incident prevention at work what you really did not know
TRANSCRIPT

Incident Prevention at Work ELIMINATE the RISK
Every day, more than 500 men or women do not come home because they were killed
by incidents at work. These are dramatic numbers which draw fairly little public
attention. Considering the fact that incidents take a considerable economic toll from
nations, companies and individuals, incidents do not get much publicity.
Fortunately there are people working with a sense of purpose, often behind the
scenes, towards understanding and managing safety and incident prevention better,
and their efforts have not been wasted. Our understanding of incident prevention and
safety is on a far higher level than ever before. We have left behind the simplistic
model of dividing behaviour and conditions into two categories: safe or unsafe.
The important observation is that two safe conditions which by themselves are safe,
may not be safe together. Workers are the connecting link, as their behaviour
changes according to the environment and their physical surroundings.
Every user of power saws knows from personal experience that this noisy, vibrating
and obviously sharp cutting tool appears to be very dangerous to use, and the
beginner operator is very cautious. However, after hours of experience operators
lose their sense of any hazard and start handling the saw less carefully. The
kickback guard may produce a similar effect. Operators who know kickback is
possible try to avoid it. When operators know that there is a mechanical device
preventing the saw from hurting them in event of kickback, they become less
cautious.
Even if these protective arrangements have been successful, in the final analysis
their effects do not have a linear relationship with safety. Two safe conditions,
kickback guard and leg protection, do not double the safety. The normal arithmetic
of one plus one equals two (1 + 1 = 2), does not apply in this case, as one plus one
makes less than two. Fortunately, one plus one (1 + 1) makes more than zero in some
cases. In other cases, however, the sum may even be negative.
The simple division of behaviours and conditions into safe and unsafe does not lead
very far toward prevention. The credit for progress has to be given to systems
management. After understanding that humans, their tasks, their equipment and the
environment make up a dynamic system, we have made considerable progress
towards more effective incident prevention.
Incident prevention has been traditionally based on learning from incidents and near
incidents (near misses). By investigating every incident, we learn about causes and
can take actions towards mitigating or removing the causes. The problem is that we
have not been able to develop, in the absence of sufficiently good theories,
investigation methods which would bring up all the relevant factors for prevention.
An investigation may give a fairly good picture about the causes. However, this

picture is usually relevant only for the specific case investigated. There may be
conditions and factors which contributed to the incident whose connections the
investigators do not recognize or understand. Generalizing from one incident to other
situations bears a degree of risk.
The new steps in safety management is the notion of
safety culture. It may be a difficult concept, since culture is not a visible entity. It is
an abstract concept prevailing within an organization or society. There are no direct
ways of adjusting it. Safety culture is, however, a crucial concept for understanding
the possibilities of prevention.
Calculating the magnitude of the incident problem; it is not a description of the
magnitude itself. In dealing with occupational incidents, the magnitude of the
problem can be estimated in different ways, depending on one’s need to estimate
how big the problem has been or how big it will be in the future. An incident may be
described as a result of a chain of events in which something has gone wrong,
resulting in an undesired conclusion. It has been shown that human intervention may
prevent the injury or damage to which such a chain of events would otherwise lead.
However, given the fact of human intervention, the potential exists for far more
dangerous possible chains of events than those actually leading to injury or damage.
These possibilities must be considered in assessing the full extent of workplace risk.
Assuming that events that might lead to injury or damage occur because of factors
in the workplace, one is led to conclude that the magnitude of the problem has to be
determined on the basis of the existence and frequency of such factors.
When dealing with incidents in the workplace, one can estimate the magnitude of
the problem retrospectively by comparing the number of incidents (incidence rate)
with the severity of the incidents (lost work days). However, if one wants to estimate
the magnitude of the problem prospectively, it is done by evaluating the presence of
risk factors in the workplace—that is, factors that might lead to incidents.
A sufficiently complete and accurate view of the state of affairs with respect to
workplace incidents can be gained by means of a comprehensive reporting and
record-keeping system. Analyses of well-prepared incident reports can give a picture
of the basic relationships essential to understanding the causes of the incidents. In
order to estimate the magnitude of the problem in detail, a determination of risk
factors is essential. Knowledge of the relevant risk factors can be obtained by
analyzing the detailed information provided with each incident record as to where
workers and operators were located when the incident occurred, what they were
doing or handling, by what means, what damages or injuries occurred and other
particulars surrounding the incident.
Risk
Risk measurement must be made on the basis of information regarding the number
and seriousness of injuries that have occurred in the past, yielding a retrospective
measurement. The risk of injury to individuals may be described by two types of
data:
� Measurement of risk provides a calculated frequency of injuries and a measurement
of the seriousness of the injury.
� Type of risk or element of danger assessment provides not only an indication of the
exposure sources and other harmful factors which may cause an incident, but also
an indication of the circumstances leading to injury or damage.
Many types of risk, not apparent to common sense, may be overlooked. With regard
to these, the worker must be informed of the risk (e.g., that noise causes hearing
damage, that some solvents cause brain damage and that certain chemicals cause
acute poisoning by inhalation). Our knowledge of types of risk, from the most to the
least conspicuous, whether gained through everyday experience or through research
efforts, is based on past events. However, it is one thing to know what has
happened, and another to assess what will happen in the future. It should be noted
that the very knowledge of the exposure sources and other potentially harmful
factors which may cause damage or injury in connection with tasks of various sorts,
as well as knowledge of the factors that can either heighten or reduce those risk
factors that influence risk measurement, can provide a basis for recognition of the
risk.
Factors Determining Risk
The factors which are of greatest relevance in determining risk are:
� factors which determine the presence or absence (or potential) of risks of any sort
� factors which either increase or minimize the probability of these risks resulting in
incidents or injuries

