“indoor air pollution” framing issues risk factor exposure outcomes background disease...
TRANSCRIPT

“Indoor Air Pollution”Framing Issues
• Risk Factor
• Exposure
• Outcomes
• Background Disease
• Counterfactual

Risk Factor
• Household solid fuel use– Clearly polluting in nearly all settings– Available in household surveys– Most common metric in epi studies
• Expands risk boundary– Portion of outdoor air pollution– Burns– Other non-air-pollution pathways, e.g. risks of
gathering biomass fuel and coal mining -?– Even a portion of climate change due to household
fuels-?– Include high-income countries where much wood is
used in households, but not for cooking-?

Difficulties of Household Solid Fuel Use as RF
• Exposures are not uniform because– Coal and biomass are different– Amount of usage usually not known– Difficulty of separating cooking from the heating often
done in non-tropical settings– Chimneys dominate in richer countries and are found
in poor ones – effectiveness variable– Location of cooking in household not uniform, which
affects exposure– A set of the major interventions being explored are
low-emissions biomass stoves

Exposure• Few studies used direct exposure assessment, i.e.,
average air pollution concentration affecting people, which roughly corresponds to annual means used in outdoor air pollution studies
• Reviews of health effects need to capture a wide range of indicators of exposures, incl: – Solid fuel vs. another (cleaner) fuel– Time spent near stove– Duration of exposure (years) to solid fuels– Separate kitchen from main house– Improved vs. Traditional stove
• How to combine? And do so in a way consistent with available household fuel inventories

Outcome Measures• A growing number of outcomes are associated with
exposures– Some have dozens of epi studies, i.e. ALRI, COPD, lung cancer
from coal – outcomes from CRA-2000– Some have less than 10 with consistent results, i.e., LBW and
cataracts– Some have less than 10 with some inconsistency, i.e., TB, lung
cancer from biomass– Some have few studies but would be expected from other
pollution exposures (outdoor air, ETS, and smoking), i.e., heart disease, adult pneumonia, and other cancers
– Some have no studies but would be expected from animal studies, i.e., birth defects and cognitive impacts
• Need to decide cut off, i.e., which to include in quantification
What to do about Heart Disease?
• CVD is probably the principal outcome from all other forms of smoke exposure– Active smoking– Passive smoking (ETS)– Outdoor air pollution
• Considerable toxicological/physiological (sub-clinical) evidence
• Although case-control studies underway, only one related study published: blood pressure in Guatemalan RCT
• The inconsistency was side-stepped in the CRA-2000, but must be addressed this time since solid fuel portion of outdoor air pollution is being assessed.

Chronic Cardiovascular Effects of Ambient Air Pollutants
Ambient PM
? Pulmonary
Reflexes
Autonomic Nervous System
Arrhythmia
Automaticity Conduction
Repolarization
Acute Phase Response & Coagulation
Factors
Pulmonary
Inflammation
Systemic Inflammation
Endothelial Dysfunction
Leukocyte & Platelet
Activation
Thrombosis Plaque Rupture
Oxidant Stress
Myocardial Infarction
Atherosclerosis
Progression and Plaque Instability
Heart Rate
Rhythm
Heart Rate
Rhythm
?
Brooks et al. Circulation 2004

RESPIRE and Blood Pressure (BP)
• RESPIRE: a randomized control trial monitoring the health impacts in women and children of introducing a woodburning stove with chimney in ~260 Guatemalan households compared to ~260 control households still using open woodfires for cooking

