influenza in
TRANSCRIPT

POSTGRAD. MED. J. (I963), 39, 567
INFLUENZA IN HOSPITAL 1960-1961G. W. HEARN, M.B.E., M.D., M.R.C.P.Physician, Dudley Road Hospital, Birmingham
DURING most winters the regional hospitals inBirmingham have become accustomed to receive anembarrassing number of acute respiratory dis-orders as emergency admissions. The clinical andepidemiological features of these periodic surgesof respiratory disease posed problems of interestand difficulty. Precise classification of individualcases might be a matter of conjecture. In patientsshowing close clinical similarity several differentkinds of bacteria might be cultured, often morethan one concurrently or serially in the same case,or none might be obtained. Radiological appear-ances varied widely. An increase in the numberof these apparently different respiratory casesat the same time, however, suggested commonfactors. The influenza virus was known to be oneof these factors. It therefore seemed desirableto investigate the range and frequency of clinicalphenomena observed in hospital admissionsduring an epidemic and to relate these clinicalstudies to the evidence of virus infection.An epidemic of influenza A2 in Birmingham in
late December i960 was therefore studied. Theonset of the epidemic was rapid; this led toprompt recognition of the epidemic situation andearly identification of the virus responsible. It wastherefore possible to undertake a clinical andvirological study of all the respiratory admissionsto a medical unit at Dudley Road Hospital duringthe course of the epidemic, the virological studybeing undertaken by Dr. Flewett. Non-respiratorycases were included in the study where influenzaappeared a possible cause. To present the rangeof clinical cases observed and to relate them toevidence of virus infection is the purpose of thispaper.
EpidemiologyDuring the last weeks of I960 there had been no
prevalence of febrile disorders and no influenzahad been reported in the British Isles. Theexistence of complicated influenza became apparenton December 26, I960, after the admission oftwo patients with fulminating staphylococcalpneumonia and three patients with influenzalbronchopneumonia. Thereafter the number ofadmissions for acute respiratory disorders rosesharply and remained high until the end of January
FIG. I.-Birmingham Bed Bureau, November I960 toMarch i96i (see text).
I96I. The progress of the epidemic was con-veniently delineated by the rise and fall inemergency admissions to Birmingham hospitalsthrough the Birmingham Emergency Bed Bureau.
In I960 the average weekly admissions were250. Fig. i shows the weekly admissions inexcess of this figure during the epidemic and chartsthe additional beds needed on the assumption of atwo-week and three-week stay.
During the winter of I960-6I the EmergencyBed Bureau did not return respiratory admissionstatistics separately, but did so subsequently.During the next winter it was therefore possibleto demonstrate in a similar epidemic that theincrease in admissions during the epidemic periodwas almost entirely due to the respiratory disorders(Fig. 2).
VirologyIn all, 103 patients were included in this study.
The intention was to take paired sera in all casesfor complement fixation studies; this was frustratedby some early deaths and some practical difficultiesbut at least one serum was obtained from each ofgo patients and on these complement fixationstudies were performed by Dr. Flewett and arereported here. His culture of autopsy materialand hmmagglutination inhibition studies confirmedthat the epidemic was due to influenza A2.
SVf. V-. wI...
copyright. on M
arch 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.456.567 on 1 O
ctober 1963. Dow
nloaded from

568 POSTGRADUATE MEDICAL JOURNAL October I963
400 PLACED
300
24C
20C
RESPIRATORY.
NOV DEC JAN FEB MAR APR.
FIG. 2.-Bed Bureau cases (see text).
