increasing the impact of assistive technology …increasing the impact of assistive technology...
TRANSCRIPT

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 1 of 45
Increasing the IMPACTof assistive technology
Introduction
Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 2 of 45
TABLE OF CONTENTS
INTRODUCTION ................................................................................................................................................. 3
1 ASSISTIVE TECHNOLOGY, AGEING AND DISABILITY........................................................... 6
1.1 ASSISTIVE TECHNOLOGY .......................................................................................................................... 61.2 DISABILITY............................................................................................................................................... 81.3 AGEING .................................................................................................................................................. 131.4 CHALLENGES OF DISABILITY AND AGEING.............................................................................................. 18
2 A GLIMPSE OF ASSISTIVE TECHNOLOGY............................................................................... 22
2.1 A WIDE VARIETY - HIGH-TECH AND LOW-TECH, DEDICATED AND GENERAL-PURPOSE............................ 222.2 ASSISTIVE TECHNOLOGY FOR DIFFERENT PROBLEM AREAS .................................................................... 242.3 TYPES OF APPLICATION........................................................................................................................... 252.4 CONTEXTS OF USE .................................................................................................................................. 26
3 HOW DO PEOPLE ACQUIRE ASSISTIVE TECHNOLOGY?.................................................... 28
3.1 THE DIFFERENT SYSTEMS IN DIFFERENT COUNTRIES............................................................................... 283.2 KEY THEMES AND ISSUES........................................................................................................................ 33
4 MANY UNMET NEEDS FOR ASSISTIVE TECHNOLOGY........................................................ 34
4.1 INTRODUCTION....................................................................................................................................... 344.2 THE EXTENT OF UNMET NEEDS ............................................................................................................... 354.3 WHY ARE UNMET NEEDS SO COMMONPLACE? ........................................................................................ 35
5 ABOUT THE REST OF THE COURSE - HOW TO BE AN ATI.................................................. 38
5.1 ASSISTIVE TECHNOLOGY INTERMEDIARIES ............................................................................................ 385.2 OVERVIEW OF THE REMAINING MODULES............................................................................................... 39
6 REFERENCES..................................................................................................................................... 42
7 GLOSSARY ......................................................................................................................................... 43
8 FURTHER INFORMATION ............................................................................................................. 44

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 3 of 45
INTRODUCTION
Elena
Elena O'Keefe is a 65-year-old woman wholives alone. She has been struggling witharthritis since she was in her thirties. As herarthritis got worse, she had to take earlyretirement back in 1982. Since then hercondition slightly improved following thereplacement of several joints.Despite this, Elena is one of a minority of arthritis patients who needs oruses a wheelchair. Her brother convinced her it might be a good idea to useone, and when Elena saw a powered wheelchair once, she thought 'thiscould be fun'. Her decision to actually start using a wheelchair has beenpositively liberating. Now, she is much more independent. She can movearound and actually do her shopping in the neighbourhood.
Nicole
Nicole is an 82-year-old woman, living inEindhoven, a medium-sized city in thesouthern part of the Netherlands. As a formercollege lecturer, she has always had an activelife with a good network of friends and asubstantial involvement with localassociations.
Since the last couple of years she has had difficulties with walking.However, she refuses to give in and has acquired a rollator: “With this tool,I am able to do many things I couldn't do otherwise, like shopping orattending the performances of the local theatre group, ... I couldn't managewithout my rollator any more”.
Nicole refuses to move to a service flat or residential care. She has beenliving in her own flat for a great many years and it is still full of memoriesof her husband, who died four years ago. Nicole still likes to go out andenjoy the company of her friends over a cup of coffee on a nice springafternoon. At home, she likes to watch television or do some embroidery.Most of all, she enjoys reading a good novel.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 4 of 45
Mary
Mary Sommers is 91 and has been livingsince 1925 in her own house in a small town.She has a daughter living nearby, within 300metres. Mary doesn't think 'going to anursing home' is a necessary or a goodoption: 'I'm so happy living here - I wouldn'tdream of leaving. This place has many goodmemories of Will, my husband, who died 15 years ago. And all ourchildren were born in this house.'Since the death of her husband, Mary has become very independent.Different kinds of assistive technology help her to cope with the problemsshe is experiencing as she gets older. She is open to tools that make lifeeasier - an attitude that she developed within the past ten years. It all startedwith the problems she experienced due to her hearing impairment, althoughat the time she didn't recognise the cause of the problems and didn't knowthe problems could be improved by assistive technology.
Anna
Anna is a 65-year-old woman living in asmall town in Finland. Prior to her stroke sheworked in different office situations and hasexperience of using PCs. Anna had a strokea few years ago, resulting in hemiparesis inher right hand, and aphasia. Immediatelyfollowing the stroke, Anna had severedifficulties in understanding speech and her speech therapist observed thatshe was not able to follow discussions or to answer simple yes/noquestions. Visually she was able to combine similar pictures, but she wasnot able to combine conceptual groups (e.g. fruit, furniture etc.). She hadmarked aphasia, with some strong stereotypical expressions and was notable to initiate communication.
This set of learning materials is concerned with ‘assistivetechnologies’. These are the technological systems and devices thatassist people who have difficulties, due to age or disability, incarrying out everyday activities. The focus is on how you, as a healthor social service professional, can help to ensure that your older ordisabled clients are in a position to benefit from the assistivetechnologies that they need.
The aim is to provide you with an overview of:• the challenges that can be posed by ageing and disability;• the role that assistive technology can play in supporting
independence and well-being for older people and disabledpeople; and

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 5 of 45
• the critical role that each of the various health and social serviceprofessions can play in making sure that the appropriate assistivetechnology is made available to those who need it.
This module provides a first introduction to the topics that areaddressed in more detail in later modules. These later modules focuson specific areas - physical functioning, vision, hearing andcommunication.
The learning goals of this and the subsequent modules are that youwill:• know enough about ageing and disability to appreciate the
importance of assistive technology;• know the main forms of assistive technology and appreciate the
wide range of products, devices and applications;• recognise that the current situation regarding availability and
take-up of assistive technology for those who need it is often veryunsatisfactory;
• understand the crucial role and responsibility of all branches ofthe health and social services, and all of their respective caringpersonnel, in remedying this situation; and
• know the main elements of the role of ‘assistive technologyintermediary’ that you can and should play as a health/socialservice professional.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 6 of 45
1 ASSISTIVE TECHNOLOGY, AGEING ANDDISABILITY
This course is primarily intended to do two things - develop yourawareness of assistive technology and teach some practical thingsthat you can do as a practitioner in this area. This section gives aninitial introduction to assistive technology, ageing and disability.
1.1 Assistive technology
! Context activity - assistive technology
Think about persons in your environment who use assistive technology andtry to answer the following questions:
• What kind of assistive technology do they use?• Why do they use it?• Where did they get it?• What health professional(s) were involved in this process?
The term ‘assistive technology’ (AT) refers to those products,devices and applications of technology that can provide support todisabled people and older people in their daily lives. It is nowcoming to be the preferred term for describing such technologies andis increasingly used in place of older terms such as ‘rehabilitationtechnology’ or ‘technical aids’. However, as you will see, bodies likethe International Standards Organisation still use the term technicalaids, as do the public services in many countries.
The International Standards Organisation defines technical aids as:
“any product, instrument, equipment or technical system used by adisabled person, especially produced or generally available,preventing, compensating, relieving or neutralising the impairment,disability or handicap.”
In fact, assistive technologies need not be restricted to those that areused directly by the disabled (or older) person themselves, but alsoinclude those that are used by carers, such as lifting aids, or that are

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 7 of 45
used to deliver services by a care service provider, such as tele-alarms.
Following from this definition, assistive technologies may be of twokinds - aids specifically designed to meet the needs of disabledpeople and older people, and more general-purpose technologies thatare nonetheless of particular benefit to disabled people and olderpeople.
In the general-purpose category are a variety of consumer products,household amenities and utilities, including labour-saving devices(e.g. washing machines), amenities (e.g. inside toilet) and utilities(e.g. the telephone) that can be particularly important for people withdisabilities. Such everyday technologies have a significant role toplay in supporting independence and self-care. However, even in aEurope approaching the end of the millennium, a small butunacceptable number of disabled people and older people still livewithout access to such basic facilities as a private indoor toilet ortelephone.
Assistivetechnologies rangefrom simple low-tech items likewalking sticks to themost sophisticated inpowered transport,computers,telecommunicationsand robotics.
The main classes of technical aids listed in the European Glossary onTechnical Aids (based on the ISO's classification system) indicate thevery wide range of equipment, devices, and adaptations, which areincluded within the scope of assistive technology.
European Glossary on Technical Aids
Here are some of the main categories listed in the Glossary:• Personal care and protection (e.g. aids for using the toilet and for
washing/bathing; adapted clothing, shoes, etc.)• Personal mobility (e.g. wheelchairs; turning and lifting aids; orientation
aids; etc.)• Housekeeping (e.g. aids for preparing meals, dish washing,
eating/drinking, and cleaning, etc.)• Home adaptation (e.g. adapted furniture; aids for opening/closing
doors, windows, curtains; lifts, safety equipment; etc.)• Communication, information, signalling (e.g. optical aids, hearing aids,
writing aids, computers and software, alarm systems, telephones, face-to-face systems, etc.)

