infection-related inferior alveolar and mental nerve paresthesia
TRANSCRIPT

Pathology
Infection-related inferior alveolar and mental nerveparesthesia: Case reportsHasan Yeler, DDS PhD'/llkerOzeç, DDS, PfiD^/Erdem Kiliç, DDS^
Nerve injury can be related to mechanical, chemical, and thermal factors. Infection-related paresthesia isusually related to mechanical pressure and ischemia associated with ttie inflammatory process. Anothercause of paresthesia could be the toxic metabolic products of bactena or inflammatory products releasedfollowing tissue damage. This article presents cases of inferior alveolar and mental nerve paresthesiacaused by an infected impacted tooth, an infected cyst, and periapioal infection.The possible pathophyslo-logic mechanism of netve injury, therapy, and prognosis for recovery are also discussed (QuintessenceInt 2004:35:313-316)
Key words: bacteria culture, infection, inferior alveolar nerve, mental nerve, neurapraxia, parestfiesia
Paresthesia is defined as a burning or prickling sen-sation or partial numhness caused by neural injury.
Paresthesia in dentistry can be caused by local or sys-temic factors. Local factors include tratamatic injuries,expanding compressive lesions, impacted teeth, localinfections, iatrogenic factors, or implantology.'-*
Mechanical, chemical, and thermal factors are in-cluded as possible mechanisms of neural injury-Mechanical damage includes compression, stretching,partial or total resection, and laceration. Compression,eventuating inneurai ischemia, might be external andcan be caused by postextraction or postsurgery bemor-rhage. edema, hematoma formation, neoplasia. cysts,implants, or overfilling of endodontic material.Compression also might be internal caused by intra-neural edema.̂ ^
'Assistant Professor, Cumhuriyet University. Dental School. Department o(
Oral and Maxjilofacial Surgery. Sivas, Turkey
'Research Assistant. Cumhunyet University. Dental Sctiool, Department ofOral and Maxillofaciai Surgery, Sivas, Turkey
pr int requests: Ilker Ôzeç, Cumhuriyet fjniversitesi.kultesi. ADÇH ve Cerrahisi A8D, Sivas. Turkey E-
ReFakcumhuriyet.edu.t
Infection-related paresthesia is usually related tomechanical pressure and Ischemia associated with theinfiarmnatory process (edema) or is caused by localpressure to the mental nerve, consequent to the accu-mulation of purulent exúdate in the mandibular bone.Another cause oí paresthesia could be the toxic meta-bolic products of bacteria or Inflammatory productsreleased following tissue damage.'-
Paresthesia of the inferior alveolar nerve is quiterare because of the unique anatomy of this nerve. Inthis article, three cases of paresthesia related to infec-tion are reported.
CASE1
A 22-year-old woman was referred to the Departmentof Orai and Maxiilofacial Surgery, Dental School.Cumhuriyet University, Turkey. Her chief complaintwas pain, swelling, and loss of sensitivity with burningsensation (which was disappearing with the use of an-tihiotics} on the left side of the mandible and lip.which had been present during the previous 4 months.The patient's general condition was good. She re-ported that she was not taking any medications.
Quintessence International 313

• Yeler et al
Fig 1 Tfiird molar tooth in close conlacimandibular canal.
Fig 2 Radicular cyst in close contact with the mentalforamen
Intraoral examination showed a swelling in thevestibular fornix. Fxamination of the dentition showedthe clinical absence of the left third mandibular molar.Testing with a dental probe showed numbness of thebuccal gingiva on the left side of the mandible.Panoramic radiographie examination confirmed thatthe left mandibular third molar tooth was impactedand in elose proximity to the inferior alveolar canal(Fig 1).
The tooth was extracted under local anesthesia. Allremnants of the dentai follicle were removed, the ex-traction site was thoroughly irrigated with saline solu-tion, and primary closure was achieved with 3-0 silksutures. The patient was given a prescription for anantibiotic (ampicillin/sulbacfam 375 mg, 1 tablet 2times daily) and analgesic.
During the operation, tissue samples were obtainedfrom the socket by means of a steriie cotton swab andsent for bacterial culture and sensitivity studies. Thebacterial culture revealed anaerobic gram-positivecocci with sensitivity to ampicillin/sulbactam.
The patient was seen again the foilowing day. Therehad already been a significant reduction in pain, how-ever, the patient was still complaining of numbness.One week later, a recall examination showed that thepatient was asymptomatic, and sensation in the buccal
gingiva had begun to return to normal. At 2 weeks fol-lowing the initial treatment, the patient was asympto-matic and the burning sensation had resolved.