Since in some cases one serum only wasobtained, and since most cases were admitted7-I4 days after onset, it was not always practicableto use a fourfold rise in titre as a criterion ofinfection. The criterion of Stuart Harris (I953)was accepted, that a titre of i :I6 or more in a
single specimen was an index of recent infection.After January 31, 196I, the number of admis-
sions and the severity of the respiratory illnessesdeclined, and of the sera studied from I5 patientsadmitted after that date I3 were negative and 2gave a positive complement fixation at a titre ofi:I6 only. This confirmed the clinical impressionthat the epidemic had largely disappeared by theend of January. If these i 5 negative or low titresera from patients admitted after January 31are excluded, from the remaining 75 sera comple-ment fixation titres with influenza A solubleantigen of i: i6 or more were obtained in 52 (69%).Stuart Harris (I953) reported positive complementfixation studies in 70% of hospital admissionsfor complicated influenza in the Influenza Aiepidemic of 195I, and Clarke, Heath, Sutton,and Stuart-Harris (1958) reported similar findingsin 74% in the I957 epidemic of Influenza A2.The approximation of the present figures suggeststhat the great majority of these cases here reportedwere in fact due to influenza A2. This conclusionis confirmed by the finding of high complementfixation titres only during the epidemic period(Table i). The distribution of complement fixa-tion titres in relation to age appears in Table 2.
Clinical StudiesThe diagnoses of patients in which serum
studies were obtained are classified in Table 3 andunder these classifications the principal clinicalfeatures are considered.
TABLE I
WEEKLY COMPLEMENT FIXATION TITRES RELATED TO NUMBERS OF EMERGENCY ADMISSIONS
Dec. Dec. Dec. Dec. Jan. Jan. Jan. Jan. Feb. Feb.Week Ending: Io I7 24 31I 7 14 21 28 4 II
Titre reciprocal:32 and above .. .. - - 2 IO 8 9 2 6Below 32 .. .. - - I 8 8 IO 3 8 9 6
Cases placedby Bed Bureau 26o 3I9 377 487 435 406 396 377 347 332Respiratory cases, Bed
Bureau .. .. .. 79 96 153 245 200 173 141 134 88 85
TABLE 2
COMPLEMENT FIXATION STUDIES-AGE DISTRIBUTION
10-19 20-29 30-39 40-49 50-59 6o-69 70-79 8o+
128 - 2 - 2 7 6 5 264 - - - 3 I 232 --I-I3 216 - I I 2 I 7 2 I8 . - 2 2- 2 - 20 I - 2 3 7 I0 6 2
copyright. on M
arch 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.456.567 on 1 O
ctober 1963. Dow
nloaded from

October I963 HEARN: Influeniza in Hospital I960-I96I 569
TABLE 3
DIAGNOSES OF CASES CHECKED BY COMPLEMENTFIXATION, 1960-6I
Male Female Total
Bronchitis and broncho-pneumonia 34 21 55
Staphylococcal infection 5 I 6Tuberculosis .. .. 5 o 5Gastroduodenal hemor-
rhage . .. .. 5 o 5Klebsiella infection . . OMiscellaneous .. 3 0 3
53 22 75
TABLE 4
COMPLEMENT FIXATION STUDIES IN BRONCHITISAND BRONCHOPNEUMONIA, I960-6I
C.F. Reciprocal Male Female Total
I28 .. .. 8 864 .. .. 4 I 532 .. .. 3 I 4i6 .. .. 8 3 II8.. .. I 2 30 .. .. 8 6 I4
Total .. 34 21 55
i6 and above=38 (70%)
Bronchitis and BronchopneumoniaThis diagnostic category included 55 patients,
34 males and 2I females; Table 4 records the titrereciprocals, a titre of i :I6 or more being obtainedin 70%. Table 5 indicates the age distribution bysexes and notes the deaths and the frequency ofprevious respiratory disease in the history.The notable features are the concentration of
cases among the more elderly, the restriction ofmortality to those over 6o years, and the frequencyin all age groups of previous respiratory disease.The clinical features were those previously
described as occurring in influenza A (Stuart-
Harris, 1953) and no detailed analysis is necessaryhere. Most, but not all, patients gave a history ofan influenzal illness at onset with cough, malaise,headache and aching in the limbs. Substernalpain on coughing was frequent, and in a smallernumber of patients vomiting occurred during thefirst two days of the disease. Admissions occurredfrom 3 to 2o days after onset and were usually theresult of continuation or relapse of fever, andprogressive respiratory deficiency. The clinicalappearances on admission were usually those ofacute obstructive lung disease due to bronchiolitisor bronchopneumonia; the contribution to thisappearance made by pre-existing chronic obstruc-tive lung disease was sometimes over-estimatedduring the acute stage. Most patients werefebrile on admission. Cyanosis was frequent andoften gross. Congestive failure due to corpulmonale or auricular fibrillation was observedand acute confusional states were a common finalcause of admission.The classical distinction as between influenzal
and post-influenzal was frequently difficult, andit is doubtful whether this distinction serves anyuseful purpose. In some patients the historysuggested a biphasic disease.The distinction between bronchitis, bronchio-
litis and bronchopneumonia could not be clearlymade. Even in those patients showing extensiveradiological changes there was rarely any altera-tion in breath sounds. Bilateral diffuse rales wereso frequent as to be the principal diagnosticfeature.