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 8 of 45
• Handling (e.g. aids for operating things; environmental controlsystems; hand, finger or reach aids; aids for carrying or transporting;robots; etc.)
• Environment improvement (e.g. climate control)• Recreation (e.g. suitable toys or games, exercise and sports facilities,
gardening equipment, etc.) • Therapy and training (e.g. dialysis, medicine dosing, testing/analysis,
stimulation, sore prevention; aids for therapy and training in a widevariety of areas, such as vocational training, arts, communication skills)
• Orthoses/prostheses (e.g. for spine or limbs; orthopaedic footwear;etc.).
The full classification can be found in ‘The European Glossary onTechnical Aids’, EU DGV, Helios-Handynet, 1996. Further information onthe ISO classification system upon which this is based can be found athttp://www.iso.ch/
In this course, the scope will cover all of these technologies with theexception of orthoses/prostheses and some of the more medically-oriented therapeutic technologies such as dialysis.
1.2 Disability
This course is about the role of assistive technology in meeting someof the important needs of disabled people and older people. At theoutset, therefore, it is important to gain an understanding of whatdisability and ageing involve for those directly concerned - disabledpeople and older people themselves. This section looks at disabilityand how various parties have conceived it over the years. Thesubsequent section looks at the meaning and experience of ageing.
One of the main reasons why disabled people have problems intoday's society and do not enjoy equality of opportunity is because ofthe way disability is defined and understood. Disability is a difficultconcept to define, and the way it is understood largely determines thehealth and social policies that are adopted and, ultimately, the impactof disability at all levels, from the individual to society.
Tom
Tom is suffering from arthritis. He hasdifficulties with walking and uses a walkingframe with wheels. He lives in an apartment onthe third floor of the building. Fortunately thereis an elevator in this building. He always usesthis elevator to go to or leave his apartmentwhen going shopping nearby. Then the small shop where he always gets hisgroceries closes, leaving only a large supermarket about two kilometresaway from his apartment. He is not able to walk to the shop to buy hisgroceries.
Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 9 of 45
! Context activity - disability
Try to explain the concept of 'disability' in Tom's case.
Over the years a variety of perspectives on disability have beendeveloped. At opposite poles are perspectives embracing the‘medical’ model and the ‘social’ model, respectively.
Traditionally, much of the health and social policy on disability wasbased on a medical model that viewed disability as a ‘personal’problem, directly caused by disease, trauma or health conditions, andone that primarily required medical care provided in the form ofindividual treatment by professionals.
The social model ofdisability, on the otherhand, sees the issue mainlyas a societal challenge toensure the integration ofdisabled people intosociety. From thisviewpoint, disability is notan attribute of a person, buta set of (potentially)restrictive conditions thatarise, not as the result ofimpairment per se, but ofsociety's failure toaccommodate the needs ofthose with disabilities andto allow them to exercise their abilities.
Apart from requiring practical actions (such as making assistivetechnology available and designing products and the environment tobe accessible to all), the social model requires a change in traditionalattitudes and the recognition, at the political level, that the challengeof disability is a question of human rights.
Nowadays, the social model has come to predominate and, as will beseen in the next section, the World Health Organisation has beenendeavouring to incorporate these emerging perspectives into itsclassification systems for disabilities.
! Context activity - disability
Will your description of the disability of Tom change when you follow thesocial model? And if it changes, in which way?

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 10 of 45
The classifications of disability by the World Health Organisation
In 1980, the World Health Organisation (WHO) published the firstversion of the ICIDH (International Classification of Impairments,Disabilities, and Handicaps). This was developed as a supplement toan older WHO classification, the International Classification ofDiseases (ICD), when the medical profession recognised thatdisability went beyond the diseases or accidents that causeimpairments and that, in order to prescribe treatment andrehabilitation, a classification was needed that would describe theconsequences of the medical conditions.
The central constructs of this ICIDH-1980 classification areimpairment, disability and handicap, and these terms are used in aprecisely defined way.An impairment is any loss or abnormality of a psychological,physiological or anatomical structure or function. A disability is anyrestriction or lack of ability, resulting from an impairment, toperform an activity in a manner considered normal for people. Ahandicap is a disadvantage, resulting from an impairment ordisability that limits the fulfilment of individual goals.
After two decades of use, it was accepted that this classificationsystem needed to be revised in the light of changes in health careprovision and the new social understanding of disability. Work onthe new ICHID-2 is already underway and is scheduled to becompleted by the year 2000 when it will be adopted by the WHOassembly.
What Disabled Peoples' International says...
Disabled Peoples' International (DPI) has stated the requirement of disabledpeople from the new WHO proposals very clearly.
“In a perfect world we would prefer to have no classification at all. We arethe only oppressed group that has to be put through the mill in order toidentify who we are.However, for the purpose of statistics, assessment for services andprograms and above all for non-discrimination legislation, we do need tohave a definition of who we are and of our situation and we reluctantlyaccept that this means some sort of classification or analysis ofdisablement. But the crucial point for us all is that any classification of usor our situation must be made in the social context and not in the individualcontext”.
The WHO's first step has been to change the names of some of thecategories in order to eliminate their negative character. Disabilityhas become activity and, by extension, limitations to activity.Handicap has become participation and, by extension, limitations toparticipation.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 11 of 45
Definitions of proposed dimensions in ICIDH-2:
Impairment is a loss or abnormality of body structure or of a physiologicalor psychological function, e.g. loss of a limb, loss of vision....
An activity is the nature and extent of functioning at the level of theperson. Activities may be limited in nature, duration and quality, e.g. takingcare of oneself, maintaining a job...
Participation is the nature and extent of a person's involvement in lifesituations in relationship to impairments, activities, health conditions andother contextual factors. Participation may be restricted in nature, durationand quality, e.g. participation in community activities, obtaining a drivinglicence...
You can follow the progress of work on ICIDH-2 at:• http://www.who.int/msa/mnh/ems/icidh/
Functional emphasis
The emphasis on activity and participation will enable national andEuropean statistics to give more attention to the functionaldifficulties being experienced by disabled people. This will be morehelpful in giving information about the number of people who areactually facing problems in achieving what they would like to do,such as watch television, bathe and wash easily, lift a telephonehandset or have a telephone conversation.
! Context activity
Remember the example of Tom and try to describe his impairment, alimitation in his activity, his participation and a contextual factor thatinfluences these descriptions.
The functional approach is especially useful when consideringdisability in older age. There is a link between ageing and disabilityin the sense that a high proportion - about 70% - of disabled peopleare over 65 years of age. However whilst all older people undergomental and physical changes, it would be wrong to consider all olderpeople as mostly frail or disabled. The majority of older people are infact living in quite good health.
In particular, it is functional status rather than medical or disabilityclassification or age that will determine whether a person can live anindependent life in the community. Functional status will alsodetermine the levels and types of assistance, including requirementsfor assistive technologies that are needed to carry out activities ofdaily living. The classification of activities in the ICIDH-2 system(see the factsheet on this for details) gives an indication of the widerange of functional capabilities that are important for everyday life.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 12 of 45
! Research activity - activities from the WHO ICIDH-2
Look at the list of activities in the factsheet and select those activities inwhich you think Tom is limited. Then compare this description of limitedactivities with the descriptions of disability you gave earlier and try tocombine these descriptions with the type of assistance and assistivetechnologies Tom could benefit from. Which description will give you themost valuable hints to define the type of assistance and/or assistivetechnologies Tom could benefit from?
Prevalence of disability
These positive developments in the conceptualisation andclassification of disabilities have yet to find their way into nationaland European statistics, however. In fact, there is not yet an adequatedata set that would allow us to make a really accurate quantificationof disability in the EU nor is there anything to provide a comparativepicture of the situation across the European countries.
The most recent prevalence data for various categories of disabilityare reported in the Eurostat publication Disabled Persons StatisticalData (Eurostat, 1995). The data is based on various nationaldefinitions of disability and gives estimates of the number ofdisabled people in the EU countries as varying between 9.3% and15.2% of the population, with most member states apparently havinga percentage close to 12% of the population. The variation may be aresult of the different age structures of the population in the differentcountries, the different methods used to define and identify personswith disability or a combination of these and other factors.
Whilst this data tells us that disability is a significant issue for thehealth and social services in Europe, the fact that it does not give abreakdown into different disability categories means that it is notvery useful, on its own, for identifying the extent of potential needfor assistive technology. For this type of data it is necessary to lookfor good quality national statistics and then extrapolate these to theEU level in order to get reasonable estimates of the numbers ofpeople with different types of disability.
Table 1 provides estimates based on a UK survey that used the WHOICIDH 1980 classifications. From this we can give an approximateindication of the numbers of people with different disabilities in theEuropean Union population of about 375 million people. (cf.Eurostat, 1995, Table 9, p.192)
We can see from the Table that large numbers of Europeansexperience disabilities in the four areas targeted in this course -physical functioning, hearing, vision and communication. It is alsoclear that many people experience multiple disabilities (the numbers