� factors affecting the seriousness of incidents associated with these risks.
To clarify the first point, it is necessary to identify the causes of the incident—
namely, exposure sources and other harmful factors; the two latter points constitute
the factors which influence the measurement of risk.
The primary factors in the working environment which are the direct causes of harm,
either by way of occupational diseases or occupational incidents, are as follows:
Exposure sources and occupational disorders
The concept of injuries due to exposure sources is often linked to the concept of
disease (or disorder) because a disease can be viewed as caused by exposure to one
or several agents over a short (acute exposure) or long (chronic exposure) period of
time. Chronic exposure agents are usually not directly harmful, but take effect rather
after a relatively constant and extended period of exposure, whereas acute
exposures are almost instantaneously harmful. The intensity, harmfulness and period
of action is of importance to the development of the injury, which may often be a
matter of a combination of the effects of several different agents. This fact makes it
difficult to point out and determine the exposure sources because (among other
reasons) monocausal correlations between specific disorders and specific exposure
sources are almost never found.
Examples of exposure sources which may result in an injury in the form of a disease-
like condition are:
� chemical exposures (solvents, cleaning agents, degreasing agents, etc.)
� physical exposures (noise, radiation, heat, cold, inadequate lighting, lack of oxygen,
etc.)
� physiological exposures (heavy loads, bad work postures or repetitive work)
� biological exposures (viruses, bacteria, flour, animal blood or leather, etc.)
� psychological exposures (work in isolation, threat of violence, changing working
hours, unusual job demands, etc.).
Harmful factors and occupational incidents
The concept of harmful factors (not including exposure sources) is linked to
occupational incidents, because this is where damages occur and workers are
exposed to the type of actions that cause instant injury. This type of action is easily
identified because the damage or injury is recognized immediately when it occurs.
The difficulty attached to this type of injury is the unexpected contact with the
harmful factor.