It is not the purpose of this paper to discusstreatment but it is worthy of note that tracheo-stomy was employed in two patients only, bothof whom died.
Staphylococcal InfectionComplement fixation studies were carried out
in 6 patients in whom staphylococcal infection
TABLE 5BRONCHITIS AND BRONCHOPNEUMONIA-AGE DISTRIBUTION
Male FemaleAge
Groups Previous PreviousTotal Chronic Previous Died Total Chronic Previous DiedCases Bronchitis Asthma Cases Bronchitis Asthma
20-29I-I 0 ----30-39 - - I 0 I I - 040-49 4 2 - 0 2 I - 050-59 9 7 - 0 2 I - 06o-69 9 7 -3 8 5 - 270-79 7 3 - 2 5 3 - I8o 4 2 -2 3 - - I
Total 34 21 (6o%) I 7 (20%) 21 II (55%) 4 (20%)
copyright. on M
arch 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.456.567 on 1 O
ctober 1963. Dow
nloaded from

570 POSTGRADUATE MEDICAL JOURNAL October I963
TABLE 6STAPHYLOCOCCAL INFECTIONS DURING INFLUENZA EPIDEMIC
C.F. DurationCase Age Diagnosis Titre of Stay Result
(Days)
I. D. B. 82 Fulminating pneumonia N.T. I Died2. J. M. 36 N.T. 43. L. D. 15 0 I4. J. M. Lung abscess o 6i5. F. T. 64 Pneumonia I28 35 Recovered6. R. D. 26 ,I28 I47. G. . 48 N.T. 278. G. B. 58 ,I28 219. B. G. 25 Staphylococcal plastic bronchitis I28 32 "
TABLE 7
TUBERCULOSIS DURING INFLUENZA EPIDEMIC
DurationCase Age Diagnosis C.F. of Stay Result
Titre (Days)
I. J. J. 73 Tub. bronchopneumonia (autopsy) 64 25 Died2. A. A. 59 Tub. bronchopneumonia (positive sputum) o 32 Transferred3. G. H. 69 Tub. bronchopneumonia (positive sputum) 64 294. H. A.(P) 45 Chronic pulmonary Tub. (radiological) 64 I45. E. P. 69 Chronic pulmonary Tub. (radiological) 32 21 ,,
was the proved or presumed cause of respiratorycomplication of influenza. Three other patientswith proved or presumed staphylococcal infectionfrom whom no sera were obtained were includedin the study. Details of these 9 patients areclassified in Table 6.There were three male patients with fulminating
pneumonia, aged 82, 36 and IS years respectively.In only one of these was there a history of previousrespiratory disease. Each patient was admittedwithin 48 hours of onset; one patient died on theday of admission and two survived 3 days. In onlyone of these three cases did the relatives permitautopsy, which revealed the classical appearancesof staphylococcal bronchopneumonia complicatinginfluenza. Hxmorrhages had occurred into bothadrenal glands. A widely sensitive staphylococcuspyogenes was cultured from the lung, and influenzaA2 virus was cultured from the tracheal mucosaand from the lung. The remaining two fulmina-ting cases were so similar that the diagnosesseemed beyond reasonable doubt although neithersputum nor serum was studied. Early admissionafter onset, cyanosis, respiratory distress andhypotension were the diagnostic features. Ineach ease it seemed certain that the infection wasacquired before admission.The illness of the patient dying of staphylococcal