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 13 of 45
in each category, when added, give a much higher figure than thetotal with at least one disability).
TABLE 1.Estimates of numbers of disabled people in the EU
(based on extrapolation of UK data)
Disability type % N(millions)
Physical functioning: Personal care 7.3 % 27.4 Locomotion/Mobility 7.8 % 29.3 Body disposition/Use of body 2.2 % 8.3 Dexterity/Clumsiness 3.1 % 11.6Visual 3.0 % 11.3Hearing 4.7 % 17.6Communication (verbal) 2.3 % 8.6Total (with a least one disability) 11.6 % 43.6
1.3 Ageing
As the European Union approaches the new millennium, a majordemographic challenge is unfolding. The number of children andyoung people in the Union is decreasing whilst the number of olderpeople continues to rise. Since the European Union was formed overthirty years ago its population has been ageing. This 'greying' of thepopulation is occurring in all EU countries, with some variation intiming in the different countries.
A number of factors are responsible for this, including a decline infertility rates and the increasing longevity or life expectancy of theolder population. As a consequence, the traditional pyramid-shapedage structure of the population, with its wide base and narrow top,has been replaced by a more column shape. That is, there is a moreeven distribution of people among different age groups. These trendsare expected to continue, accelerated by the ageing of the post-war‘baby boomers’, further flattening the pyramid structure of thepopulation (Figure 2).
Growing numbers of older peopleThere are more than 75 million people aged 60 years and over in theEuropean Union at present, representing about one in five of the totalpopulation. This figure is expected to rise rapidly in the comingdecades so that by the year 2020 more than one quarter of theUnion's population will have reached their sixtieth birthday (Figure3).

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 14 of 45
Figure 1. Age pyramid: EU estimates for 2020Source: reproduced from Eurostat/ILO data
Figure 2. People aged 60+ years and 80+ years as a % of the totalpopulation of the EU 1990-2020
1009590
858075706560555045403530
2520151050
0.2 0.4 0.60 0.8 1.00.8 0.6 0.41.0 0.2 0
1919
1929
1939
1949
1959
1969
1979
1989
1999
2009
2019
1919
1929
1939
1949
1959
1969
1979
1989
1999
2009
2019
AgeYear of birth Males Females Year of birth
% of total population = 1990
20
26
0
10
20
30
40
People aged 60+ years
Per
cen
t
1990
2020
3.4
5.7
0
2
4
6
8
People aged 80+ years
Per
cen
t
1990
2020

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 15 of 45
Figure 3. People aged 80 and over as a % of total population ineach EU country.
(Source: Eurostat Demographic Statistics, 1997; *national forecastsnot given)
Because of different fertility, mortality and migration rates inmember states, the rate of population ageing varies across the EU.Nevertheless, all member states are expecting a significant increasein their older populations in the next twenty years.
What's in a name
People aged 60 and over were recently asked in an opinion poll what theypreferred to be called. Although there was no consensus across the wholeCommunity, with the majority being split between 'older people' and 'seniorcitizens', they overwhelmingly came down against being called 'elderly' -the term most commonly used by the media and policy makers. (Cronin & McGlone, 1993).
Very old peopleEven more significant than the growth in the proportion of olderpeople in the EU is the ageing of the older population itself. The veryold - aged 80 years and over - are the fastest growing section of theolder population and will number 20 million people by 2020 (Figures3 and 4). This represents an increase of about 60% on averagebetween 1990 and 2020.
More older women than older menWhilst more Europeans than ever before are reaching old age andvery old age, this does not apply equally to both sexes. Womenoutlive men by an average of 6 years. The longer life expectancy ofwomen results in an imbalance between the sexes in old age. Nearlythree in five older people aged 60-79 in the EU are women, as areseven in ten aged 80 and over.
Falling birth rates and dependency ratiosAs noted earlier, falling birth rates are an important factorcontributing to the ageing of the population overall. The averagenumber of children per woman in the EU has been falling since the
B DK D EL* E F IRL I L NL A P* FIN S UK0
1
2
3
4
5
6
7
8
Per
cen
t
B DK D EL* E F IRL I L NL A P* FIN S UK
1990
2020

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 16 of 45
mid 1960's, from 2.63 in 1960 to 1.58 in 1990, and is now below thepopulation replacement level of 2.1 children per woman. Becausepeople are having fewer children there will be fewer family membersto provide care for older people in the future. This reduction in theavailability of informal carers is likely to be compounded by pressurefrom the labour market to encourage ‘typical’ family carers (usuallywomen in their middle years) to take-up paid employment. Thesetrends will increase the importance of assistive technology that canhelp self-care and independent living.
Disability amongst older people in Europe
At age 60, the average life expectancy in the EU is 20 years and, formost people, many of these years will be spent in fairly good health.There is of course enormous variation between people in the extentto which ageing is accompanied by problems in daily living and verylittle is known about the complex processes involved. Research intoprotecting and maintaining health and independence amongst healthyolder people is in its infancy but is receiving increasing support.
Whilst it is true that the majority of older people are in good healthand remain capable of caring for themselves - in fact many are carersthemselves - nevertheless a sizeable minority do have healthproblems that affect their functional abilities and require someassistance in carrying out activities of daily living. Between onequarter and one third of those aged 70 and older need some level ofassistance and it is estimated that over 40% of those aged 80 or olderare severely incapacitated.
Prevalence of functional limitations amongst older people
As noted earlier, in the case of older people, functional limitationsrather than disabilities tend to be the focus, although these areobviously largely overlapping. Functional limitations relating toactivities of daily living are traditionally divided into those affectingbasic activities (ADLs) and instrumental activities (IADLs),respectively. ADL activities are those that provide directly for theprimary needs of personal care and maintenance (e.g. fornourishment, keeping warm, looking well-groomed). IADLs are thesecondary activities that are instrumental to sustaining these basicneeds in independent community living (e.g. shopping and cooking).Basic and instrumental activities cover various areas such as theexamples given in the following box (based on Guralnik et. al.,1996).

