initial assessment and care in spinal trauma patient dr. seyed mani mahdavi orthopedic spine surgeon
TRANSCRIPT
INITIAL ASSESSMENT AND CAREIN SPINAL TRAUMA PATIENT
DR. Seyed Mani MahdaviOrthopedic Spine Surgeon
• Advanced Trauma Life Support
• As a general rule, all trauma patients need to be fully investigated for spinal injury
• Even mild complaints of pain or posterior midline tenderness
Field Care
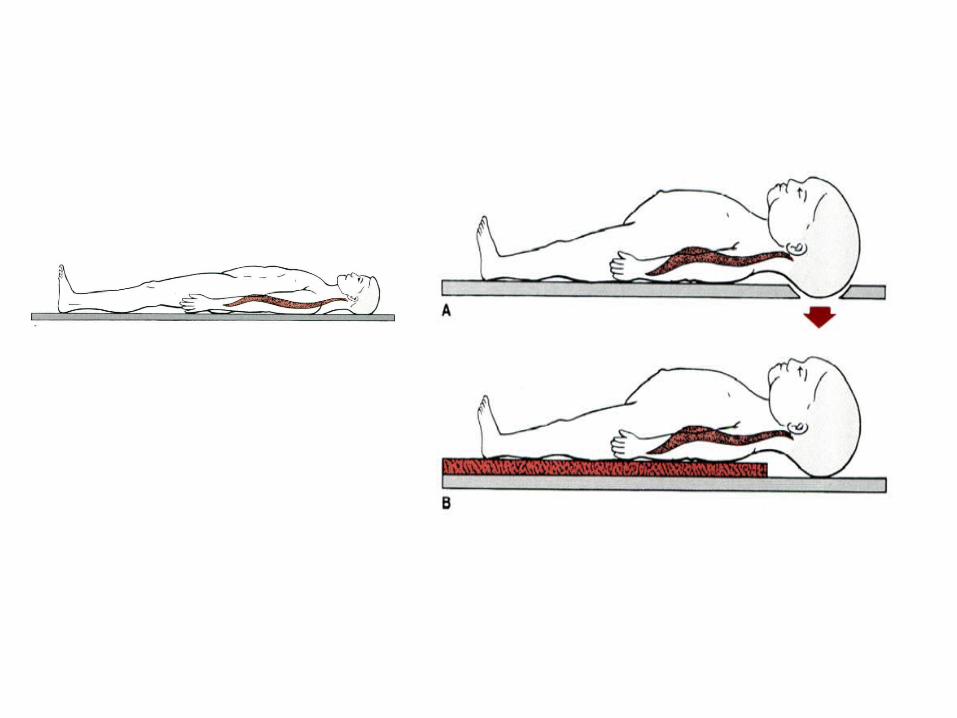
• The head and neck need to be aligned with the long axis of the trunk and immobilized in
this position

Kendrick Extrication Devicefor Spinal Immobilization
