infection prevention and control in the built environment
TRANSCRIPT
Infection Prevention and Control in the Built Environment. Page 1 of 27 Version 1.1 March 2019
Infection Prevention and Control Assurance - Standard Operating Procedure 15 (IPC SOP 15)
Infection Prevention and Control in the Built Environment
Why we have a procedure?
The Health and Social Care Act 2008: Code of Practice for the NHS for the Prevention and Control of Healthcare Associated Infections (revised January 2015) stipulates that NHS bodies must, in relation to preventing and controlling the risk of Health Care Associated Infections (HCAI), have in place appropriate core policies/procedures, including procedures for providing and maintaining a clean and appropriate environment that facilitates the prevention and control of infections. A well designed environment encourages good practice and is easier to clean and maintain. Implementation of this procedure will contribute to the achievement and compliance with the Act.
What overarching policy the procedure links to?
This procedure is supported by the Infection Prevention and Control Assurance Policy
Which services of the trust does this apply to? Where is it in operation?
Group Inpatients Community Locations
Mental Health Services all
Learning Disabilities Services all
Children and Young People Services all
Who does the procedure apply to?
This procedure applies to all members of staff (regardless of status or grade) who may be involved in the design and delivery of building and refurbishment projects (including the installation of equipment or IT installations), located on any of the sites under the management of the Trust. (The same principles apply to sites leased by the Trust to provide patient services).
All stakeholders should consider infection prevention and control from the conception of the project throughout the design phase and in the subsequent build/development.
Housekeeping managers should be kept informed/involved with refurbishments/ renovations as increased cleaning may be required. A planned cleaning programme is essential when building/refurbishment work of any nature is planned.
The Infection Prevention and Control Team (IPCT) must be involved from the earliest stages of all building, maintenance and engineering projects. It is important that infection prevention and control requirements are ‘designed in’ at the planning stages of healthcare facilities including new builds or refurbishment projects with input from the IPCT continuing through to the final stage of each project.
Infection Prevention and Control in the Built Environment. Page 2 of 27 Version 1.1 March 2019
The Infection Prevention and Control Team’s role is to help non-clinical professionals to understand the main principles of how infection is spread in the context of the built environment and considering these three aspects:
- Source
- Mode of transmission (Appendix 1)
- Susceptible recipient
These three principles should be applied at all stages of the development/refurbishment of the healthcare facility. (See below for further details)
When should the procedure be applied?
Effective prevention and control of healthcare associated infection (HCAI) must be embedded
into everyday practice and applied consistently. Crucial to this are the identification of risk and
the adoption of measures to remove or control such risks.
All staff/stakeholders have a responsibility to have an awareness of the risks associated with
renovations, repairs, structural works of premises and facilities during any demolition, design,
construction, new builds, refurbishment and planned preventative maintenance in the area in
which they work.
All precautionary measures outlined in this procedure must be complied with to protect
patients, staff, visitors and contractors during this type of activity.
Additional Information/ Associated Documents
Infection Prevention and Control Assurance Policy & associated Standard Operating Procedures Water Management Assurance Policy & associated Standard Operating Procedures
Control of Substances Hazardous to Health (COSHH) Policy
Health and Safety Policy Aims
People receiving treatment in, or visiting, hospitals can expect the services and facilities in the hospital to be maintained using the principles of good infection control, to minimise the risk of infection.
To provide guidance on the prevention of cross infection to those involved and responsible for the planning, design and maintenance of new and refurbished healthcare facilities and to provide a best practice approach to the delivery of construction projects in existing healthcare premises.
To avoid costly modification at a later stage in the projects by ensuring good infection prevention and control practice is ‘designed in’ as far as is reasonably practical.
Infection Prevention and Control in the Built Environment. Page 3 of 27 Version 1.1 March 2019
Definitions
Construction The work of making or building or putting something together
Environment The totality of the patient’s surroundings including the fabric of the building and related fixtures, fittings and services e.g. air and water supplies
HBNs Health Building Notes – give best practice guidance on the design and planning of new healthcare buildings and on the adaptation/extension of existing facilities
HTMs Health Technical Memoranda – give comprehensive guidance on the design, installation and operation of specialised building and engineering technology used in the delivery of healthcare applicable to new and existing sites
HVAC system Heating, ventilation, air conditioning system
Refurbishment To renovate e.g. painting, repairing, cleaning etc. to make as new
Risk Assessment Risk assessment is fundamental in the planning and design stages of a healthcare facility, yet it is often overlooked or compromised throughout the lifecycle of the project. Disseminating good specialist knowledge and involving Infection Prevention and Control Teams throughout all phases of construction and renovation projects will reduce risks. Failure to properly assess prevention and control of infection risk can lead to expensive redesign later and expose the patient and healthcare worker to infection hazards. The risk of infection increases when micro-organisms exist in sufficient numbers in the environment and have the means of transmission to a susceptible host. Implementation of effective prevention and control of infection reduce the risk of transmission by promoting an environment where the risk of interaction between the organism and the susceptible host is minimised by ensuring:
Design and maintenance of suitable ventilation systems which minimise accumulation of liquids in the airstream.
Adequate space for storage of equipment and consumables.
Design which facilitate cleaning and good housekeeping.
Easy access to adequate hand hygiene facilities.
Adequate decontamination facilities e.g. housekeepers room and dirty utility rooms etc.
Adequate space for patient, staff and equipment movement.
Surfaces, finishings and fittings which minimise dust accumulation.
Surfaces, finishings and fittings which can withstand recommended decontamination processes and which are cleanable.
Secure and prompt waste and laundry disposal.
Key Principles and Considerations

Infection Prevention and Control in the Built Environment. Page 4 of 27 Version 1.1 March 2019
Once the project management team becomes aware of any proposed building/refurbishment work within the Trust, they must complete Appendix 2 and 3 and send them to the Infection Prevention and Control Team (IPCT). The IPCT will complete appropriately and forward to the named Project Manager within 3 working days.
Project Team The project team must include representatives from the following groups as a minimum:
Capital Planning and Estates
Infection Prevention and Control Team
Clinical/ department representatives
Service Manager
Lead Nurse/Matrons
Design team e.g. architects, service consultants, project manager etc.
Site Concierge considering housekeeping, catering, portering, security issues etc.
Procurement
Fire Officer
Health and Safety Officer
Risk Facilitator
Information from these representatives can be used to inform the Design Team and to amend existing schedules before and during the construction phase. Considerations The Project Team must consider the following:
How will the product, equipment, room, ward or clinic be used?
What possible solutions are available?
What are the budgetary limitations?
Which infection prevention and control principles or external regulations apply?
What does the evidence suggest in relation to the specific context?
What are the laws governing the project?
What are the standards and guidelines from architectural and engineering bodies, government departments and accrediting agencies?
Which product or design best balances the infection control requirements with employee and patient safety and satisfaction and cost constraints?
General infection prevention and control environmental requirements can be seen in Appendix 4. Before Work Commences It is important to consider certain issues before construction/renovation work commences including:
The type and extent of demolition, construction or renovation work
The likelihood of contamination to adjacent patient care areas - consider risks e.g. aspergillus.
The impact on traffic for supplies e.g. stock storage and delivery.

Infection Prevention and Control in the Built Environment. Page 5 of 27 Version 1.1 March 2019
The air flow and pressure differentials in the area (differentials may be varied by external wind strength and direction). Are there industries in the vicinity posing a risk of pollution which may affect operational issues e.g. windows being kept closed?
Are there adjacent cooling towers which pose a risk of legionella infection?
Does the proposed new build pose a risk to existing healthcare premises?
The susceptibility of the occupants to infection e.g. through respiratory problems, immune-compromised or vulnerable patients.
Do the plans meet the requirements of the relevant building and technical guidance to build-in infection prevention?
Requirements for extra cleaning services?
Work Flow
Work flow and agreed timescales are important to prevent incidents that potentially put patients, staff and visitors at risk, clinicians must be involved to ensure co-operation and risk reduction
Where work is being undertaken whilst patient services continue consideration must be given to the level of dust produced and appropriate dust control be put in place in addition to the cleaning programme
Frequent monitoring of the area is required to highlight any problems or systems failures with regard to cleaning during the project
Demolition and Disturbance The airborne route of transmission is important for of a number of pathogenic microorganisms such as Aspergillus, and every attempt should be made to maintain an environment as free from dust, aerosols and spores as possible during engineering and building works carried out in the healthcare environment. When any demolition work is indicated, no matter how small, it is essential that precautions are taken to minimise the level of dust. These precautions will depend on the amount of dust anticipated. Any disturbance of the environment caused by maintenance, demolition, construction and renovation presents risk of infection to the occupants including:
Exposure to air-borne micro-organisms and fungal spores such as Aspergillus species
Water entry and absorption into building materials leading to increased microbial contamination
Access for insect pests and vermin
Increased traffic through the facility
Dust and debris in patient care areas Additional cleaning programmes will need to be introduced to manage the level of dust generated to ensure that patient areas remain clean. Dust Control Barriers may be required for dust control where work is to be carried out near patient areas e.g. during:
Demolition of walls, plaster and ceilings.