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 17 of 45
Activities of daily living
Basic
EatingTransferring (bed to chair)ToiletingDressingGrooming (e.g. toenails)BathingWalking (400 metres)Using steps and stairs
Instrumental
Meal preparationWalking outsideHouseworkShoppingHandling moneyPhone useSelf-medicationUsing public transport
The ability to perform these different activities unaided typicallydoes not decline at the same rate with increasing age. This is shownin Figure 1, which is based on data from a Finnish study of over1,000 older people aged from 60 years of age upwards (Ferrucci etal., 1998). Figure 1 shows that whereas nearly 50% of people agedover 60 reported not being able to do heavy housework, only 3%reported not being able to feed themselves.
Figure 4. Prevalence of functional limitation by activity
Ageing - a triumph, a crisis, a challenge?Population ageing represents a triumph of social development andpublic health. It should therefore be viewed as a positivedevelopment, not a problem or a crisis. The focus of the health andsocial services should be on prolonging independence, participation
0 5 10 15 20 25 30 35 40 45 50
Prevalence of Limitation (%)
Heavy housework
Cut own toenails
Shopping daily
Light housework
Cooking for oneself
Bathing/Showering
Walking 400m
Using stairs
Dressing/Undressing
Using lavatory
Getting in/out of bed
Feeding oneself

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 18 of 45
and quality of life, and on helping to unlock the enormous resourceof experience, wisdom and skills that the older population provides.
Assistive technology has an important role to play in this approach. Itcan help older people to do things that would otherwise be difficultand can enhance the dignity and reciprocity of caring relationships.
! Review and context activity - summary of ageing section
Summarise the core message of this section. Discuss the implications fromdifferent perspectives, e.g. the ageing person, your profession, socialpolicy, ...
1.4 Challenges of disability and ageing
Although the experiences of ageing and disability are to a largeextent determined by the nature of the society that we live in, theynevertheless do pose practical challenges at a number of levels:
• for disabled people and older people themselves• for family carers• for health and social services• for society as a whole.
Implications for disabled people and older people themselves
Given the preceding discussions it should be evident that, at least inan ideal world, having a disability or an age-related functionallimitation should not necessarily cause restrictions in daily life. Toput it simply, the impact will be minimised if the environment, in thebroadest meaning of the word, is conducive to the needs of disabledpeople and older people. This includes:
• design (buildings, transport, equipment, etc.)• attitudes (of employers, service providers, and indeed everyone
in society)• availability of help and support (from formal or informal sources
of care) and• availability of assistive technology.
In practice, of course, things are seldom as perfect as this. Indeed, inmany European countries various aspects of the environment (apartfrom informal care and support) are often very poorly developed.This means that having a disability or a functional limitation canresult in significant negative impacts.
Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 19 of 45
One area of impact ison the capacity to liveindependently in thecommunity. This is thedesired situation for thevast majority of people,including older peopleand younger peoplewith disabilities.However, without asupportive environment(including necessaryassistive technology)disabled people andolder people may losetheir independence evento the extent of ending up in residential care. At a minimum, manywill experience difficulties in carrying out the everyday activities ofdaily living. Other impacts include the difficulties that disabledpeople of working age often have in gaining employment(unemployment rates of up to 80% can be found in some of theEuropean countries) and restricted opportunities in many other areasof life, including access to education and social life more generally.
Assistive technologies that support activities of everyday life haveenormous potential to minimise functional limitations and otherimpacts of disability for the individuals concerned.
Challenges for family carers
Although the health and social services play a crucial role, it isrecognised that family members provide the bulk of care and supportfor disabled people and older people. In the case of younger peopleand children, parents are the usual providers of care. In the case ofolder people, a spouse or adult child (usually a daughter) are thetypical primary carers.
Although family care is given in the context of the ties andreciprocities that are at the core of family relationships, it must alsobe recognised that provision of care can be very demanding and canhave significant costs for the care providers. At a practical level, carecan be physically demanding and can result in physical strains andeven injury (back injury caused by inappropriate lifting being themost common). Perhaps even more important are the psychologicaland emotional strains that can result, especially where care isprovided 24-hours per day and opportunities for respite are limited ornon-existent. Caring for people with dementia (for example,Alzheimer's disease) can be particularly stressful.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 20 of 45
Opportunity costs must also be taken into account. In particular, careresponsibilities can reduce or eliminate the employmentopportunities of carers.
Again, assistivetechnologiesoffer enormouspotential tominimise thesestrains andrestrictions.They cansupport theprovision ofcare in apractical sense(e.g. hoists toassist with lifting) and can also, of course, enable more self-care. Inthis way they can be very liberating for both carer and cared-for.
Challenges for the health and social services
Disability and age-related functional limitations pose a variety ofchallenges for the health and social services as well. These includethe question of how best to provide quality care and support withinthe context of the cost containment pressures being experienced inmost countries.
Again we willsee that assistivetechnology canplay a majorrole in both thepractical aspectsof care deliveryand in meetingstrategic cost-benefit goals.With regard toquality issues,assistivetechnology canoften be a prime contributor to meeting the goals of independence,participation and quality of life.
With regard to cost-containment, it has been demonstrated thatassistive technologies can be very cost-effective solutions in manyareas of service delivery (e.g. tele-alarm services can save costs interms of acute and long-term hospital or other forms of residentialcare).

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 21 of 45
Challenges for society as a whole
Overall, these practical aspects of ageing and disability, alongside theneed to ensure that older people and disabled people are afforded fullrespect, dignity and rights, pose fundamental challenges for societyas a whole. In fact, it has been suggested that the level ofdevelopment and civilisation of a society can be measured by thequality of its treatment of its disabled and older citizens.
Assistive technology is often a pre-requisite for equality ofopportunities for full participation and for a good quality of life fordisabled people and older people, so society has a duty to make surethat appropriate technologies are available and affordable.
In the future these issues are going to become even more critical. Onthe one hand, the ageing of the population will mean that olderpeople and disabled people make up an increasing proportion of thepopulation. On the other hand, there will be labour market pressuresthat encourage the participation of disabled people, later retirementof older people, and more participation by the traditional providers ofcare for older people and disabled people - women in their middleyears.
Again, assistive technology can play a significant role. Wideavailability of assistive technology options would be greatlyliberating for all of us.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 22 of 45
2 A GLIMPSE OF ASSISTIVE TECHNOLOGY
This section provides an initial introductory overview of assistivetechnology. The aim is to give the student an appreciation of thevariety of types of technology and their uses. More in-depthtreatment of particular technologies will be provided in latermodules.
2.1 A wide variety - high-tech and low-tech, dedicated and general-purpose
There are literally thousands of assistive technology products andservices available. They range from simple low-tech devices to thelatest in high-tech computers, smart homes and robotics. Included areboth general-purpose items that are of particular benefit to olderpeople and disabled people and dedicated devices that have beenspecifically designed with the needs of disabled people and olderpeople in mind.
! Context activity - scope of assistive technology
Explore the scope of assistive technology.
You can find overviews of assistive technology:1. In databases and catalogues held by the agency or agencies providing
assistive technology services in your country or region (find out whothey are and see what information they provide);
2. By acquiring catalogues from commercial retailers of assistivetechnology (you may get information on these from the nationalagencies mentioned above or in the classified telephone directory);
3. By visiting web-based sites such as http://www.rehadat.de/ orhttp://www.abledata.com/
General-purpose items can be very useful
Many assistive technology products serve both people withfunctional restrictions and those without. These products makeactivities easier and more efficient for everyone. Examples includethe electric toothbrush, electric tin opener, long-handled shoe horn,fruit peeling machine and palm, foot or armrests (supporting

