infant spring 12 without graphics
DESCRIPTION
Nursing Buddies.... No graphic PPTTRANSCRIPT
NUR 2310 Pediatric Nursing Concepts
ANDREA STORRIE,MSN, CPNP
GROWTH AND DEVELOPMENT
Unit 1Developmental influences on child
health promotion

One hundred years from nowit will not matter
What kind of car I drove.What kind of house I lived in.
How much money I had in my bank account.
Nor what my clothes looked like.But the world may be
a little better Because I was important in the life of a child.

CHILDREN’S HEALTHA CHANGING PARADIGM
• Sixty years ago leading causes of death
were infections and catastrophic disease
• Today’s leading causes are complications of low birth weight, congenital anomalies and injury
• Antibiotics, immunizations and cancer advances changed the paradigm
• How do pediatric nurses function now and how will the future change pediatric nsg.?

GROWTH AND DEVELOPMENT
GROWTH
– Increase in the size and number of cells resulting in increased size and/or weight of a part
– Quantitative change

GROWTH AND DEVELOPMENT
DEVELOPMENT
• Gradual change and expansion progressing from lower to advanced complexity. The emerging and expanding of individual capacities
• Qualitative change
G & D CONTINUEDMATURATION
– An increase in competence and adaptabilityDIFFERENTIATION
– Process by which early cell structures are systemically modified to achieve specific properties.
– A development from simple to more complex activities and functions.
– All four of these processes are interrelated simultaneously.
– None occur without the other.

BASIC ASSUMPTIONS ABOUT CHILD DEVELOPMENT
• Development is orderly
• Development has direction
• Development is complex
• Each child is unique
• Development necessitates practice
• Development requires a role model
BASIC ASSUMPTIONS CON’T
• Development requires energy to be expended
• Children develop through conflict and adaptation
• Development goes through cycles
• Development has sensitive periods

DEVELOPMENTAL INFLUENCES
PATTERNS OF GROWTH & DEVELOPMENT:
DIRECTIONAL TRENDS
– CEPHALOCAUDAL
– PROXIMODISTAL (NEAR TO FAR)
– DIFFERENTIATION
– GENERAL (MASS) TO SPECIFIC
FACTORS INFLUENCING GROWTH AND DEVELOPMENT
• Heredity• Neuroendocrine
factors• Nutrition• Interpersonal
relationships • Socioeconomic
factors
• Disease• Environmental
hazards• Stress• Mass media
– AAP

ERIKSON’S STAGES OF PERSONALITY DEVELOPMENT
• Involves a specific conflict or developmental task
• Infant - Trust vs. Mistrust
• Toddler - Autonomy vs. Shame and Doubt
• Preschooler - Initiative vs. Guilt
• Schoolager - Industry vs. Inferiority
• Adolescent - Identity vs. Role Confusion
• Adulthood- Intimacy vs. Isolation
Piaget’s Stages of Cognitive Development
• Sensorimotor (Birth to 2 years)
progress from reflex to sense of cause and effect
• Preoperational (2 to 7 years)
egocentric - thinking is concrete and tangible
• Concrete operational (7 to 11 years)increasingly logical and coherent - develop conservation
• Formal operations (11 to adulthood)think abstractly - adaptable and flexible
FREUD - PSYCHOSEXUAL DEVELOPMENT
• Oral stage - birth to one year
• Anal stage - one to three years
• Phallic stage - three to six years
• Latency period - six to twelve years
• Genital period - age twelve and over
DURING CHILDHOOD, CERTAIN REGIONS OF THE BODY ASSUME A PROMINENT
PSYCHOLOGIC SIGNIFICANCE WHICH SHIFTS FROM ONE PART OF THE BODY TO ANOTHER
PLAY
• Universal medium for learning
• Children learn what no one else can teach them
• Play is the work of children
http://www.brightcove.tv/title.jsp?title=894297564&channel=825544798

CLASSIFICATION OF PLAY
Practice play referred to as functional or sensorimotor play
Symbolic play
Games

SOCIAL ASPECTS OF PLAY
• Solitary play
• Onlooker play
• Parallel play
• Associative play
• Cooperative play

FUNCTIONS OF PLAY• Physical development• Cognitive development• Emotional
development• Social development• Moral development• Therapeutic value

Anticipatory Guidance
• Parents need to know how to a provide safe environment for their child
• Need to know what to expect before it happens
• Based on child's developmental level
• Awareness of the child’s changing capabilities allows the parents to be more alert and reactive to safety hazards the child is likely to encounter
SAFETY PRECAUTIONS WITH INFANT TOYS
• Select toys that are smooth and rounded and made of wood or plastic
• Plastic toys should be made of tough and resilient material
• Avoid fuzzy and furry stuffed animals
• Inspect toys for small removable parts
• Check toys for toxic paint
• Supervise infants if playing with paper, string, or cloth
PEDIATRIC UNIT SAFETY PRECAUTIONS
• Baby proof room
• Provide only age appropriate toys
• Remove all medical equipment except when used for treatments
• Cords out of reach
• Outlets covered
• Crib rails up to highest adjustment
• Maintain physical contact if infant or toddler is on an unguarded surface such as a scale or treatment table
• NEVER LEAVE UNATTENDED NEAR WATER !
CHILDREN’S RESPONSE TO HOSPITALIZATION
• Separation Anxiety:
– Protest: crying, screaming, wrongly viewed as misbehavior
– Despair: decreased activity or withdrawal, often viewed as a good thing or “settling in”
– Denial or detachment: starts to play & form other attachments, resigned not content
CHILDREN’S RESPONSE CON’T
• Fear of the unknown
• Fear of pain or mutilation
• Loss of control
• Anger
• Guilt
• Regression

PARENTAL STRESSORS
• Fear of the unknown
• New environment
• Separation from child
• Guilt
• Financial burden
• Fear that child will suffer or even die
• Fatigue
• work, care of other children, distance to hospital
COMMUNICATING WITH CHILDREN
• Allow time to feel comfortable
• Avoid rapid advance or other threatening gestures
• Talk with parent if child is initially shy
• Communicate through transition objects such as dolls or puppets
• Assume an eye level position

COMMUNICATION CON’T.
– Speak in a quiet, unhurried, confident tone of voice
– Speak clearly, be specific, and use simple words and short sentences
– State directions and suggestions positively
– Offer a choice only if one exists
– Be honest
– Allow time to express concerns and fears
– Give older child the chance to talk without parents present
GUIDELINES FOR ADMISSION
• Introductions
• Orient child and family
• Apply identification
• Explain hospital rules
• Perform nursing admission history
• Take baseline vital signs & obtain specimens
• Support child and parents as necessary

HEALTH HISTORY
• Immunizations current?
• Well Child Care?
• Sick Care only?
• Who is the provider?
• What routines are normal for the child?
– Bedtime ritual? Read a story? Rock?
IMMUNIZATIONS
http://www.cdc.gov/vaccines/recs/schedules/child-schedule.htm#printable
http://www.cdc.gov/vaccines/pubs/pinkbook/pink-chapters.htm
http://www.flshots.com/