lung abcess was almost certainly influenzal inorigin owing to the mode of onset and coincidence
in time, although no C.F. antibody was presentin the serum. He was admitted with a broncho-pneumonia of the right upper lobe which shortlybecame confluent, cavitated, yielded Staph.pyogenes and apparently healed with prolongedantibiotic therapy. At the end of the sixth weekthe patient was ready for discharge when hisfever recurred and an abscess appeared at theleft apex; this seemed to be responding to anti-biotic therapy when the abscess ruptured andcaused death by flooding the bronchial tree withpus.The sole female patient presented with a
staphylococcal plastic bronchitis, a complementfixation titre of I :128 being obtained. A knownasthmatic, she presented during the seventh monthof pregnancy not with asthma but with a severehyperpncea causing respiratory alkalosis, the causebeing obscure until a reflex origin was indicatedby the development of obstructive stridor.Tracheostomy by Mr. D. Lloyd Davies revealeda cast the size of a small finger lying below thevocal cords; its removal was followed by theevacuation of 50 ml. of staphylococcal pus. Thecast was composed of fibrin and Staph. pyogenes.During the next- two weeks io similar casts wereremoved by bronchoscopy through the tracheo-stomy orifice. At no time were radiologicalchanges observed. The patient finally made acomplete recovery, was delivered at term of a
copyright. on M
arch 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.456.567 on 1 O
ctober 1963. Dow
nloaded from
October I963 HEARN: Influenza in Hospital I960-I96I 571
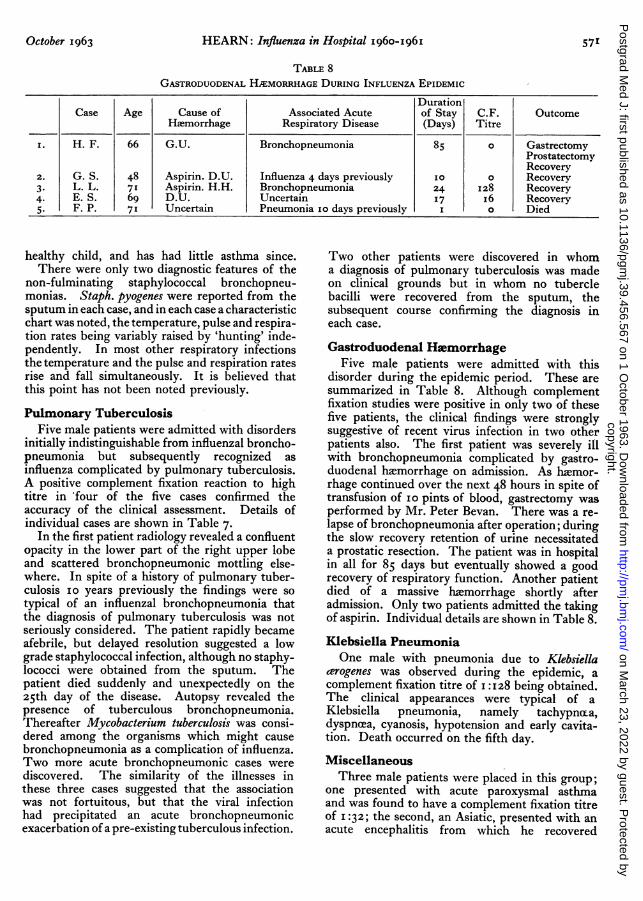
TABLE 8GASTRODUODENAL HIEMORRHAGE DURING INFLUENZA EPIDEMIC
DurationCase Age Cause of Associated Acute of Stay C.F. Outcome
Hlemorrhage Respiratory Disease (Days) Titre
I. H. F. 66 G.U. Bronchopneumonia 85 o GastrectomyProstatectomyRecovery
2. G. S. 48 Aspirin. D.U. Influenza 4 days previously 10 0 Recovery3. L. L. 71 Aspirin. H.H. Bronchopneumonia 24 I28 Recovery4. E. S. 69 D.U. Uncertain 17 i6 Recovery5. F. P. 71 Uncertain Pneumonia IO days previously I O Died
healthy child, and has had little asthma since.There were only two diagnostic features of the
non-fulminating staphylococcal bronchopneu-monias. Staph. pyogenes were reported from thesputum in each case, and in each case a characteristicchart was noted, the temperature, pulse and respira-tion rates being variably raised by 'hunting' inde-pendently. In most other respiratory infectionsthe temperature and the pulse and respiration ratesrise and fall simultaneously. It is believed thatthis point has not been noted previously.