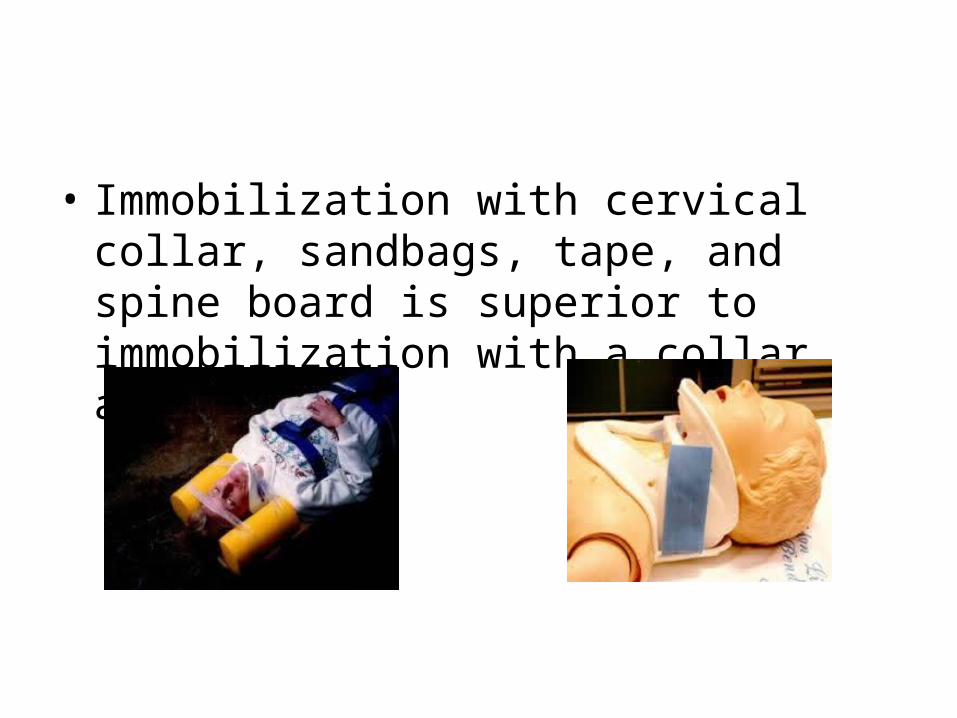
• Immobilization with cervical collar, sandbags, tape, and spine board is superior to immobilization with a collar alone
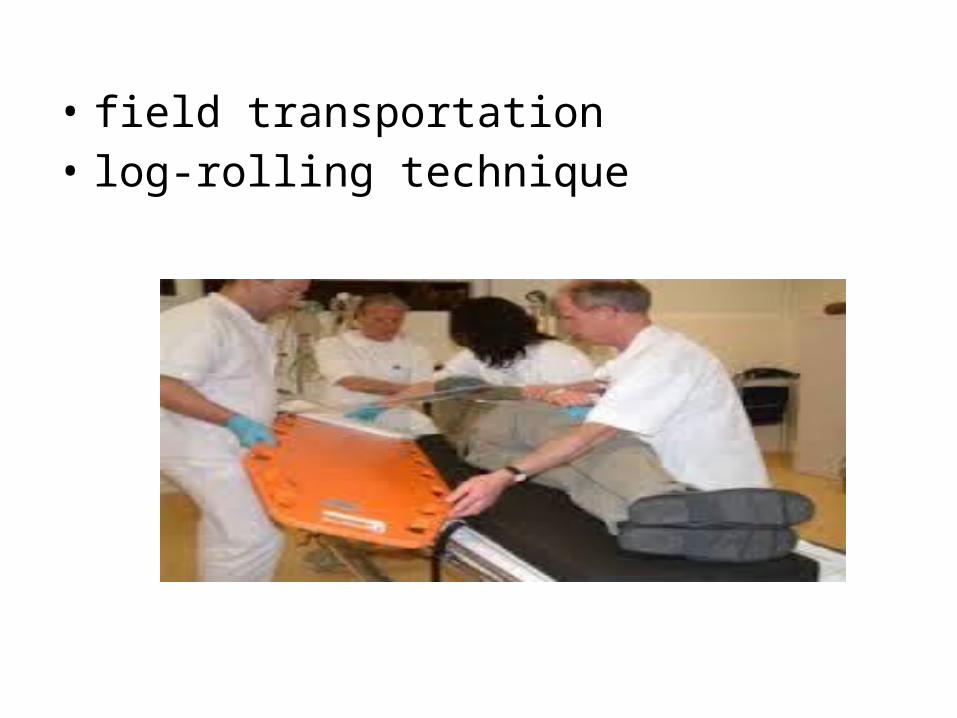
• field transportation• log-rolling technique
• Neutral flexion-extension head and neck alignment is optimal during pre hospital transport of cervical spine injury patient
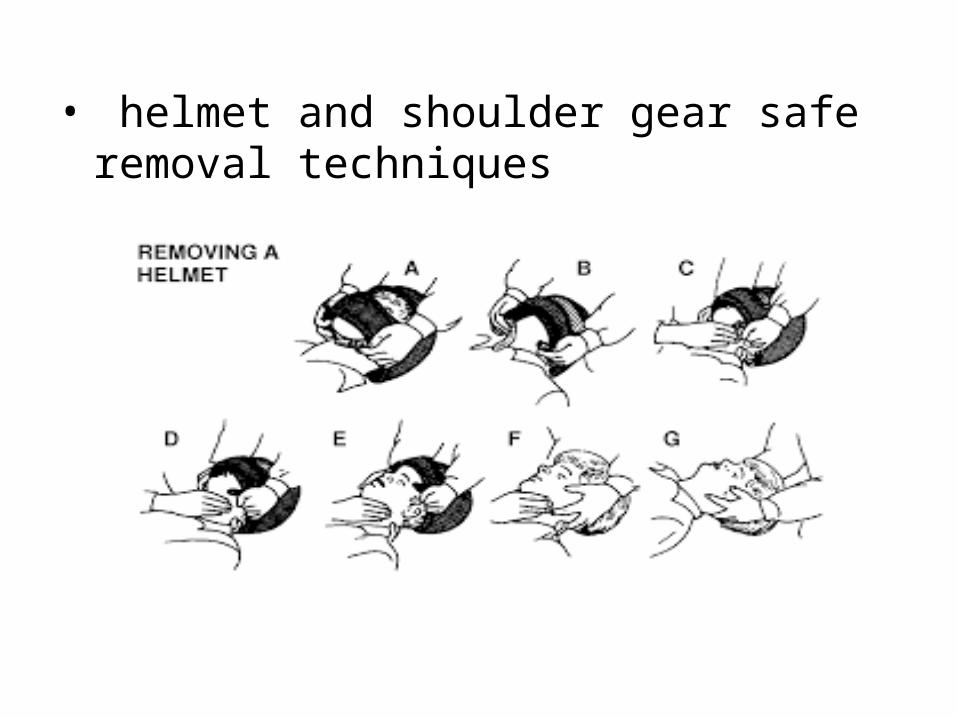
• helmet and shoulder gear safe removal techniques
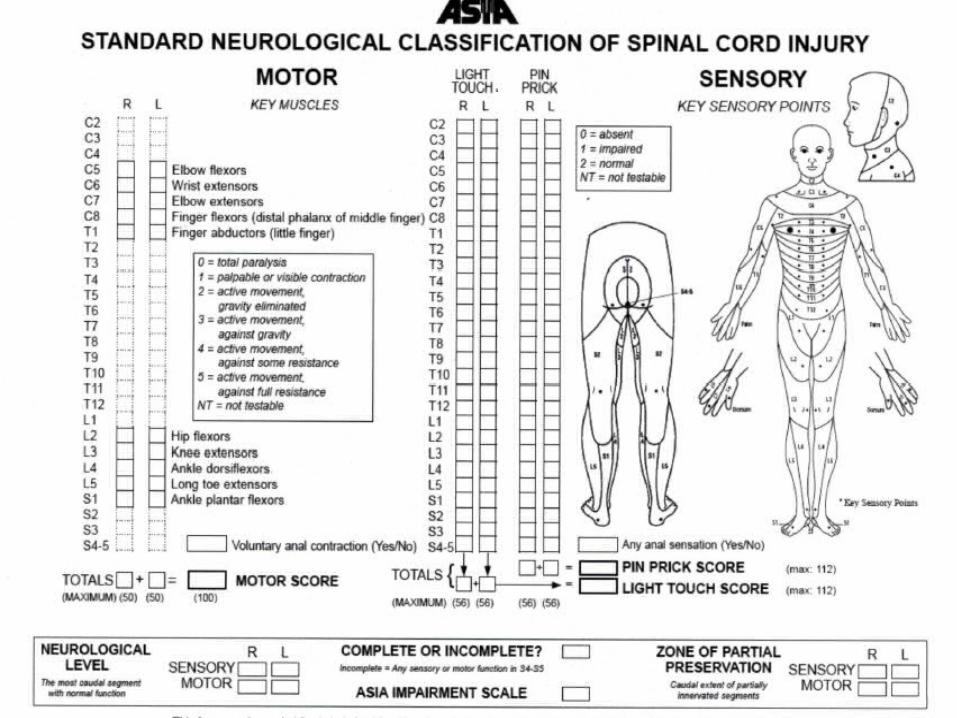
• Preliminary assessment of neurologic status in the field extremely valuable