Removal of flooring, carpets, windows and doors.
Routine maintenance activities.
Infection Prevention and Control in the Built Environment. Page 6 of 27 Version 1.1 March 2019
Any work with water which may aerosolise water droplets in high risk areas.
Exposure of ceiling voids.
Repairing water damage. Environmental Monitoring The robustness of the environmental control measures should be monitored on a daily basis by the Project Manager and the site Concierge, however it may be necessary for the Infection Prevention and Control Team to support and advice in certain circumstances.
Dust proof barriers should be inspected at least daily to ensure they remain intact.
Construction teams should be regularly monitored by the Estates and Facilities Team to ensure compliance with Trust policy and procedures.
Recommendations for the Control of Contamination Risks
Communication with all parties including the IPC Team is essential to reduce the risks of infection through all stages of the demolition/construction work.
The construction/demolition area should be sealed fully and erection of airtight plastic and dry wall barriers around the site, a dust barrier should be created from floor to the ‘true ceiling’ and edges sealed; however for more long-term projects this should be a solid sealed barrier. In addition covering of all air intake and exhaust vents in the ‘construction zone’ to prevent the introduction of contaminated air into the healthcare environment including heating, ventilation and air conditioning systems, capping open ends of any existing ventilation ducts in the zone. It may be necessary to create a lobby (anteroom) if the barrier is the entrance/egress for construction workers.
Windows, doors, vents, plumbing penetrations, electrical outlets and any other source of potential air leak should be sealed in the construction zone.
Air pressure in the construction zone should be negative compared with adjacent areas; an extract fan may be used for this purpose. Air from the construction zone should be exhausted directly outside, if this is not possible it should be filtered through HEPA filters before being re-circulated to the healthcare environment. (Ensuring filters are properly fitted and strictly monitored.
Redirection of construction traffic away from patient areas with workmen having separate access to the construction site. Wherever possible patients, staff and visitors should be prevented from entering the healthcare environment adjacent to major construction/ demolition sites or where debris or dust is being removed from the works area.
Regular removal of construction debris from the site in sealed containers (or covered with an impermeable moistened sheet) before removing for disposal, this should be done at least daily. An external chute will need to be erected if the construction work is not taking place at ground level. All skips used for temporary storage and disposal of waste materials should be covered and lockable to prevent dust release and unauthorised disturbance.
Cleaning – damp dusting and not dry cleaning is recommended, vacuum and wet mop area as needed to maintain an environment as free from dust as possible. Wipe horizontal and vertical work surfaces with hot soapy water. Increasing the existing cleaning regimes to prevent dust accumulation on surfaces, ceilings and air duct grilles.
Multi-layer sticky/tacky mats to be used at site entrance/egress to trap dirt, dust and possible contaminants from footwear and wheels before entering clean areas. This should be changed at least daily or more frequently if visibly soiled or no longer tacky.
Overshoes should be considered including facilities for disposal and decontamination of hands following their removal.
Infection Prevention and Control in the Built Environment. Page 7 of 27 Version 1.1 March 2019
All windows, doors (apart from essential access points) and vents should be sealed in areas of the healthcare environment containing the most susceptible patients as advised by the IPC Team.
Alternative routes which avoid the construction site should be identified during construction. Clean or sterile supplies or equipment should be transported by a route that minimises contamination risks; this may involve reviewing delivery schedules.
Post Completion of Work
Upon completion the contractor is responsible for the first level of cleaning.
Thereafter the Facilities Team are to undertake a deep clean of the area.
The area will only be declared fit for use once a member of the Infection Prevention and Control Team is satisfied with the level of cleanliness.
The project team should be aware that the immediate healthcare environment can be a potential reservoir of micro-organisms and source of infection or contamination, MRSA for example may survive and persist in the environment leading to recurrent outbreaks. Therefore designers and planners need to consider eliminating potential sources of infection by practising good design in relation to:
Adequate and well organised storage facilities to minimise clutter in the environment and provide safe storage of essential equipment and consumables.
Choice of materials, avoiding unnecessary surfaces that may become reservoirs for infectious agents.
Ensuring materials and surfaces can be cleaned and maintained easily.
Attention to the prevention of airborne infection by the use of ventilation in specialist areas. Correct engineering and mechanical services contribute greatly to reducing potential reservoirs of infection in the built environment.
Elimination of other environmental sources of infection e.g. pests, insects, birds, small animals which carry micro-organisms and disposal of litter and waste should be considered throughout the project.
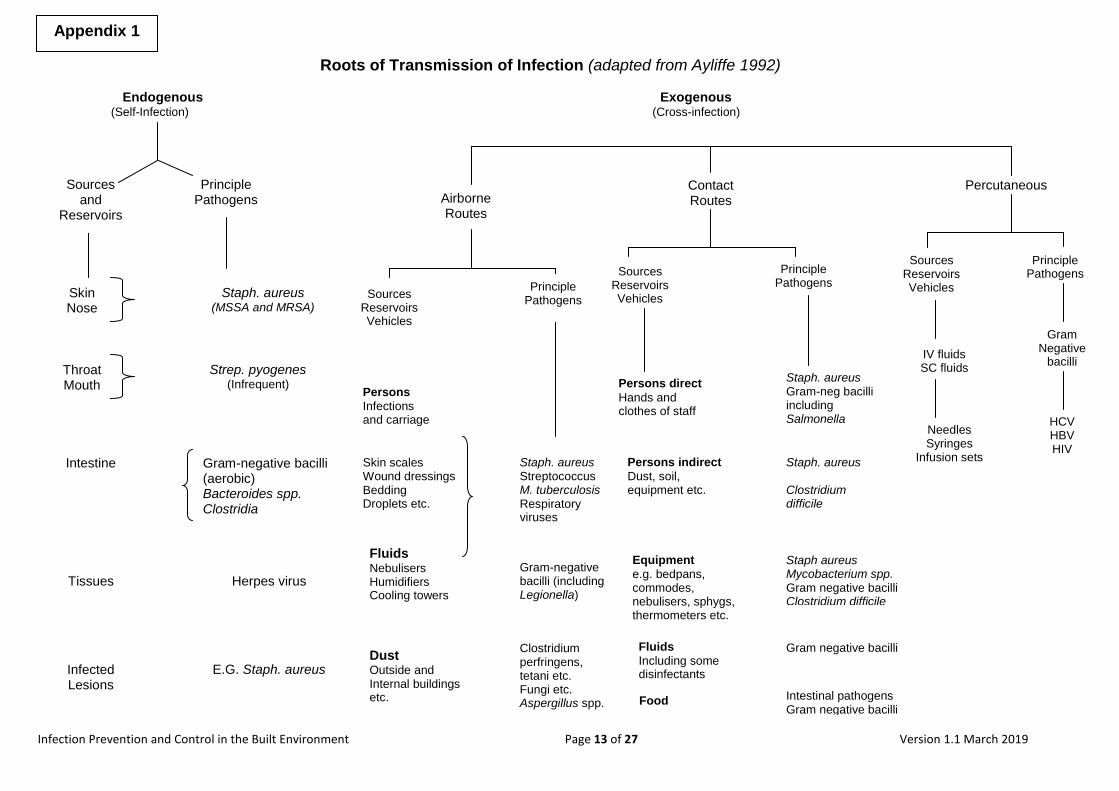
Mode of Transmission (see Appendix 1) Micro-organisms can be transmitted in three main ways:
Direct transmission - involving direct transfer of micro-organisms to the skin or mucous membranes by direct contact
Indirect transmission - involving an immediate stage between the source of infection and the individual e.g. infected food, water or vector borne transmission by insects
Airborne transmission - involving inhalation of aerosols containing micro-organisms e.g. legionella or tuberculosis
Susceptible Recipient (patient) Some groups of patients are particularly susceptible to certain infectious agents to which they may be exposed in the healthcare construction/refurbishment environment e.g.
Sources of Infection

Infection Prevention and Control in the Built Environment. Page 8 of 27 Version 1.1 March 2019
immunocompromised patients, those with significant underlying conditions, the very old and the very young. Transmission of micro-organisms with potential to cause infection requires three main elements:
A susceptible host.
Reservoir of an infectious agent.
An environment which allows the infectious agent to colonise and possibly cause an infection to a susceptible host.
Therefore it is important to assess the infection risks throughout all stages of the project, environmental airborne contaminants and infectious agents are closely related to water and moist conditions which feature prominently in construction and refurbishment activities.
Common errors in design and construction can be costly to rectify, therefore risk management should ensure that these common errors do no occur, for example:
Pressure to choose the cheapest products or design.
Air intakes placed too close to exhausts or other mistakes in the placement of air intakes.
Incorrect air turnover and airflow patterns.
Air-handling systems which function only during the week or on particular days/times.
Ventilations systems which are not fully commissioned.
Carpet placed where vinyl should be used.
Aerators on taps (also avoid swan-neck where possible).
Inability due to design factors to undertake regular planned flushing or maintenance of water systems.
Patient rooms or treatment rooms which do not have compliant sinks in which healthcare workers can wash their hands.
Doors to narrow to allow beds and equipment to be moved in and out of rooms.
