information sharing and public private partnerships .../media/files/activity files... ·...
TRANSCRIPT
Information Sharing and Public Private Partnerships: Responding to 2009 H1N1
Pandemic
Aaron DeVries, MD MPH Medical Director, Infectious Disease Division
Minnesota Department of Health
1
April 1, 2009
http://www.jornada.unam.mx/ultimas/2009/04/01/veracruz-reporta-agente-municipal-extrano-brote-epidemico-que-ha-cobrado-dos-vidas

Death
Critical Illness
Hospitalization
Moderate Outpatient Illness
Mild Outpatient Illness
Minimal or No Symptoms
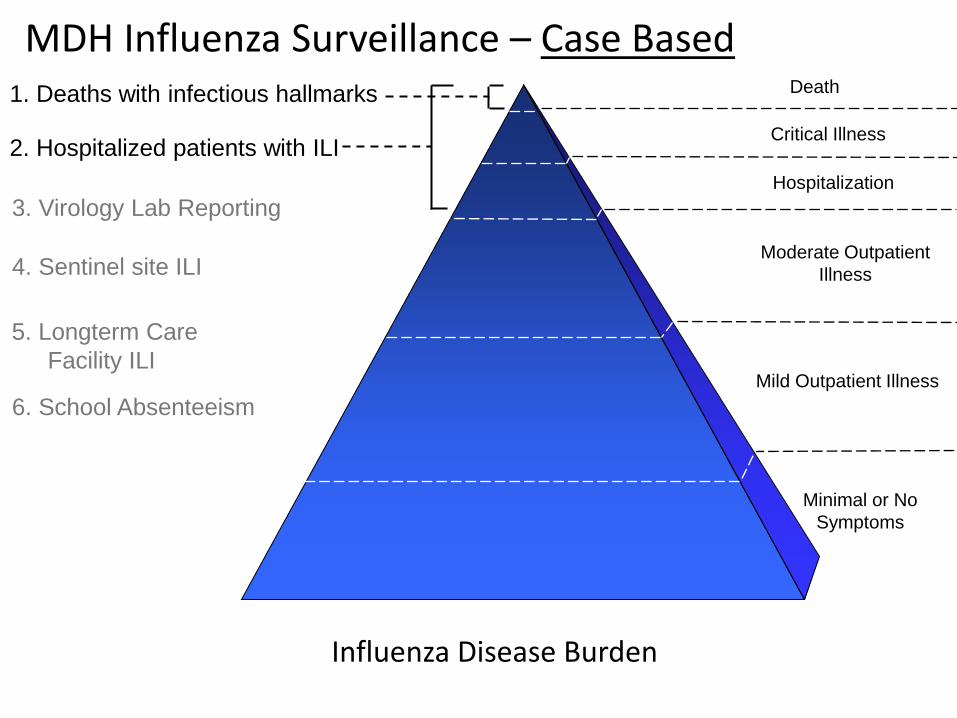
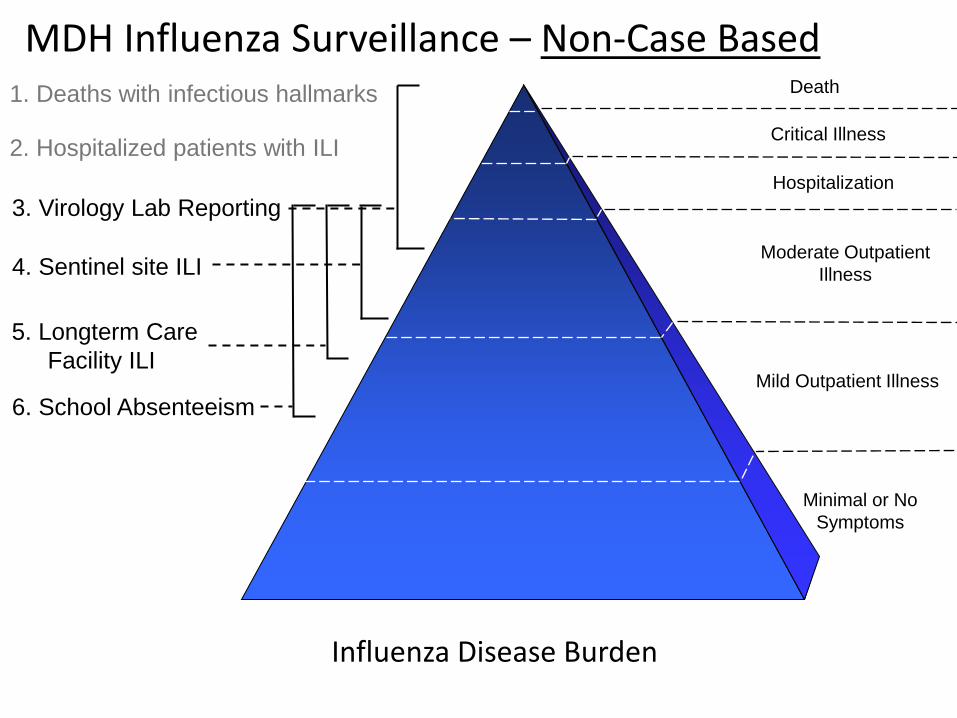
1. Deaths with infectious hallmarks
2. Hospitalized patients with ILI
3. Virology Lab Reporting
Influenza Disease Burden
MDH Influenza Surveillance – Case Based
6. School Absenteeism
5. Longterm Care Facility ILI
4. Sentinel site ILI
1. Deaths with infectious hallmarks