ASSESSMENT GUIDELINES
• Perform in an appropriate, nonthreatening area• Provide time for play & getting acquainted• Observe for readiness to cooperate• Avoid prolonged explanations about procedures• Involve child and parent in exam process• Use a firm, direct approach• Proceed with exam in an organized sequence• Reassure child throughout exam & use praise• Discuss findings with the family
Pediatric Assessment
• Toddlers are the most challenging to examine
– Sequence is flexible
• What are some differences of a pediatric assessment vs. the assessment of an adult?
• Lymph nodes are often palpable in healthy infants and children up to 12 years or age (cervical, axillary, inguinal, and occipital areas)

PLAGIOCEPHALY (POSITIONAL)
• Misshapen head • Back of head is flattened due to constantly being
placed in supine position• Infants need belly time• Treatment
– DOC band– Need to be worn 23 hours a day– Frequent adjustments

PLAGIOCEPHALY (POSITIONAL)

PLAGIOCEPHALY (POSITIONAL)

PERFORMING A PEDIATRIC PROCEDURE
Before the procedure
– Offer ways to cope with pain or discomfort
– Use developmentally appropriate words
– Give choices when possible
– Be sure consent form is signed
– Always wash hands thoroughly
During the procedure
Talk to the child if he/she desires
Keep the child informed of progress
Tell the child when the ”worst is over”
PERFORMING A PEDIATRIC
PROCEDURE
PED PROCEDURES CON’T
After the procedure
– Praise the child for attempting to cooperate
– Provide an opportunity to vent feelings
– Reunite the child with parents
– Reward the child in an age-appropriate way
– Record the process and it’s outcomes
MEDICATION ADMINISTRATION
“8” rights– Patient, Order, med., dose, time, route, documentation, &
attitude
– Oral medications– Intramuscular administration– Vastus lateralis– Intravenous administration– NG, OG, or Gastrostomy administration– Rectal Administration
ADDITIONAL PROCEDURES WITH VARIATIONS
• Measurement of I & O
• Parenteral fluid therapy
• Inhalation therapy
• Chest physiotherapy
• Postural drainage
• Gavage or gastrostomy feeding
• Ostomies
BIOLOGICAL DEVELOPMENT
• GAINS 5-7 OUNCES WEEKLY FOR 1ST 5-6 MO.
• DOUBLES BIRTH WEIGHT BY 6 MO.
• TRIPLES BIRTH WEIGHT BY 12 MO
• BIRTH LENGTH INCREASES 50% BY 12 MO.
• HEAD SIZE INCREASES 33% BY 12 MO.

BIOLOGICAL DEVELOPMENT
• BRAIN INCREASES IN WEIGHT BY 2 ½ TIMES
• ORGAN SYSTEMS BEGIN TO MATURE
• GROWTH CHARTS ARE MOST ACCURATE ASSESSMENT OF CHILD’S GROWTH

BIOLOGICAL DEVELOPMENT
• BRAIN INCREASES IN WEIGHT BY 2 ½ TIMES
• ORGAN SYSTEMS BEGIN TO MATURE
• GROWTH CHARTS ARE MOST ACCURATE ASSESSMENT OF CHILD’S GROWTH

GROSS MOTOR MILESTONES• HEAD CONTROL ESTABLISHED @ 4-6 MONTHS• TURNS ABD. TO BACK @ 4-5 MONTHS• TURNS BACK TO ABD. @ 6-7 MONTHS• SITS WITHOUT SUPPORT @ 8-9 MO.• CRAWLS AND PULLS UP @ 8-9 MO.• STANDS ALONE @ 10-12 MO.• WALKS W/ ONE HAND HELD 10-12 M• WALKS INDEPENDENTLY 12-15 MO.
FINE MOTOR MILESTONES
• 1 MONTH - HANDS FISTED – PALMAR GRASP
• 3 MONTHS - CAN HOLD RATTLE
• 4-5 MONTHS – BEGINS REACHING & GRASPING WITH PALMS
• 6-7 MONTHS – PICKS UP OBJECT WELL -TRANSFERS OBJECTS FROM HAND TO HAND

FINE MOTOR MILESTONES
• 8-9 MONTHS - PINCER GRASP DEVELOPS, REACHES FOR TOYS, RAKES FOR OBJECTS
• 10-12 MONTHS – RELEASES CUBE INTO CUP AFTER DEMO. – PINCER GRASP COMPLETE
– FEED SELF WITH SPOON
SOCIAL MILESTONES
• SMILES RESPONSIVELY TO STIMULI @ 6-8 weeks.
• SHOWS FEAR AND ANGER @ 4-8 MO.
• SMILES AT SELF IN MIRROR @ 6-7 MO– PLAYS PEEK- A -BOO
SOCIAL MILESTONES
• STRANGER ANXIETY HEIGHTENS @ 6-8 MO.
• QUIETS SELF AND QUIETED BY MUSIC @ 10-12 MO.
• HAS MOOD CHANGES @ 10-12 MO.
LANGUAGE MILESTONES
• RESPONDS TO SOUNDS @ BIRTH
• COOS, BABBLES- 3 MOS
• BABBLING COMMON @ 4-5 MONTHS
• MAKES VOWEL SOUNDS “ee, ah, ooh”- 4-5 months

LANGUAGE MILESTONES
• BELLY LAUGHS & TALKS TO TOYS 6-7 MO.• First few words have meaning- 8-9 mos “mama, dada”
– Understands simple demands- “wave bye bye”– Comprehends –”No,no”
• 10 -12 months says “mama or dada”• By 1 year recognizes objects by names
• CAN SAY 3-5 WORDS WITH MEANING BY 1 YEAR– Knows own name– Enjoys jabbering
PSYCHOSOCIAL DEVELOPMENT-ERIKSON
• TRUST VS. MISTRUST – THE BASIC DEVELOPMENTAL TASK OF INFANCY
– TRUST OF SELF, OTHERS , AND THE WORLD
– TRUST DEVELOPS WHEN INFANT’S NEEDS ARE CONSISTENTLY MET
– IF NEEDS NOT CONSISTENTLY MET MISTRUST OF WORLD DEVELOPS
COGNITIVE DEVELOPMENTPIAGET
• SENSORIMOTOR – INITIALLY RELATES TO WORLD THROUGH REFLEXES
– Realize others besides themselves control the environment
– Object permanence by 9 months• One of the key tasks of this stage
• Seen in the development of separation anxiety

COGNITIVE DEVELOPMENTPIAGET
– FOUR STAGES DURING INFANCY• USE OF REFLEXES
– Sucking, rooting, grasping
• PRIMARY CIRCULAR RESPONSE (1-4 months)– Replacement of reflexive behaviors with voluntary acts
• SECONDARY CIRCULAR RESPONSE-Continuation of primary lasts until 8 months- Primary circular reactions are repeated and prolonged for the response that
results
• COORDINATION OF SECONDARY SCHEMAS– Use previous behavioral achievements primarily as the foundation for adding
new intellectual skills– Object permanence
Development of Body Image
• Parallels sensorimotor development• As physical needs are met they feel comfort and satisfaction with
their body • Messages convey by caregivers reinforce these feelings• Object permanence is basic to development of self image• By the end of the first year they realize they are distinct from
their parents– At the same time is increased interest in their image– Smile at themselves in the mirror
IMMUNIZATIONS REQUIRED FIRST 6 MONTHS
• DTaP SERIES
• HEPATITIS B SERIES
• POLIO SERIES
• STREP PNUEMOCOCCUS SERIES (Prevnar)
• H. INFLUENZA B- HIB SERIES
• Rotavirus vaccine

