inferior aponeurosis tucking revisited
TRANSCRIPT
Inferior Aponeurosis Tucking Revisited JAMES LEONARD HARGISS, MD
Abstract: In a retrospective study of 134 cases of senile entropion treated by inferior aponeurosis tucking, the recurrence rate was lower with tucking to pretarsal fascia than with tucking to the inferior tarsal edge, and there were no recurrences in 58 cases with tucking plus orbicularis-to-aponeurosis "barrier" sutures. [Key words: barrier suture, inferior aponeurosis, pretarsal fascia, senile entropion.] Ophthalmology 87:1001-1004, 1980
In 1973, when this investigator compared 50 cases of orbital septum tucking followed for seven years with 47 cases of inferior aponeurosis tucking for senile entropion followed for three and one-half years, no recurrences were found in the latter group. 1 Subsequently, with 16 months' to eight years' follow-up, there have been recurrences in three of the original 47 and five of 87 subsequent cases treated by inferior aponeurosis tucking, for a total recurrence rate of six percent.
Though this rate is less than reported recurrences by other methods, it is greater than that of Schaefer's report,2 which compiled his and my figures as well as those of Wobig, Reeh, and others for inferior aponeurosis tucking. This study is an attempt to determine factors that may contribute to recurrence of entropion treated by this operation.
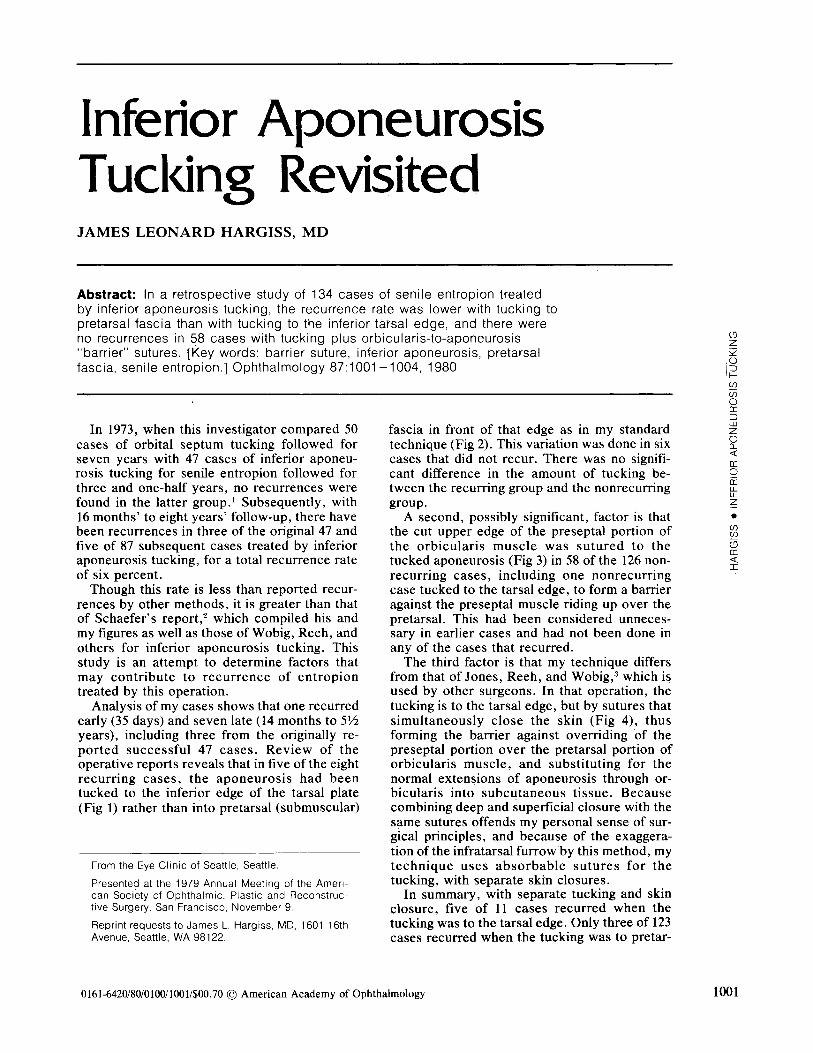
Analysis of my cases shows that one recurred early (35 days) and seven late (14 months to 5Y2 years), including three from the originally reported successful 47 cases. Review of the operative reports reveals that in five of the eight recurring cases, the aponeurosis had been tucked to the inferior edge of the tarsal plate (Fig 1) rather than into pretarsal (submuscular)
From the Eye Clinic of Seattle, Seattle.
Presented at the 1979 Annual Meeting of the American Society of Ophthalmic, Plastic and Reconstructive Surgery, San Francisco, November 9.
Reprint requests to James L. Hargiss, MD, 1601 16th Avenue, Seattle, WA 98122.
