inguinal hernia repair 2019 - uphs.upenn.edu · 4. inguinal hernia repair with mesh lichtenstein...
TRANSCRIPT
Inguinal Hernia Repair 2019
Alan L. Schuricht MD, FACSClinical Associate Professor of SurgeryUniversity of PennsylvaniaPhiladelphia, Pennsylvania USA
2
Question # 1Should inguinal hernia repair be performed with mesh?

3
Question # 1Should inguinal hernia repair be performed with mesh?
YES
NO

4
Inguinal Hernia Repair with Mesh Lichtenstein repair
• A flat mesh is placed on top of the defect• Tension-free repair• Complications
– Chronic pain (10-50%)– Foreign body sensation– Stiffness– Ischemic orchitis/testicular atrophy– Ejaculatory problems (12%)
• Low recurrence rate (<2%)
Lichtenstein, IL; Shulman, AG (1986). "Ambulatory outpatient hernia surgery. Including a new concept, introducing tension-free repair". International surgery 71 (1): 1–4.
Wantz, GE (1993). "Testicular atrophy and chronic residual neuralgia as risks of inguinal hernioplasty". The Surgical clinics of North America 73 (3): 571–81.
Ridgway, P.F.; Shah, J.; Darzi, A.W. (2002). "Male genital tract injuries after contemporary inguinal
hernia repair". BJU International 90 (3): 272–6. Aasvang, Eske Kvanner; Møhl, Bo; Bay-Nielsen, Morten; Kehlet, Henrik (2006). "Pain related sexual dysfunction after inguinal herniorrhaphy". Pain 122 (3): 258–63.
5
Question #1bWhat about plugs?
6
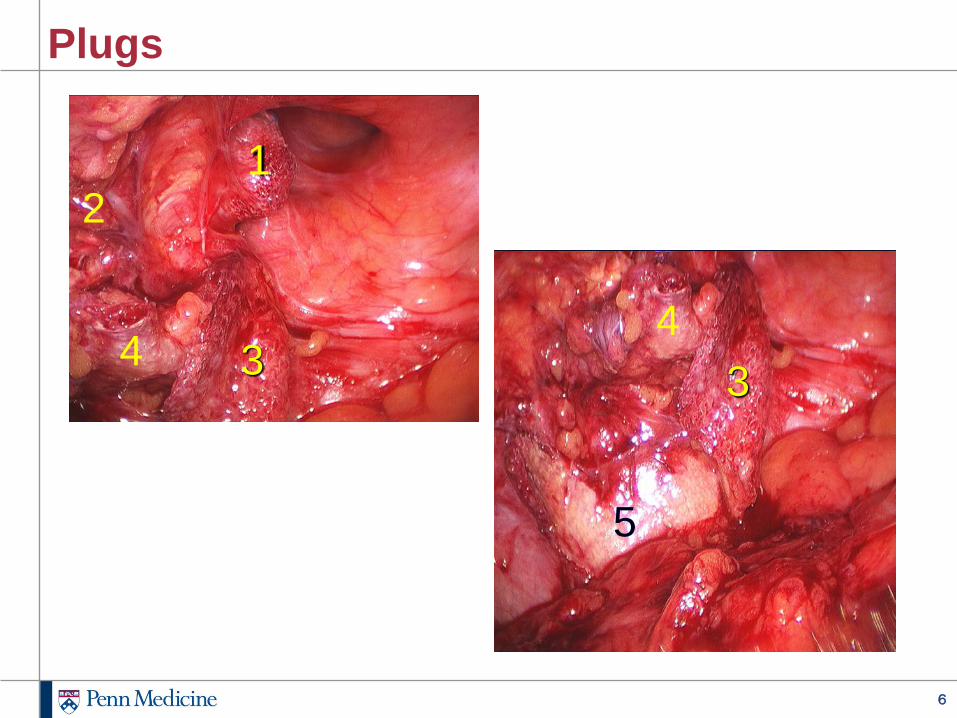
Plugs
44
12
3 3
5
7
Question #2 How common is post-herniorrhaphy pain after
inguinal hernia repair?
8
Question #2 How common is post-herniorrhaphy pain after
inguinal hernia repair?
WHAT’S THAT?
PRETTY RARE
FAIRLY COMMON
WAY TOO COMMON
9
Post-herniorrhaphy Inguinodynia True incidence is difficult to determine 419 Lichtenstein patients
• At 1 year: 19% pain (6% moderate or severe)– Predictors– Recurrent hernia– High pain score at 1 or 4 weeks
Scottish study (4062 patients)• 3 months: 43% mild pain and 3% severe or very severe pain• 30 months: 29% resolved, 39% improved, 26% continued with severe
or very severe pain 750 laparoscopic vs. open repairs
• Pain scores at 2 and 5 years• Questionnaire• 2 years: chronic pain 24.3% (lap) vs. 29.4% (open)• 5 years: 18.1% (lap) vs. 20.1% (open)
10
Post-herniorrhaphy Inguinodynia 1370 patients
• Randomized to TEP vs. open repair with mesh• Lower pain rates in TEP (10%) vs. open (20%)• Symptoms decreased over time• Questionnaire at 9.4 years: physical ability more affected in open
group Mesh-based vs. suture based repair
• Less inguinodynia in Shouldice vs. Lichtenstein in young men
Callesen, T.; Bech, K.; Kehlet, H. (1999). "Prospective study of chronic pain after groin hernia repair". British Journal of Surgery 86 (12): 1528–31.
Courtney, C. A.; Duffy, K.; Serpell, M. G.; O'Dwyer, P. J. (2002). "Outcome of patients with severe chronic pain following repair of groin hernia". British Journal of Surgery 89 (10): 1310–4. Grant, A. M.; Scott, N. W.; O'Dwyer, P. J.; MRC Laparoscopic Groin Hernia Trial Group (2004). "Five-year follow-up of a randomized trial to assess pain and numbness after laparoscopic or open repair of groin hernia". British Journal of Surgery 91 (12): 1570–4.
Eklund, A.; Montgomery, A.; Bergkvist, L.; Rudberg, C.; Swedish Multicentre Trial of Inguinal Hernia Repair by Laparoscopy (SMIL) study group (2010). "Chronic pain 5 years after randomized comparison of laparoscopic and Lichtenstein inguinal hernia repair". British Journal of Surgery97 (4): 600–8.

