualization and is a suitable adjunct to current methods of maintaining puncture site pressure after brief manual compres- sion following arterial catheterization.
Key words: artery, catheterization, pressure
c 1992 Wlley-LIma. Inc
INTRODUCTION
Femoral arterial puncture and cannulation is the most widely used vascular access technique in diagnostic and interventional radiology and cardiology procedures. Af- ter the procedure and removal of the arterial catheter, hemostasis is obtained by applying direct pressure over the puncture site. The most common technique to obtain initial hemostasis is manual compression for 15-20 min [ 1-51. This methodology was empirically established from the first procedures over 30 years ago. Compressive dressings with rolled gauze and elastic bandages for pres- sure maintenance after the initial manual compression are generally ineffective [2,3]. There are several me- chanical clamp devices which are alternatives to manual compression and provide a means of “hands off,” initial and sustained pressure to the puncture site. The clamp devices are generally used for only the brief period of time (15-30 min) required to obtain hemostasis and not generally used for longer maintenance periods of arterial compression. In some patients with hypertension or who received anticoagulation who are at risk for bleeding, it is often desirable to maintain pressure over the site for several hours after initial hemostasis has been obtained. Long-term pressure maintenance has been attempted with elastic dressings and compressing gauze packs or 10 lb sandbags, methods which, in our experience, are only minimally effective and associated with difficulties in pressure device positioning, identifying continued bleed-
ing and patient discomfort. Because of the poor results with the elastic dressings and sandbag techniques, we evaluated a new hemostasis device with improved fea- tures facilitating an approach to maintaining pressure long-term in the postprocedural period.
Hemostasis System The stasis system is composed of 3 components-a
disposable sterile plastic Stasis Button (Arch Develop- ment Group); a reusable, non-sterile stainless steel stasis weight (3 lb, Arch Development Group); and 2 strips of elastic bandage (i.e., ElastoplastTM or 3M Micro- foamm, 4 inch wide) (Fig. 1).
After initial hemostasis has been obtained (either man- ually or mechnically), the stasis button is placed above (cranial to) the puncture site (Fig. 2) and is secured to the skin by means of adhesive foam pad on the base of the stasis button. One of two strips of elastic dressing is stretched diagonally from the iliac crest over the stasis button and under the thigh (Fig. 3). The weighted cyl- inder (stasis weight) is positioned on the peg of the stasis button under the fmt strip of elastic dressing. The second strip of elastic bandage is now placed at a 45” angle to the first strip to form a criss-cross over the weight. The weighted cylinder does not touch the patient and is set off by the mounting peg of the stasis button. The elevated position of the weight beneath the elastic dressing per- mits unobstructed observation of the puncture site.
Unlike sandbags and gauze wedges, downward pres- sure at the puncture site is adjusted by the tension applied with the second elastic bandage strip. The bandages and weight result in a focused application of pressure directly over the puncture site. Also, in contrast to sandbags, after the two elastic strips are in place, the position of the stasis button remains stable during patient movement, especially important during transfer from stretcher to bed.
From the Cardiology Division, St. Louis University Hospital, St. Louis.
Received December 16, 1 9 9 1 ; revision accepted February 22, 1992.
Address reprints requests to Rob Roth, RN, Cardiac Catheterization Laboratory, St. Louis University Hospital, 3635 Vista Avenue at Grand, St. Louis, MO 631 10-0250.
0 1992 Wiiey-Liss, Inc.

242 Roth et al.
Fig. 1. A: The "stasis" button (rlght) and "stasis" weight (left). B: The "stasis" weight posi- tioned on the button peg.
TABLE 1. Initial E&ence Wlth Hemostssls Button Svstem
Indication for application
Post-PTCA sheath removal Bleeding around sheath post-PTCA 5 min compression time + device Rebleed after initial manual hemostasis Post-PTCA sheath removalhalf strength heparin Postcath, post-thrombolytic agent
Hypertensives (systolic blood pressure > 150mm Hg) Prolonged manual compression >20 min
status post-valvuloplasty
No. of cases
260 19 10 9 8 5 5 4 3
%
78 5 .1 3 2.1 2.4 1.5 1.5 1.2 0.9
Hematoma post-manual compression 3 0.9 Prolonged manual compression >20 min + aortic
insufticienc y 2 0.6 Prolonged prothrombin time (<20% activity) 1 0.3 Coughing and hiccoughs after sheath removal 1 0.3
Total caSeS 330 100 Fig. 2. puncture skin entry site.
Positlonlng of the stasis button cranial fo the arterial
Evaluation After Hemostasis System Application The hemostasis device was used to maintain pressure
for several hours after the femoral arterial catheter or sheath was removed. As with all pressure devices for arterial compression, distal pulses were evaluated both prior to and after device placement.