Pulmonary TuberculosisFive male patients were admitted with disorders
initially indistinguishable from influenzal broncho-pneumonia but subsequently recognized asinfluenza complicated by pulmonary tuberculosis.A positive complement fixation reaction to hightitre in *four of the five cases confirmed theaccuracy of the clinical assessment. Details ofindividual cases are shown in Table 7.
In the first patient radiology revealed a confluentopacity in the lower part of the right upper lobeand scattered bronchopneumonic mottling else-where. In spite of a history of pulmonary tuber-culosis io years previously the findings were sotypical of an influenzal bronchopneumonia thatthe diagnosis of pulmonary tuberculosis was notseriously considered. The patient rapidly becameafebrile, but delayed resolution suggested a lowgrade staphylococcal infection, although no staphy-lococci were obtained from the sputum. Thepatient died suddenly and unexpectedly on the25th day of the disease. Autopsy revealed thepresence of tuberculous bronchopneumonia.Thereafter Mycobacterium tuberculosis was consi-dered among the organisms which might causebronchopneumonia as a complication of influenza.Two more acute bronchopneumonic cases werediscovered. The similarity of the illnesses inthese three cases suggested that the associationwas not fortuitous, but that the viral infectionhad precipitated an acute bronchopneumonicexacerbation of a pre-existing tuberculous infection.
Two other patients were discovered in whoma diagnosis of pulmonary tuberculosis was madeon clinical grounds but in whom no tuberclebacilli were recovered from the sputum, thesubsequent course confirming the diagnosis ineach case.
Gastroduodenal HmemorrhageFive male patients were admitted with this
disorder during the epidemic period. These aresummarized in Table 8. Although complementfixation studies were positive in only two of thesefive patients, the clinical findings were stronglysuggestive of recent virus infection in two otherpatients also. The first patient was severely illwith bronchopneumonia complicated by gastro-duodenal haemorrhage on admission. As haemor-rhage continued over the next 48 hours in spite oftransfusion of io pints of blood, gastrectomy wasperformed by Mr. Peter Bevan. There was a re-lapse of bronchopneumonia after operation; duringthe slow recovery retention of urine necessitateda prostatic resection. The patient was in hospitalin all for 85 days but eventually showed a goodrecovery of respiratory function. Another patientdied of a massive hlimorrhage shortly afteradmission. Only two patients admitted the takingof aspirin. Individual details are shown in Table 8.
Klebsiella PneumoniaOne male with pneumonia due to Klebsiella
cerogenes was observed during the epidemic, acomplement fixation titre of I:I28 being obtained.The clinical appearances were typical of aKlebsiella pneumonia, namely tachypnt-a,dyspncea, cyanosis, hypotension and early cavita-tion. Death occurred on the fifth day.
MiscellaneousThree male patients were placed in this group;
one presented with acute paroxysmal asthmaand was found to have a complement fixation titreof I :32; the second, an Asiatic, presented with anacute encephalitis from which he recovered
copyright. on M
arch 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.456.567 on 1 O
ctober 1963. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
spontaneously, complement fixation titre beingi:i6; the third, also an Asiatic, presented with asevere herpes febrilis affecting the upper and lowerlids of both eyes, complement fixation titre beingi :i6.