IMMUNIZATIONS REQUIRED@ 12-15 MONTHS
• BOOSTERS
– DTAP
– PNUEMOCOCCUS
– HIB
• MMR
• VARICELLA
INFANT NUTRITION• HUMAN MILK MOST DESIRABLE COMPLETE DIET FOR THE FIRST 6 MONTHS
• BREAST MILK OR FORMULA UNTIL 12 MONTHS
• IRON SUPPLEMENTS @ 4-6MO FOR BREAST FED BABIESD/T DEPLETED IRON STORES
• FORMULA BABIES MAY HAVE ENOUGH FROM DIET
• NO BOTTLES IN MICROWAVE TO HEAT
• NO SOLIDS UNTIL 4-6 MONTHS
– EARLY EXPOSURE TO SOLIDS CAN PRODUCE ALLERGIES– EXTRUSION REFLEX IS STRONG IN YOUNG INFANTS

ADDITION OF SOLID FOODS• IRON FORTIFIED RICE CEREAL USUALLY FIRST
• FRUIT JUICES CAN BE ADDED AFTER 6 MONTHS
• STRAINED VEGETABLES USUALLY NEXT
• FOLLOWED BY STRAINED FRUITS, THEN MEATS
• EGGS, COW’S MILK, AND CITRUS ARE THE MOST COMMON INFANT ALLERGENS. DELAY INTRODUCTION UNTIL INFANT 12 MONTHS OLD
INTRODUCING SOLID FOODS TO INFANTS
• INTRODUCE WHEN INFANT IS HUNGRY
• BEGIN BY PUSHING FOOD TO BACK OF TONGUE BECAUSE OF EXTRUSION REFLEX
• USE A SMALL SPOON WITH A STRAIGHT HANDLE
• BEGIN WITH 1-2 TEASPOONS OF FOOD, INCREASE GRADUALLY
• INTRODUCE FOODS ONE AT A TIME WITH 4-7 DAYS BETWEEN ADDING NEW FOODS

• AS AMOUNT OF SOLID FOOD INCREASES, DECREASE AMOUNT OF FORMULA TO PREVENT OVERFEEDING
• DO NOT INTRODUCE FOODS BY MIXING WITH FORMULA IN THE BOTTLE
• EARLY FEEDING EXPERIENCES ARE SLOPPY
• CHILDREN CAN’T BE PRESSURED INTO EATING NEATLY UNTIL THEY HAVE MANIPULATIVE SKILLS
PLAY
• SOLITARY OR ONE-SIDED PLAY
• OVER THE YEAR BECOMES MORE SOPHISTICATED AND INTERDEPENDENT
• SENSORY STIMULATION IS VERY IMPORTANT
• INFANTS NEED TO BE PLAYED WITH, NOT MERELY ALLOWED TO PLAY
CLEFT LIP & CLEFT PALATE
• MULTIFACTOR ETIOLOGY
• TENDS TO RUN IN FAMILIES
• ENVIRONMENTAL TERATOGENS MAY PLAY A ROLE
• CHROMOSOMAL ANOMALIES OFTEN HAVE CLEFTS AS A FEATURE
• MATERNAL SMOKING IN 1ST TRIMESTER ASSOCIATED WITH 10 % OF CASES
• APPEARS MOST OFTEN IN ASIAN AND NATIVE AMERICAN INFANTS - LEAST IN AFRICAN-AMERICAN
• Maternal intake of folic acid may prevent (NIH, 2007)

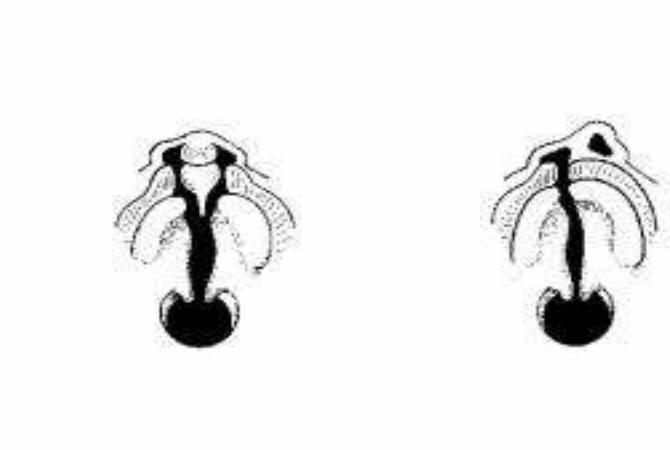
CLEFT LIP & CLEFT PALATE
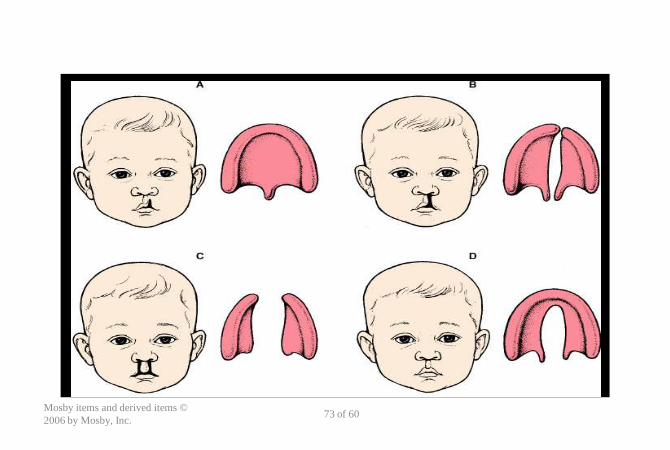
• PATHOPHYSIOLOGY- FAILURE OF THE MAXILLARY AND PREMAXILLARY PROCESSES TO MEET AND FUSE. NOTHING IS MISSING, ALL THE PIECES ARE THERE.
• CAN BE INCOMPLETE OR COMPLETE
• CLEFT PALATE CAN BE MISSED. FULL VISUALIZATION AND PALPATION OF THE PALATE NEEDED DURING NEWBORN EXAMINATIONS
• CLEFT LIP CAN BE UNILATERAL OR BILATERAL– EXTENT OF CLEFT AND NASAL DEFORMITY IS VARIABLE