11
Question #2bShould an open inguinal hernia repair involve a neurectomy?
12
Question #2bShould an open inguinal hernia repair involve a neurectomy?
YES
NO
SELECTIVELY

13
Neurectomy Mui et al
• Incidence of chronic pain at 6 months was significantly lower in those patients who had prophylactic ilioinguinal neurectomy (one nerve only)
• 8% vs. 28.6%, P = 0.008• 100 randomized patients
Mui WL, Ng CS, Fung TM, et al. Prophylactic ilioinguinal neurectomy in open inguinal hernia repair: a double-blind randomized controlled trial. Ann Surg. 2006;244:27–33.
14
Neurectomy Italy: 973 cases
• Preservation vs. division of all three inguinal nerves• Overall (mild, moderate, and severe) groin pain at 6 months and 1
year of follow-up was 9.7% and 4.1%• No pain in any case of hernia repair when all 3 nerves were preserved• Risk of groin pain increases with number of nerves undetected• Relative risk increases from 2.2 to 19.2, if 1 or 3 nerves have not been
recognized• Division of nerves was clearly correlated with presence of chronic pain
Alfieri S, Rotondi F, Di Giorgio A, et al. Influence of preservation versus division of ilioinguinal, iliohypogastric, and genital nerves during open mesh herniorrhaphy: prospective multicentric study of chronic pain. Ann Surg. 2006;243:553–558

15
Neurectomy Although routine prophylactic neurectomy during groin
hernia repair is safe and may reduce the incidence of post-herniorrhaphy neuralgia, it may lead to troublesome sensory changes such as numbness or dysesthesia in some patients. Thus, the choice of groin nerve preservation versus sacrifice should be made individually for each patient after careful discussion of potential outcomes.

16
Question #3Should the asymptomatic patient undergo elective hernia repair?
17
Asymptomatic Patients Multicenter RCT: immediate tension-free repair vs. watchful
waiting• Minimally symptomatic inguinal hernias• 353 patients • Immediate repair (< or = 6 months, N = 288)• Delayed repair (> 6 months, N = 65)• Comparable surgical time, surgical complications, recurrence rates,
and satisfaction with outcome• Multivariate analyses: no relation between duration until hernia repair
and operative time, incidence of complications, long-term pain, or functional status
Thompson JS, Gibbs JO, et al. Does delaying repair of an asymptomatic hernia have a penalty? Am J Surg. 2008 Jan;195(1):89-93
18
Asymptomatic Patients RCT January 1999 through December 2004,
• 720 men (364 watchful waiting, 356 surgical repair) followed up for 2 to 4.5 years.
• Watchful-waiting patients followed up at 6 months and annually• Repair patients received standard open tension-free repair and were
followed up at 3 and 6 months and annually• Primary intention-to-treat outcomes were similar at 2 years for watchful
waiting vs surgical repair• Pain limiting activities (5.1%(S) vs 2.2% (WW), respectively; P=.52) • PCS (improvement over baseline, 0.29 points vs 0.13 points; P=.79)• 23% of patients assigned to watchful waiting crossed over to receive
surgical repair• 17% assigned to receive repair crossed over to watchful waiting
19
Asymptomatic Patients• Occurrence of postop complications was similar in patients who
received repair as assigned and in watchful-waiting patients who crossed over
• One watchful-waiting patient (0.3%) experienced acute hernia incarceration without strangulation within 2 years
• One watchful-waiting patient (0.3%) had acute incarceration with bowel obstruction at 4 years
• Frequency of 1.8/1000 patient-years inclusive of patients followed up for as long as 4.5 years
Watchful waiting is an acceptable option for men with minimally symptomatic inguinal hernias. Delaying surgical repair until symptoms increase is safe because acute hernia incarcerations occur rarely
Fitzgibbons RJ, Giobbie-Hurder A, et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. JAMA. 2006 Jan 18;295(3):285-92.