Inadequate space to allow safe use and storage of medical devices, equipment and consumables.
The purpose of evaluation is to improve future project appraisal, design management and implementation. The Project Team will undertake the evaluation with contributions from all parties involved including the Infection Prevention and Control Team. The evaluation will need to be undertaken when the facility has been in use for some time and will include:
Project appraisal
Monitoring and evaluation of the project
Review of project operations, what worked well, and what could be improved etc.
Common Problems to Avoid
Post Project Evaluation

Infection Prevention and Control in the Built Environment. Page 9 of 27 Version 1.1 March 2019
Lessons learnt.
Infection Prevention and Control in the Built Environment. Page 10 of 27 Version 1.1 March 2019
The principle is to maintain sufficient space for activities to take place and to avoid the transmission of organisms either by air or by contact with blood and body fluids or equipment.
Compliance with hand hygiene guidelines can be improved by conveniently placed and well-designed hand hygiene facilities.
Design, accessibility and space in patient areas must be sufficient to take into account ease of cleaning and maintenance.
There must be sufficient sanitary facilities and they must not be used as storage facilities.
There must be sufficient facilities designed to accommodate systems for decontamination of medical devices, if appropriate for the area.
Important
Always consult the Infection Prevention and Control Team at an early stage:
Whenever refitting or refurbishment is planned
Whenever major capital bids are planned
Whenever installation of new equipment is planned e.g. boilers, macerators, clinical equipment etc.
Do not wait until:
The patients are ready to move in or
Fixtures and fittings or equipment and furnishings have been purchased Most infection prevention and control advice will be common sense but not always popular financially, do not let space or cost override reason.
Where do I go for further advice or information?
Estates Manager
Capital Planning Officer
Infection Prevention and Control Team Your Service Manager, Matron, General Manager, Head of Nursing, Group Director
Your Group Governance Staff and Risk Facilitator Key national standard documents e.g. Health Building Notes (HBNs) etc.: Health Building Notes (HBNs) are the key documents for all health building, planning and briefing guidance in England. They draw together the best current knowledge for healthcare needs and should be regarded as setting standards of best practice and providing essential information on how to comply with the statutory and policy framework and help to achieve value for money solutions for the planning and design of healthcare facilities.
HBN 00-01: General design guidance for healthcare buildings (2014)
HBN 00-02: Designing sanitary spaces like bathrooms (2016)
HBN 00-03: Designing generic clinical and clinical support spaces (2013)
Recommendations

Infection Prevention and Control in the Built Environment. Page 11 of 27 Version 1.1 March 2019
HBN 00-04: Designing stairways, lifts and corridors in healthcare buildings (2013)
HBN 00-09: Infection control in the built environment (2013)
HBN 00-10: Design for flooring, walls, ceilings, sanitary ware and windows (2013)
HBN 03-01: Adult mental health units, planning and design (2013)
HBN 04-01: Adult in-patient facilities, planning and design (2013)
HBN 04-01: Supplement 1 – isolation facilities for infectious patients in acute settings (2013)
HBN 08-02: Dementia-friendly health and social care environments (2015)
HBN 12: Designing an out-patients department (2004)
HTM 03-01:Specialised ventilation for healthcare premises: Part A – Design and validation (2007)
HTM 03-01:Specialised ventilation for healthcare premises: Part B – Operational management and performance verification (2007)
HTM 04-01: Safe water in healthcare premises – Part A: Design, installation and testing. (2016)
HTM 04-01: Safe water in healthcare premises – Part B:Operational management (2016)
HTM 04-01: Safe water in healthcare premises – Part C: Pseudomonas aeruginosa - advice for augmented care units (2016)
HTM 04-01: Supplement – Performance specification D 08: thermostatic mixing valves (healthcare premises) (2017)
HTM 07-01: Management and disposal of healthcare waste (2013)
HTM 07-04: Water management and water efficiency – best practice advice for the healthcare sector (2013)
HTM 07-02: EnCO2de 2015 – making energy work in healthcare. Environment and sustainability Part A: Policy and management (2015)
HTM 07-02: EnCO2de 2015 – making energy work in healthcare. Environment and sustainability Part B: Procurement and energy considerations for new and existing building facilities (2015)
HTM 01-04: Decontamination of linen for health and social care. Management and provision (2016)
HTM 01-04: Decontamination of linen for health and social care. Engineering, equipment and validation (2016)
HTM 01-04: Decontamination of linen for health and social care. Guidance for linen processors implementing BS EN 14065 (2016)
Training Staff may receive training in relation to this procedure, where it is identified in their appraisal as part of the specific development needs for their role and responsibilities. Please refer to the Trust’s Mandatory and Risk Management Training Needs Analysis for further details on training requirements, target audiences and update frequencies. Monitoring / Review of this Procedure In the event of planned change in the process(es) described within this document or an incident involving the described process(es) within the review cycle, this SOP will be reviewed and revised as necessary to maintain its accuracy and effectiveness.

Infection Prevention and Control in the Built Environment. Page 12 of 27 Version 1.1 March 2019
Equality Impact Assessment Please refer to overarching policy
Data Protection Act and Freedom of Information Act Please refer to overarching policy
Infection Prevention and Control in the Built Environment Page 13 of 27 Version 1.1 March 2019
Roots of Transmission of Infection (adapted from Ayliffe 1992) Endogenous Exogenous (Self-Infection) (Cross-infection)
Appendix 1
Sources and
Reservoirs
Principle Pathogens
Skin Nose
Throat Mouth
Intestine
Tissues
Infected Lesions
Staph. aureus (MSSA and MRSA)
Strep. pyogenes (Infrequent)
Gram-negative bacilli (aerobic) Bacteroides spp. Clostridia Fungi
Herpes virus
E.G. Staph. aureus
Airborne Routes
Contact Routes
Percutaneous
Sources Reservoirs Vehicles
Principle Pathogens
Persons
Infections and carriage
Skin scales Wound dressings Bedding Droplets etc.
Fluids Nebulisers Humidifiers Cooling towers
Dust Outside and Internal buildings etc.
Staph. aureus Streptococcus M. tuberculosis Respiratory viruses
Gram-negative bacilli (including Legionella)
Clostridium perfringens, tetani etc. Fungi etc. Aspergillus spp.
Sources Reservoirs Vehicles
Principle Pathogens
Persons direct
Hands and clothes of staff
Persons indirect
Dust, soil, equipment etc.
Equipment
e.g. bedpans, commodes, nebulisers, sphygs, thermometers etc.
Fluids
Including some disinfectants
Food
Staph. aureus Gram-neg bacilli including Salmonella Viruses
Staph. aureus Clostridium difficile
Staph aureus Mycobacterium spp. Gram negative bacilli Clostridium difficile
Gram negative bacilli
Intestinal pathogens Gram negative bacilli
Sources Reservoirs Vehicles
Principle Pathogens
IV fluids SC fluids
Needles Syringes
Infusion sets
Gram Negative
bacilli
HCV HBV HIV

Infection Prevention and Control in the Built Environment. Page 14 of 27 Version 1.1 March 2019
Infection Prevention and Control in the Built Environment – Risk Assessment Form
Site: Building:
Rooms: Project start date:
Estimated duration:
Project Manager: Direct Phone No:
Description of activity:
Step 1: Identify building / construction activity type from the table below:
TYPE A Inspection and non-invasive activities, includes but not limited to:
Removal of ceiling tiles for visual inspection on corridors and non-clinical areas
Painting and minimum preparation in corridors and non-clinical areas
Electrical trim work (all plugs, switches, light fixtures, smoke detectors and ventilation fans
Minor plumbing and activities that do no generate dust or require cutting of walls or access to ceilings other than for inspection.
TYPE B Small scale, short duration activities that create minimal dust includes:
Removal of a limited number of ceiling tiles in low risk clinical areas for inspection only
Installation of telephone and computer cabling
Access to chase spaces
Cutting of walls or ceiling where dust migration can be controlled in non-clinical areas
TYPE C Any work of long/short duration which generates a moderate to high level of dust or requires minor building works, demolition or removal of any fixed building components or assemblies. Includes but is not limited to:
Sanding of walls/woodwork for painting or wall covering
Removal of floor coverings, ceiling tiles, panelling and wall mounted shelving and cabinets
New wall construction
Minor duct work or electrical work above ceilings
Major cabling activities
TYPE D Major demolition and construction projects. Includes but is not limited to new construction/ machinery and equipment installations, rectifications and modifications.
Step 2: Then identify the population/risk group likely to be affected by area
Group 1 (low risk) Group 2 (medium risk) Group 3 (high risk)
Office areas
Corridors
Plant rooms
Service ducts
Unoccupied wards
Staff rooms
Clinical departments e.g. out-patients
Pharmacy dispensing rooms
Consulting rooms
Hydrotherapy pools
Staff kitchens
Clozapine clinic rooms
ECT suite
Food production kitchens
All in-patient areas
Any area caring for immune-compromised patients e.g. on high dose steroids, chemotherapy, previous organ or bone marrow transplantation.