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 23 of 45
wrists/arms/legs whilst using a keyboard or other activities). Suchproducts are usually available in ordinary retail outlets.
Specifically-designed products from specialist outlets
Other assistive technologies (such as the majority of those describedin later sections) are specifically designed with the needs of disabledpeople or older people in mind. These products tend to be madeavailable through specialist outlets, provided either by private sectorretailers or public sector assistive technology services.
The ‘assistive technology’ can be in the design
Some assistive technology comes not in the form of special productsbut rather in the way they are designed. For example, a water tap thathas a turning knob is harder to use for those with frail hands than onewith a lever handle; a tap with one handle for more/less and hot/coldwater by be even easier to use. Such a product may initially havebeen designed as, and still be considered as, a luxury but also canmake daily activities easier and support independent living.
The terms ‘design for all’ or ‘universal design’ are used to describedesign approaches where there is an explicit aim to design productsand services so that they meet the needs and circumstances of thewidest possible range of users, including disabled people and olderpeople. Further information on ‘design for all’ can be found athttp://www.stakes.fi/include/
Wide price range
Whilst it may be commonly thought that assistive technology isprimarily 'high-tech, expensive equipment', many assistivetechnology products are in fact low-tech and cost less than 100 ECU.Products like a flashing doorbell, memory telephone or magnifyingruler cost no more than a book. Of course, there are also moreexpensive items, such as powered wheelchairs costing as much as asmall car or television loops costing in the region of 2500 ECU's.
‘Medical’ assistive technologies
Although as noted earlier, medical technologies are generally outsidethe scope of this course, nevertheless some of the productscommonly included in a broad definition of assistive technologyhave a medical dimension.
Many of these products are becoming more common in home care ascitizens aim to stay in their familiar environment as long as possibleand social policy makers across Europe try to reduce the length ofhospital stays.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 24 of 45
Such technology goes beyond the standard medical thermometer thatis present in every household and includes items such as medicationorganisers, glucose monitors (also available in low vision design forpeople with diabetes-related vision problems), blood pressuremonitors, high-low beds and aerosol equipment.
2.2 Assistive technology for different problem areas
One way to begin to appreciate the range of technologies that areinvolved is to consider the types of assistance and support that mightbe needed for some of the more commonly experienced problems ofdisabled people or older people.
! Research activity - Assistive Technology
Write down 10 examples of assistive technology. Then write down 10examples of assistive technology in the room that you are sitting in. Look atthe answers and describe the difference between them.
Physical functioningIn the area of physical functioning the typesof assistive technology of relevance cover awide range. Examples include walkingaids, wheelchairs, aids for reaching andlifting, aids for manipulation of objects andlifting aids.
Hearing
For hearing problems there aretwo main categories - devices toaugment residual hearing (hearingaids) and the wide variety ofdevices that can substitute visualor vibrating signals for auditorysignals. The latter include texttelephones, vibrating or flashingalarms, text captioning facilities in video cassette recorders and manyother devices and adaptations.
VisionFor visual problems, again there are twomain categories - in this case devices toaugment residual vision (e.g. magnifiers)and devices to substitute auditory ortactile signals for visual signals, forexample speech output and Braille.
Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 25 of 45
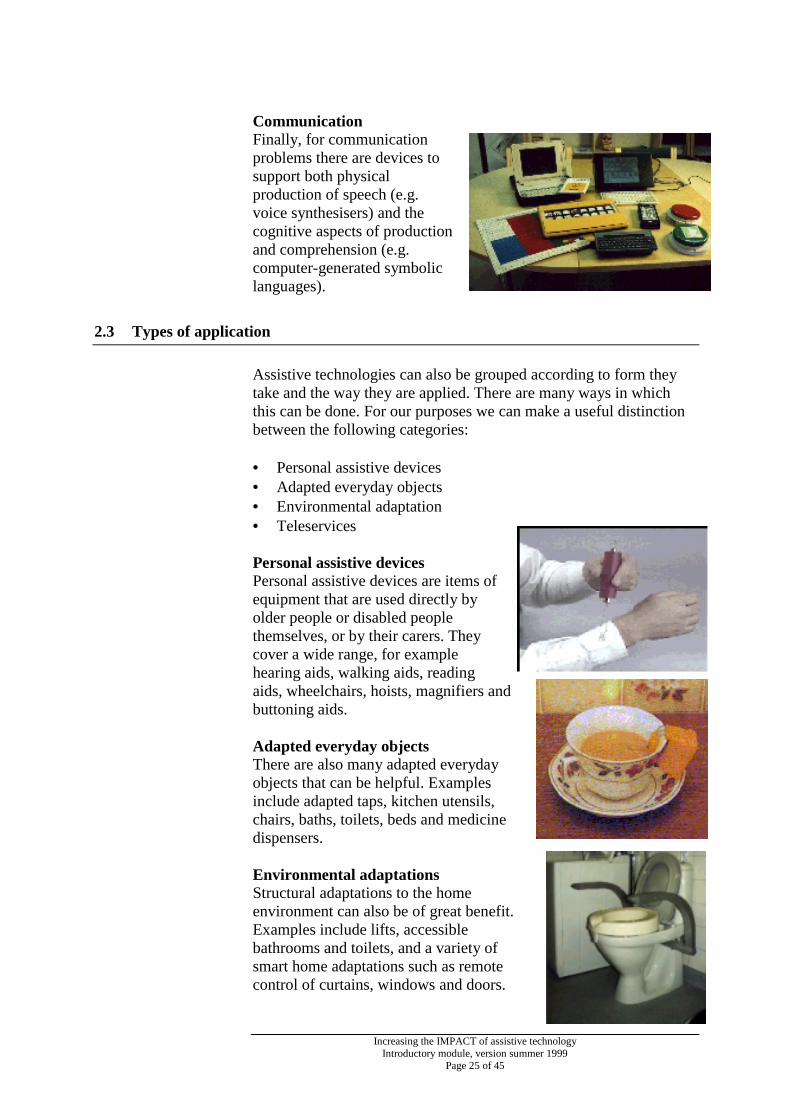
CommunicationFinally, for communicationproblems there are devices tosupport both physicalproduction of speech (e.g.voice synthesisers) and thecognitive aspects of productionand comprehension (e.g.computer-generated symboliclanguages).
2.3 Types of application
Assistive technologies can also be grouped according to form theytake and the way they are applied. There are many ways in whichthis can be done. For our purposes we can make a useful distinctionbetween the following categories:
• Personal assistive devices• Adapted everyday objects• Environmental adaptation• Teleservices
Personal assistive devicesPersonal assistive devices are items ofequipment that are used directly byolder people or disabled peoplethemselves, or by their carers. Theycover a wide range, for examplehearing aids, walking aids, readingaids, wheelchairs, hoists, magnifiers andbuttoning aids.
Adapted everyday objectsThere are also many adapted everydayobjects that can be helpful. Examplesinclude adapted taps, kitchen utensils,chairs, baths, toilets, beds and medicinedispensers.
Environmental adaptationsStructural adaptations to the homeenvironment can also be of great benefit.Examples include lifts, accessiblebathrooms and toilets, and a variety ofsmart home adaptations such as remotecontrol of curtains, windows and doors.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 26 of 45
TeleservicesTelecommunications play an increasingly important role in allaspects of life today and have allowed a range of ‘teleservices’ to beadded to the repertoire of assistive technologies for older people anddisabled people. These are services based on telecommunicationsthat allow things to be done from a distance.
Teleshopping,for example, canbe very helpfulfor people whohave difficultiesleaving home.Videotelephonescan enablepeople who aredeaf tocommunicate bysign language orlip-reading.Health andsocial servicescan also be delivered remotely nowadays. A familiar example wouldbe the tele-alarm systems that are now quite commonly used byvulnerable older people in many countries. Other examples aretelemedicine and the delivery of various social services byvideotelephony.
2.4 Contexts of use
For purposesof thiscourse ourprimaryinterest is inassistivetechnologiesfor use fordaily livingpurposes,whether athome orabroad in thewidercommunity.There arealso a wide variety of applications of technology oriented towardsemployment, education and transportation. These are of great