20
Asymptomatic Patients Patients followed for an additional 7 years with a maximum follow-
up of 11.5 years. T The estimated cumulative CO rates using Kaplan-Meier analysis
was 68%. Men older than 65 years crossed over at a considerably higher rate
than younger men (79% vs 62%). The most common reason for CO was pain (54.1%). A total of 3
patients have required an emergency operation, but there has been no mortality.
Men who present to their physicians because of an inguinal hernia even when minimally symptomatic should be counseled that although WW is a reasonable and safe strategy, symptoms will likely progress and an operation will be needed eventually.
Fitzgibbons RJ, Ramanan B, et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. Ann Surg. 2013 Sep;258(3):508-15.
21
Question #4What approach should be used in the repair of an incarcerated / strangulated hernia?
22
Question #4What approach should be used in the repair of an incarcerated / strangulated hernia?
OPEN
LAPAROSCOPIC
IT DOESN’T MATTER
23
Question 4b Can the repair of a strangulated hernia involve
mesh?

24
Question 4b Can the repair of a strangulated hernia involve
mesh?
YES
NO
25
Use of Mesh in a Contaminated Field
The use of porcine small intestinal submucosa as a prosthetic material for laparoscopic hernia repair in infected and potentially
contaminated fields: long-term follow-up.
Franklin ME, Trevino JM, Portillo G, Vela I, Glass JL, Gonzalez JJ
Surg Endosc. 2008 Sep;22(9):1941-6
26
Use of Mesh in a Contaminated Field May 2000 to October 2006 116 patients 133 procedures Surgisis mesh (porcine SIS) in infected or potentially contaminated Studied in a prospective fashion All laparoscopic Mean follow-up was 52 +/- 20.9 months 39 cases: infected field
• 25 intestinal obstruction• 16 strangulated hernias• 17 required small bowel resection• 85% 5-year follow-up• 7 recurrences
27
Use of Mesh in a Contaminated Field
Outcomes of synthetic mesh in contaminated ventral hernia repairs.
Carbonell AM, Criss CN, Cobb WS, Novitsky YW, Rosen MJ
J Am Coll Surg. 2013 Dec; 217(6):991-8

28
Use of Mesh in a Contaminated Field Open VHRs performed with polypropylene mesh in the retro-rectus
position in clean-contaminated and contaminated fields were evaluated
100 patients Mean age of 60 ± 13 years Mean BMI of 32 ± 9.3 42 clean-contaminated and 58 contaminated cases SSO: 26.2% (clean-contaminated) and 34% (contaminated) 30 day SSI: 7.1% (clean-contaminated) and 19.0% (contaminated) 7 recurrences with mean follow-up of 10.8 ± 9.9 months Mesh removal was required in 4 patients
• 2 due to early anastomotic leaks• 1 due to stomal disruption and retraction in a morbidly obese patient• 1 from a long-term enterocutaneous fistula
29
Question #6What is the best approach for the repair of a recurrent hernia?
30
Question #6What is the best approach for the repair of a recurrent hernia?
OPEN
LAPAROSCOPIC
IT DOESN’T MATTER
31
Question #6What is the best approach for the repair of a recurrent hernia AFTER AN ANTERIOR REPAIR?
What is the best approach for the repair of a recurrent hernia AFTER AN POSTERIOR REPAIR?