2. Hospitalized patients with ILI
3. Virology Lab Reporting
6. School Absenteeism
5. Longterm Care Facility ILI
4. Sentinel site ILI
Influenza Disease Burden
MDH Influenza Surveillance – Non-Case Based Death
Critical Illness
Hospitalization
Moderate Outpatient Illness
Mild Outpatient Illness
Minimal or No Symptoms
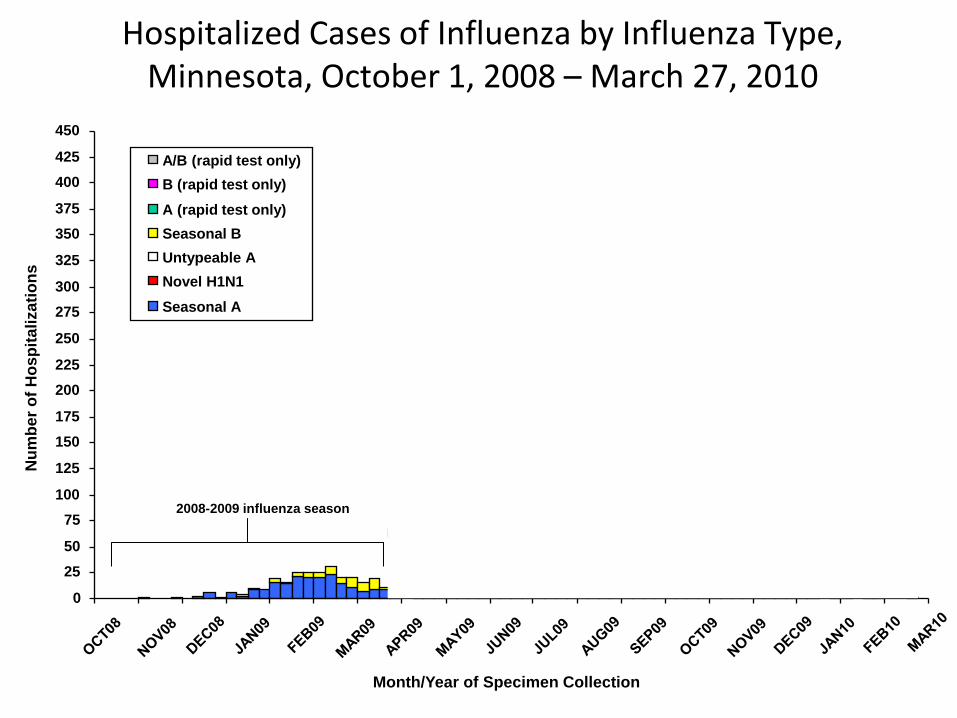
Hospitalized Cases of Influenza by Influenza Type, Minnesota, October 1, 2008 – March 27, 2010
2008-2009 influenza season
2009-2010 influenza season 2nd H1N1 wave
Summer surveillance 1st H1N1 wave
1st H1N1 hospitalized
case
0
25
50
75
100
125
150
175
200
225
250
275
300
325
350
375
400
425
450
Month/Year of Specimen Collection
Num
ber o
f Hos
pita
lizat
ions
A/B (rapid test only) B (rapid test only) A (rapid test only) Seasonal B Untypeable A Novel H1N1
Seasonal A
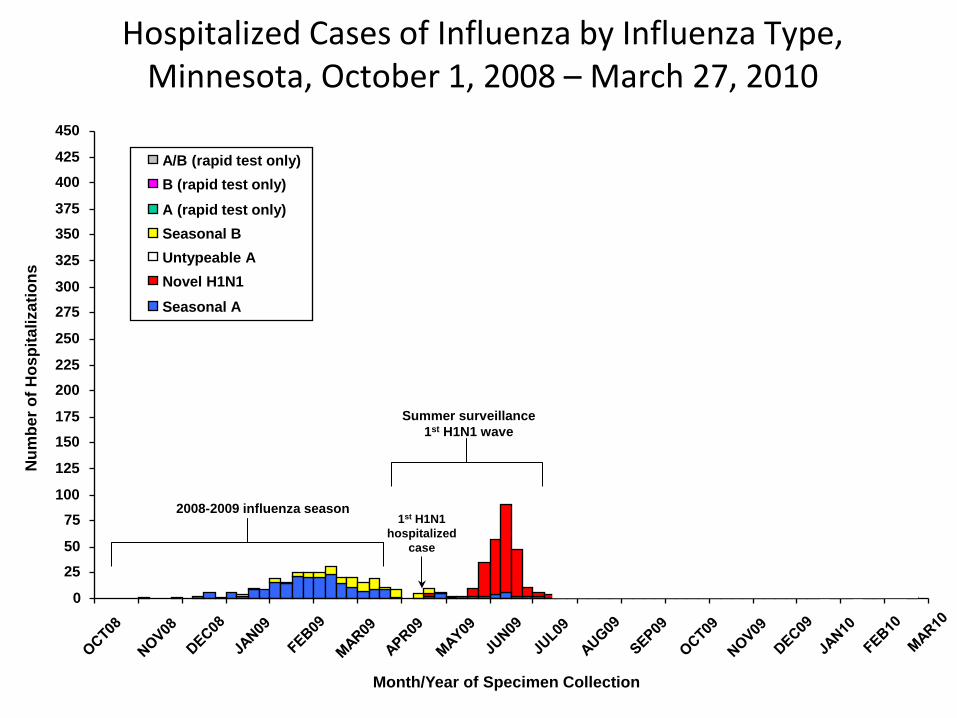
Hospitalized Cases of Influenza by Influenza Type, Minnesota, October 1, 2008 – March 27, 2010