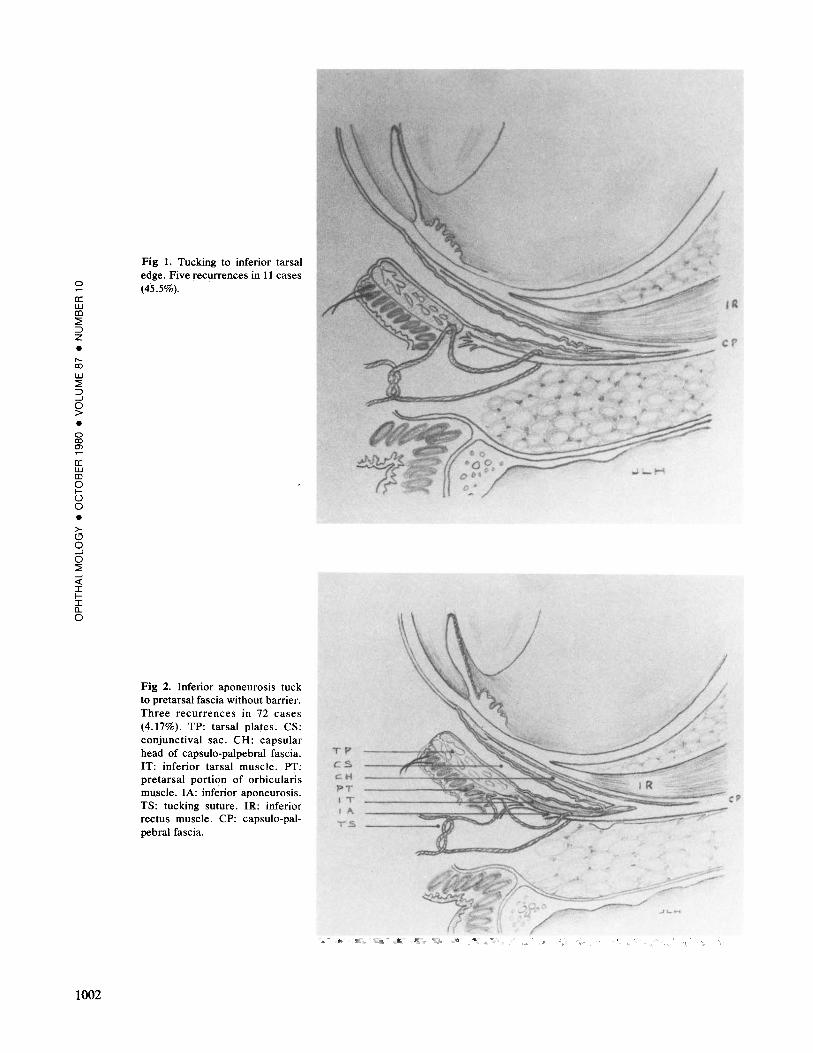
fascia in front of that edge as in my standard technique (Fig 2). This variation was done in six cases that did not recur. There was no significant difference in the amount of tucking between the recurring group and the nonrecurring group.
A second, possibly significant, factor is that the cut upper edge of the preseptal portion of the orbicularis muscle was sutured to the tucked aponeurosis (Fig 3) in 58 of the 126 nonrecurring cases, including one nonrecurring case tucked to the tarsal edge, to form a barrier against the preseptal muscle riding up over the pretarsal. This had been considered unnecessary in earlier cases and had not been done in any of the cases that recurred.
The third factor is that my technique differs from that of Jones, Reeh, and Wobig,3 which is used by other surgeons. In that operation, the tucking is to the tarsal edge, but by sutures that simultaneously close the skin (Fig 4), thus forming the barrier against overriding of the preseptal portion over the pretarsal portion of orbicularis muscle, and substituting for the normal extensions of aponeurosis through orbicularis into subcutaneous tissue. Because combining deep and superficial closure with the same sutures offends my personal sense of surgical principles, and because of the exaggeration of the infratarsal furrow by this method, my technique uses absorbable sutures for the tucking, with separate skin closures.
In summary, with separate tucking and skin closure, five of 11 cases recurred when the tucking was to the tarsal edge. Only three of 123 cases recurred when the tucking was to pretar-
0161-6420/80/0100/10011$00.70 ©American Academy of Ophthalmology
~ z ~ .u I~ (f)
U5 0 a: :J w z 0 Q_ <(
a: 0 a: w u.. z • (f)
SQ ~ a: <( I
1001
0
a: UJ co :2 ::J z • ,...._ 00
UJ :2 ::J ....1
§2 • 0
~ a: UJ co 0 f() 0
• >CJ 0 ....1 0 :2 ....1 <( I fI [l_
0
1002
Fig 1. Tucking to inferior tarsal edge. Five recurrences in 11 cases (45.5%).