CASE 2
A 42-year-old woman was referred because of severepain and swelling of the left side of the mandible. Thepatient's general condition was not good, and general-ized malaise was present. On extraoral examination,there was asymmetry and tender swelling. The cervicalnodes were not palpable. Examination of the dentitionshowed many carious lesions and many edentulousareas. Panoramic radiographie evaluation revealed alarge, well-defined, unilocular radiolucency surroutid-ing the roots of the left mandibular canine and premo-lars. Radiograpbs disclosed deep carious involvementof the mandibular left premolars. The mental foramenappeared in close proximity to the periapical radiolu-cent area (Fig 2).
There was an area of paresthesia relating exactly tothe distribution of the left mental nerve. Testing with adental probe showed numbness of the labial gingivaon the left side of the mandible and of the left half ofthe lower lip. Electric vitality tests indicated the right
314 Volume 35, Number 4, 2004
• Yeler et al
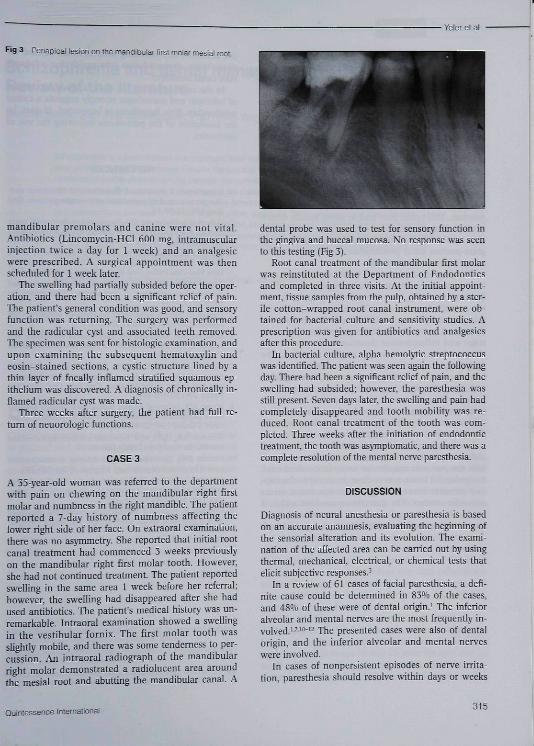
Fig 3 Periapical iesion on the mandibular first molar mesial root.
mandibular premolars and canine were not vital.Antibiotics (Lincomycin-HCl 600 mg. intramuscularinjection twice a day for 1 week) and an analgesicwere prescribed. A surgical appointment was tbenscbeduled for 1 week later.
The swelling had partially subsided before tbe oper-ation, and there bad been a significant relief of pain.Tbe patient's general condition was good, and sensoryfunction was returning. Tbe surgery was performedand tbe radictilar cyst and associated teetb removed.Tbc specimen was sent for bistologic examination, andupon examining tbe subsequent hematoxylin andeosin-stained sections, a cystic structure lined by athin layer of focally inflamed stratified squamous ep-ithelium was discovered. A diagnosis of chronically in-fiamed radicular cyst was made.
Three weeks after surgery, the patient had fuU re-turn of neuorologic functions.
CASE 3
A 35-year-old woman was referred to tbe departmentwith pain on chewing on the mandibular rigbt firstmolar and numbness in tbe right mandible. Tbe patientreported a 7-day history of numbness affecting thelower rigbt side of her face. On extraoral examination,there was no asymmetry. She reported that initial rootcanal treatment had commenced 3 weeks previouslyon the mandibular right first molar tooth. However,she had not continued treatment Tbe pafient reportedswelling in the same area 1 week before her referral;bowever, tbe swelling bad disappeared after sbe hadused anfibiotics. The patient's medical history was un-remarkable. Intraoral examination showed a swellingin the vestibular fornix. The first molar tooth wassfigbtly mobile, and there was some tenderness to per-cussion. An intraoral radiograph of the mandibularright molar demonstrated a radiolucent area aroundtbe mesial root and abutfing the mandibular canal. A
dental probe was used fo test for sensory fimction inthe gingiva and buccal mucosa. No response was seento tbis testing (Fig 3).
Root canal treatment of tbe mandibular first molarwas reinstituted at tbe Department of Endodonticsand completed in three visits. At tbe initial appoint-ment, tissue samples from the pulp, obtained hy a ster-ile cotton-WTapped root canal instrument, were ob-tained for bacterial eulture and sensitivity studies. Aprescription was given for antibiotics and analgesicsafter tbis procedure.
In bacterial culture, alpha hemolyfic streptococcuswas identified. Tbe patient was seen again the followingday. There had been a significant relief of pain, and tbeswelling had subsided: however, the paresthesia wasstill present. Seven days later, the swelling and pain badcompletely disappeared and tooth mobility was re-duced. Root canal treatment of the tootb was com-pleted. Tbree weeks after the initiafion of endodonfietreatment, tbe tootb was asjTrtptomafic, and there was acomplete resolution of the mental nerve parestbesia.
