increasing transrectal ultrasound guided prostate biopsy associated infection; is a change in...
TRANSCRIPT
Increasing transrectal ultrasound guided prostate biopsy associated infection; is a change in antimicrobial prophylaxis the solution?
Authors: Ni Bhuachalla C1, McNamara E2, Carroll A2, Lynch T1, Boyle B1
1. St James’s Hospital, Dublin 8, Ireland. 2. Public Health Laboratory HSE, Dublin 10, Ireland.
TRUS biopsy associated infection• Surveillance/ diagnostic protocol•Post procedure infection rates
1- 3% UTI 0 .5- 1% BSI
•Strategies to reduce rate of infectionAntimicrobial prophylaxisPre procedure screeningDecontamination protocolOperator training
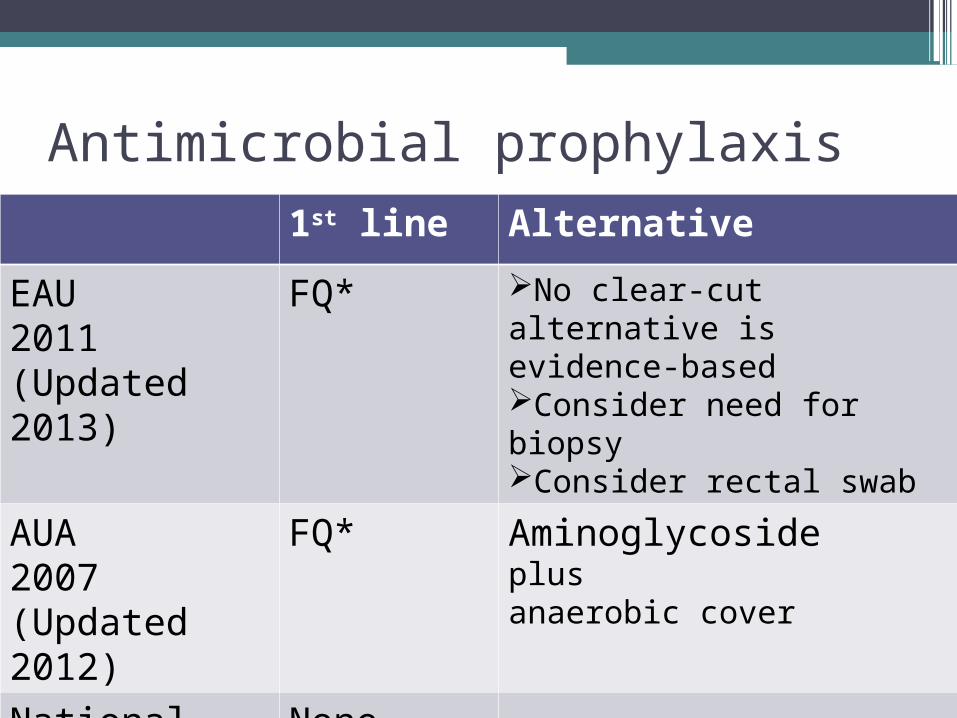
Antimicrobial prophylaxis1st line Alternative
EAU2011(Updated 2013)
FQ* No clear-cut alternative is evidence-basedConsider need for biopsyConsider rectal swab
AUA2007 (Updated 2012)
FQ* Aminoglycoside plusanaerobic cover
National guideline
None

“...clear lack of standardization in antibiotic prophylaxis for transrectal prostate biopsy...”
“...in nine trials we observed that antibiotic prophylaxis is effective in preventing infectious complications and hospitalization following prostate biopsy...”
“...several classes of antibiotics are effective for prophylaxis in prostate biopsy, with the quinolones the best analysed class...”