In selected patients (described below), the stasis but- ton system was attached after a brief period of manual compression either in the catheterization laboratory or at bedside. After the hemostasis system was in place, the puncture site and distal pulses were frequently checked (e.g., q 1/2-1 hr). The device was left in place for 2-6 hrs. If puncture site bleeding or oozing continued, ad- justment of the dressing and longer application was per-
formed. If distal pulses were diminished, the device was removed. When longer pressure application was needed, more frequent observation of the puncture site and distal pulses was performed. Skin integrity at the puncture site was evaluated if the device was in place longer than 6 hours.
CLINICAL EXPERIENCE
From October 1990 to October 1991, the hemostasis system was used in 330 patients (Table I). Initially, pa- tients thought to be at high risk for puncture site bleeding (e.g., hypertension, aortic insufficiency, continued hep- arin infusion or those requiring prolonged manual com- pression) were selected. Patients in whom bleeding oc-
Hemostasis After Femoral Arterial Puncture 243
C D
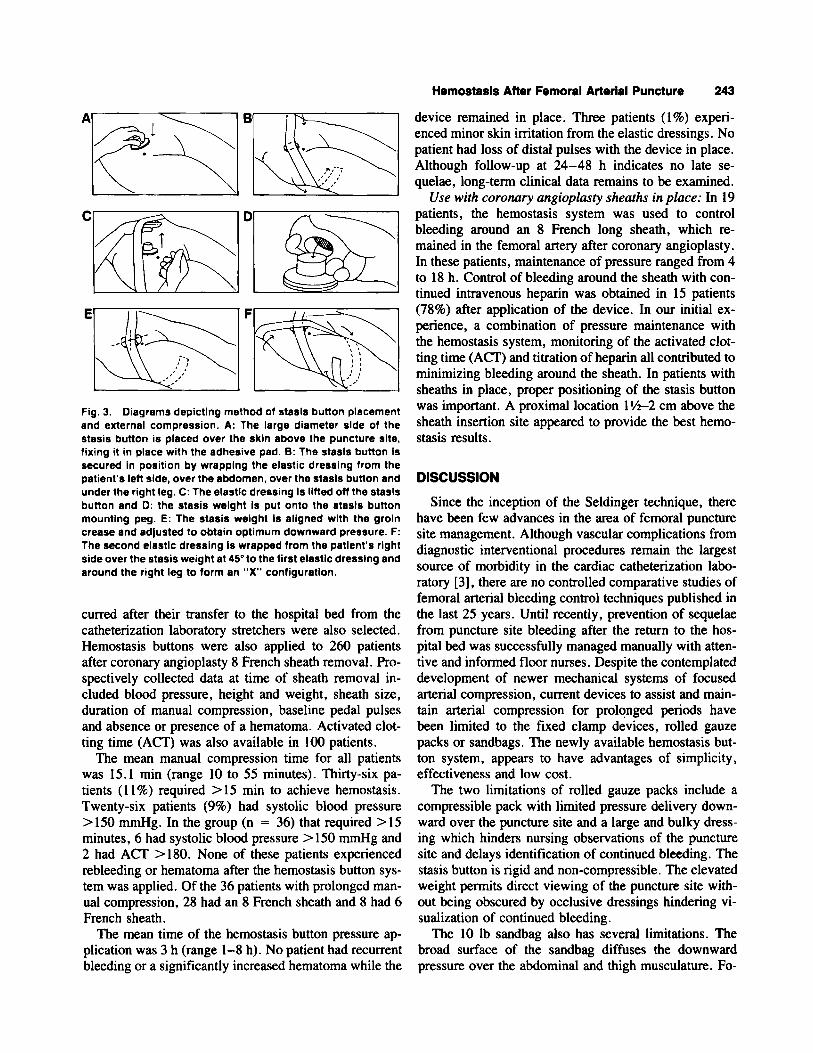
Fig. 3. Diagrams depicting method of stesls button placement and external compression. A: The large diameter slde of the stasis button is placed over the skin above the puncture site, fixing it in place with the adhesive pad. 8: The stasis button Is secured In position by wrapping the elastic dresslng from the patient's left slde, over the abdomen, over the stasls button and under the right leg. C: The elastic dressing Is lifted off the stasls button and D: the stasis weight Is put onto the stasls button mounting peg. E: The stasis weight is aligned with the groln crease and adjusted to obtain optimum downward pressure. F: The second elastic dressing is wrapped from the patient's right side over the stasis weight at 45" to the first elastic dresslng and around the right leg to form an "X" configuretion.
curred after their transfer to the hospital bed from the catheterization laboratory stretchers were also selected. Hemostasis buttons were also applied to 260 patients after coronary angioplasty 8 French sheath removal. Pro- spectively collected data at time of sheath removal in- cluded blood pressure, height and weight, sheath size, duration of manual compression, baseline pedal pulses and absence or presence of a hematoma. Activated clot- ting time (ACT) was also available in 100 patients.
The mean manual compression time for all patients was 15.1 min (range 10 to 55 minutes). Thirty-six pa- tients (1 l%) required > 15 min to achieve hemostasis. Twenty-six patients (9%) had systolic blood pressure >150 mmHg. In the group (n = 36) that required >15 minutes, 6 had systolic blood pressure > 150 mmHg and 2 had ACT > 180. None of these patients experienced rebleeding or hematoma after the hemostasis button sys- tem was applied. Of the 36 patients with prolonged man- ual compression, 28 had an 8 French sheath and 8 had 6 French sheath.