ConclusionsThis study demonstrated that during the winter
of i960/6I the 'winter load' was due to acuterespiratory disorders occurring as complicationsof influenza A (Asian). The range of these compli-cations was wider than had been anticipated andtheir severity considerable.The most frequent complications were bron-
chitis and bronchopneumonia. These disordersoccurred only in older age groups and usuallyin those with previous respiratory disease. Deathoccurred in 20% of patients of each sex and onlyin those of 6o years or more. Apart from thefrequent finding of widespread rales and theresults of virological study there was nothing todistinguish these patients from those commonlyadmitted in winter regarded as suffering fromexacerbation of chronic obstructive lung diseasedue to chronic asthma and/or bronchitis.The next most frequent complication was
staphylococcal infection. Eight males wereobserved with influenzal staphylococcal pneumoniaof whom 4 died (50%). One female was admittedsuffering from influenzal staphylococcal plasticbronchitis, occurring during the seventh monthof pregnancy; mother and foetus survived. Thesecomplications were observed scattered throughoutall age groups and often in those without previousrespiratory disease.The predominant feature of the three fatal
cases presenting as fulminating influenzal staphy-lococcal pneumonia (i proved, 2 clinical) washypotension due to acute circulatory insufficiency.This was the cause of rapid death which was notprevented by energetic antibiotic and steroidtherapy, but which was partly explained by thefinding of bilateral adrenal biemorrhage in theonly fulminating case submitted to autopsy.Hers (I955) had already reported adrenal hlimor-rhages in all of seven cases of influenzal staphylo-coccal pneumonia subjected to intensive post-mortem study. He noted the absence of suchhemorrhages in non-staphylococcal influenzaldeaths, concluding that the adrenal haemorrhageswere bacterio-toxic and not viro-toxic in nature.These manifestations were in fact those of theWaterhouse-Friderichsen syndrome in which thecauses for the failure of treatment are not yetfully understood. Talbot (I962) discussing'bactera,mic shock' occurring in infections dueto gram-negative bacilli noted the good resultsthat followed immediate therapy with an anti-
biotic to which the organism was sensitive. Instaphylococcal 'bacteremic shock' the same successwas not apparent with the three cases reportedhere or in other series; and the failure was certainlynot due to the resistance of the staphylococci toantibiotics. In one single fulminating case inwhich autopsy study was permitted a fully sensi-tive staphylococcus was recovered. In the sevencases reported by Hers (1955) and quoted above,strains of fully sensitive staphylococci wererecovered from six. This finding was confirmedby Robertson, Caley and Moor, (1958), whorecovered sensitive staphylococci from I2 of I4patients with fulminating influenzal staphy-lococcal pneumonia dying within seven days ofonset.
It is necessary to consider whether any of theseinfections were due to hospital cross-infection.In the three fatal fulminating cases the severityof the illnesses on admission, the early deaths andthe finding of a fully sensitive staphylococcus inthe one case where an organism was recovered, allsuggest that infection occurred before admission.Of the six non-fulminating cases, fully sensitivestaphylococci were recovered from three on thesecond day of admission and from one on thesixth day. In seven of nine cases, therefore, thereare grounds for concluding that infection wasacquired before admission. In the remainingtwo patients cross-infection cannot be excluded;in one who survived, a strain of Staph. pyogeneswas recovered on the ninth day, sensitive tochloramphenicol and novobiocin only; in the other,who succumbed from the rupture of a staphy-lococcal lung abscess, a strain of Staph. pyogenesinsensitive to penicillin, tetraycline and erythro-mycin was obtained. The high mortality, thesensitivity of many of the staphylococci and theevidence in favour of the acquisition of infectionbefore admission have been reported previously.Robertson and others (1958) noted the highmortality (47%) in patients affected with staphy-lococcal infections in the influenza A2 epidemicof I957 in Sheffield, and observed that this appliedequally to those patients with sensitive strainsacquired before admission, and to those withinsensitive strains, not all of which were clearlyacquired after admission.The finding of 3 proved and 2 clinical cases
of pulmonary tuberculosis complicating influenzawas disturbing. In the first case the sputum wasnot examined for tubercle bacilli as pulmonarytuberculosis was not suspected; the diagnosis wasmade at autopsy. In the second case tuberclebacilli were noted only after sputum culture andby the time this was reported the patient was soill as to appear moribund, although in fact a slowrecovery followed the institution of specific
October I963572copyright.