2008-2009 influenza season
2009-2010 influenza season 2nd H1N1 wave
Summer surveillance 1st H1N1 wave
1st H1N1 hospitalized
case
0
25
50
75
100
125
150
175
200
225
250
275
300
325
350
375
400
425
450
Month/Year of Specimen Collection
Num
ber o
f Hos
pita
lizat
ions
A/B (rapid test only) B (rapid test only) A (rapid test only) Seasonal B Untypeable A Novel H1N1
Seasonal A
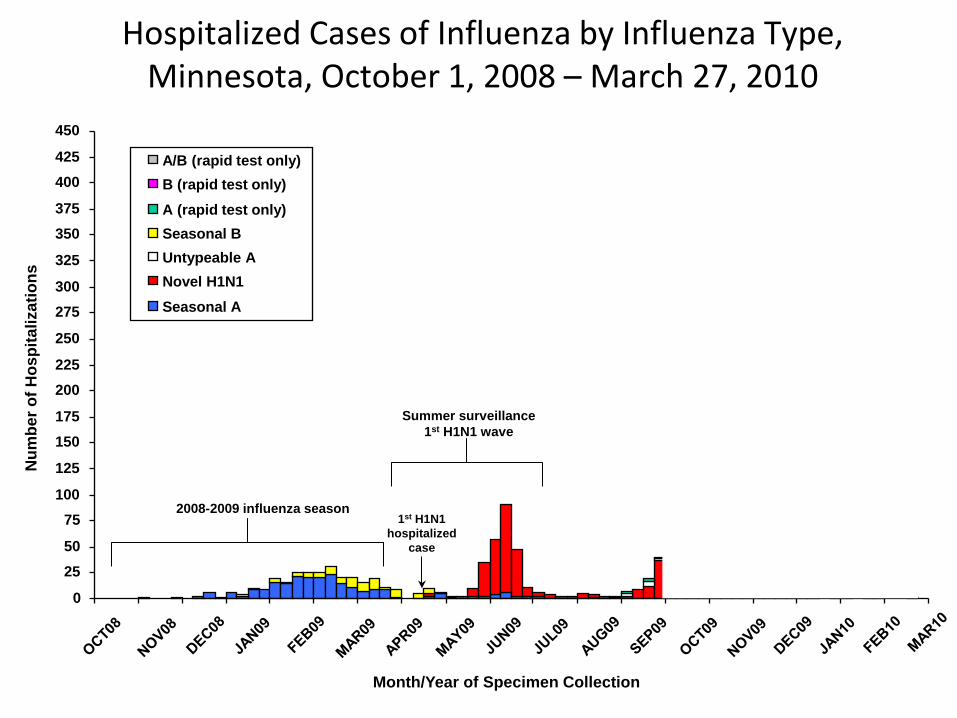
Hospitalized Cases of Influenza by Influenza Type, Minnesota, October 1, 2008 – March 27, 2010
2008-2009 influenza season
2009-2010 influenza season 2nd H1N1 wave
Summer surveillance 1st H1N1 wave
1st H1N1 hospitalized
case
0
25
50
75
100
125
150
175
200
225
250
275
300
325
350
375
400
425
450
Month/Year of Specimen Collection
Num
ber o
f Hos
pita
lizat
ions
A/B (rapid test only) B (rapid test only) A (rapid test only) Seasonal B Untypeable A Novel H1N1
Seasonal A