CLEFT LIP & CLEFT PALATE
• SURGICAL TREATMENT
– CLEFT LIP REPAIRED BY AGE 3 TO 6 MO
– CLEFT PALATE REPAIRED AT 6-24 MO.
• MULTIDISCIPLINARY TEAM APPROACH D/T PROBLEMS WITH SPEECH, ORTHODONTIA AND EARS/SINUSES
CLEFT LIP & CLEFT PALATE
• NURSING CARE- CLEFT LIP REPAIR
– PREOP- DEAL WITH FEEDING PROBLEMS
– ENCOURAGE PARENT/INFANT BONDING
– Z-PLASTY REPAIR OF LIP MINIMIZES NOTCHING
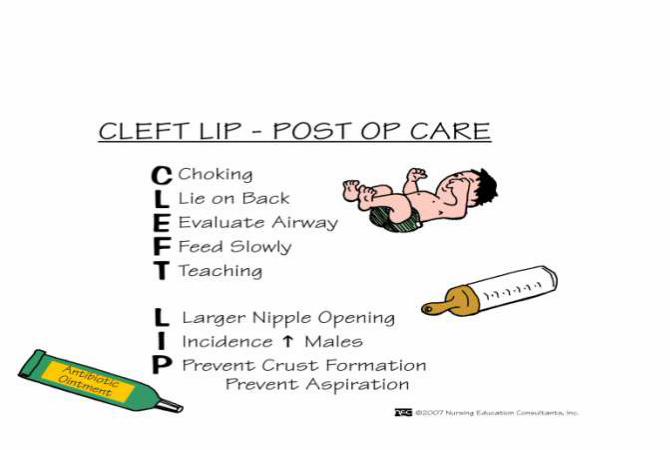
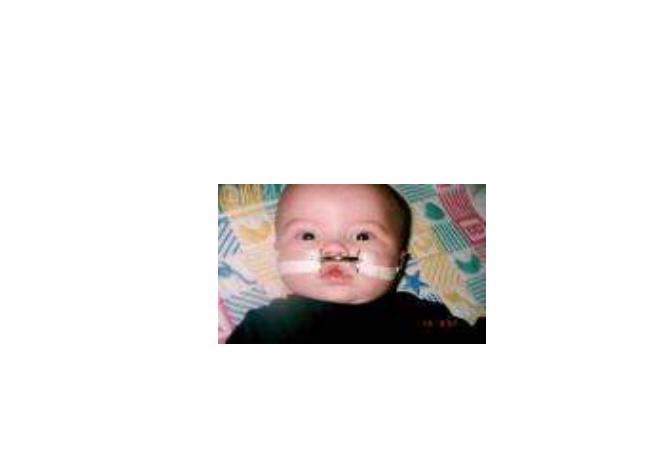
– POST OP- PREVENT INFANT CRYING, CLEAN SUTURE LINE, MAINTAIN SUPINE POSITIONING, MAINTAIN ELBOW RESTRAINTS AND LIP BOW (LOGAN BOW)
Mosby items and derived items ©
2006 by Mosby, Inc.73 of 60

Cleft Lip Repair

CLEFT LIP & CLEFT PALATE
• NURSING CARE- CLEFT PALATE REPAIR
– PERFORMED BEFORE FAULTY SPEECH HABITS OCCUR
– PREOP- DEAL WITH FEEDING PROBLEMS
– POST OP- PREVENT INFANT CRYING, ASSESS FOR PAIN, PREVENT CHILD FROM INSERTING HARD OR POINTED OBJECTS IN MOUTH AND AVOID HARD FOODS
– NEED TO MONITOR RESPIRATORY STATUS CLOSELY
– OBSERVE FEEDING ONCE RESUMED- I & O
• Liquids to soft diet within 48 hours

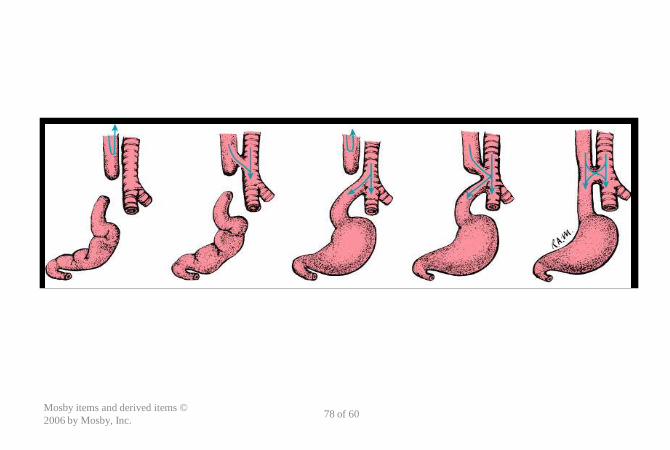
ESOPHAGEAL ATRESIA WITH TRACHEAL-ESOPHAGEAL FISTULA
• PATHOPHYSIOLOGY:
• FAILURE OF THE ESOPHAGUS TO FORM AS A CONTINUOUS PASSAGE
• THE PROXIMAL SEGMENT TERMINATES INTO A BLIND POUCH
• THE DISTAL SEGMENT IS CONNECTED TO THE TRACHEA OR THE PRIMARY BRONCHUS BY A SHORT FISTULA

Mosby items and derived items ©
2006 by Mosby, Inc.78 of 60

CLINICAL MANIFESTATIONS
– EXCESSIVE SALIVATION AND DROOLING
– THE THREE “C’s”= COUGH, CHOKING AND CYANOSIS
– APNEA
– RESPIRATORY DISTRESS WITH FEEDS
– ABDOMINAL DISTENTION

ESOPHAGEAL ATRESIA WITH TRACHEAL-ESOPHAGEAL FISTULA
• THERAPEUTIC MANAGEMENT– PREVENTION OF ASPIRATION AND PNEUMONIA
• NPO AND IV FLUIDS
• “POUCH TUBE” TO REMOVE SECRETIONS
• ELEVATE HEAD
• GASTROSTOMY TO DRAIN STOMACH CONTENTS (decompression)
- SURGICAL CORRECTION
ESOPHAGEAL ATRESIA WITH TRACHEAL-ESOPHAGEAL FISTULA
• NURSING CARE – PREOP
– IF SUSPECTED MAKE INFANT NPO
– ELEVATE HEAD
– CLEAR SECRETIONS WITH CONTINUOUS SUCTION
– OXYGEN FOR RESPIRATORY DISTRESS
ESOPHAGEAL ATRESIA WITH TRACHEAL-ESOPHAGEAL FISTULA
• NURSING CARE- POST OP
– MAINTAIN GASTROSTOMY TUBE
– If a staged repair- care of cervical esphagostomy
– SLOW RETURN OF ORAL FEEDS
– DISCHARGE AFTER ORAL FEEDINGS RESUMED AND G-TUBE REMOVED

DIAPHRAGMATIC HERNIA
• FAILURE OF DIAPHRAGM TO CLOSE PRENATALLY ALLOWING ABDOMINAL ORGANS TO BE DISPLACED INTO THE ABDOMEN
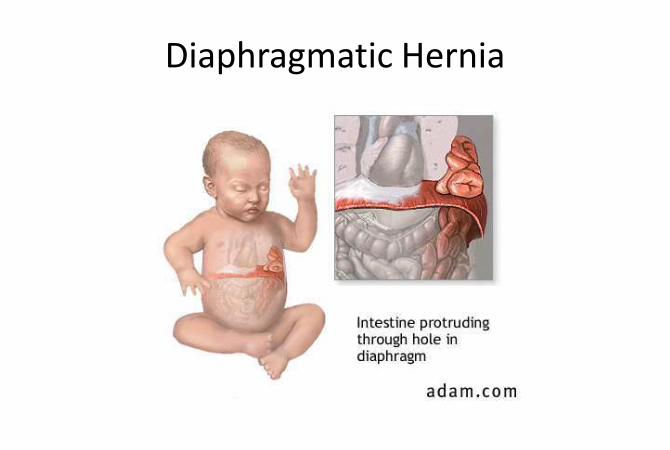
Diaphragmatic Hernia
DIAPHRAGMATIC HERNIA
• DEFECT ON IS USUALLY ON THE LEFT SIDE. BOWEL ENTERS THE CHEST CAVITY AND PUSHES HEART TO THE RIGHT. IMPEDES GROWTH OF THE LUNG
• AFTER BIRTH THE BOWEL FILLS WITH AIR WHICH FURTHER COMPROMISES BREATHING AND CIRCULATION