Fig 2. Inferior aponeurosis tuck to pretarsal fascia without barrier. Three recurrences in 72 cases (4.17%). TP: tarsal plates. CS: conjunctival sac. CH: capsular head of capsulo-palpebral fascia. IT: inferior tarsal muscle. PT: pretarsal portion of orbicularis muscle. lA: inferior aponeurosis. TS: tucking suture. IE.: inferior rectus muscle. CP: capsulo-palpebral fascia.
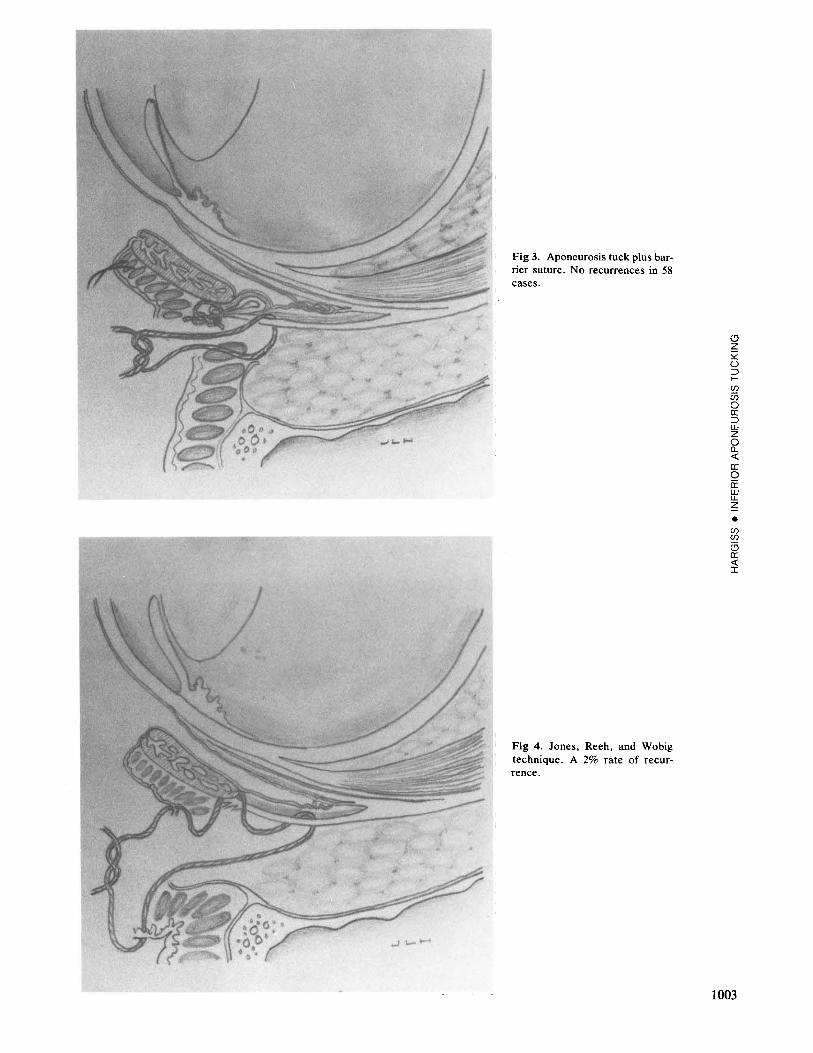
Fig 3. Aponeurosis tuck plus barrier suture. No recurrences in 58 cases.
Fig 4. Jones, Reeh, and Wobig technique. A 2% rate of recurrence.
<.9 z ~ 0 ::J ~ (/)
ii5 0 a: ::J UJ z 0 a.. <(
a: 0 a: UJ lL z
• (/) (/)
(3 a: <( I
1003

0
a: w Ill 2 => z • ,..__ co w 2 => ___!
0 > • 0 co 0)
a: w Ill 0 fu 0
• >(9 0 ___!
0 2 ___! <( I fI (L
0
1004
sal fascia. There were no recurrences in 58 cases in which the barrier against override was established by suturing orbicularis to the tucked aponeurosis, including one where the tucking was to the tarsal edge. When the tucking is to the lower edge, the recurrence rate is lower if an orbicularis barrier is established either by incorporating skin closure with the tucking sutures or by suturing orbicularis to the tucked aponeurosis. My present technique includes tucking to the pretarsal fascia rather than to the tarsal edge and suturing orbicularis to the tucked aponeurosis, both with absorbable su-
tures, and separate skin closure with running intradermal suture.
REFERENCES
1. Hargiss JL. Inferior aponeurosis vs. orbital septum tucking for senile entropion. Arch Ophthalmol 1 973; 89:210-3.
2. Schaefer AJ. (Abstract) statistical summary: senile entropion surgery. Ophthalmic Surg 1977; 8(2):125-6.
3. Jones LT, Reeh MJ, Wobig JL. Senile entropion: a new concept for correction. Am J Ophthalmol 1972; 74:327-9.