Novel A H1N1 Hospitalizations per 100,000 PersonsMinnesota, April 1, 2009 - January 30, 2010
0
2
4
6
8
10
12
14
17-18
19-20
21-22
23-24
25-26
27-28
29-30
31-32
33-34
35-36
37-38
39-40
41-42
43-44
45-46
47-48
49-50
51-52 1-2
MMWR Week of Specimen Collection
Hos
pita
lizat
ions
per
100
,000
per
sons 7-county MSP Greater MN
“Summer wave”
“Fall wave”
Smoothed lines
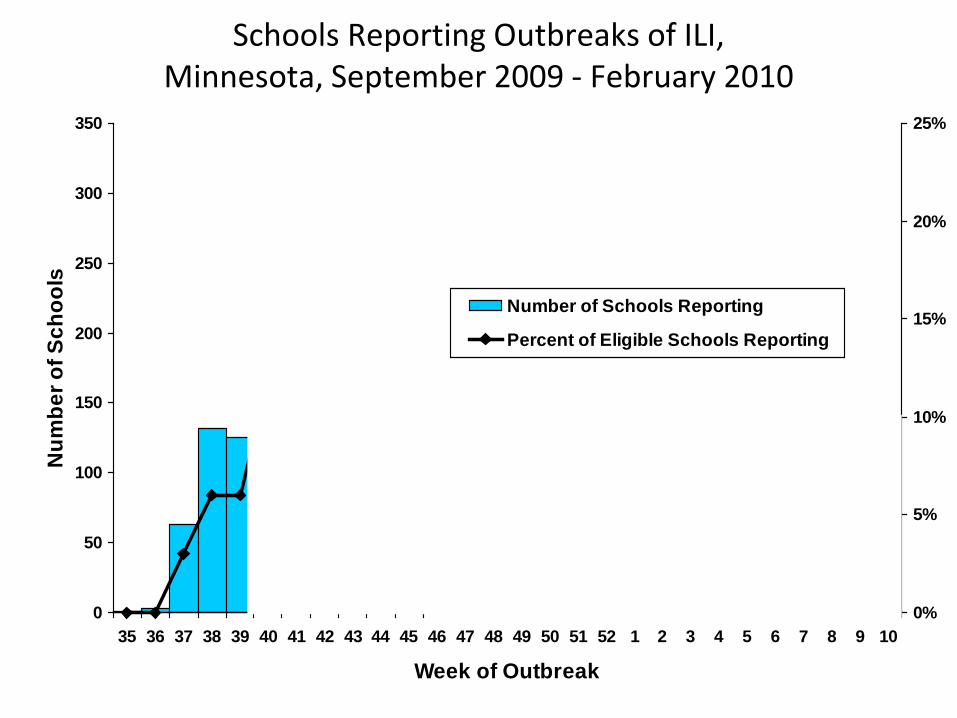
Schools Reporting Outbreaks of ILI, Minnesota, September 2009 - February 2010
0
50
100
150
200
250
300
350
35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 1 2 3 4 5 6 7 8 9 10
Week of Outbreak
Num
ber o
f Sch
ools
0%
5%
10%
15%
20%
25%
Number of Schools Reporting
Percent of Eligible Schools Reporting
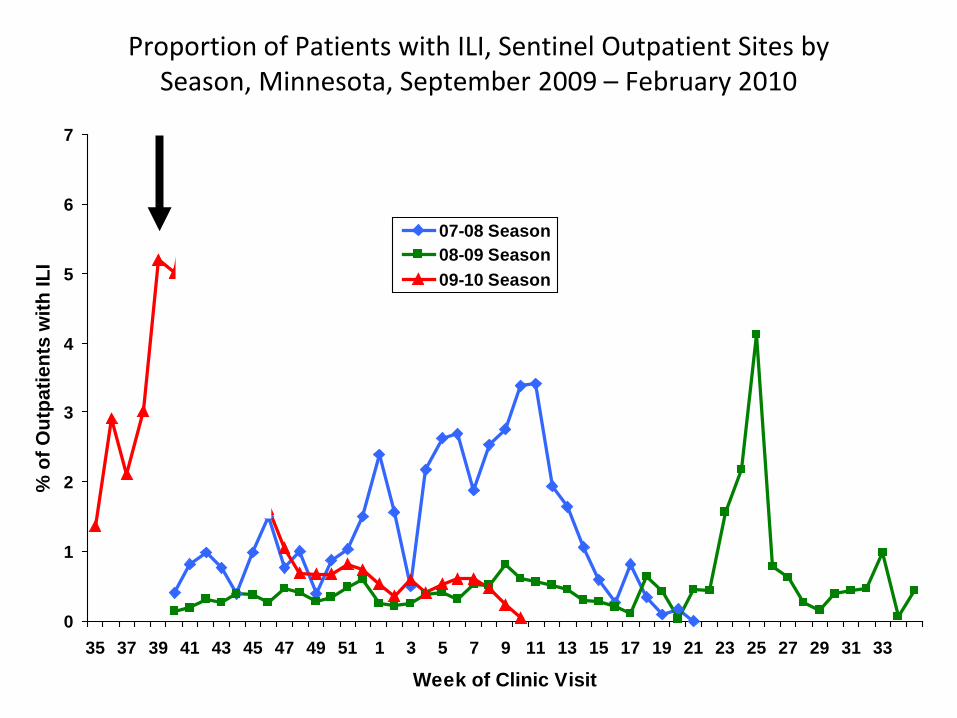
Proportion of Patients with ILI, Sentinel Outpatient Sites by Season, Minnesota, September 2009 – February 2010