The mean time of the hemostasis button pressure ap- plication was 3 h (range 1-8 h). No patient had recurrent bleeding or a significantly increased hematoma while the
device remained in place. Three patients (1%) experi- enced minor skin imtation from the elastic dressings. No patient had loss of distal pulses with the device in place. Although follow-up at 24-48 h indicates no late se- quelae, long-term clinical data remains to be examined.
Use with coronary angioplasry sheaths in place: In 19 patients, the hemostasis system was used to control bleeding around an 8 French long sheath, which re- mained in the femoral artery after coronary angioplasty. In these patients, maintenance of pressure ranged from 4 to 18 h. Control of bleeding around the sheath with con- tinued intravenous heparin was obtained in 15 patients (78%) after application of the device. In our initial ex- perience, a combination of pressure maintenance with the hemostasis system, monitoring of the activated clot- ting time (ACT) and titration of heparin all contributed to minimizing bleeding around the sheath. In patients with sheaths in place, proper positioning of the stasis button was important. A proximal location 1 Yi-2 cm above the sheath insertion site appeared to provide the best hemo- stasis results.
DISCUSSION
Since the inception of the Seldinger technique, there have been few advances in the area of femoral puncture site management. Although vascular complications from diagnostic interventional procedures remain the largest source of morbidity in the cardiac catheterization labo- ratory [3], there are no controlled comparative studies of femoral arterial bleeding control techniques published in the last 25 years. Until recently, prevention of sequelae from puncture site bleeding after the return to the hos- pital bed was successfully managed manually with atten- tive and informed floor nurses. Despite the contemplated development of newer mechanical systems of focused arterial compression, current devices to assist and main- tain arterial compression for prolonged periods have been limited to the fixed clamp devices, rolled gauze packs or sandbags. The newly available hemostasis but- ton system, appears to have advantages of simplicity, effectiveness and low cost.
The two limitations of rolled gauze packs include a compressible pack with limited pressure delivery down- ward over the puncture site and a large and bulky dress- ing which hinders nursing observations of the puncture site and delays identification of continued bleeding. The stasis button is rigid and non-compressible. The elevated weight permits direct viewing of the puncture site with- out being obscured by occlusive dressings hindering vi- sualization of continued bleeding.
The 10 lb sandbag also has several limitations. The broad surface of the sandbag diffuses the downward pressure over the abdominal and thigh musculature. Fo-

244 Roth et el.
cused pressure to the puncture site does not occur. The sandbag often slips off the leg when the patient adjusts position to minimize back and leg discomfort associated with the sandbag. Additionally, the sandbag may overlie a bulky or large dressing, further contributing to delayed identification of hematoma formation. The stasis button is secured in position by the adhesive pad and the elastic dressings. Changes in patient position have little effect on the downward pressure maintenance with the stasis button. Back and leg discomfort with the stasis button was not reported in the initial evaluation.
Since both the button and elastic bandages have adhe- sive backings, caution should be exercised when remov- ing the system in patients with delicate skin or adhesive sensitivities.
The initial findings in our laboratory suggest that pa- tients at high risk for vascular bleeding after catheter (or sheath) removal can benefit from sustained compression with the stasis button. Although our preliminary data suggested a potential benefit relative to historical results, a prospective comparison of bleeding outcomes with other modalities and the stasis button system in matched patients will be needed to establish definitive clinical efficacy.
SUMMARY
A new arterial puncture hemostasis system, the stasis button, is available which maintains puncture site pres-
sure in the post-catheterization period. This device is intended to be used only after initial manual or mechan- ical hemostasis has been obtained. The design features of this system suggest that it may offer an improved ap- proach compared to sandbags or elastic dressings and gauze packs in the management of patients susceptible to post-procedure arterial bleeding.
ACKNOWLEDGMENTS
The authors wish to thank the J.G. Mudd Cardiac Catheterization Laboratory Team and Donna Sander for manuscript preparation.
REFERENCES
I . Halpern M: Percutaneous transfemoral arteriography: an analysis of the complications in 1 ,OOO consecutive cases. Am J Roentgenol
2. Eisenberg RL, Mani RL: Pressure dressings and postangiographic care of the femoral puncture site. Radiology 122:677-678, 1977.
3 . Christenson R, Staab EV, Burko H, Foster J: Pressure dressings and postarteriographic care of the femoral puncture site. Radiology
4. Lang EK. Prevention and treatment of complications following arteriography. Radiology 88:950-956. 1967.
5. Deligonul U, Roth R. Arterial and venous access. In Kern MJ (4): “The Cardiac Catheterization Handbook.” St. Louis: Mosby Year Book, Inc, 1991, pp 36-97.
92~918-934, 1964.
119~97-99, 1976.