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 27 of 45
importance in enabling full participation in all aspects of social andeconomic life in today's society.
! Classifying assistive technology
While exploring the scope of assistive technology, highlight some of theways to classify the many products and services.
Your answers should include whether they are:• low-tech or high-tech• low-cost or high-cost• available across the counter or need to be personally adapted• for personal use or for environmental adaptations, and• the various other classificatory dimensions discussed above.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 28 of 45
3 HOW DO PEOPLE ACQUIRE ASSISTIVETECHNOLOGY?
This section provides an overview of the services (so-called‘assistive technology service delivery systems’) that are provided inthe European countries to help people to acquire the assistivetechnology that they need. You will see that there are a variety ofapproaches and levels of service in the different countries.
3.1 The different systems in different countries
A major European survey of assistive technology services wascarried out in 1993 under the EU-funded HEART study (de Witte etal., 1994). This study found that there were a wide variety ofapproaches in the different countries. Each country has its ownunique system. To simplify matters, the countries can be groupedinto clusters sharing certain key features in common. Below, someexamples of countries in four clusters - Scandinavian, ContinentalEuropean, Mediterranean, and UK and Ireland - are provided.
The country descriptions provide a brief summary of the situation inthe following areas:• eligibility and financing• the professionals who identify needs and make assessments, and• decision making and supply of assistive technology
The material is based on the work of the HEART study and reflectsthe situation as it prevailed in 1993. One point to note is there is a lotmore detail available for some countries than for others. This cansometimes be a little misleading, in that more problems may becomeapparent when we have more detailed information. Therefore, itshould not be surmised that the fact that an issue is not mentioned fora given country indicates that everything is fine for that country!
Overall, however, although the situation may have changed andimproved in some cases since 1993, the descriptions below give auseful illustration of the main types of system and their relativestrengths and weaknesses.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 29 of 45
Scandinavian countries
Under the ‘socialised’ systems of the Scandinavian countries,assistive technology services and policy are clearly stated andsupported by legislated rights. Services are provided independent ofthe user's financial situation; they are free of charge and provision isbased on need. However, even universal services such as these canbe susceptible to the economic climate, and economic recession canlead to restrictions in the actual provision of technical aids.
DenmarkAll citizens are eligible, independent of their financial situation, tothe assistive technology they require. The costs are financed bytaxes. Municipalities and counties have the primary financialresponsibility for aids for persons living at home. For persons over65 years the municipality pays the cost; for persons less than 65years, counties and municipalities share the cost.
The person requiring assistive technology contacts their municipalsocial worker or the county TAC (technical aids centre) for adviceand assessment. Assessment sometimes requires specialist expertise,e.g. from organisations representing blind or deaf persons. Decisionsare made locally in the municipality, usually by the social worker.Aids are provided from local stocks or ordered from dealers free ofcharge.
FinlandTechnical aids that are provided under health and welfare legislationare free of charge. The main responsibility for providing aids lieswith municipal health care at local health centres. Costs are met atthe municipality level from their own tax revenue or state grants. Inthe past, financial constraints have led to limitations in the actualprovision of aids, with the most severely impaired persons having thestrongest claim on funds.
Services are easily accessible but not always known. The personrequiring technical aids is often first made aware of assistivetechnology services by home care personnel. An assessment is madeby a welfare worker, physiotherapist or other professional, includingan assessment of the person's home environment. Decisions are takenat a higher level by a physician or financial officer. Technical aidcentres (TAC) may deliver aids from stock or order it from suppliers.
Continental European countries
Under the continental European ‘pluralist’ systems, there is often aproblem with the complexity of the system and the dividedresponsibility of insurance schemes. Theoretically, everyone shouldreceive the assistive technology they require, but sometimes it is hardto find out from whom. Another source of confusion is sometimes

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 30 of 45
the great selection and variety of aids available on the market. Healthand social service professionals may find it difficult to get a clearpicture of the appropriate range of aids, and people can end up beingpoorly and inadequately provided for.
The NetherlandsTechnical aids are not universally provided or always free of charge.The system is complex and specific regulations cover specificsituations. Persons under 65 years are covered by social insurance,implemented through care insurers. Provisions for disabled peopleare typically covered by social insurance and not by the health caresystem. People over 65 years are often not covered by socialinsurance and their needs may be covered by General FinancialAssistance if they fall below a certain income level.
Generally, if aged less than 65 years, a person requiring assistivetechnology applies to their care insurers. They decide on theapplication following advice from its medical assessment unit. Partof the cost of the aid (the first ECU 65 in 1993) is paid by theapplicant and many low-tech aids can cost less than this. Aids areclassified as fixed or non-fixed, with non-fixed aids covered by theabove procedure. For aids, which must be fixed to walls, applicationis made to the local community for assessment and funding. Again,part of the cost is paid by the applicant (the first ECU 220 in 1993)and costs over a certain level (ECU 7000 in 1993) are reimbursed ininstalments.
Older people applying for technical aids will be covered by socialinsurance if the impairment occurred before 65 years of age. If theimpairment is acquired after 65 years, the person is not covered andhas to pay unless eligible for community financial support because oflow income, or unless the aid is required for medical reasons. Forexample, a socially active 68-year-old man on an average pensionwho has recently become deaf will have to pay for a text telephonehimself.
GermanyAssistive technology aids are financed under various statutoryinsurance schemes, typically health insurance or pension insurance.The cause of disability is very relevant in determining which sector isfinancially responsible, and sometimes there is difficulty in agreeingresponsibility. Negotiation between insurance bodies is quitecommon and in complex cases the person may be sent from door todoor because no one accepts responsibility. Funding in relation tohome care for older people has involved both pension and healthinsurance but a new nursing and care insurance has been introduced.Persons outside the statutory insurance schemes, which are typicallylinked to employment, are considerably disadvantaged and must relyon benefits under social assistance.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 31 of 45
The person requiring an aid or their family starts the process byasking for a medical prescription from a physician, e.g. a prescriptionfor a computer peripheral for a blind person. A medical report givingthe cause of impairment and a prescription (with a cost estimate forthe technical aid) are necessary when applying for funding from theresponsible insurance body. The medical service of the statutoryinsurance scheme then assesses the necessity for the aid, for exampletext telephones are often not accepted as necessary.It is useful for the person and their family to inform themselves ofthe range of aids available before consulting the doctor as he or shemay have only a limited familiarity with what is available. Choice ofaids is restricted to a Catalogue of Aids, covering an extensive list ofmanufacturers and products. Insurance schemes only pay for aidsprescribed from the list. Comprehensive technical aid centres do notyet exist, but large assistive technology exhibitions regularly takeplace.
Mediterranean countries
In general, although there are considerable variations acrosscountries in the levels of service provided, services in theMediterranean countries tend to be less well developed than in othercountries.
SpainProvision of technical supports is in principle universal but inpractice lack of funds limits the supply of aids. The basic criterionfor support is possession of a Certificate of Handicap, with a similarcertificate required for older people.The next distinction is whether applicants qualify for support fromthe National Health System, in which case listed aids are supplied bylegal right. For those not eligible for free health care, support fromthe social services is discretionary and subject to financialavailability. For blind people, there is a strong voluntaryorganisation, which supports funding of technical aids.
A person or their family looking for assistive technology will firsthave to find out where to get help. Unless being discharged from ahospital setting, the person is likely to have a difficult time seekingsupport. When approached, social services may have littleknowledge of technical aids.They may have some lists of products and distributors, but areunlikely to carry out a serious assessment of needs. The person ortheir family going to a private store will be in the hands of thesalesperson. Upon presentation of the bill, part of the cost may berefunded depending on an investigation of financial circumstances.Even when coming out of hospital, there may be little knowledge andexperience of technical aids, and normally the family must help untila rehabilitation period is over.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 32 of 45
ItalyAll persons registered as disabled have the right through the NationalHealth System to receive assistive devices listed in the NationalRegister. Other devices may be provided by Social Assistancethrough the municipalities, depending on the disabled person's needsand economic circumstances. Disabilities (other than those due tolabour accidents) are assessed by a medical panel in the local healthunits and this can take from months to years. Eligibility for assistivedevices requires 34% disability.
As in many other countries, the person in need of assistivetechnology will first have to come to the attention of the relevantservices, of course, and there are no systematic procedures to ensurethat this will always happen.
UK and Ireland
UKThere is no uniform policy on the provision of technical aids. LocalAuthority (or municipality) social service departments have primaryresponsibility for home care and daily living aids, with provisionbeing non-statutory, and services are developed depending on theamount of finance available. Many authorities chose not to makecharges until recently, but many have now begun to charge forpreviously free services. When provided free but where funds are notavailable, the person will be placed on a waiting list. Local housingdepartments provide grants for major home adaptations; these aremeans-tested or income related. Devices required for medical reasonsare funded by the National Health Service. A separate wheelchairservice exits for the free provision of wheelchairs.
A person requiring technical aids may approach the local SocialServices Department. Assessment is usually carried out by anoccupational therapist or sometimes by a relevant voluntary agencyunder contract. Factors taken into account are the degree of need,degree of impairment, degree of isolation and likely level of usage.Decisions are made by the assessor's senior manager. Depending onlocal conditions, the aid can be provided free of charge, or partiallyfunded on a means-tested basis, or the request may be put on awaiting list. If the person is assessed as not yet being an urgent case,it can take three months to 18 months to receive the equipment.
IrelandTechnical aids are supplied free of charge only to fully eligibleapplicants, basically medical card and long-term illness cardholders.The process of delivering technical aids is the responsibility of thecommunity care services of the eight regional Health Boards.However, in many cases specialised voluntary organisations providethe service for deaf, blind or speech impaired persons and arerefunded by the health boards or from their own resources. The cost