Antimicrobial resistance
• prevalence fluoroquinolone (FQ) resistance
• prevalence gentamicin resistance • Previous exposure to antimicrobials • Previous health care contact

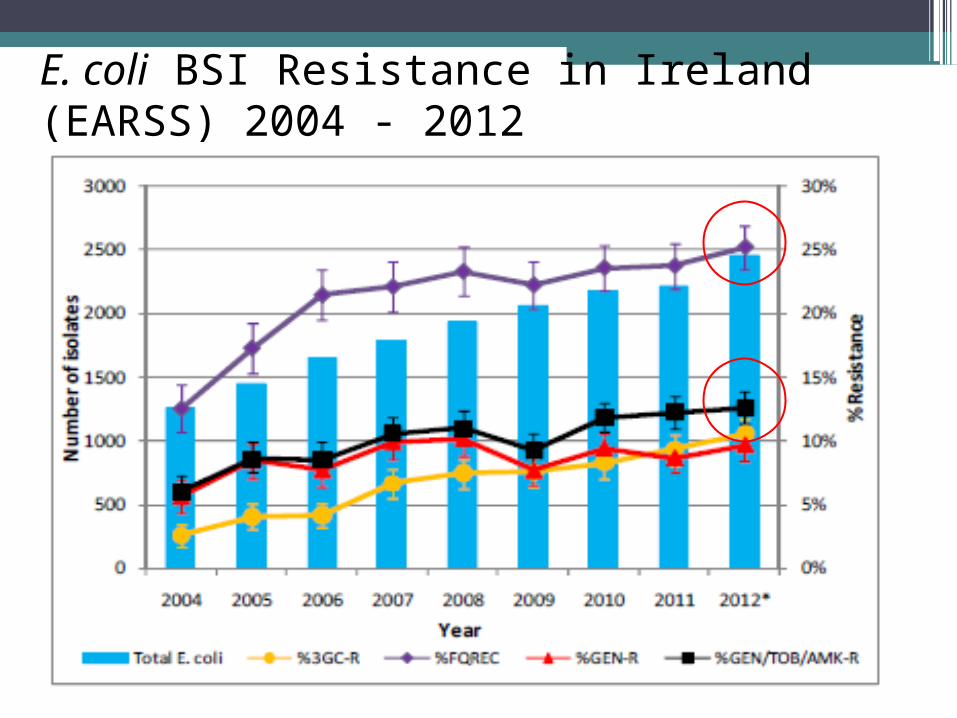
E. coli BSI Resistance in Ireland (EARSS) 2004 - 2012
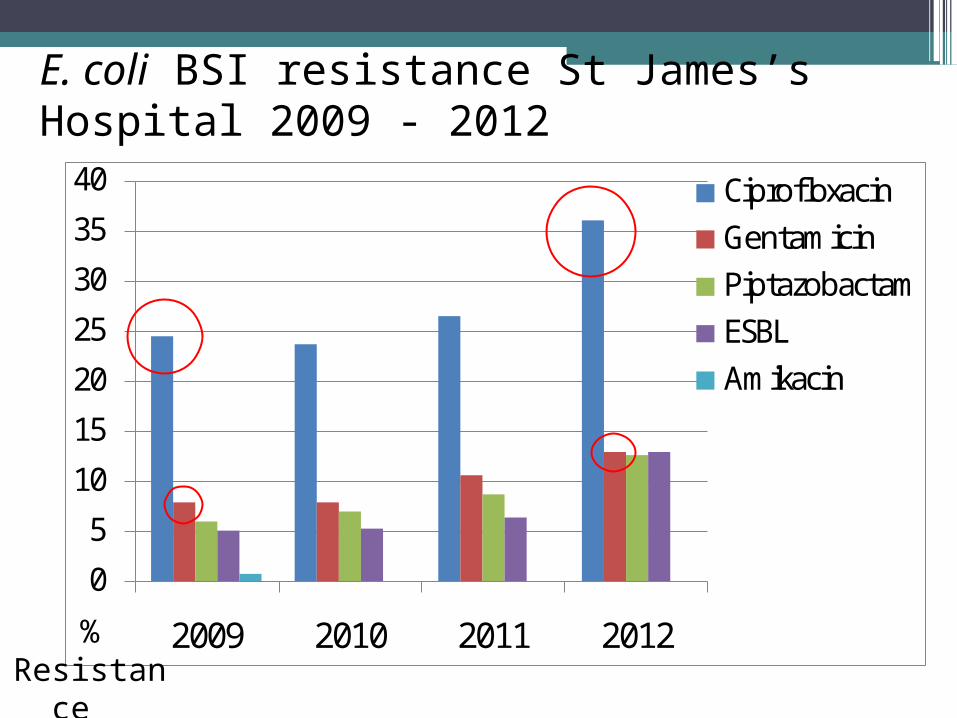
E. coli BSI resistance St James’s Hospital 2009 - 2012
0
5
10
15
20
25
30
35
40
2009 2010 2011 2012
CiprofloxacinGentamicinPiptazobactamESBLAmikacin
% Resistance
Aims
• To identify all patients with post TRUS biopsy infection from Jan 2010 - Nov 2012
•Review isolates and susceptibilities causing infection
•Review antimicrobial prophylaxis administered
•To assess efficacy of change in prophylaxis from Dec 2012 to date
MethodsStudy period 1
(Retrospective)• Jan 2010 – Nov 2012•Prophylaxis
gentamicin and FQ• ID and susceptibility
testing Vitek 2•Typed by PFGE
(pulse net protocol)
Study period 2 (Prospective)
•Dec 2012 – Feb 2013
•Prophylaxis amikacin and FQ