DIAPHRAGMATIC HERNIA• CLINICAL MANIFESTATIONS
– HEART SOUNDS LOUDER ON THE RIGHT
– SCAPHOID ABDOMEN
– BOWEL SOUNDS IN CHEST
– INCREASING RESPIRATORY DISTRESS
• STABILIZATION PRE-OP– RESUSCITATED WITH ET TUBE NOT MASK
– ELEVATE HEAD OF BED
– AFFECTED SIDE DOWN
– NPO AND GASTRIC DECOMPRESSION (NG TUBE)

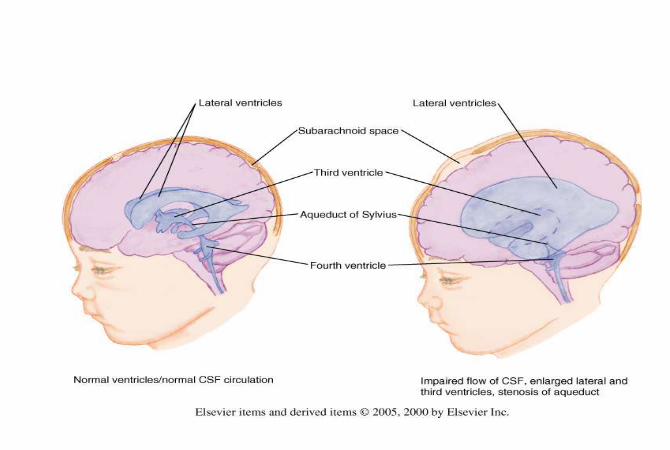
HYDROCEPHALUS
• IMBALANCE BETWEEN PRODUCTION AND ABSORPTION OF CSF CAUSING ACCUMULATION IN VENTRICLES– Communicating
– Noncommunicating
• FOUND EARLY ON WELL EXAMS BY SERIALLY MEASURING AND GRAPHING HEAD CIRCUMFERENCES
• VERY OFTEN ASSOCIATED WITH MYELOMENINGOCELE


HYDROCEPHALUS
• EARLY PHYSICAL SIGNS– BULGING FONTANELS
– DILATED SCALP VEINS
– SEPARATED SUTURE LINES
• LATE PHYSICAL SIGNS– SETTING SUN SIGN- SCLERA VISIBLE ABOVE IRIS
– SHRILL HIGH PITCHED CRY DUE TO ICP
– OPISTHOTONOS

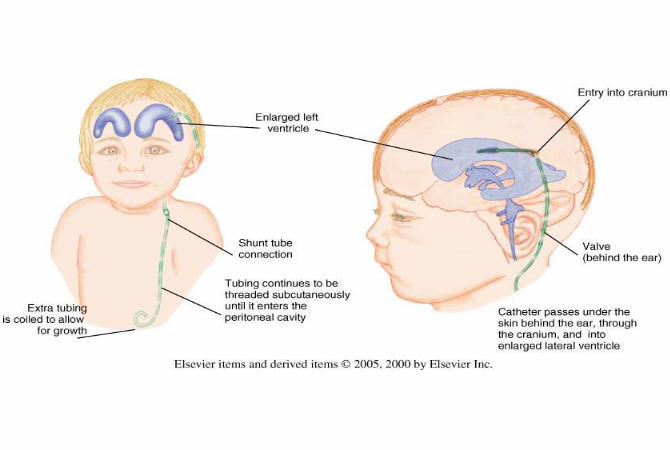
HYDROCEPHALUS
• VENTRICULAR-PERITONEAL SHUNT USUALLY NEEDED (VP shunt)
• Infection is greatest hazard
• Monitor closely for signs of infection and ICP
• Pain management
• Educate parents on signs of infection and increases ICP
• Teach parents how to change dressing

NEURAL TUBE DEFECTS
• SPINAL BIFIDA OCCULTA
– DEFECT PRESENT IN VERTEBRA
– NO SAC PRESENT
– NO OBVIOUS DEFICITS BUT “SOFT” SIGNS MAY BE PRESENT

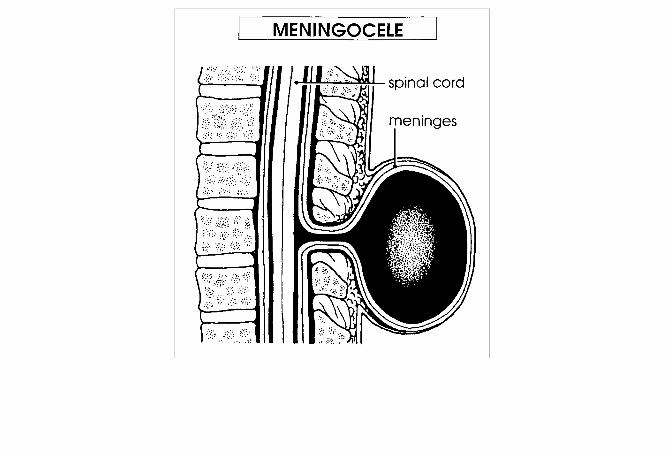
Spina Bifida Cystica
• Meningocele
• Sac contains meninges and spinal fluid but no neural elements
• Not associated with neurological defect
Spinal Bifida Cystica
• Myelomeningocele
• Sac contains meninges, spinal fluid, and nerves
• Manifestations relate to degree of defect, which is determined by the level of the lesion


NEURAL TUBE DEFECTS
• CAN BE DETECTED BY ULTRASOUND
• CAN BE DETECTED BY AFP
• INITIAL CARE
– PREVENTION OF INFECTION
– NEUROLOGIC ASSESSMENT
– DEALING WITH IMPACT ON FAMILY

NEURAL TUBE DEFECTS
• MULTIDISCIPLINARY APPROACH
– NEUROLOGICAL AND NEUROSURGICAL EVALUATION
– ORTHOPEDIC EVALUATION
– GENITOURINARY EVALUATION
– GASTROINTESTINAL (BOWEL CONTROL) EVALUATION

Nursing Considerations
• After birth:
– Prone positioning
– Radiant warmer to maintain temp without clothing
– Application of moist, nonadherent sterile dressing over sac
– Prevent infection

Nursing Considerations
• Post op care same as any surgical procedure
• Latex allergy precautions
• Family support
• Education
DEVELOPMENTAL DYPLASIA OF THE HIP
• HIP JOINT INSTABILITY
• MULTIFACTORAL ETIOLOGY
• FRANK BREECH PRESENTATION HAS HIGH ASSOCIATION WITH D.D.H.