0
1
2
3
4
5
6
7
35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33
Week of Clinic Visit
% o
f Out
patie
nts
with
ILI
07-08 Season08-09 Season09-10 Season
http://www.health.state.mn.us/divs/idepc/diseases/flu/stats/index.html
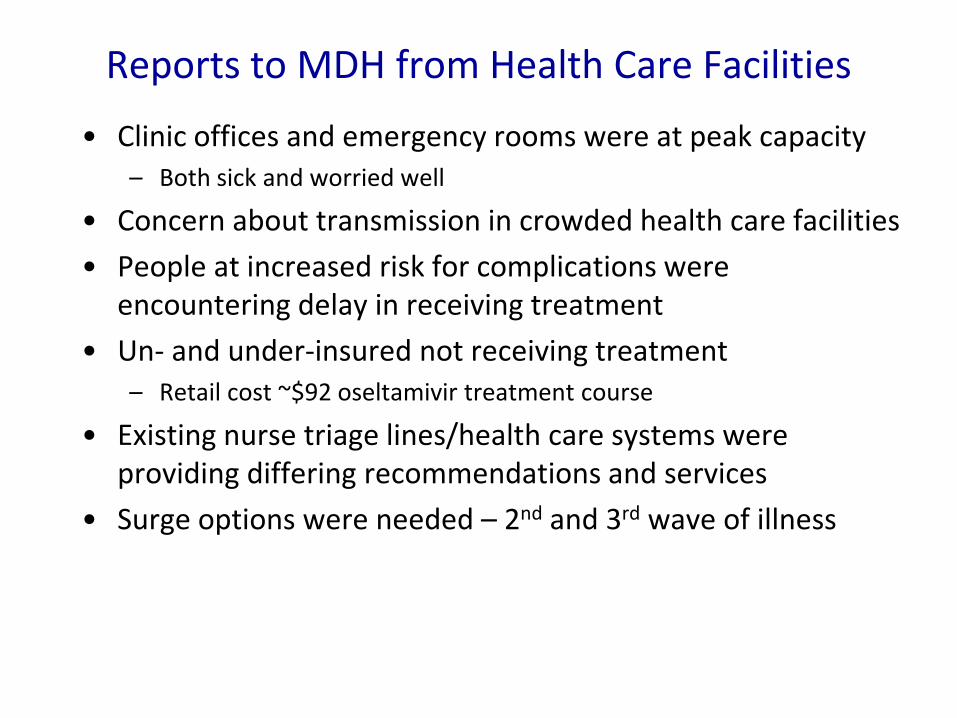
Reports to MDH from Health Care Facilities
• Clinic offices and emergency rooms were at peak capacity – Both sick and worried well
• Concern about transmission in crowded health care facilities • People at increased risk for complications were
encountering delay in receiving treatment • Un- and under-insured not receiving treatment
– Retail cost ~$92 oseltamivir treatment course
• Existing nurse triage lines/health care systems were providing differing recommendations and services
• Surge options were needed – 2nd and 3rd wave of illness