Step 3: Identify risk class by correlating construction type with risk group in 1 and 2 above using Matrix below:
CONSTRUCTION ACTIVITY
Risk of Area TYPE A TYPE B TYPE C TYPE D
Group 1 (low) NO NO NO YES
Group 2 (medium) NO NO YES YES
Group 3 (high) NO YES YES YES
Appendix 2
Infection Prevention and Control in the Built Environment. Page 15 of 27 Version 1.1 March 2019
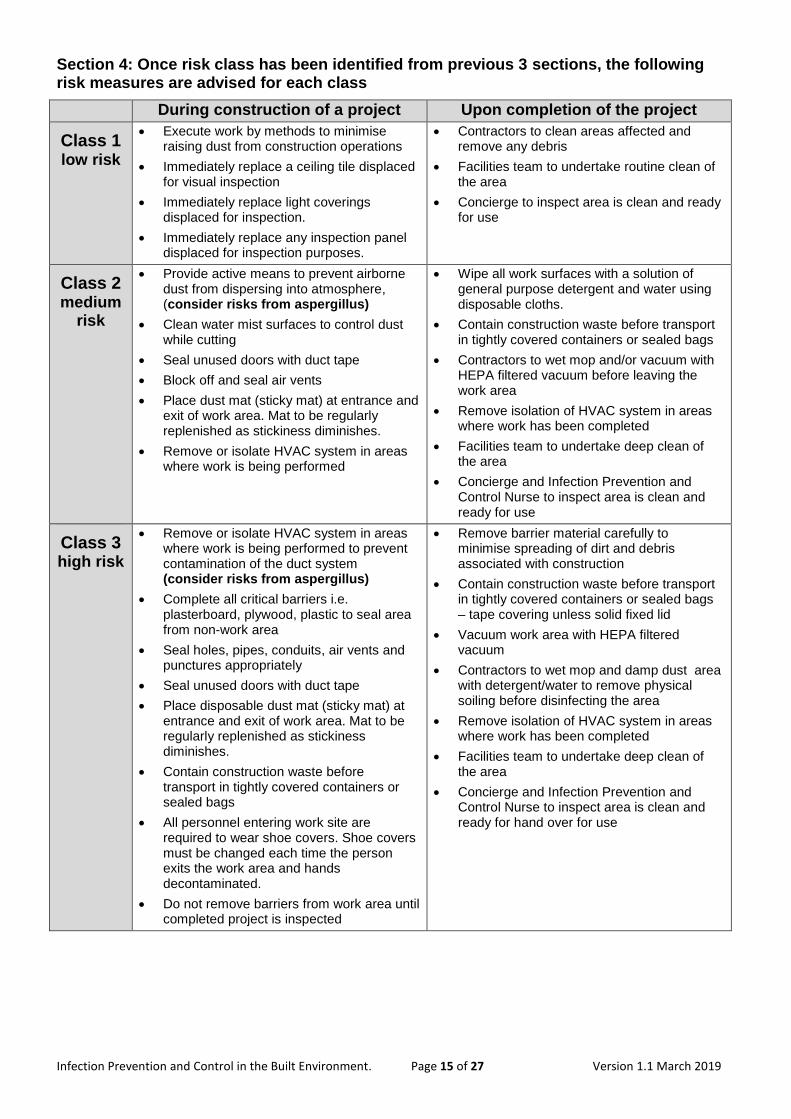
Section 4: Once risk class has been identified from previous 3 sections, the following risk measures are advised for each class
During construction of a project Upon completion of the project
Class 1 low risk
Execute work by methods to minimise raising dust from construction operations
Immediately replace a ceiling tile displaced for visual inspection
Immediately replace light coverings displaced for inspection.
Immediately replace any inspection panel displaced for inspection purposes.
Contractors to clean areas affected and remove any debris
Facilities team to undertake routine clean of the area
Concierge to inspect area is clean and ready for use
Class 2 medium
risk
Provide active means to prevent airborne dust from dispersing into atmosphere, (consider risks from aspergillus)
Clean water mist surfaces to control dust while cutting
Seal unused doors with duct tape
Block off and seal air vents
Place dust mat (sticky mat) at entrance and exit of work area. Mat to be regularly replenished as stickiness diminishes.
Remove or isolate HVAC system in areas where work is being performed
Wipe all work surfaces with a solution of general purpose detergent and water using disposable cloths.
Contain construction waste before transport in tightly covered containers or sealed bags
Contractors to wet mop and/or vacuum with HEPA filtered vacuum before leaving the work area
Remove isolation of HVAC system in areas where work has been completed
Facilities team to undertake deep clean of the area
Concierge and Infection Prevention and Control Nurse to inspect area is clean and ready for use
Class 3 high risk
Remove or isolate HVAC system in areas where work is being performed to prevent contamination of the duct system (consider risks from aspergillus)
Complete all critical barriers i.e. plasterboard, plywood, plastic to seal area from non-work area
Seal holes, pipes, conduits, air vents and punctures appropriately
Seal unused doors with duct tape
Place disposable dust mat (sticky mat) at entrance and exit of work area. Mat to be regularly replenished as stickiness diminishes.
Contain construction waste before transport in tightly covered containers or sealed bags
All personnel entering work site are required to wear shoe covers. Shoe covers must be changed each time the person exits the work area and hands decontaminated.
Do not remove barriers from work area until completed project is inspected
Remove barrier material carefully to minimise spreading of dirt and debris associated with construction
Contain construction waste before transport in tightly covered containers or sealed bags – tape covering unless solid fixed lid
Vacuum work area with HEPA filtered vacuum
Contractors to wet mop and damp dust area with detergent/water to remove physical soiling before disinfecting the area
Remove isolation of HVAC system in areas where work has been completed
Facilities team to undertake deep clean of the area
Concierge and Infection Prevention and Control Nurse to inspect area is clean and ready for hand over for use

Infection Prevention and Control in the Built Environment. Page 16 of 27 Version 1.1 March 2019
Stage of Infection Prevention and Control Assessment Required
Stages at which input from the Infection Prevention and Control Team (IPCT) into
construction, renovation and refurbishments projects required
Tick
which is appropriate
Comments
1. Concept / Feasibility
The IPCT should review clinical operational policies and procedures e.g.:
Adding beds to ward areas may require extra sluice, single room isolation, hand washing facilities or additional storage capacity
Adding additional specialist services may need a review of decontamination facilities, equipment or instruments
Additional services will require infection prevention and control input/advice/visits etc.
Sketch plans will need to give a broad view of infection control issues at this stage in clinical areas
2. Detail Planning
Discussion regarding the locations of clinical areas for correct workflows / infection prevention practice e.g. wards, clinics, kitchens etc.
Discussion of finer details including location and type of fixtures and fittings, airflows, water maintenance, hand wash sinks, flooring, room layouts etc. Consider infection risks in detail.
3. Construction
The IPCT will need input here if new build is attached to existing healthcare building to prevent risk to patients
4. Equipment
Decision on equipment should be made as an on-going process – IPCT to consider decontamination requirements.
5. Trust Commissioning / equipping
The IPCT should have an input during this stage if costly mistakes are not to be made.
6. Evaluation
Stage at which lessons learnt can be highlighted for future projects.
Appendix 3
Infection Prevention and Control in the Built Environment. Page 17 of 27 Version 1.1 March 2019
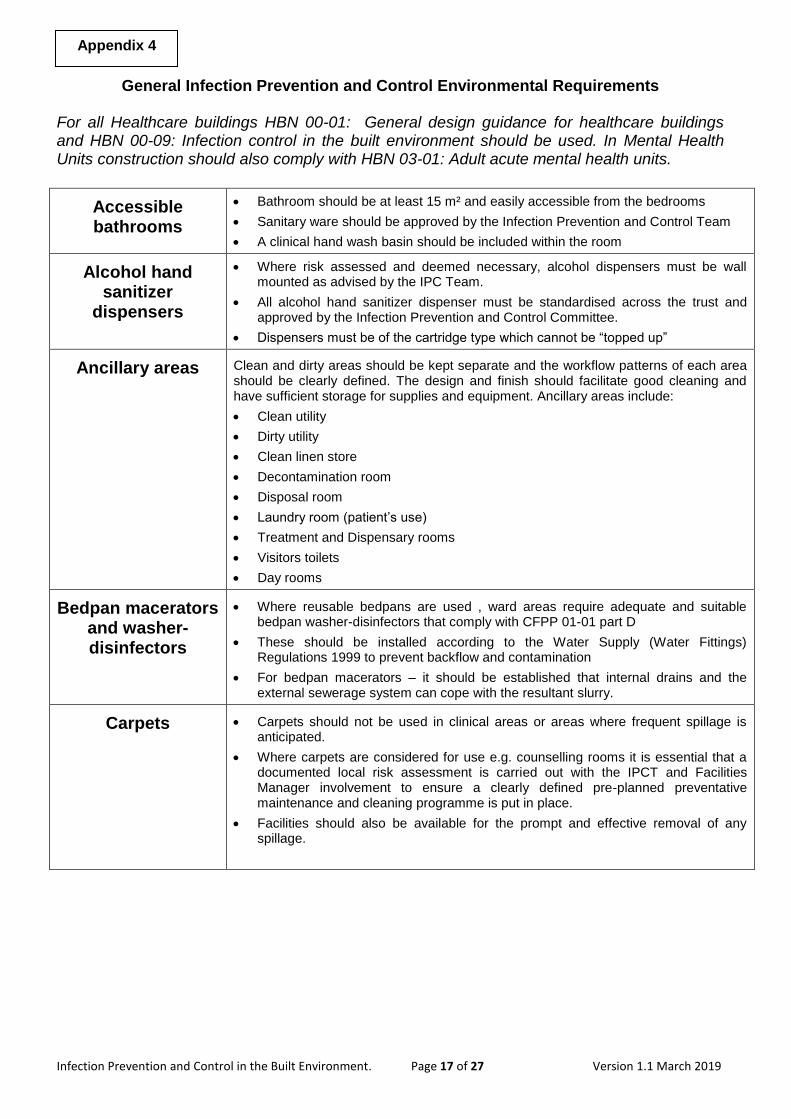
General Infection Prevention and Control Environmental Requirements
For all Healthcare buildings HBN 00-01: General design guidance for healthcare buildings and HBN 00-09: Infection control in the built environment should be used. In Mental Health Units construction should also comply with HBN 03-01: Adult acute mental health units.