DEVELOPMENTAL DYPLASIA OF THE HIP
• DIAGNOSTIC EVALUATION
– POSITIVE BARLOW OR ORTOLANI MANEUVERS DURING ASSESSMENTS
– RESTRICTED ABDUCTION
– ASYMMETRICAL SKIN FOLDS ON POSTERIOR THIGHS
– APPARENT FEMUR SHORTENING
– DDH

DEVELOPMENTAL DYPLASIA OF THE HIP
• THERAPEUTIC MANAGEMENT
– “DOUBLE DIAPER”
– PAVLIK HARNESS
– HIP SPICA CAST
• AVOID INDENTING WET CAST WITH FINGERS. USE FLATS OF HANDS
• DO NOT PULL ON ABDUCTION BAR
• PROTECT CAST FROM SOILING

Pavlik Harness

Spica Cast
CLUB FOOT
• FOOT TWISTED OUT OF THE NORMAL POSITION
• EXACT CAUSE NOT KNOWN
• UNILATERAL CLUB FOOT IS MORE COMMON
• IF MILD TREATED WITH EXERCISES
• IF MORE INVOLVED SERIAL CASTING IS PERFORMED
• IF MAXIMUM CORRECTION IS NOT ACHIEVED 3-6 MO., SURGERY FOLLOWS
• LONG-TERM FOLLOW UP INDICATED
CLUB FOOT
• Serial casting is begun immediately
• Correction usually takes 8 to 12 weeks
• Severe case or cases in which casting does not correct deformity require surgery
– Done between 4 months and 1 year of age


Care of child with a cast
• Assessments– Circulation
– Sensation
– Movement
• Interventions– Elevate limb
– Avoid indenting the cast while it is drying
– Parent education
IRON DEFICIENCY ANEMIA ANEMIA CAUSED BY INADEQUATE SUPPLY OF DIETARY IRON
MATERNAL IRON STORES ADEQUATE FOR 4-6 MONTHS (FULL-TERM) AND 2-3 MONTHS (PREEMIE)
TREATMENT IRON FORTIFIED FORMULA ORAL IRON SUPPLEMENT VITAMIN C DECREASE WHOLE MILK AND ADD Iron Fortified CEREALS,
VEGETABLES, AND MEATS
IRON DEFICIENCY ANEMIA
ANEMIA CAUSED BY INADEQUATE SUPPLY OF DIETARY IRON
MATERNAL IRON STORES ADEQUATE FOR 4-6 MONTHS (FULL-TERM) AND 2-3 MONTHS (PREEMIE)
TREATMENT IRON FORTIFIED FORMULA ORAL IRON SUPPLEMENT VITAMIN C DECREASE WHOLE MILK AND ADD Iron Fortified
CEREALS, VEGETABLES, AND MEATS
Fe Deficiency Lab Values
• RBC- low
• Hgb/HCT- low
• MCV/MCH- low- microcytic anemia
• Ferritin levels (iron storage) low

Anemia: Lab Evaluation
– Normal Peripheral Smear • Iron Deficiency Anemia

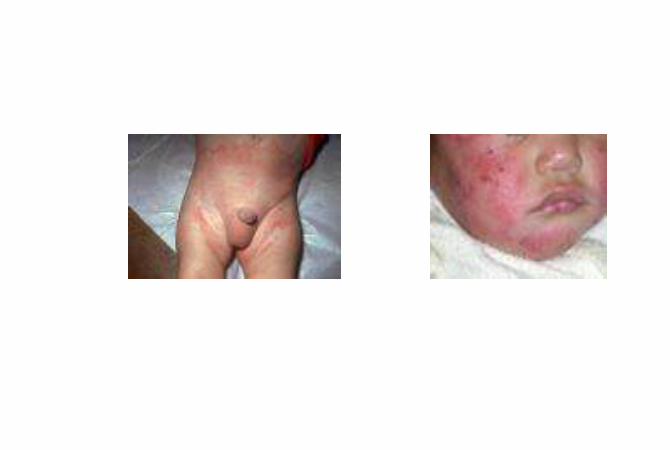
ECZEMA / ATOPIC DERMATITIS• ATOPIC DERMATITIS IS PROBABLY GENETICALLY DETERMINED WITH CONTRIBUTING FACTORS
• A PRURITIC ECZEMA ASSOCIATED WITH DRY SKIN, ALLERGY, AND EMOTIONAL STRESS WHICH STARTS IN INFANCY & MAY CLEAR BY 2-3 YRS.
• AFFECTS 9-12% OF YOUNG CHILDREN
ECZEMA / ATOPIC DERMATITIS

ECZEMA/ATOPIC DERMATITIS
THERAPEUTIC MANAGEMENT
MOISTURIZE SKIN
REDUCE INFLAMMATION (TOPICAL OR ORAL STEROIDS)
RELIEVE ITCH (MEDS AND LUBRICATION)
PREVENT SECONDARY INFECTION
REMOVE IRRITANTS AND ALLERGENS
IDENTIFY AND AVOID POTENTIAL FOOD TRIGGERS
ECZEMA/ATOPIC DERMATITIS• TREATMENT METHODS
– AVOID ENVIRONMENTAL TRIGGERS SUCH AS OVERHEATING, SOAPS, WOOL, ETC.
– ORAL ANTIHISTAMINES (Atarax, Benadryl, Claritin)
– INFREQUENT TEPID BATHING, WET COMPRESSES, OCCLUSIVE CREAMS AND COOL COMPRESSES
– LOW POTENCY ANTI-INFLAMMATORY CREAMS (Elocon, Cutivate)

FAILURE TO THRIVE (FTT)
• PERSISTENT DEVIATION FROM NORMAL
GROWTH CURVE (GROWTH < 5TH
PERCENTILE)
• ORGANIC FTT- THERE IS A PHYSICAL
PATHOLOGICAL PROCESS PRESENT. THE FTT
MAY OR MAY NOT BE CORRECTABLE
DEPENDING ON THE UNDERLYING CAUSE.
FAILURE TO THRIVE (FTT)
• NON-ORGANIC FTT
– CAUSES• DISTURBED PARENT-CHILD RELATIONSHIP
• POVERTY
• HEALTH BELIEFS
• INADEQUATE NUTRITIONAL KNOWLEDGE
• FAMILY STRESS
• MIXED FTT
– Combination of organic and inorganic etiologies

FAILURE TO THRIVE (FTT)
CLINICAL MANIFESTATIONS
• GROWTH FAILURE
• DEVELOPMENT DELAY
• APATHY
• POOR EYE CONTACT/RADAR GAZE
• STIFF POSTURE
• NO FEAR OF STRANGERS
FAILURE TO THRIVE (FTT)
• MANAGEMENT
– Reversal of malnutrition
– Treat any underlying medical conditions
– Multidisciplinary approach
Nursing Considerations
• Accurate assessment of initial weight and
height
• Record of all food intake and eating
behaviors
• Assessment of parent child relationship

SUDDEN INFANT DEATH SYNDROME (SIDS)
• UNEXPLAINED DEATH AFTER POST MORTEM EVALUATION OF A CHILD LESS THAN 1 YR. OLD
• EPISODES HAVE DECREASED 40% SINCE THE “BACK TO SLEEP” CAMPAIGN
• INCIDENCE NOW 0.6 IN 1000 LIVE BIRTHS
• PEAK AGE 2-4 MONTHS
• 95% OF DEATHS OCCUR BY 6 MONTHS

SUDDEN INFANT DEATH SYNDROME - SIDS
• MANY THEORIES BUT NO KNOWN ETIOLOGY
• SLEEP APNEA NOT THE CAUSE OF SIDS
• MONITORING OF SUBSEQUENT SIBLINGS NOT RECOMMENDED - 99% CHANCE OTHER INFANTS WILL NOT DIE OF SIDS

Risk factors
• Infants born weighing less than 3.5 pounds.
• Infants exposed to cocaine, heroin, or
methadone during the pregnancy.
• Infants who have had an apparent life-
threatening event.