Study period 1Jan 2010 – Nov 2012
No. TRUS biopsies conducted 1398
Overall infection rate 1% (15)
Type of post biopsy infection 0.4 %BSI/ SSI (6/15)0.6% UTI (9/15)
Isolates All E.coli
Previous TRUS biopsy 60% (9/15)
Isolates All E.coli
Ciprofloxacin resistance 73.3% (11/15)
Gentamicin resistance 40% (4/10)
Amikacin resistance 0% (5/5)
ESBL producer 6.7% (1/15)

Number of TRUS associated infections Jan 2010- Nov 2012
0 1 140
100200300400500600700
2010 2011 2012
No of TRUS biopsies per year
No of TRUS associated infections per year
477
604540
(until end of Nov 2012)
(0.2%) (2.5%)
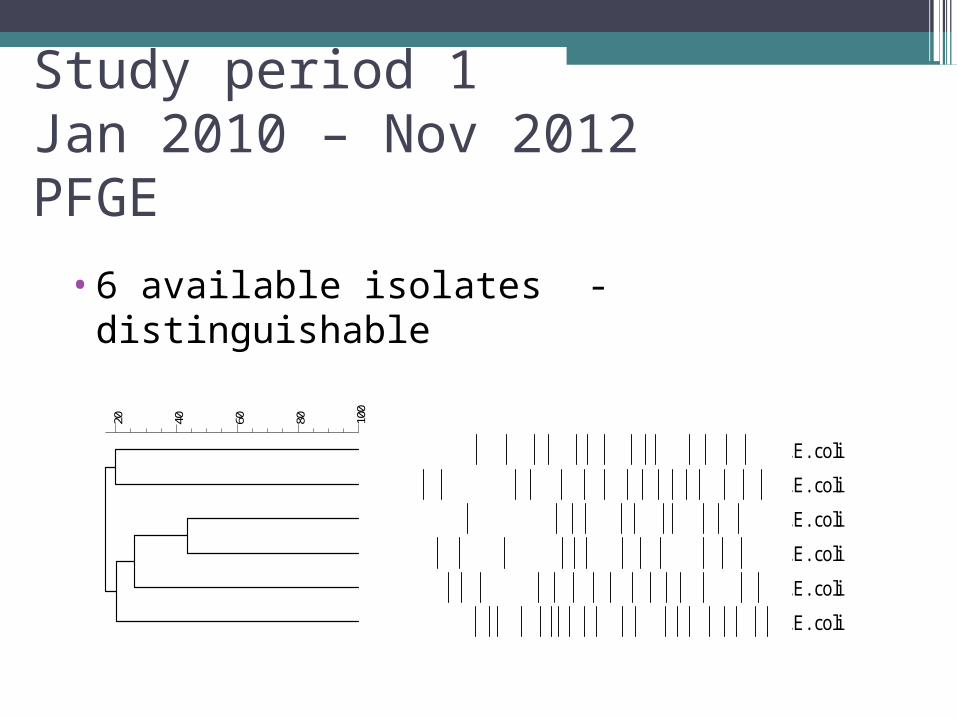
Study period 1Jan 2010 – Nov 2012PFGE
•6 available isolates - distinguishableDice (Tol 0.6%-0.6%) (H>0.0% S>0.0%) [0.0%-100.0%]
100
80604020
.
.
.
.
.
.
E. coli
E. coli
E. coli
E. coli
E. coli