• asking about neck pain, back pain, numbness, and weakness
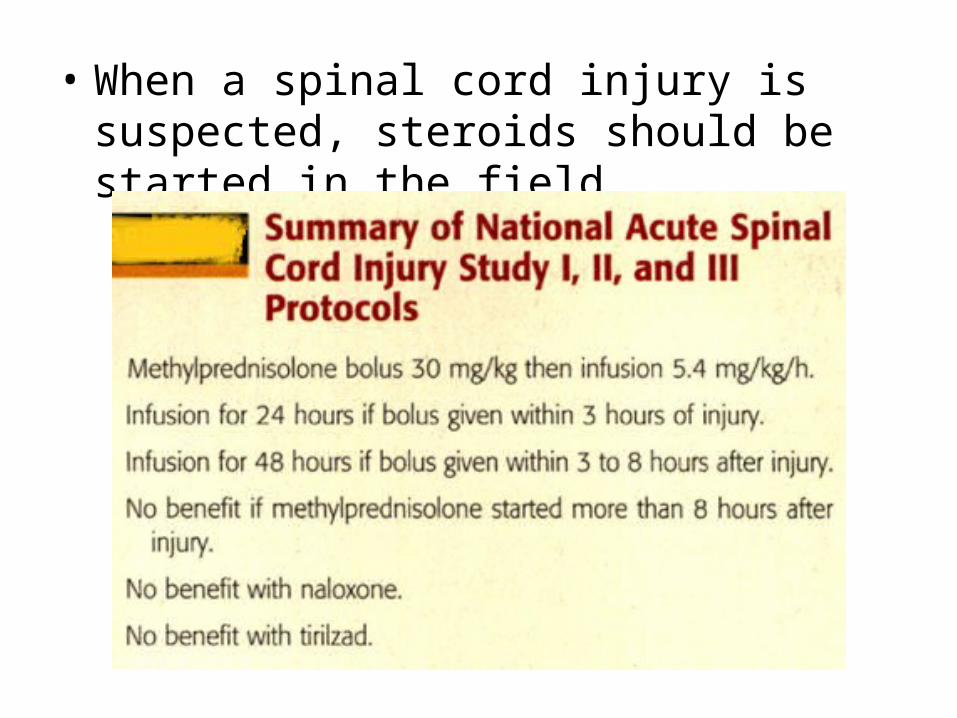
• When a spinal cord injury is suspected, steroids should be started in the field
Emergency Room Care
• Assessment of gross neurologic function• Diagnosis of severely unstable injuries• Assessment of hemodynamic parameters
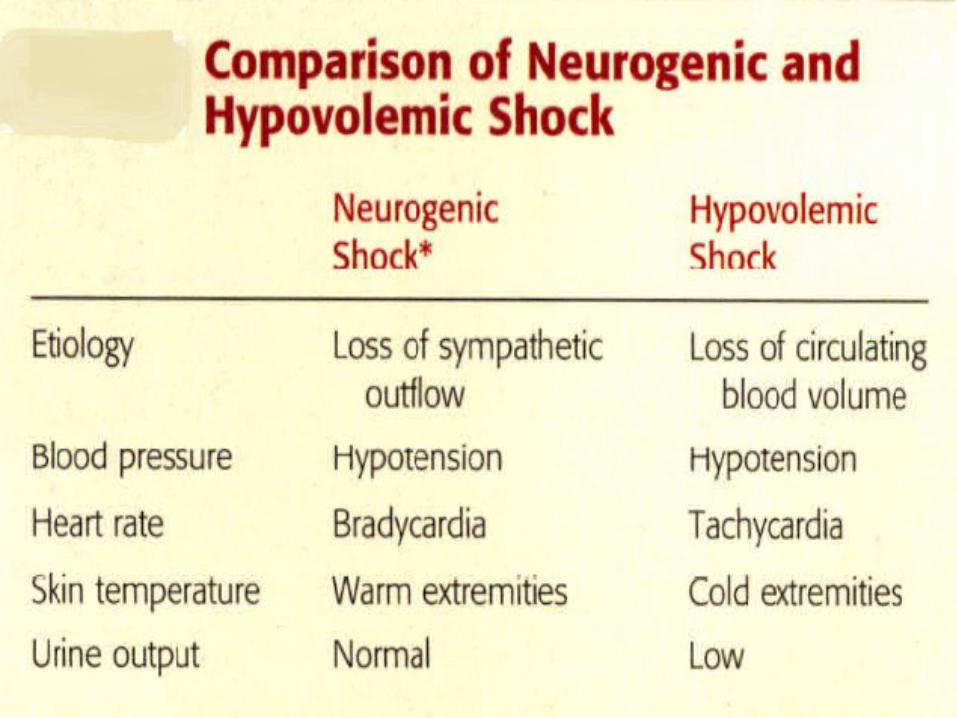
(neurogenic shock)• spinal shock should be distinguished from
neurogenic shock(Spinal shock refers to depressed spinal reflexes caudal to spinal cord injury)
IMAGING AND DIAGNOSTIC STUDIES
Clearing the spine frequently requires considerable time, with one study reporting a median time of 15 hours
• Most spine injuries occur at the junctions: craniocervical ,cervicothoracic, and thoracolumbar. They are often the most difficult to see on standard radiographs.
• Emergent life-saving interventions, such as intubation, anesthesia, and abdominal or chest surgery, can be performed relatively safely using appropriate precautions in a patient with incompletely evaluated cervical spine.
• AP chest radiograph,AP pelvis radiograph, and a lateral cervical spine radiograph
The End