Reducing the risks
Supine position only No more side lying (AAP, 2005)
No blankets, soft, bedding, bumpers, toys etc in the crib
Do not over clothe the infant
Pacifiers use at time of sleep (controversial)
No co-sleeping
SUDDEN INFANT DEATH SYNDROME - SIDS
CARE OF FAMILY AFTER SIDS EVENT
COMFORT FAMILY AND ALLOW OPPORTUNITY TO SAY GOODBYE
PROVIDE WRITTEN MATERIAL
ARRANGE FOR F/U HOME VISIT WHEN FAMILY IS READY
REFER TO SIDS SUPPORT GROUP
Cystic Fibrosis
Pathophysiology:
Increased viscosity of mucous gland secretions
Elevation of sweat electrolytes (NA)
Mechanical obstruction as a result of thick secretions
Small passages in organs become obstructed (lungs and pancreas) Meconium ileus
Pancreatic fibrosis
CYSTIC FIBROSIS
• AUTOSOMAL RECESSIVE
• MULTISYSTEM DISEASE
– RESPIRATORY SYSTEM
– DIGESTIVE SYSTEM
– INTEGUMENTARY SYSTEM
– REPRODUCTIVE SYSTEM
CYSTIC FIBROSIS
DIAGNOSIS FAMILY HISTORY
ABSENT PANCREATIC ENZYMES INCREASE SWEAT CHLORIDE - >60 mEq/L CHRONIC PULMONARY INVOLVEMENT
THERAPEUTIC MANAGEMENT PREVENT/MINIMIZE PULMONARY COMPLICATIONS ENSURE ADEQUATE NUTRITION ASSIST CHILD/FAMILY TO ADAPT TO ILLNESS

CYSTIC FIBROSIS• PULMONARY CARE
– CLEAR AIRWAY (CHEST PT, FLUTTER DEVICE, PERCUSSION VEST)
– THIN MUCUS THROUGH NEBULIZED MEDS (PULMOZYME)
– INHALED BRONCHODILATORS
– PROMPT ANTIBIOTIC TREATMENT OF INFECTIONS
– DAILY PHYSICAL EXERCISE

CYSTIC FIBROSIS• GASTROINTESTINAL CARE
– PANCREATIC ENZYMES-IF CAN NOT SWALLOW PILLS MAY BE MIXED WITH A LITTLE FOOD
– HIGH PROTEIN, HIGH CARB, HIGH CALORIE DIET
– VITAMINS A,D,E AND K, IN WATER SOLUBLE FORM
Cystic Fibrosis Related Diabetes
• Shares features of Type I and Type II
• Unique an distinct form that requires special management
• Average age of onset is 18- 21 years of age
GASTORENTERITIS
• CAUSES ARE VIRAL, BACTERIAL, METABOLIC AND PARASITIC
• MOST PEDIATRIC CASES ARE VIRAL
• EVEN VIRAL GASTROENTERITIS CAN KILL A CHILD THROUGH DEHYDRATION
• Approximately 400 children aged 1 month to 4 years die annually as a result of volume depletion
GASTORENTERITIS• DEHYDRATION AND KIDS
– ASSOCIATED WITH METABOLIC ACIDOSIS
– KIDS HAVE A GREATER EXTRA CELLULAR FLUID TO INTRACELLULAR FLUID RATIO THAN ADULTS WHICH RESULTS IN GREATER AND MORE RAPID LOSS OF FLUID
– CHILDREN EXPERIENCE GREATER INSENSIBLE WATER LOSS

WATER BALANCE DIFFERENCES
Infants and young children have a greater need for water
More vulnerable to alterations in fluid and electrolyte balance
Greater I & O relative to size
Higher basal metabolic rate
Greater production of metabolic waste
Immature kidney function

EXTRACELLULAR FLUID COMPARTMENT
Constitutes more than half total body water at birth
Has greater ECF until about age 2
Greater and more rapid water loss
during this age
WATER LOSS
2/3 of insensible water loss is through skin
1/3 through respiratory tract
Insensible fluid loss is increased by heat, humidity, temperature and respiratory rate
Infants and toddlers tend to be more highly febrile

Dehydration
• Sodium is the main solute in the ECF
• When ECF volume is reduced in acute
dehydration, total body sodium is almost
always reduced, regardless of serum values

Isotonic Hypotonic (hyponatremic) Hypertonic (hypernatremic, hyperosmotic)
ISOTONIC DEHYDRATION Primary form of dehydration in children Water and salt are lost in equal amounts Major loss is from ECF Reduction in plasma volume, circulating volume, Shock is greatest threat to life Child will display characteristic symptoms of hypovolemic
shock Serum sodium remains normal (130-150 meq/L)
Types of Dehydration
Lab Values
K+ normal to low
NA initially normal but then may be low
BUN and Creatinine – High
CO2- low (indicator of severity of dehydration)

Signs and Symptoms of Dehydration
Fewer wet diapers than usual
No tears when crying; inside of mouth dry and sticky
Irritability, high-pitched cry
Difficulty in awakening
Increased respiratory rate or difficulty breathing
Sunken fontanel, sunken eyes with dark circles
Abnormal skin color, temperature, or dryness
Slow cap refill
Decreased turgor

GASTORENTERITIS
ORAL REHYDRATION THERAPY MAY AVOID HOSPITALIZATION
CHOICE OF IV FLUID REPLACEMENT IS BASED ON THE CHILD’S TYPE OF DEHYDRATION (ISOTONIC, HYPOTONIC OR HYPERTONIC).
MAKE SURE THE CHILD IS VOIDING BEFORE ADDING K+ TO ANY IV FLUID.