Accessible bathrooms
Bathroom should be at least 15 m² and easily accessible from the bedrooms
Sanitary ware should be approved by the Infection Prevention and Control Team
A clinical hand wash basin should be included within the room
Alcohol hand sanitizer
dispensers
Where risk assessed and deemed necessary, alcohol dispensers must be wall mounted as advised by the IPC Team.
All alcohol hand sanitizer dispenser must be standardised across the trust and approved by the Infection Prevention and Control Committee.
Dispensers must be of the cartridge type which cannot be “topped up”
Ancillary areas
Clean and dirty areas should be kept separate and the workflow patterns of each area should be clearly defined. The design and finish should facilitate good cleaning and have sufficient storage for supplies and equipment. Ancillary areas include:
Clean utility
Dirty utility
Clean linen store
Decontamination room
Disposal room
Laundry room (patient’s use)
Treatment and Dispensary rooms
Visitors toilets
Day rooms
Bedpan macerators and washer-disinfectors
Where reusable bedpans are used , ward areas require adequate and suitable bedpan washer-disinfectors that comply with CFPP 01-01 part D
These should be installed according to the Water Supply (Water Fittings) Regulations 1999 to prevent backflow and contamination
For bedpan macerators – it should be established that internal drains and the external sewerage system can cope with the resultant slurry.
Carpets Carpets should not be used in clinical areas or areas where frequent spillage is anticipated.
Where carpets are considered for use e.g. counselling rooms it is essential that a documented local risk assessment is carried out with the IPCT and Facilities Manager involvement to ensure a clearly defined pre-planned preventative maintenance and cleaning programme is put in place.
Facilities should also be available for the prompt and effective removal of any spillage.
Appendix 4
Infection Prevention and Control in the Built Environment. Page 18 of 27 Version 1.1 March 2019
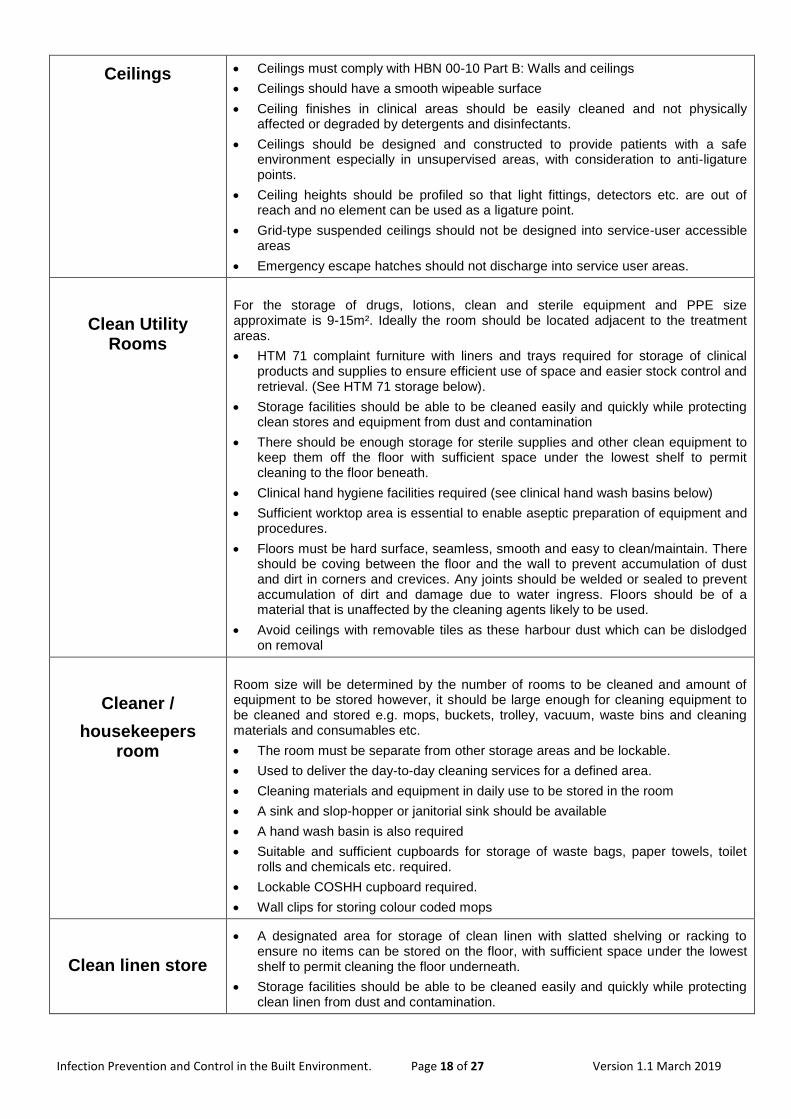
Ceilings Ceilings must comply with HBN 00-10 Part B: Walls and ceilings
Ceilings should have a smooth wipeable surface
Ceiling finishes in clinical areas should be easily cleaned and not physically affected or degraded by detergents and disinfectants.
Ceilings should be designed and constructed to provide patients with a safe environment especially in unsupervised areas, with consideration to anti-ligature points.
Ceiling heights should be profiled so that light fittings, detectors etc. are out of reach and no element can be used as a ligature point.
Grid-type suspended ceilings should not be designed into service-user accessible areas
Emergency escape hatches should not discharge into service user areas.
Clean Utility Rooms
For the storage of drugs, lotions, clean and sterile equipment and PPE size approximate is 9-15m². Ideally the room should be located adjacent to the treatment areas.
HTM 71 complaint furniture with liners and trays required for storage of clinical products and supplies to ensure efficient use of space and easier stock control and retrieval. (See HTM 71 storage below).
Storage facilities should be able to be cleaned easily and quickly while protecting clean stores and equipment from dust and contamination
There should be enough storage for sterile supplies and other clean equipment to keep them off the floor with sufficient space under the lowest shelf to permit cleaning to the floor beneath.
Clinical hand hygiene facilities required (see clinical hand wash basins below)
Sufficient worktop area is essential to enable aseptic preparation of equipment and procedures.
Floors must be hard surface, seamless, smooth and easy to clean/maintain. There should be coving between the floor and the wall to prevent accumulation of dust and dirt in corners and crevices. Any joints should be welded or sealed to prevent accumulation of dirt and damage due to water ingress. Floors should be of a material that is unaffected by the cleaning agents likely to be used.
Avoid ceilings with removable tiles as these harbour dust which can be dislodged on removal
Cleaner /
housekeepers room
Room size will be determined by the number of rooms to be cleaned and amount of equipment to be stored however, it should be large enough for cleaning equipment to be cleaned and stored e.g. mops, buckets, trolley, vacuum, waste bins and cleaning materials and consumables etc.
The room must be separate from other storage areas and be lockable.
Used to deliver the day-to-day cleaning services for a defined area.
Cleaning materials and equipment in daily use to be stored in the room
A sink and slop-hopper or janitorial sink should be available
A hand wash basin is also required
Suitable and sufficient cupboards for storage of waste bags, paper towels, toilet rolls and chemicals etc. required.
Lockable COSHH cupboard required.
Wall clips for storing colour coded mops
Clean linen store
A designated area for storage of clean linen with slatted shelving or racking to ensure no items can be stored on the floor, with sufficient space under the lowest shelf to permit cleaning the floor underneath.
Storage facilities should be able to be cleaned easily and quickly while protecting clean linen from dust and contamination.