32
Approach to the Patient with Pain
33
Approach to the Patient with Pain Avoiding pain
• Absorbable sutures associated with a lower rate and shorter duration of postoperative groin pain, compared with nonabsorbable sutures
Jeroukhimov I, Wiser I, Karasic E, et al. Reduced postoperative chronic pain after tension-free inguinal hernia repair using absorbable sutures: a single-blind randomized clinical trial. J Am Coll Surg 2014; 218:102.
• Use of fibrin glue (eg, Tisseel/Tissucol) has been shown to reduce postoperative pain in both open and laparoscopic approaches
Benizri EI, Rahili A, Avallone S, et al. Open inguinal hernia repair by plug and patch: the value of fibrin sealant fixation. Hernia 2006; 10:389.Campanelli G, Pascual MH, Hoeferlin A, et al. Randomized, controlled, blinded trial of Tisseel/Tissucol for mesh fixation in patients undergoing Lichtenstein technique for primary inguinal hernia repair: results of the TIMELI trial. Ann Surg 2012; 255:650.Tolver MA, Rosenberg J, Juul P, Bisgaard T. Randomized clinical trial of fibrin glue versus tacked fixation in laparoscopic groin hernia repair. Surg Endosc 2013; 27:2727.Berney CR, Yeo AE. Mesh fixation with fibrin sealant during endoscopic totally extraperitoneal inguinal hernia approach: a review of 640 repairs. Hernia 2013; 17:709.Shah NS, Fullwood C, Siriwardena AK, Sheen AJ. Mesh fixation at laparoscopic inguinal hernia repair: a meta-analysis comparing tissue glue and tack fixation. World J Surg 2014; 38:2558.Antoniou SA, Köhler G, Antoniou GA, et al. Meta-analysis of randomized trials comparing nonpenetrating vs mechanical mesh fixation in laparoscopic inguinal hernia repair. Am J Surg 2016; 211:239.Sun P, Cheng X, Deng S, et al. Mesh fixation with glue versus suture for chronic pain and recurrence in Lichtenstein inguinal hernioplasty. Cochrane Database Syst Rev 2017; 2:CD010814.
34
Approach to the Patient with Pain Avoiding pain
• The use of cyanoacrylate glue (Histoacryl) did not reduce postoperative pain in patients who underwent repair
Rönkä K, Vironen J, Kössi J, et al. Randomized Multicenter Trial Comparing Glue Fixation, Self-gripping Mesh, and Suture Fixation of Mesh in Lichtenstein Hernia Repair (FinnMesh Study). Ann Surg 2015; 262:714.Hoyuela C, Juvany M, Carvajal F, et al. Randomized clinical trial of mesh fixation with glue or sutures for Lichtenstein hernia repair. Br J Surg 2017; 104:688.
• The use of a self-gripping mesh (Progrip) did not reduce the risk of chronic pain compared with a standard mesh secured with sutures
Rönkä K, Vironen J, Kössi J, et al. Randomized Multicenter Trial Comparing Glue Fixation, Self-gripping Mesh, and Suture Fixation of Mesh in Lichtenstein Hernia Repair (FinnMesh Study). Ann Surg 2015; 262:714.Pandanaboyana S, Mittapalli D, Rao A, et al. Meta-analysis of self-gripping mesh (Progrip) versus sutured mesh in open inguinal hernia repair. Surgeon 2014; 12:87.Verhagen T, Zwaans WA, Loos MJ, et al. Randomized clinical trial comparing self-gripping mesh with a standard polypropylene mesh for open inguinal hernia repair. Br J Surg 2016; 103:812.
35
Approach to the Patient with PainManagement of pain
• Postoperative pain is common and easily treated– Opioids – Nonsteroidal anti-inflammatory drugs (NSAIDs).
• Most often, pain subsides within six to eight weeks• When pain persists beyond three months
– Not attributable to another cause– Post-herniorrhaphy neuralgia diagnosed– Managed with multimodal analgesia including a nerve block

36
Approach to the Patient with PainManagement of pain in patients diagnosed with
neuralgia• Groin nerve block should be performed
– Control pain– Confirm diagnosis (block should relieve the pain of
neuralgia)• Usually performed by a pain specialist • Can be performed by a surgeon• Nerve block
– Long-acting local anesthetic– Glucocorticoid– Injected into the tissue surrounding the affected nerve
37
Approach to the Patient with PainManagement of pain
• Groin nerve block can break the pain cycle and cures the neuralgia.
• In others, pain recurs after the effect of treatment wears off in a few days.
• Patients with a positive response to an initial nerve block can be treated with weekly injections until pain relief becomes sustained.
• For those who fail to achieve a sustained response to repeated nerve blocks, groin nerve sacrifice may be best option