Controlling Exposures
Exposure sources or other harmful factors are to a great extent governed by the
nature of the processes, technologies, products and equipment to be found in the
workplace, but may also be governed by the way in which the work is organized.
From the point of view of measurable risk, it should be recognized that control of the
probability of exposures and the seriousness of injuries to workers often depends on
the following three factors:
� Elimination/substitution safety measures. Workplace hazards in the form of
exposure sources or other harmful factors may be eliminated or mitigated by
substitution (e.g., a less harmful chemical may replace a toxic chemical in a
process). It should be noted that this is not totally possible, as exposure sources and
other harmful factors will always be present in human surroundings (not least with
respect to human working conditions).
� Technical safety measures. These measures, often called engineering controls,
consist of separating persons from harmful factors by encapsulating the harmful
elements, or installing barriers between workers and the factors which may cause
injury. Examples of these measures include, but are not limited to, automation,
remote control, use of ancillary equipment and machine protection (guarding).
� Organizational safety measures. Organizational safety measures, also known as
administrative controls, include separating persons from harmful factors either by
means of special working methods or by separation in time or space.
Controlling Human Conduct
It is often not possible to isolate all hazards using the above control measures. It is
commonly supposed that incident prevention analysis ends here because it is
believed that the workers will then be able to take care of themselves by acting
“according to the rules”. This means that safety and risk will at some point depend
on factors which control human conduct—namely, whether the individual person has
the knowledge, the skills, the opportunity and the will to act so as to ensure safety
in the workplace. The following illustrates the role of these factors.
� Knowledge. Workers must first be aware of the types of risk, potential hazards and
elements of danger that may be found in the workplace. This usually requires
education, training and job experience. The risks also need to be identified,
analyzed, recorded and described in a readily understandable manner so that
workers know when they are in a specific risk situation and what consequences are
liable to follow from their actions.
� The opportunity to act. It must be possible for the workers to act safely. It is
necessary for workers to be able to make use of the available technical and
organizational—as well as physical and psychological—opportunities for action.
Positive support of the safety program must be forthcoming from management,
supervisors and the surroundings, including concern about risk taking, designing and
following working methods with safety in view, safe use of the proper tools, clearly
defining tasks, establishing and following safe procedures, and providing clear
instructions on how equipment and materials are to be safely handled.
� The will to act safely. Technical and organizational factors are important with
respect to workers’ readiness to behave in ways that will ensure workplace safety,
but social and cultural factors are at least equally important. Information on the
causes of incidents serves the following purposes:
� It can demonstrate where something is wrong and what needs to be changed.
� It indicates the types of harmful factors that cause incidents (or near incidents) and
also describes the situations that result in damage and injuries.
� It identifies and describes the underlying circumstances that determine the
presence of potential hazards and risky situations and that will result in optimum
safety by their being altered or eliminated.
Information of a general sort can be obtained by a thorough analysis of the damage
or injuries and the circumstances under which they occurred. Information obtained
from other similar incidents may point out more general factors of importance, thus
disclosing less immediately visible causal relationships.
Analysis of individual incidents has two primary purposes:
First, it can be used to determine the cause of an incident and the specific work
factors that contributed to it. Following analysis, one can assess the extent to which
the risk has been recognized. One may also decide upon technical and organizational
safety measures and the degree to which more job experience might have
diminished the risk. Furthermore, a clearer view is gained of the possible actions
that might have been taken to avoid the risk, and the motivation that a worker must
have to take these actions.
Second, one can gain knowledge which may be used for analyses of many similar
incidents at both the enterprise level and at more comprehensive (e.g., organization-
wide or national) levels. The identity of the workplace and the work itself (that is,
information relating to the sector or the trade in which the workplace is positioned),
and the work processes and the technology that characterize the work
� the nature and the seriousness of the incident
� factors causing the incident, such as exposure sources, the way in which the
incident occurred and the specific working situation causing the incident

� general conditions at the workplace and the working situation (comprising the
factors mentioned in the foregoing paragraph).
There are five primary types of analyses of incidents, each having a distinct purpose:
� Analyses and identification of where and which types of incidents occur. The goal
is to determine the incidence of the injuries, as associated, for example, with
sectors, trade groups, enterprises, work processes and types of technology.
� Analyses with respect to monitoring developments in the incidence of incidents.
The purpose is to be warned of changes, both positive and negative. Measuring the
effect of preventive initiatives may be the result of such analyses, and increases in
new types of incidents within a specified area will constitute warning of new risk
elements.
� Analyses to prioritize initiatives that call for high degrees of risk measurement,
which in turn involve calculating the frequency and seriousness of incidents. The
goal is to establish a basis for prioritization to determine where it is more important
to carry out preventive measures than elsewhere.
� Analyses to determine how the incidents occurred and, especially, to establish both
direct and underlying causes. This information is then applied to the selection,
elaboration and implementation of concrete corrective action and preventive
initiatives.
� Analyses for elucidation of special areas which have otherwise attracted attention
(a sort of rediscovery or control analyses). Examples include analyses of incidences
of a special injury risk or the discovery of a hitherto unrecognized risk identified in
the course of examining an already known risk.
Phases of the Analysis
Irrespective of the level from which an analysis starts, it will usually have the
following phases:
� identification of where the incidents occur at the general level selected
� specification of where the incidents occur at a more specific level within the
general level
� determination of goals in view of the incidence (or frequency) and seriousness of
the incidents
� description of exposure sources or other harmful factors—that is, the direct causes
of damage and injury

� examination of the underlying causal relation and causal development.
Different levels of incident analysis
The type of workplace risk is established by descriptions of the types of incidents
that take place and the way in which they arise within the individual workplace
areas. In this way, knowledge is obtained of the exposure sources and other harmful
factors present in the workplace in the event that preventive measures—attention to
safety conditions, awareness of risk, providing opportunity for action and the appeal
to the workers’ will—have proved insufficient to avert the incident.
Identification, measurement and description of incidents together provide the basis
for what is to be done and who is to do it in order to reduce the risk. If, for example,
specific exposure sources can be linked to specific technologies, it will help
determine what special safety measures are necessary to control the risk. This
information may also be used to influence manufacturers and suppliers associated
with the technology in question.