E. coli
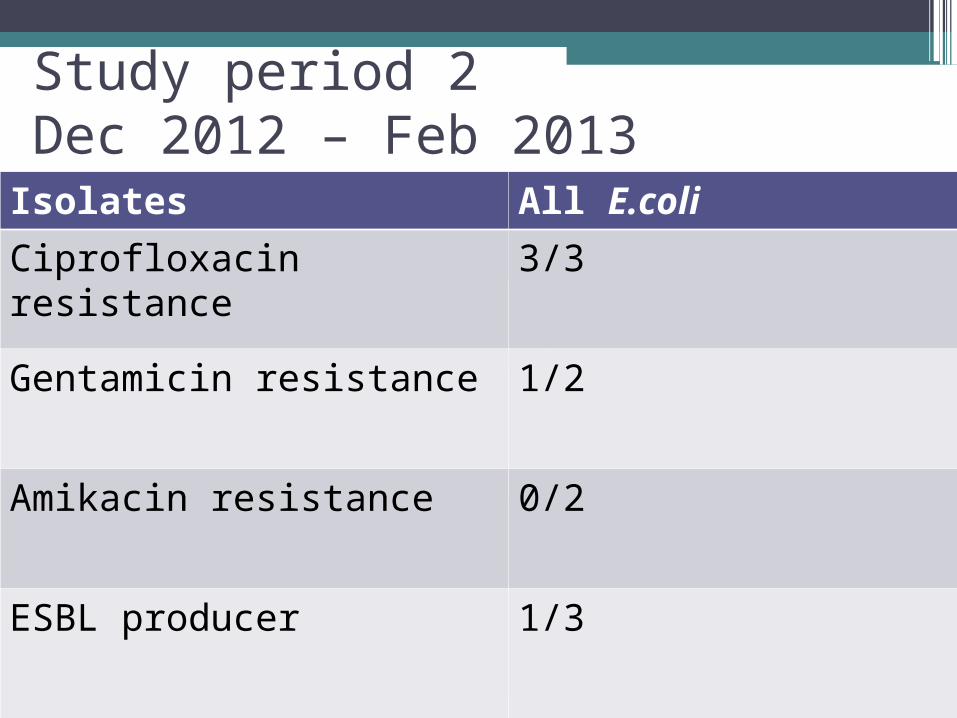
Study period 2Dec 2012 – Feb 2013
No. TRUS biopsies conducted
140
Overall infection rate 2% (3)
Type of post biopsy infection
1.3% BSI (2)0.7% UTI (1)
Isolates All E.coli
Previous TRUS biopsy 2/3
Isolates All E.coli
Ciprofloxacin resistance 3/3
Gentamicin resistance 1/2
Amikacin resistance 0/2
ESBL producer 1/3

Post TRUS infection rate Jan 2010 to date
Change of prophylaxis
0.2%
2.5%
2%


Local interim Recommendations Amikacin and FQ? Avoid fluoroquinolone use in empiric
treatment of post biopsy infection Targeted treatment of post biopsy
infection when susceptibilities available Targeted prophylaxis?

Conclusions Increase in TRUS biopsy associated
infection Increasing antimicrobial resistance Prospective surveillance Potentially multifactorial process