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 33 of 45
of aids to applicants is dependent on financial status. Costs are fullycovered for holders of general medical cards, for aids provided froma standard product list. Items of higher cost may require acontribution from the applicant. Non-card holders will be asked topay part or all of the cost.
The person seeking a technical aid is referred to the health boardcommunity care service by their doctor, health nurse, social workeror other professional. A health board occupational therapist willassess the person and their claim for an aid. Claims for daily livingand mobility aids are processed directly by community care services.Approval is made by a health board programme manager. Otherrequests may be referred on to voluntary organisations that provideservices and sometimes financial support in this area.
3.2 Key themes and issues
A number of observations can be made about the services that areavailable in the European countries. First, it is clear that they varysignificantly in their level of universality and in the range of productsand services that are provided. Second, there is considerablevariation in terms of the types of professionals that are involved andin the nature of their involvement. In some cases medical doctorsplay a key role, even to the extent of it being necessary to have amedical prescription for assistive technology before being eligiblefor public financing. In other cases, a variety of professionals mayplay a key role, including occupational therapists, social workers,community nurses and home helps. Third, there are wide differencesin the extent to which there are systematic procedures in place topick up unmet needs and also in the extent to which services areintegrated and comprehensive follow-up is ensured once needs areinitially identified.
! Review activity
Explore the assistive technology services further in your country.
• How do these operate for people with physical, vision, hearing andcommunication impairments?
• What are the advantages and disadvantages of the way these servicesoperate in your country?
• What are the main problem areas?• What are the key organisations?

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 34 of 45
4 MANY UNMET NEEDS FOR ASSISTIVETECHNOLOGY
4.1 Introduction
Despite the wide range of useful technologies and the existence ofpublic assistive technology services in every country, it isdisappointing to have to note that very many older people anddisabled people in Europe are currently not availing of the potentialthat is on offer. Although the extent of under-utilisation variessignificantly across countries, there is no country in which it can besaid that everyone who needs or could benefit from assistivetechnology is currently doing so. This section looks at the extent ofunmet needs and at some of the main factors that have given rise tothis very unsatisfactory situation.
Margaret
Margaret, a middle-aged Irish woman living in a rural area west of Dublin,has been caring for her elderly father for several years. For about 5 monthsshe has been getting up every two hours at night to turn her father over, inorder to prevent pressure sores. Then she discovered that special mattressesare available to reduce the likelihood of sores developing. Once one ofthese was provided, Margaret was able to sleep through the night and wasmuch more capable of providing good quality care during the day.
Martin
Martin, an active 75-year-old citizen of Antwerp, is struggling with loss ofhearing. Increasingly, he finds social contacts more tedious. Friends andfamily visit him less often because he talks very loudly, his younggrandchildren have become a bit scared of this 'shouting' man and hisspouse complains daily about the loudness of the TV. After a long time heeventually accepted the facts and agreed to the installation of a simple,homemade television amplification system. Now everyone is much happierin Martin's household.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 35 of 45
4.2 The extent of unmet needs
There is extensive under-utilisation of assistive technology by thosewho could benefit from it. Levels of take-up are highest in the Nordiccountries and lowest in the Mediterranean countries and Ireland, withthe remaining countries somewhere in between. Although there hasnot yet been any comprehensive and systematic quantification of thesituation across the various disability and older person groupings,there is much evidence to support this assessment of the currentsituation. For example:
• In many countries, the majority of older people with functionallimitations use few if any assistive technologies, not even basiclow-price adaptations and devices.
• There are wide variations across countries in the levels ofavailability and take-up of what are considered to be basicrequirements and are universally provided in the more advancedcountries; for example there are only small numbers of users oftele-alarm services in the Mediterranean countries compared withlarge numbers of users in the Nordic countries.
• There are also wide variations in the take-up of technologies thatare essential for participation in the everyday life of society; forexample, text telephones are essential for many deaf people ifthey are to be able to make and receive telephone calls but only asmall proportion of deaf people have them in Ireland and in thesouthern countries, compared to much larger numbers in theNordic countries.
4.3 Why are unmet needs so commonplace?
Poor quality of assistive technology services in many countries
One cause of this situation is the poor quality of the (public) assistivetechnology service delivery systems in many countries. These are theservices described in the last section that are provided by state,regional and municipal agencies to identify needs for assistivetechnologies and make available the necessary technologies. Asidentified in the already-mentioned HEART study, there aresignificant problems with the existing services in many countries.
Under financingOne problem concerns lack of finance. Because disabled people tendto have lower than average incomes and older people, although onaverage being better off now than they have been previously, are at arelatively high risk of poverty in a number of countries, availabilityof public financing is an important determinant of the extent of take-

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 36 of 45
up of assistive technologies. In many countries the extent of publicfinancing is very limited and provided under quite stringentcircumstances.
Lack of co-ordinationLack of co-ordination and unclear responsibilities are other commonproblems. Often, responsibilities for delivering assistive technologyservices are not formally specified for particular professions and/orbranches of the health and social services. Also, responsibilities maybe distributed, often arbitrarily, across sectors (including health,social services, education and employment). As a consequence manypeople fall through the net and do not get the assistive technologythat they need.
Lack of comprehensivenessAnother problem concerns the range of technologies and/or the rangeof users that are covered within the scope of the assistive technologyservices in the different countries. As noted before, older people areoften not explicitly catered for. Also, there is often a tendency toprovide quite well for people who need assistive technology foreducational or occupational purposes but less well or not at all forpeople who need them for everyday living. The services in thedifferent countries also vary widely in the technologies that are madeavailable. In some countries, for example, electric wheelchairs arenot covered (only manual ones are financed), only some forms ofhousing adaptations are covered, and the more modern computer- ortelecommunications-based systems are often not provided.
No one place to goThe fact that some assistive technologies are to be found in general-purpose outlets and some only in specialist ones can also poseproblems. On the one hand, there are the difficulties caused by thelack of a ‘one-stop-shop’ where all necessary assistive technologiescould be acquired. There is also the related concern aboutstigmatisation, whether real or perceived, when assistive technologyis only available in special outlets for people who ‘have problems’.This can be an important factor in reducing uptake amongst olderpeople who could benefit significantly from assistive technology.
Needs not identified in the first place
Apart from these deficiencies in the publicly provided assistivetechnology services in many countries, there is also the problem ofneeds not being identified in the first place.
Lack of awarenessOne important factor is lack of awareness of assistive technology onthe part of disabled people and older people, and amongst familycarers and the public more generally. Again, there are widevariations across the European countries in this regard, with levels of

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 37 of 45
awareness apparently a lot higher in the Nordic countries comparedto some of the others.
Not enough attention from non-specialist professionalsGiven this situation of lack of awareness and the often poor qualityof formal systems of assistive technology service delivery, it wouldbe very helpful if all branches of the health and social services gave ahigh priority to addressing unmet needs for assistive technologywithin the scope of their work and their services to clients.Unfortunately this does not tend to be the case, and typically thecaring professions do not seem to give much attention, eitherorganisationally or individually, to unmet needs for assistivetechnology.
This gap is the main target of this course and the aim is to provide allrelevant health and social service personnel with the motivation andcompetencies to include assistive technology within the scope oftheir professional activities.
! Research activity - how to increase the attention given to assistivetechnology
As you know, this course is all about teaching health and social serviceprofessionals about the importance of assistive technology. Whatsuggestions do you have for ways to increase the attention given by yourprofession to this topic?