MDH Challenges • Vaccine was weeks/months away • Large stock of MN and federal purchased
antivirals • High priority
– Maintaining a sustained response – Un- under-insured – Rapid treatment when needed – Ensuring a supply for those who were unable to
get antivirals through usual supply chain
Development of MN FluLine
• Multiple evaluation/distribution models discussed – An infection preventionist at a children's hospital
approached MDH with the idea for an integrated Nurse Triage Lines (NTL)
• Nurse triage line seemed to be the most effective and quickest to operationalize – Rapid evaluation – Target high risk groups – Recommend level of care (home vs clinic vs ER) – Recommend antiviral if home care advised
Private Health Partners: All MN health systems with an NTL
17
FluLine Single Point of Contact

Development of Partnerships
• MDH contacted all health care systems with an NTL – All agreed to coordinate NTL services – Provide an integrated NTL with a single toll free number – Standard protocol for evaluation – NTL would prescribe oseltamivir via protocol when
indicated and call in a script to a local pharmacy – Pharmacies separately contracted with MDH to distribute
state stockpile meds • Communication tools
– Multiple (daily) conference calls, in-person meetings – NTL decision makers and Medical Directors
• Vendor was identified to operate system • Named Minnesota FluLine
18 Public Health Rep, 2012; 127: 532-40