Concept of Oral Rehydration
• Rehydration solution of 75 to 90 mEq of Na+ per liter
• Give 40 to 50 ml/kg over first 4 hours
• Maintain hydration with solution of 40 to 60 mEq Na+ per liter
• Daily volume of maintenance hydration 150 ml/kg/day
Mosby items and derived items ©
2006 by Mosby, Inc.152 of 60
Prevention of Diarrhea
• Most diarrhea is spread by the fecal-oral route
• Teach personal hygiene
• Clean water supply/protect from contamination
• Careful food preparation
• Handwashing
Mosby items and derived items ©
2006 by Mosby, Inc.153 of 60
PYLORIC STENOSIS
PYLORUS MUSCLE INCREASES IN SIZE AND MASS
OBSTRUCTS FOOD FROM LEAVING THE STOMACH
IF UNTREATED DEATH FROM DEHYDRATION AND ELECTROLYTE IMBALANCES
REQUIRES SURGICAL CORRECTION (PYLOROMYOTOMY)


PYLORIC STENOSIS
CLINICAL MANIFESTATIONS
– VOMITING BEGINS BETWEEN 1 TO 10 WEEKS OF AGE
– VOMITING BECOMES PROJECTILE
– PALPABLE PYLORIC MASS (OLIVE SHAPED)
– VISIBLE GASTRIC PERISTALTIC WAVES
– IRRITABLE AND HUNGRY INFANT
DIAGNOSTIC PROCEDURES
– ULTRASOUND
– BARIUM SWALLOW

PYLORIC STENOSISNURSING CARE
– PREOP MANAGE FLUIDS & ELECTROLYTES
• DECOMPRESSION OF STOMACH BY NG TUBE
• IV FLUIDS AND ELECTROLYTES– MAY HAVE K, Na, & Cl DEPLETION
– POST OP - MONITOR FEEDINGS• CLEAR LIQUIDS 4-6 HR. AFTER SURGERY
• STEP WISE PROGRESSION TO FULL FORMULA OR BREAST MILK OVER 48 HOUR PERIOD
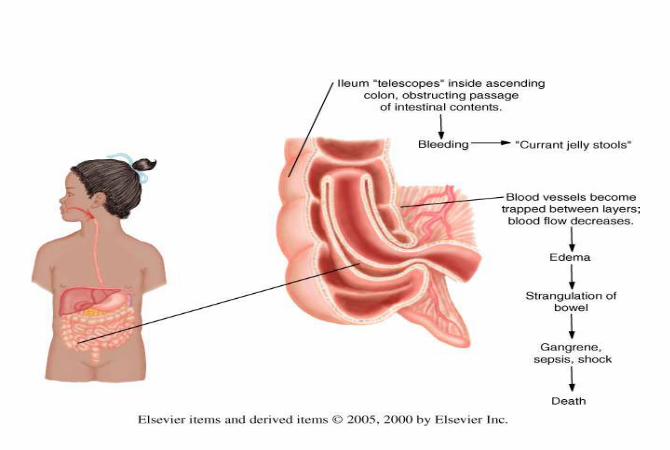
INTUSSUSCEPTION
TELESCOPING OF INTESTINE USUALLY AT THE ILEOCECAL VALVE
– Terminal ileum telescopes into the ascending colon
OCCURS BETWEEN AGES OF 3 MONTHS AND 5 YEARS - HALF IN INFANTS UNDER 1 YEAR
SYMPTOMS DEVELOP BECAUSE BLOOD SUPPLY TO COLON IS COMPROMISED

INTUSSUSCEPTION
CLINICAL MANIFESTATIONS
WAVES OF COLICKY SEVERE PAIN VOMITING CURRANT JELLY STOOLS LETHARGY (LATE IN COURSE)
COMPLICATIONS
ISCHEMIA PERFORATION AND PERITONITIS SHOCK

Intussusception
BARIUM ENEMA IS PRIMARILY DONE AS A DIAGNOSTIC PROCEDURE
THE BARIUM ENEMA MAY REDUCE THE OBSTRUCTION BY HYDROSTATIC PRESSURE.
NONOPERATIVE REDUCTION SUCCESSFUL IN 80-90% OF CASES
BARIUM ENEMA IS NOT DONE IF SIGNS OF SHOCK OR PERFORATION ARE PRESENT

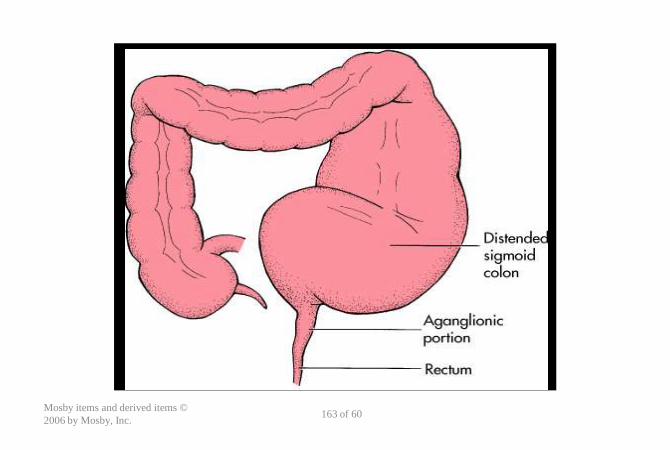
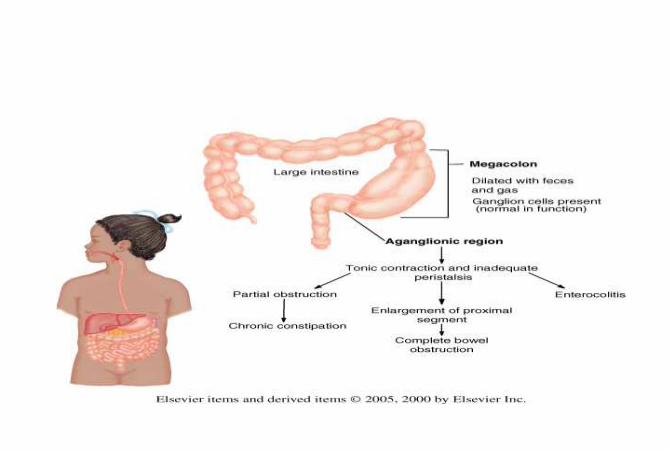
Clinical Manifestations of Hirschsprung
• Cogenital aganglionic megacolon
• Aganglionic segment usually includes the rectum and proximal colon
• Accumulation of stool with distention
• Failure of internal anal sphincter to relax
• Enterocolitis may occur
Mosby items and derived items ©
2006 by Mosby, Inc.162 of 60
Mosby items and derived items ©
2006 by Mosby, Inc.163 of 60
Therapeutic Management
Mosby items and derived items © 2006 by
Mosby, Inc.165 of 60
• Surgery
• Two stages
– Temporary ostomy
– Second stage—“pull-through” procedure
Vesicoureteral Reflux -VUR
• Retrograde of urine into ureters
– Reservoir for bacteria
• Primary – congential abnormal insertion of the ureters into the bladder
• Secondary – due to an acquired condition

Complications
• Associated with recurring kidney infections
– Pyelonephritis – high fever, vomiting, chills
– Can cause renal scarring in children
• Can occur with the first episode of febrile UTI
Management• Prevent bacteria from entering the kidney
– Low dose antibiotic therapy
– Urine culture every 2-3 months and prn fever
– Many will outgrow
– Annual cystourethrogram
– Surgery if significant anatomic abnormality , UTI’S, non compliance with meds, VUR after puberty especially in females
Prognosis
• Usually excellent with prompt treatment at time of diagnosis
• Early diagnosis essential to prevent long term complications

Nursing education
• Wipe from front to back
• Observe frequently for signs of pain, difficulty voiding

Short Bowel Syndrome (SBS)
• A malabsorptive disorder
• Results from decreased mucosal surface area, usually as result of small bowel resection
• Therapeutic management
• Nursing considerations
Mosby items and derived items ©
2006 by Mosby, Inc.171 of 60