DISCUSSION
Diagnosis of netiral anestbesia or paresthesia is basedon an accurate anamnesis, evaluating the begirming oftbe sensorial alterafion and its evolution. The exami-nation of the affected area can he carried out by usingthermal, mechanical, electrical, or chemical tests thatelicit subjecdve responses.^
In a review of 61 cases of facial paresthesia, a defi-nite cause could be determined in 83<i'o of the cases,and 48'*o of these were of dental origin.' Tbe inferioralveolar and mental nerves are the most frequently in-volved.'-'"-^- "Ilie presented cases were also of dentalorigin, and tbe inferior alveolar and mental nerveswere involved.
In cases of nonpersistent episodes of nerve irrita-tion, paresthesia should resolve within days or weeks
Quintessence Internationai 315

• Yeler et ai
as the cause is removed. Infection-related paresthesiasubsides after infection, and inflammation resolvesthrough antibiotic therapy, endodontie treatment, pe-riapical surgery, or looth extraction,'
The paresthesia in the first case was likely causedby several factors. One is mechanical pressure. Theexpanding infectious process and the associated hostinflammatory process (edema) may cause pressure onthe nerve fibers that is severe enough tc induce thesymptoms of paresthesia. A second factor is related tomicrobial products. Certain microbes, such as gram-negative bacteria, have been involved in the produc-tion of neuropathies. It has been hypothesized thatmicrobial products can breach the protective peri-neurium. This could then lead to nerve bundle deteri-oration. Tissue metabolism in the region of the infec-tion could impair neural conduction. Anaerobicgram-positive cocci proliferation were found on bac-terial culture in the first case.
The paresthesia described in the second case mayhave been caused by the effects of pressure and in-flammation arising from the pathosis associated withthe mandibular premolars. The area associated withthis paresthesia was consistent with involvement ofthe mental nerve. As the lesion passed from the acutestage and inflammation decreased, the paresthesiachanged from numbness to a tingling sensation. Thetemporary interruption of neural conduction withoutloss of axonal continuity (neuropraxia) is compatiblewith the pathophysiology of short-term pressure phe-nomena. Paresthesia was likely secondary to a "com-pression neuropraxia" created by the infected radicu-lar cyst. Another possibility is that the inflammation inthe cyst wall also involved the nerve.
Involvement of the inferior alveolar nerve is a pos-sible complication of periapical pathosis associatedwith the posterior mandibular teeth. In the third case,the periapical lesion was in close proximity to the infe-rior alveolar nerve, though there was not a directanatomic contact. The paresthesia resolved within 2weeks after root canal treatment and antibiotic ther-apy. In this case, there is little doubt that the periapi-
cal infection and resulting inflammation caused theparesthesia: the resolution was rapid alter adequateroot canal treatrnent.
In the cases reported, the simultaneous occurrenceof infection and paresthesia strongly suggests a causalrelationship. This hypothesis is supported, in part, bythe resolution of the paresthesia following the use ofantibiotics.
REFERENCES
1. Lamhrianidis T, Molyvdas ). Paresthesia of the inferior alve-olar nerve caused hy periodontal-endodontic pathosis OralSurg 1987;63:90-92.
2. Gilhert BO, Diekerson AW. Paresthesia of the mental nerveafter an acute exacerbation of ehronic apical periodontitis, JAm Dent Assoc 1981:103:588-590.
3. Lenarda RD, Cadenaro M, Stacchi C, Paresthesia of themental nerve induced hy periapical infection. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2000;90:746-749.
4. Tuzum Mg, Paresthesia of the inferior alveolar nerve causedhy periapical pathology: A case report. Quintessence Int1989:20:153-154.
5. Ograyd JF. Mental paresthesia: An ominous symptom. Casereports. Ausl DentJ 1996 ;41:370-372.
6. Goldberg MH, Galbraith DA. Late onset of mandibular andlingual dysesthesia secondary to postextraction infection.Oral Surg 1984;58:269-271.
1. Giuhani M, Lajolo C, Deli G, Silveri C. Interior alveolarnerve paresthesia caused hy endodontie pathosis: A case re-port and review of lhe literature. Oral Surg Oral Med OralPathol 2001;92:670-674.
8. Morse DR. Infection-related mental and inferior alveolarnerve paresthesia: Literature review and presentation of twocases. J Endod 1997 ;23:457-460.
9. Ellinston NK, Hoen MM. Infectious transient dental-relatedparesthesia. Gen Dent 1996:44:66-69.
10. Antrim DD. Paresthesia of the inferior alveolar nervecaused hy periapical pathology J Endod 1978;4:220-221.
11. Barrett AP, Bucklay DJ. Selective anesthesias of peripheralhranches of the trigeminal nerve due to odontogenic infee-tion. Oral Surg 1986:62:226-228.
12. Cohenca N, Rotstein 1. Mental nerve paresthesia associatedwith a non-vital tooth. Endod Dent Traumatoi 1996;12:298-300.
316 Voiume 35, Number 4