Sept Oct Nov
First MDH discussion on NTL
2009
First conference call with health plans
21
MN FluLine Launch and Press Conference
Protocol Development
NTL provider contract work
Pharmacy contract work
Antiviral placement in pharmacies
NTL training
Timeline of FluLine Development

Callers to 1-866-259-4655
Medical Screener Contract Provider
Not ill, not exposed - Information only
• 211 • MDH public hotline • Websites (MDH, CDC, Mayo) • Other community resources
Ill or exposed to someone with ILI
MN FluLine System Design
20 Public Health Rep, 2012; 127: 532-40

Callers to 1-866-259-4655
Medical Screener Contract Provider
Not ill, not exposed - Information only
• 211 • MDH public hotline • Websites (MDH, CDC, Mayo) • Other community resources
Ill or exposed to someone with ILI
Health plan participating in the MN
Flu Line
Partner administers MDH protocol
MN FluLine System Design
No insurance or health plan not participating in
MN FluLine
Contractor administers MDH
protocol
21 Public Health Rep, 2012; 127: 532-40


MDH Protocol
Home Care Only Home Care AND Antiviral indicated
Call MD Go to ED Call 911
Clinical Evaluation
See MD
23 Public Health Rep, 2012; 127: 532-40

MDH Protocol
Home Care Only Home Care AND Antiviral indicated
Call MD Go to ED Call 911
Clinical Evaluation
See MD
RN prescribes per protocol
Retail Pharmacy dispenses
Market Supply Insurance billed
State and Federal Stockpile
• Uninsured • Underinsured • Market interruptions
Antiviral Distribution
24 Public Health Rep, 2012; 127: 532-40

25
FluLine Data • Reported 1-3 days to MDH
– Total call numbers to the toll free number – Call numbers managed by our contractor where the
medical protocol was administered
• Not reported timely – Data on calls transferred to partner NTLs – Demographics, severity of illness of callers – Number accessing state oseltamivir stockpile – Clinical outcome – Satisfaction with service – Collected from a sample of callers during program
evaluation after completion
26

Week of Specimen Collection or MN FluLine Call
Num
ber o
f Hos
pita
lizat
ions
0
50
100
150
200
250
300
350
400
34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 1 2 3 4 5 6 7 8 9 10 0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
Cal
ls to
MN
Flu
Line
Sept Oct Nov Dec Jan Feb Mar
Minnesota Hospitalized PCR-Confirmed 2009 H1N1 Cases and Calls to MN FluLine, Sept. 2009 – February 2010
2009 H1N1 Hospitalizations
Calls to MN FluLine
2009 2010
Public Health Rep, 2012; 127: 532-40 27
Public Health Rep, 2012; 127: 532-40

MDH Protocol N=5,949
Home Care Only Home Care AND Antiviral indicated
Call MD Go to ED Call 911
Clinical Evaluation
See MD
2,292 (39%) 374 (6%) 1,292 (22%) 875 (15%) 122 (2%)
Other
496 (8%)
497 (8%)
39%
6% 8%
22%
15%
2% 8%
3,659 (62%) were recommended to NOT seek in-person care