on March 23, 2022 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.39.456.567 on 1 October 1963. D
ownloaded from

October I 963 HEARN: Influenza in Hospital 1960-I96I 573
therapy. This diagnosis would not have beenmade without the experience provided by thefirst case. In the two clincial cases radiologyrevealed bilateral apical opacities typical ofpulmonary tuberculosis of low grade activity. Thevirus infection had apparently done no more thanprovide a reason for the radiology that revealedthe presence of tuberculous lesions. But in thethree other cases an acute tuberculous broncho-pneumonia was present which appeared to havebeen aggravated by the viral infection. In thesepatients the clinical and radiological appearanceswere indistinguishable from those of influenzalstaphylococcal bronchopneumonia although thecharacteristic temperature chart of the lattercondition was lacking. This difficulty in distin-guishing between pyogenic and tuberculousbronchopneumonia complicating influenza wasnoted by Rich (I944) who, discussed the possiblerelationship between influenza and exacerbationof tuberculosis without reaching any conclusion.Certainly in the 'five cases reported here positiveevidence of influenza was present in four and theobservation of three cases of bronchopneumonictuberculosis during the course of the epidemic
strongly suggested a relationship, since it hadbecome exceptional by I960 to observe threesuch cases in so short a period.The finding of preceding respiratory infection
in four of five patients with gastroduodenal himor-rhage, with C.F. studies positive in two of these,is of importance not only in relation to aspirintherapy, which was a final cause of lxmorrhage intwo cases and a possible cause in two others, butthe preceding respiratory infection is a severehazard if gastrectomy proves necessary, as it didin one case reported here.
Finally, it is noteworthy that with the exceptionof 20 cases of influenzal bronchitis and broncho-pneumonia and one case of stapylococcal bron-chitis, all the complicated cases occurred in males.This suggests that a study of the smoking habitsof patients admitted for complications of influenzain future epidemics would be desirable.
I am indebted to Dr. T. H. Flewett for his meticulous-virological studies and for his critical advice; to Dr.W. D. Foster for his bacteriological studies; to Dr.I. S. Buchanan for his permission to include some ofhis cases in this study, and to my house physicians andward sisters, whose enthusiastic collaboration made thisstudy possible.
REFERENCESCLARKE, S. K. R., HEATH, R. B., SUTTON, R. N. P., and STUART-HARRIS, C. H. (1958): Serological Studies with Asian
Strain of Influenza A, Lancet, i, 814.HERS, J. F. PH. (1955): 'Histopathology of the Respiratory Tract in Human Influenza'. Leiden: H. E. Stenfert
Kroese N.V.RICH, A. R. (1944): 'Pathogenesis of Tuberculosis'. Springfield, Illinois: Charles C Thomas.ROBERTSON, L., CALEY, J. P., and MOORE, J. (1958): Importance of Staphylococcus aureus in Pneumonia in the 1957
Epidemics of Influenza A, Lancet, ii, 233.STUART-HARRIS, C. H. (1953): 'Influenza and other Infections of the Respiratory Tract'. London: Edward Arnold.TALBOT, C. H. (I962): Szpticomia Due to Gram Negative Bacilli, Lancet, i, 668.
copyright. on M
arch 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.39.456.567 on 1 O
ctober 1963. Dow
nloaded from