38
Approach to the Patient with PainManagement of pain
• Response to a nerve block, even a transient one, indicates that the pain is neuropathic in origin.
• If a specific groin nerve block (eg, ilioinguinal or iliohypogastric) is reproducibly effective, but the effect is transient, that nerve can be sacrificed to achieve permanent pain relief.
• Nerve sacrifice can be accomplished by percutaneous nerve ablation or surgical neurectomy.
• Nerve ablation– Performed in a similar manner to nerve block except that a
neurolytic solution such as phenol or alcohol is injected instead of a local anesthetic
– Destroys the offending nerve ending and reduces chronic inflammation caused by the mesh or postoperative fibrosis
– Alternative techniques include radiofrequency ablation or cryoablation
39
Approach to the Patient with PainManagement of pain
• Outcomes of percutaneous nerve ablation may be less favorable than surgical nerve excision– Nerve ablation is minimally invasive– Does not cause significant side effects– Those who respond to a nerve ablation can be spared of
potential complications of a surgical neurectomy• Observational studies: surgery appears to be the most effective
treatment for persistent groin pain in patients with neuralgia– Groin exploration and neurectomy– Neurolysis– Simple nerve division– Mesh excision alone
40
Approach to the Patient with PainManagement of pain
• Nerve excision (neurectomy) relieves groin pain in the majority of patients with post-herniorrhaphy neuralgia and is indicated when all other measures to control pain have failed
Success rates range from 70 to 100 percent Madura JA, Madura JA 2nd, Copper CM, Worth RM. Inguinal neurectomy for inguinal nerve entrapment: an experience with 100 patients. Am J Surg 2005; 189:283.Keller JE, Stefanidis D, Dolce CJ, et al. Combined open and laparoscopic approach to chronic pain after inguinal hernia repair. Am Surg 2008; 74:695.Loos MJ, Scheltinga MR, Roumen RM. Tailored neurectomy for treatment of postherniorrhaphy inguinal neuralgia. Surgery 2010; 147:275.Rosen MJ, Novitsky YW, Cobb WS, et al. Combined open and laparoscopic approach to chronic pain following open inguinal herniarepair. Hernia 2006; 10:20.Delikoukos S, Fafoulakis F, Christodoulidis G, et al. Re-operation due to severe late-onset persisting groin pain following anterior inguinal hernia repair with mesh. Hernia 2008; 12:593.Deysine M, Deysine GR, Reed WP Jr. Groin pain in the absence of hernia: a new syndrome. Hernia 2002; 6:64.Starling JR, Harms BA, Schroeder ME, Eichman PL. Diagnosis and treatment of genitofemoral and ilioinguinal entrapment neuralgia.Surgery 1987; 102:581.Bower S, Moore BB, Weiss SM. Neuralgia after inguinal hernia repair. Am Surg 1996; 62:664.

41
Approach to the Patient with PainManagement of pain
• Nerve excision (neurectomy) relieves groin pain in the majority of patients with post-herniorrhaphy neuralgia and is indicated when all other measures to control pain have failed
Success rates range from 70 to 100 percent Kim DH, Murovic JA, Tiel RL, Kline DG. Surgical management of 33 ilioinguinal and iliohypogastric neuralgias at Louisiana State University Health Sciences Center. Neurosurgery 2005; 56:1013.Stulz P, Pfeiffer KM. Peripheral nerve injuries resulting from common surgical procedures in the lower portion of the abdomen. Arch Surg 1982; 117:324.Hameroff SR, Carlson GL, Brown BR. Ilioinguinal pain syndrome. Pain 1981; 10:253.Murovic JA, Kim DH, Tiel RL, Kline DG. Surgical management of 10 genitofemoral neuralgias at the Louisiana State University Health Sciences Center. Neurosurgery 2005; 56:298.Nahabedian MY, Dellon AL. Outcome of the operative management of nerve injuries in the ilioinguinal region. J Am Coll Surg 1997;184:265.Amid PK. Causes, prevention, and surgical treatment of postherniorrhaphy neuropathic inguinodynia: triple neurectomy with proximal end implantation. Hernia 2004; 8:343.Krähenbühl L, Striffeler H, Baer HU, Büchler MW. Retroperitoneal endoscopic neurectomy for nerve entrapment after hernia repair.Br J Surg 1997; 84:216.Zacest AC, Magill ST, Anderson VC, Burchiel KJ. Long-term outcome following ilioinguinal neurectomy for chronic pain. J Neurosurg 2010; 112:784.Wong J, Anvari M. Treatment of inguinodynia after laparoscopic herniorrhaphy: a combined laparoscopic and fluoroscopic approach to the removal of helical tackers. Surg Laparosc Endosc Percutan Tech 2001; 11:148.

42
Approach to the Patient with Pain