Infection Prevention and Control in the Built Environment. Page 19 of 27 Version 1.1 March 2019
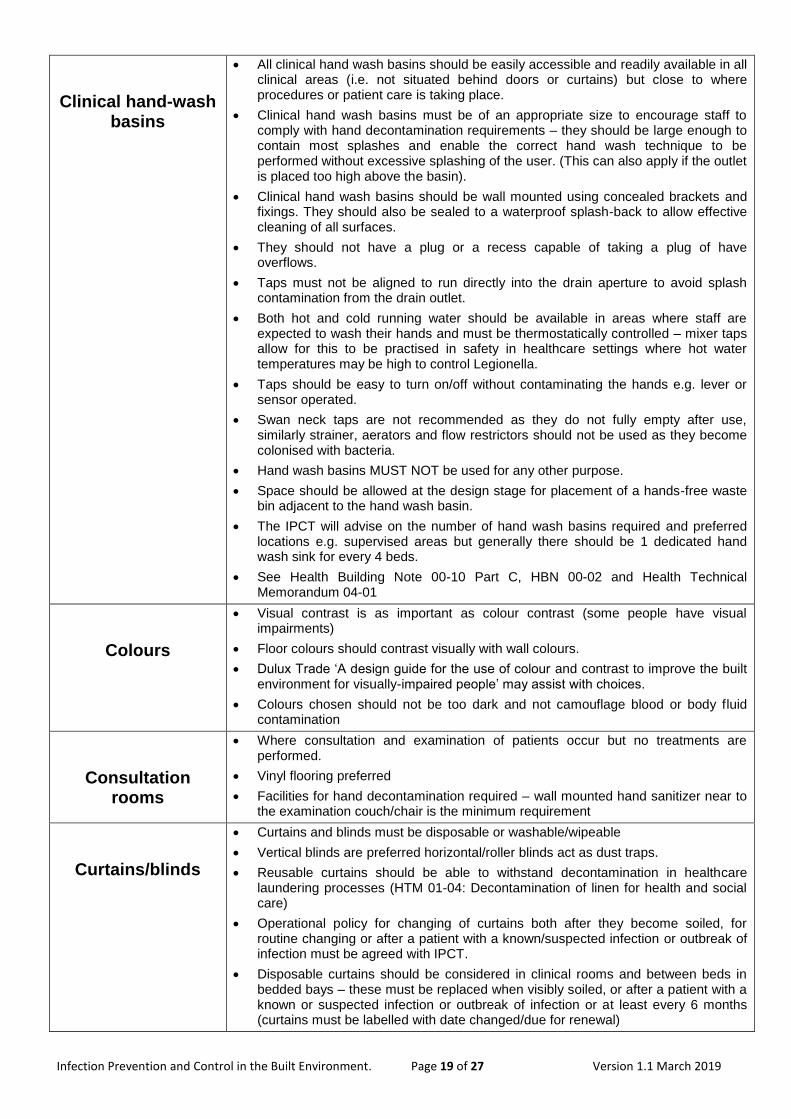
Clinical hand-wash basins
All clinical hand wash basins should be easily accessible and readily available in all clinical areas (i.e. not situated behind doors or curtains) but close to where procedures or patient care is taking place.
Clinical hand wash basins must be of an appropriate size to encourage staff to comply with hand decontamination requirements – they should be large enough to contain most splashes and enable the correct hand wash technique to be performed without excessive splashing of the user. (This can also apply if the outlet is placed too high above the basin).
Clinical hand wash basins should be wall mounted using concealed brackets and fixings. They should also be sealed to a waterproof splash-back to allow effective cleaning of all surfaces.
They should not have a plug or a recess capable of taking a plug of have overflows.
Taps must not be aligned to run directly into the drain aperture to avoid splash contamination from the drain outlet.
Both hot and cold running water should be available in areas where staff are expected to wash their hands and must be thermostatically controlled – mixer taps allow for this to be practised in safety in healthcare settings where hot water temperatures may be high to control Legionella.
Taps should be easy to turn on/off without contaminating the hands e.g. lever or sensor operated.
Swan neck taps are not recommended as they do not fully empty after use, similarly strainer, aerators and flow restrictors should not be used as they become colonised with bacteria.
Hand wash basins MUST NOT be used for any other purpose.
Space should be allowed at the design stage for placement of a hands-free waste bin adjacent to the hand wash basin.
The IPCT will advise on the number of hand wash basins required and preferred locations e.g. supervised areas but generally there should be 1 dedicated hand wash sink for every 4 beds.
See Health Building Note 00-10 Part C, HBN 00-02 and Health Technical Memorandum 04-01
Colours
Visual contrast is as important as colour contrast (some people have visual impairments)
Floor colours should contrast visually with wall colours.
Dulux Trade ‘A design guide for the use of colour and contrast to improve the built environment for visually-impaired people’ may assist with choices.
Colours chosen should not be too dark and not camouflage blood or body fluid contamination
Consultation rooms
Where consultation and examination of patients occur but no treatments are performed.
Vinyl flooring preferred
Facilities for hand decontamination required – wall mounted hand sanitizer near to the examination couch/chair is the minimum requirement
Curtains/blinds
Curtains and blinds must be disposable or washable/wipeable
Vertical blinds are preferred horizontal/roller blinds act as dust traps.
Reusable curtains should be able to withstand decontamination in healthcare laundering processes (HTM 01-04: Decontamination of linen for health and social care)
Operational policy for changing of curtains both after they become soiled, for routine changing or after a patient with a known/suspected infection or outbreak of infection must be agreed with IPCT.
Disposable curtains should be considered in clinical rooms and between beds in bedded bays – these must be replaced when visibly soiled, or after a patient with a known or suspected infection or outbreak of infection or at least every 6 months (curtains must be labelled with date changed/due for renewal)
Infection Prevention and Control in the Built Environment. Page 20 of 27 Version 1.1 March 2019
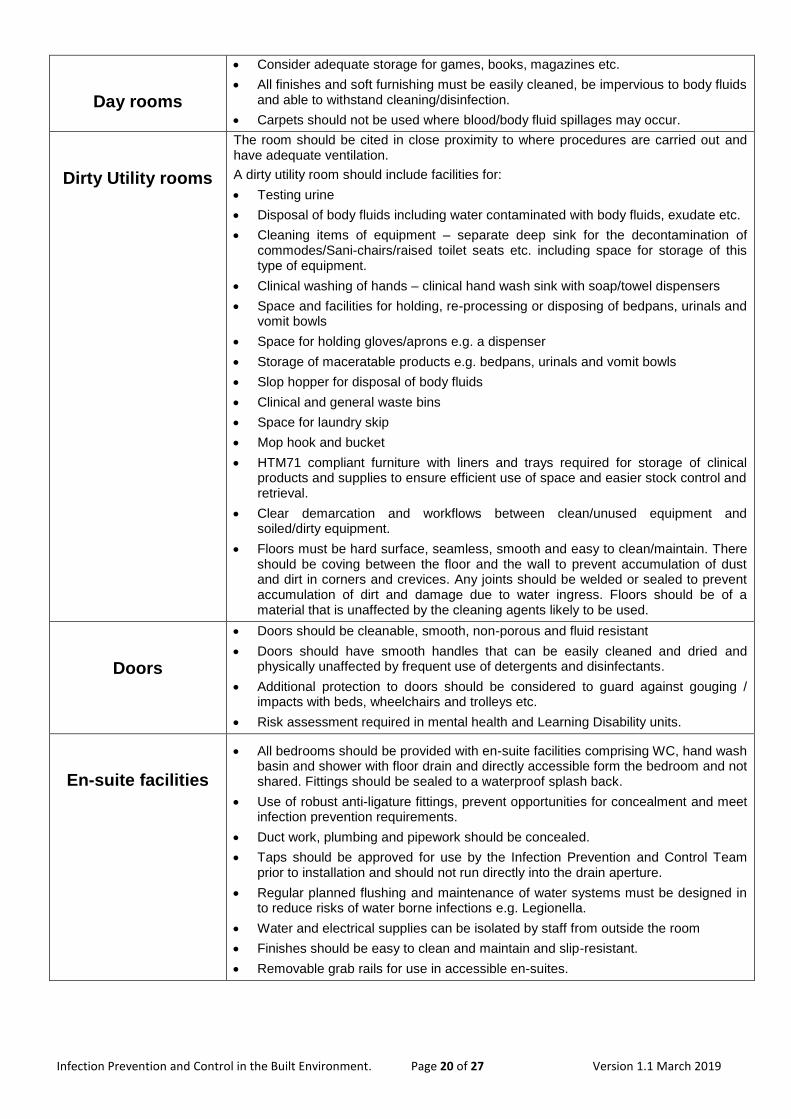
Day rooms
Consider adequate storage for games, books, magazines etc.
All finishes and soft furnishing must be easily cleaned, be impervious to body fluids and able to withstand cleaning/disinfection.
Carpets should not be used where blood/body fluid spillages may occur.
Dirty Utility rooms
The room should be cited in close proximity to where procedures are carried out and have adequate ventilation.
A dirty utility room should include facilities for:
Testing urine
Disposal of body fluids including water contaminated with body fluids, exudate etc.
Cleaning items of equipment – separate deep sink for the decontamination of commodes/Sani-chairs/raised toilet seats etc. including space for storage of this type of equipment.
Clinical washing of hands – clinical hand wash sink with soap/towel dispensers
Space and facilities for holding, re-processing or disposing of bedpans, urinals and vomit bowls
Space for holding gloves/aprons e.g. a dispenser
Storage of maceratable products e.g. bedpans, urinals and vomit bowls
Slop hopper for disposal of body fluids
Clinical and general waste bins
Space for laundry skip
Mop hook and bucket
HTM71 compliant furniture with liners and trays required for storage of clinical products and supplies to ensure efficient use of space and easier stock control and retrieval.