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 38 of 45
5 ABOUT THE REST OF THE COURSE - HOW TOBE AN ATI
This section outlines the structure and content of the remainder of thecourse. It also provides a first introduction to the concept of AssistiveTechnology Intermediary (ATI).
5.1 Assistive Technology Intermediaries
Teaching you how to become a so-called ‘Assistive TechnologyIntermediary’ (ATI) is what this course is all about. An ATI is ahealth and social service professional who, whilst not being aspecialist in assistive technology, nevertheless helps to ensure thathis or her clients acquire the assistive technology that they need.Being an ATI means watching out for unmet needs arising becauseof disability or because of age-related functional problems, andtaking appropriate action when such needs are spotted.
The following figure provides a summary of the key features of theATI role. You will come across this model in each of the othermodules of the course.
In essence, the role of ATI is quite straightforward - you need to bealert to functional difficulties and to unmet needs for assistivetechnology solutions.
Signals Follow upValidate
Help the clientto deal with it
Refer to an occupationaltherapist or other relevantspecialist service
Deal with ityourself

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 39 of 45
First, you need to be able to spot the signals that can indicate thatsomeone has a physical, hearing, visual or communication problem.In some cases you may also wish to validate or confirm this byapplying some simple checks or tests.
Once a need has been identified, there are various ways in which youcan help your client. There are three basic options:
• help your client to deal with the situation themselves• refer on to someone with more expertise and resources• deal with the problem yourself.
And, of course, in all cases you need to ensure appropriate
• follow-up.
Which option or combination of options you choose will depend verymuch on a variety of contextual factors:
• the type of need and the circumstances of the client• your familiarity with the particular functional difficulty in
question• the professional boundaries and competencies that apply in your
situation• the assistive technology solutions that are available and suitable• the characteristics of the prevailing assistive technology service
delivery system in your area.
In later modules you will find out more about how different types ofneeds can be spotted in the various client settings and what you cando as an ATI in the different situations.
5.2 Overview of the remaining modules
The rest of this course is organised into four core learning modulesand a final module that looks again, but in more detail, at how youcan act as an ATI. The four core modules cover:
• Physical functioning• Vision• Hearing• Communication
These areas have been selected for a number of reasons. First, theyare areas where functional difficulties commonly pose significantproblems in daily life. Second, they are areas where older people areparticularly likely to have unmet needs for assistive technologies.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 40 of 45
Third, they are areas where there are many assistive technologysolutions available, often simple devices that cost relatively little.
Older people who have acquired temporary or permanent disabilitieslater in life are the largest group who could benefit if all health andsocial service professionals were motivated to act effectively asATIs. However, whilst the emphasis in this course is often on olderpeople, attention must also be given to the needs of younger peopleas well because they too may slip through the net of existing assistivetechnology services.
Each of the modules addressing a specific problem area is organisedinto two parts:
• The main part introduces the problem area, the needs that it cangive rise to and the assistive technologies that can providesolutions
• Setting-specific parts then look at how the particular problemmay manifest itself in the different settings where health andsocial service professionals come into contact with older peopleor disabled people.
Three settings are addressed for each problem area:
• at home (visits by community nurses, home helps or socialworkers, for example);
• at the doctor (mainly family doctors, General Practitioners orother primary care physicians);
• in hospital (where various staff may be involved, includingdoctors, nurses or social workers).
At homeVarious professionals may be in contact with clients in the homesetting, especially home helps, community nurses and communitysocial workers. People living in residential care and the health andsocial service personnel caring for them are also addressed in thissetting. The home visit situation provides an ideal opportunity towatch out for unmet needs for assistive technology. You will be ableto see for yourself how well the client is functioning in their daily lifeand whether there are unmet needs where assistive technology canmake a contribution.
At the doctorCommon medical consultations such as visits to family doctors, localhealth clinics and hospital day clinics provide a crucial setting forspotting unmet needs for assistive technology. Because almosteveryone uses their services on a reasonably regular basis, familydoctors in particular can act as central gatekeepers to assistivetechnology services. In some countries this is already a formal part oftheir responsibilities but in others it is not an explicit aspect of the

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 41 of 45
professional role. It is important that medical practitioners take abroader view of their role and give as much attention to thefunctional requirements of everyday living as to the purely medicalaspects of their clients' conditions.
In hospitalHospitals are another very important setting for picking up andaddressing unmet needs for assistive technology. On the one hand,the consequences of a specific condition and/or treatment may giverise to a need for assistive technology. On the other hand, a hospitalstay gives a good opportunity to observe the more generalfunctioning of older people and to identify needs for assistivetechnology that may be unrelated to the immediate reason forhospitalisation and treatment. In either case, it is important that needsfor assistive technology are properly addressed in discharge planningand post-discharge follow-up.

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 42 of 45
6 REFERENCES
This module was designed to give you a brief overview of disability,ageing and assistive technology. If you are interested you can extendthis information by looking in your college library or through theresources of local association's for disabled people.
Alternatively, you can browse the World Wide Web for furtherinformation. Although you can start by searching with words like'disability', 'impairment' or 'assistive technology, we suggest you startat http://www.socialnet.lu/ where you will find a very extensive list ofweb sites under their ‘Handitel’ service.
Other sources of information cited in the text are:
• Cronin, N. & McGlone, F. (1993) Older People in the EuropeanCommunity. Family Policy Studies Centre: London
• De Witte, L., Johnson, I. & Parker, M. (1994) European ServiceDelivery Systems in Rehabilitation Technology. IRV:Hoensbrock, The Netherlands
• European Glossary on Technical Aids. European Commission:DGV, Helios-Handynet, 1996
• Eurostat Demographic Statistics 1997• Eurostat Disabled Persons Statistical Data 1995.• Ferrucci L. et al. (1998) Constant Hierarchic Patterns in Physical
Functioning across Five Countries. Gerontologist, 38:3:286-294• Guralnik J. at al. (1996) Disability as a Public Health Outcome in
the Ageing Population. Annual Review Public Health, 17:25-46• Sinclair, I. & Williams, J. (1990) Elderly people: coping and
quality of life. In: I. Sinclair et. al. The Kaleidoscope of Care: AReview of Research on Welfare Provision for Elderly People.HMSO: London

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 43 of 45
7 GLOSSARY
• ADL: activities of daily living - activities basic to personal careand maintenance (e.g. for nourishment, keeping warm, lookingwell-groomed)
• Disability: (the current term used in the WHO classification ofdisabilities; will be replaced by the term ‘activity’ in the future)any restriction or lack of ability, resulting from an impairment, toperform an activity in a manner considered normal for people
• Handicap: (the current term used in WHO classification ofdisabilities; will be replaced by the term ‘participation’ in thefuture) a disadvantage, resulting from an impairment or disabilitythat limits the fulfilment of individual goals
• IADL: instrumental activities of daily living - secondary activitiesinstrumental to sustaining the basic activities (ADLs) inindependent community living (e.g. shopping cooking)
• Impairment: (the current term used in WHO classification ofdisabilities) any loss or abnormality of a psychological,physiological or anatomical structure or function

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 44 of 45
8 FURTHER INFORMATION
" Activities from the WHO ICIDH-2 Classification of Activities
COMMUNICATION ACTIVITIES
Understanding messagesUnderstanding messages in speech and formal sign languageUnderstanding non-verbal messages (other than formal sign language)Understanding written language
Producing messagesProducing messages in speech or formal sign language
Communicating messagesProducing non-verbal messages other than formal sign languageProducing written language
Using communication deviceUsing communication devices / techniquesOther
MOVEMENT ACTIVITIES
Maintaining and changing body positionMaintaining a body positionShifting the weight of the bodyChanging a body position
Transferring oneselfWalking and related activitiesTransferring oneself while sitting or lying
Manipulating and moving objectsActivities involving fine hand useActivities involving arm and coarse hand useActivities aimed at making objects move
Other Unspecified
MOVING AROUND
Moving around without using transportationMoving around in the general environmentClimbingMoving around in specified environmentsMoving around in traffic situations as a pedestrian
Moving around using transportationUsing transportation

Increasing the IMPACT of assistive technologyIntroductory module, version summer 1999
Page 45 of 45
Moving around in traffic situations as a driverOther
DAILY LIFE ACTIVITIES
Keeping self clean and appropriately groomedWashing oneselfCare of body parts, teeth, nails and hairActivities related to excretionDressing
Eating and drinkingCaring for own well-beingDealing with everyday objects and appliancesOther
CARE OF NECESSITIES AND DOMESTIC ACTIVITIES
Procurement and care of necessitiesProcuring and taking care of daily necessities (e.g. shopping and
clothing)Procuring and taking care of shelter
Domestic ActivitiesTaking care of mealsLaundry and caring for clothes and footwearTaking care of dwelling
Caring for household members, animals and plantTaking care of other household or family membersLooking after possessions, plants and animals
Other
RESPONDING TO AND DEALING WITH PARTICULARSITUATIONS
Managing environmental demands and circumstancesManaging in specific climate or temperatureManaging in other environmental circumstancesManaging in a dangerous environment
Work- and school-related skillsWork- and school-related behavioursWork acquisition and retention skills
Social activities and economic skillsPersonal social activitiesEconomic skills
Other