Impact • Over 27,000 individuals called (0.5% of Minnesotans)
– Over 17,000 needed information only – Median age of patient - 22 years – Callers were from 86 counties – 14% had no insurance coverage (MN uninsured rate in 2009 - 9%)
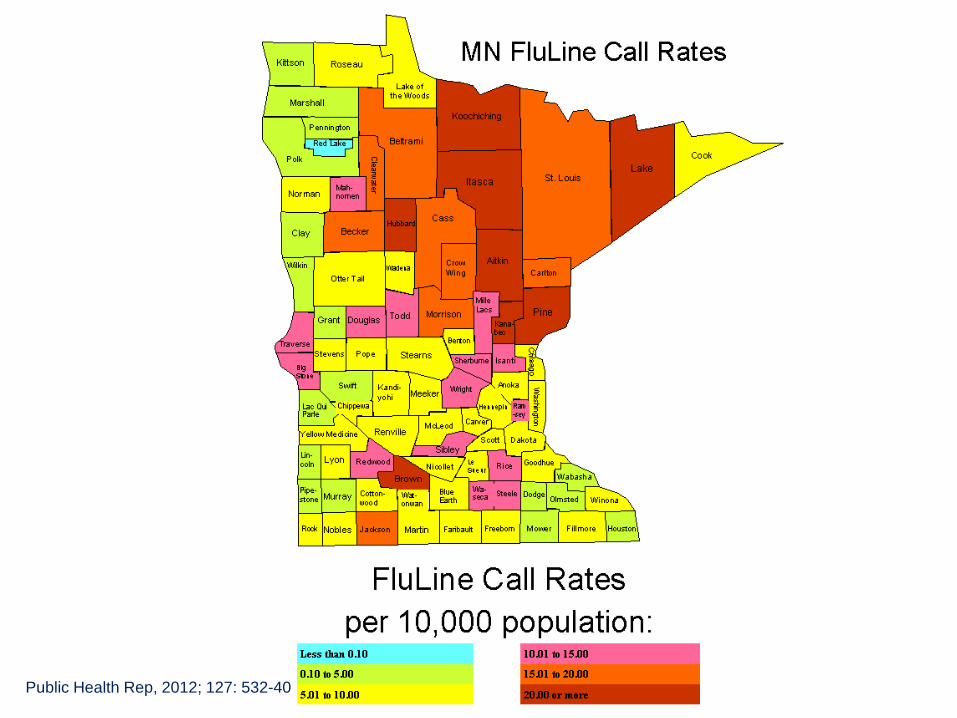
• Highest call volumes per capita were in predominantly rural, northeast MN
• Up to an estimated 11,000 in-person health care encounters prevented
• 92% were satisfied or very satisfied with their experience • Contract cost of MN FluLine service was $331,226
30 Public Health Rep, 2012; 127: 532-40 PLOS ONE, 2013, 8(1): e50492. doi:10.1371/journal.pone.0050492

Lessons Learned • Telephonic triage can have a major impact on decompressing
the healthcare system • Leverage existing infrastructure
– Health plans and healthcare delivery organizations wanted to keep their own patients
– Nurse triage in MN was well established – Pharmacists could have performed the same function
• System was designed for clinical service and not data collection. If more time and planning: – Realtime numbers of callers and their clinical presentation – Geo-location, demographics – Outcome of those who had the protocol administered
31

Lessons Learned • Data collection was a direct cost to our vendors
– Type and amount of data collected was addressed in contract
– Prioritize each data point collected
• Over estimate the service use during a time of crisis • Find decision makers as quickly as possible
– Getting prescriber buy-in on the protocol was critical
• Engagement with pharmacies earlier – Distribution fee – Burden of documentation required
• Legal framework in MN is not typical 32

Acknowledgements Minnesota Department of Health • Dr. Ruth Lynfield • Commissioner Dr. Sanne Magnan • Alison Spaulding • Deb Radi • Michelle Larson • Craig Acomb • Legal Unit Staff • Infectious Disease Division Staff • Office of Emergency Preparedness Staff
Children’s Physician Network • Heather Macleod • Dr. Peter Dehnel • Terri Hyduke • Nursing and triage staff
Children’s Hospitals and Clinics • Patsy Stinchfield
University of Minnesota • Dr. John Nyman • Dr. Judith Garrard • Dr. Eileen Harwood
Centers for Disease Control and Prevention • Dr. Alex Kallen • Dr. John Jernigan • Public Health Emergency Response Grant • Influenza Division • Emerging Infections Program
Health Care System Partners • Blue Cross and Blue Shield of MN • Children’s Hospitals and Clinics of MN • Children’s Physician Network • Fairview Health Service • HealthPartners • Mayo Clinic • Medica • Metropolitan Health Plan • OptumHealth • Park Nicollet Health Services • Prime West Health • Saint Mary’s Duluth Clinics • UCare • United Way 211
33

Legal Framework • Existing MN legal framework allowed this activity
– A licensed practitioner may prescribe without reference to a specific patient via a protocol administered by a nurse, medical student, physician assistant, or pharmacist – MN Statute 151.37
– Supported by MN Mass dispensing authority – MN Statute 144.4198
– All partner Nurse Triage Lines had a medical director who already approved their protocols
35

Legal Framework (cont.) • Improving buy-in from non-governmental partners
– Allow all medical directors of partner NTL’s to edit the protocol – became a consensus document
– Federal public health emergency declaration – PREP Act – State Epidemiologist and Medical Director signed the
protocol under the delegated authority of the Commissioner of Health (also a physician)
– Coordination with the Board of Pharmacy
36