Clear demarcation and workflows between clean/unused equipment and soiled/dirty equipment.
Floors must be hard surface, seamless, smooth and easy to clean/maintain. There should be coving between the floor and the wall to prevent accumulation of dust and dirt in corners and crevices. Any joints should be welded or sealed to prevent accumulation of dirt and damage due to water ingress. Floors should be of a material that is unaffected by the cleaning agents likely to be used.
Doors
Doors should be cleanable, smooth, non-porous and fluid resistant
Doors should have smooth handles that can be easily cleaned and dried and physically unaffected by frequent use of detergents and disinfectants.
Additional protection to doors should be considered to guard against gouging / impacts with beds, wheelchairs and trolleys etc.
Risk assessment required in mental health and Learning Disability units.
En-suite facilities
All bedrooms should be provided with en-suite facilities comprising WC, hand wash basin and shower with floor drain and directly accessible form the bedroom and not shared. Fittings should be sealed to a waterproof splash back.
Use of robust anti-ligature fittings, prevent opportunities for concealment and meet infection prevention requirements.
Duct work, plumbing and pipework should be concealed.
Taps should be approved for use by the Infection Prevention and Control Team prior to installation and should not run directly into the drain aperture.
Regular planned flushing and maintenance of water systems must be designed in to reduce risks of water borne infections e.g. Legionella.
Water and electrical supplies can be isolated by staff from outside the room
Finishes should be easy to clean and maintain and slip-resistant.
Removable grab rails for use in accessible en-suites.
Infection Prevention and Control in the Built Environment. Page 21 of 27 Version 1.1 March 2019
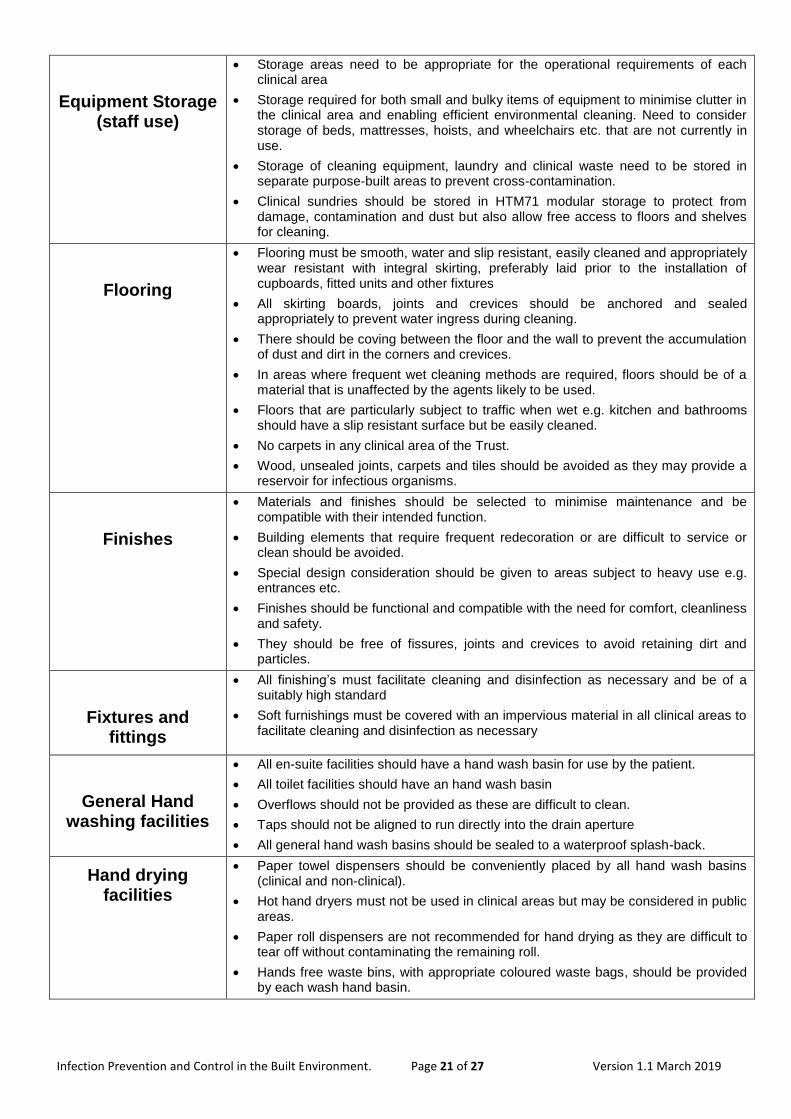
Equipment Storage (staff use)
Storage areas need to be appropriate for the operational requirements of each clinical area
Storage required for both small and bulky items of equipment to minimise clutter in the clinical area and enabling efficient environmental cleaning. Need to consider storage of beds, mattresses, hoists, and wheelchairs etc. that are not currently in use.
Storage of cleaning equipment, laundry and clinical waste need to be stored in separate purpose-built areas to prevent cross-contamination.
Clinical sundries should be stored in HTM71 modular storage to protect from damage, contamination and dust but also allow free access to floors and shelves for cleaning.
Flooring
Flooring must be smooth, water and slip resistant, easily cleaned and appropriately wear resistant with integral skirting, preferably laid prior to the installation of cupboards, fitted units and other fixtures
All skirting boards, joints and crevices should be anchored and sealed appropriately to prevent water ingress during cleaning.
There should be coving between the floor and the wall to prevent the accumulation of dust and dirt in the corners and crevices.
In areas where frequent wet cleaning methods are required, floors should be of a material that is unaffected by the agents likely to be used.
Floors that are particularly subject to traffic when wet e.g. kitchen and bathrooms should have a slip resistant surface but be easily cleaned.
No carpets in any clinical area of the Trust.
Wood, unsealed joints, carpets and tiles should be avoided as they may provide a reservoir for infectious organisms.
Finishes
Materials and finishes should be selected to minimise maintenance and be compatible with their intended function.
Building elements that require frequent redecoration or are difficult to service or clean should be avoided.
Special design consideration should be given to areas subject to heavy use e.g. entrances etc.
Finishes should be functional and compatible with the need for comfort, cleanliness and safety.
They should be free of fissures, joints and crevices to avoid retaining dirt and particles.
Fixtures and fittings
All finishing’s must facilitate cleaning and disinfection as necessary and be of a suitably high standard
Soft furnishings must be covered with an impervious material in all clinical areas to facilitate cleaning and disinfection as necessary
General Hand washing facilities
All en-suite facilities should have a hand wash basin for use by the patient.
All toilet facilities should have an hand wash basin
Overflows should not be provided as these are difficult to clean.
Taps should not be aligned to run directly into the drain aperture
All general hand wash basins should be sealed to a waterproof splash-back.
Hand drying facilities
Paper towel dispensers should be conveniently placed by all hand wash basins (clinical and non-clinical).
Hot hand dryers must not be used in clinical areas but may be considered in public areas.
Paper roll dispensers are not recommended for hand drying as they are difficult to tear off without contaminating the remaining roll.
Hands free waste bins, with appropriate coloured waste bags, should be provided by each wash hand basin.

Infection Prevention and Control in the Built Environment. Page 22 of 27 Version 1.1 March 2019
Heating and ventilation
Heating and ventilation grilles should be easily accessible for cleaning
There should be no ledges or ridges where dust can collect
Pipework in clinical areas should be encased to allow and facilitate cleaning, pipework running externally along a wall traps dust and is difficult to clean
Hot and cold water systems
Water storage tanks should have a programme of maintenance and cleaning approved by the Water Management Group.
Hot water supplies must be monitored by the Estates and Facilities team to ensure consistent high temperatures in compliance with the Water Management Policy
Dead legs in water systems should be avoided
HTM 71 storage (clinical rooms)
The benefits of HTM 71 modular storage are:
A single Stocking Point saving direct nursing time
Quicker Stock recognition
Improved stock rotation
Pre-determined stock levels held
Reduced risk of picking error
Reduced stock damage
Maximised storage – freeing space for other use
Wall mounted cupboards should have sloping tops as standard to aid cleaning and prevent items being stored on top of cupboards
In-patient bedrooms
Ideally should be arranged in pairs so that they share common services. All pipework and services should be located in a secure duct adjacent to the room and should only be accessible from the circulation area or non-service user area
Healthcare staff must have access to at least one side of the bed.
Doorways and circulation space must allow for trolleys and wheelchairs
Bedrooms should be a minimum of 15 m² including an en-suite facility.
Each bedroom should have a staff-call facility
A cleaner’s socket should be included within each room
Isolation facilities
Storage and ready access to clean PPE to be considered – ideally a lobby to assist staff to comply with hand hygiene and donning of PPE prior to entering the patients room and appropriate waste receptacles for its disposal once worn.
Clinical hand wash basins should be provided in addition to facilities provided for the patients use.
Isolation rooms should be single occupancy and have en-suite facilities
Removable ceilings are not advised in isolation rooms.
Extract ventilation recommended.