RESPIRE Results
“Control w/ stoves” values are the average reduction seen in BP of the control group after receiving the new stoves
*Adjusted for age, BMI, asset index, smoking, secondhand tobacco smoke, apparent temperature, season, day of week, time of day, random subject intercept
SBP (95% CI)
DBP (95% CI)
Intervention Group
-3.7 mmHg (-8.1, --0.6)
-3.0 mmHg (-5.7, -0.4)
Control w/ stoves
-3.1 mmHg (-5.3, --0.8)
-1.9 mmHg (-3.5, -0.4)
McCracken et al., 2007
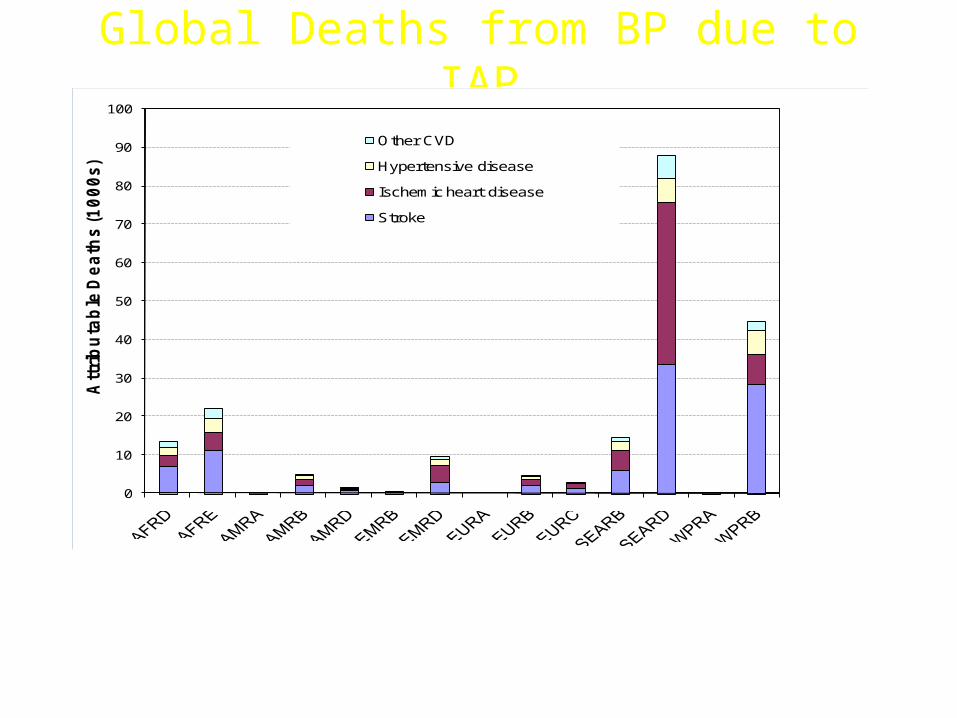
Global Deaths from BP due to IAP
0
10
20
30
40
50
60
70
80
90
100A
ttri
bu
tab
le D
ea
ths
(1
00
0s)
Other CVD
Hypertensive disease
Ischemic heart disease
Stroke
Estimated cardiovascular deaths in 2004 attributable to elevated BP caused by solid fuel smoke exposure. Number of deaths preventable by a 50% reduction in solid fuel smoke exposure by WHO sub-region and disease category.
McCracken and Schwartz, 2009

Heart Disease?• Options to fill gap
– Use BP results • Only one study• Not pathway thought to dominate CVD effect
– Use exposure estimates to apply against outdoor and ETS results
• Exposure response probably not linear• Do not have exposure estimates for most of world, although
hoping to have for India– Use COPD to calibrate, i.e., apply COPD/CVD ratio in
outdoor and ETS studies • Ratio probably different at different exposure levels• Some evidence that biomass smoke less dangerous for CVD
than fossil fuel smoke, although similar for respiratory outcomes
Background Disease
• For applying PAF values– Separate rates for rural and urban pops?– Separate rates for smoking and non-smoking
pops?
• How to deal with inability to separate LBW into IUGR and prematurity?

Counterfactual• In CRA-2000, non-solid fuel use, i.e.,
electricity, gas, or kerosene– Roughly fit available epi and HH survey data– Clearly feasible – half world already there
• Problems: physical– Kerosene not clean in many circumstances– Even gas stoves have been associated with ill-
health in dozens of first world studies• Problems: methodological
– Clear that there is much exposure misclassification with use of binary variables
– True low-exposure control groups rare or non-existent in current studies due to high levels of confounding with SE status

Simple MeasurementsMixed Model Predictions

0 1 2 3 4 5 6 7
CO Exposure (ppm)
ALR
I Rat
e (p
er 1
00 C
hild
-Yr)
2030
4060
80
(A)
MD-diagnosed ALRI
RESPIRE-Guatemala
Approximate PM2.5 exposure in 100s of ug/m3

0 1 2 3 4 5 6 7
CO Exposure (ppm)
Hyp
oxic
ALR
I Rat
e (p
er 1
00 C
hild
-Yr)
1015
2030
40
(B)
Severe (hypoxic) MD-ALRI
RESPIRE-Guatemala
Approximate PM2.5 exposure in 100s of ug/m3

Many thanks
Solid-Fuel-Use CRA Website:http://ehs.sph.berkeley.edu/krsmith/page.asp?id=25