Windows should be able to be opened (restricted)
Observation window should have integral privacy blinds which can be controlled by both the patient and the staff.
Kitchens
In clinical areas the kitchen must be sited away from the clinical and dirty utility areas.
Avoid risks of cross contamination raw and cooked foods
Adequate storage – preferably stainless steel units
Main kitchens clear workflows essential and separate staff changing

Infection Prevention and Control in the Built Environment. Page 23 of 27 Version 1.1 March 2019
Lighting
Should be designed so that there are no ledges, ridges etc. where dust can gather easily, build up and then be dispersed if the light is knocked or moved.
Lighting units should be fully sealed for ease of cleaning.
Directional lighting e.g. examination lamps should be included in the cleaning schedule
Lighting should be sufficient in all areas to allow staff to undertake cleaning more effectively.
Lighting should be designed to permit easy changing of lamps and frequent cleaning.
Flush ceiling fittings are acceptable, but not open up-lights which accumulate dust.
Linen disposal
Facilities should be designed in to allow for easy disposal and storage of soiled linen in a secure area located near to the production of soiled linen to avoid unnecessary handling of soiled linen.
Space required to store linen skips etc.
Facilities for hand decontamination and storage of PPE required
Laundries
Laundry equipment should comply with the HTM 01-04 recommendations
Clinical hand wash sink required in addition to an equipment sink
Clear workflow from dirt to clean required
Secure storage for washing powder etc.
Sufficient space for ironing
Washing machine to have a sluice cycle and be able to achieve and hold the recommended temperatures
Nappy changing area
Facilities for the disposal of soiled nappies is required
The nappy changing area should have a surface that can be easily cleaned and disinfected.
Hand washing facilities should be available
Pipework siting and access
Pipework should be contained in a smooth surfaced box that is easy to clean.
Pipework sited along a wall can become a dust trap and be impossible to clean.
Play/children’s areas
Porous or fabric furniture must be avoided, vinyl upholstery is preferred.
All surfaces must be able to withstand regular cleaning with detergent and chlorine based disinfectants.
Radiators Wherever possible radiators should be accessible and cleanable. The use of Deep
Clean radiator guards are recommended for ease of cleaning and maintenance.
In clinical areas supply pipework should be concealed.
In all cases the installation should be neat and easy to clean and maintain. Radiators should be placed high enough on a wall to enable the area underneath to be cleaned.
Sanitary facilities WCs, bathrooms and showers should be designed to be easily cleaned and
maintained
Wash hand basins, soap and paper towels should be provided adjacent to WCs
Shower heads should be regularly cleaned and descaled to prevent possibility of bacterial colonisation.
Baths should be easy to clean
In wet rooms, high quality water-resistant cladding should be used on the walls to prevent mould. See HBN 00-10 and HBN 00-02
Fixtures such as shower seats etc. should be easy to clean
In wet rooms, high quality water-resistant cladding should be used on the walls to prevent mould.
Single accessible bedroom
Should be at least 17m² to 19m² including the ensuite to accommodate a person in a wheelchair or who may require assistance.
Variable height bed should be considered. (Consider storage for when this type of bed is not required).

Infection Prevention and Control in the Built Environment. Page 24 of 27 Version 1.1 March 2019
Sinks and disposal facilities
Disposal facilities should be provided in areas where dirty water is disposed e.g. dirty utility rooms, cleaners cupboards etc.
Dirty water must not be disposed of in hand wash sinks.
Soap dispensers Liquid soap dispensers should be wall-mounted at all hand wash basins and be
designed to be operated without contamination from the users hands coming into direct contact with the dispensing mechanism.
Dispensers should be of a single cartridge design and not the top-up refillable type
Dispensers must be smooth for ease of cleaning
Soft furnishings All upholstery should be water/stain resistant and capable of withstanding disinfection with chlorine based disinfectant. Vinyl is preferable.
Chairs/treatment chairs/couches must have impervious covers.
Specimen W.C. If required it requires direct access to a dirty utility room i.e. a testing hatch for testing to reduce carriage of body fluids in the healthcare environment.
Staff changing facilities
To enable staff to change out of their uniform or change contaminated clothing following a blood or body fluid spill.
Access to a shower required – cleaning and regular flushing to be included in the cleaning schedule.
Sufficient storage i.e. lockers for outdoor clothing etc.
Hand wash facilities
Storage and distribution of
water
Preventative measures include:
Routine inspections of water storage tanks with cleaning required
Identifying and removing dead-legs
Temperature monitoring and control – keeping cold water systems cold and hot water systems hot to reduce risks of Legionella
Regular flushing of seldom used outlets
Water fittings (washers etc.) should not support microbiological growth
Use of flexible hoses should be avoided – where these must be used e.g. hi-lo baths they must be lined with a suitable alternative to ethylene propylene diene monometer (EPDM) and be WRAS-approved.
Storage The need for sufficient storage should not be underestimated – this can have implications for both clinical practice and infection prevention and control.
Storage
(patient possessions)
Storage areas should be appropriate to the patients’ needs and be easy to clean and maintain.
Storage for small and bulky items needs to be considered along with secure storage for valuable items.
Storage should be sufficient in order to minimise clutter and enable environmental cleaning.
Louvre doors must not be fitted as they are difficult to clean.
Risk assessment required in mental health and learning disability units to determine the type of furniture.

Infection Prevention and Control in the Built Environment. Page 25 of 27 Version 1.1 March 2019
Treatment room / dispensary
Minimum size 15m² - If privacy curtains are required around examination couches/chairs they should be disposable and replaced at least every six months or immediately if visibly soiled – this should be included in the cleaning schedule. Curtain tracks must be included in the cleaning schedule.
Work surfaces should be easy to clean, any joints must be butt joined and joining strips must not be used.
Adequate storage facilities must be provided to ensure work surfaces are kept clear.
HTM71 compliant furnishing/storage facilities
Visitors toilets Facilities for the disposal of sanitary waste should be provided where applicable
The number of facilities (toilets/urinals/hand wash basins) should be sufficient for the size of the facility
Hot air hand dryers may be used unless the facility is situated close to patient areas where noise from the dryers may be a problem.
Ventilation ductwork
All ventilation plant should meet a minimum requirement in terms of control of Legionella and safe access for inspection and maintenance.
All ventilation plant should be inspected annually and the performance of all critical ventilation systems should be verified annually.
Duct work internal surfaces must be able to be cleaned regularly to prevent transmission of dust, dirt and organic material which are valuable nutrients for microorganisms to vulnerable patients.
Walls Smooth and impervious surfaces must be used for walls
Surfaces near plumbing fixtures must be smooth, non-porous and water resistant.
Waste disposal room
Healthcare waste must be stored in a secure, cleanable area away from patient flow areas but close to the production of waste to avoid unnecessary handling of waste, used for that purpose only including:
The temporary storage of supplies and equipment that have been removed for cleaning, reprocessing or disposal e.g. used linen, waste bags and full sharps bins etc.
Size should take into consideration predicted levels and types of waste (including waste segregation) to be generated and the frequency of collections.
Must be secure and inaccessible to the public
Hand washing facilities required
Best located at entrances to wards or departments with access from both ward and hospital corridor to facilitate collection by authorised personnel only, separate exit should be via an external door. Waste can then be stored without taking up valuable space in the dirty utility room.
Waste receptacles
The size required needs to be in line with the quantity of waste generated.
Waste receptacles should be foot operated only (not possible to open them by hand) and should be easy to clean
Lids need to be capable of being cleaned and disinfected and colour coded to indicate type of waste for disposal e.g. black for household waste and orange for clinical waste etc.
Waste bins should be approved by IPC and Facilities Manager prior to orders being placed.

Infection Prevention and Control in the Built Environment. Page 26 of 27 Version 1.1 March 2019
Water fittings
Water fittings should not support microbiological growth
All fittings should satisfy the requirements of the Water Supply (Water Fittings) Regulations 1999.
The use of flexible hosed should be avoided. Where flexible hoses must be used e.g. hi-lo baths they must be lined with a suitable alternative to EPDM as well as being WRAS approved.
Water coolers Only plumbed in water coolers to be used, bottled coolers increase risks of contamination.
Windows Window dressings must be easy to clean
Blinds must be of a standard agreed with IPCT.

Infection Prevention and Control in the Built Environment. Page 27 of 27 Version 1.1 March 2019
Standard Operating Procedure Details
Review and Amendment History
Version Date Description of Change
1.1 Mar 2019 Procedure reviewed as required. No changes required. All references checked & updated
1.0 Apr 2016 New Procedure established to supplement Infection Control Assurance Policy
Unique Identifier for this SOP is BCPFT-COI-POL-05-15
State if SOP is New or Revised Revised
Policy Category Control of Infection
Executive Director whose portfolio this SOP comes under
Executive Director of Nursing, AHPs and Governance
Policy Lead/Author Job titles only
Infection Prevention and Control Team
Committee/Group Responsible for Approval of this SOP
Infection Prevention and Control Committee
Month/year consultation process completed
April 2019
Month/year SOP was approved April 2019
Next review due April 2022
Disclosure Status ‘B’ can be disclosed to patients and the public