Incident Causation Theories
The domino theory
According to W.H. Heinrich (1931), who developed the so-called domino theory, 88%
of all incidents are caused by unsafe acts of people, 10% by unsafe actions and 2%
by “acts of God”. He proposed a “five-factor incident sequence” in which each factor
would actuate the next step in the manner of toppling dominoes lined up in a row.
The sequence of incident factors is as follows:
1. ancestry and social environment
2. worker fault
3. unsafe act together with mechanical and physical hazard
4. incident
5. damage or injury.
In the same way that the removal of a single domino in the row would interrupt the
sequence of toppling, Heinrich suggested that removal of one of the factors would
prevent the incident and resultant injury; with the key domino to be removed from
the sequence being number 3. Although Heinrich provided no data for his theory, it
nonetheless represents a useful point to start discussion and a foundation for future
research.
Multiple causation theory
Multiple causation theory is an outgrowth of the domino theory, but it postulates that
for a single incident there may be many contributory factors, causes and sub-causes,
and that certain combinations of these give rise to incidents. According to this
theory, the contributory factors can be grouped into the following two categories:
Behavioural. This category includes factors pertaining to the worker, such as
improper attitude, lack of knowledge, lack of skills and inadequate physical and
mental condition.
Environmental. This category includes improper guarding of other hazardous work
elements and degradation of equipment through use and unsafe procedures.
The major contribution of this theory is to bring out the fact that rarely, if ever, is an
incident the result of a single cause or act.

The pure chance theory
According to the pure chance theory, every one of any given set of workers has an
equal chance of being involved in an incident. It further implies that there is no
single discernible pattern of events that leads to an incident. In this theory, all
incidents are treated as corresponding to Heinrich’s acts of God, and it is held that
there exist no interventions to prevent them.
Biased liability theory
Biased liability theory is based on the view that once a worker is involved in an
incident, the chances of the same worker becoming involved in future incidents are
either increased or decreased as compared to the rest of workers. This theory
contributes very little, if anything at all, towards developing preventive actions for
avoiding incidents.
Incident proneness theory
Incident proneness theory maintains that within a given set of workers, there exists
a subset of workers who are more liable to be involved in incidents. Researchers
have not been able to prove this theory conclusively because most of the research
work has been poorly conducted and most of the findings are contradictory and
inconclusive. This theory is not generally accepted. It is felt that if indeed this theory
is supported by any empirical evidence at all, it probably accounts for only a very low
proportion of incidents without any statistical significance.
The energy transfer theory
Those who accept the energy transfer theory put forward the claim that a worker
incurs injury or equipment suffers damage through a change of energy, and that for
every change of energy there is a source, a path and a receiver. This theory is useful
for determining injury causation and evaluating energy hazards and control
methodology. Strategies can be developed which are either preventive, limiting or
ameliorating with respect to the energy transfer.
Control of energy transfer at the source can be achieved by the following means:
� elimination of the source
� changes made to the design or specification of elements of the work station
� preventive maintenance.

The path of energy transfer can be modified by:
� enclosure of the path
� installation of barriers
� installation of absorbers
� positioning of isolators.
The receiver of energy transfer can be assisted by adopting the following measures:
� limitation of exposure
� use of personal protective equipment.
The “symptoms versus causes” theory
The “symptoms versus causes” theory is not so much a theory as an admonition to
be heeded if incident causation is to be understood. Usually, when investigating
incidents, we tend to fasten upon the obvious causes of the incident to the neglect
of the root causes. Unsafe acts and unsafe conditions are the symptoms—the
proximate causes—and not the root causes of the incident.
Structure of Incidents
The belief that incidents are caused and can be prevented makes it imperative for us
to study those factors which are likely to favour the occurrence of incidents. By
studying such factors, the root causes of incidents can be isolated and necessary
steps can be taken to prevent the recurrence of the incidents. These root causes of
incidents can be grouped as “immediate” and “contributing”. The immediate causes
are unsafe acts of the worker and unsafe working conditions. The contributing
causes could be management-related factors, the environment and the physical and
mental condition of the worker.

Structure of incidents
Incident causation is very complex and must be understood adequately in order to
improve incident prevention. With such a diversity of theories, it will not be difficult
to understand that there does not exist one single theory that is considered right or
correct and is universally accepted. These theories are nonetheless necessary, but
not sufficient, for developing a frame of reference for understanding incident
occurrences.
HUMAN FACTORS IN INCIDENT MODELLING
Traditional models of incident causation placed superficial emphasis on human
factors. Where human factors were included, they were depicted as linked to error
occurring in the immediate sequence of events leading to the incident.

Incident Causation Models
Recent models have extended the role of human factors beyond the immediate
causal events leading to the incident. Models now tend to include additional factors
in the wider circumstances of the incident.
Model of incident causation
The Nature of Error
An essential component of incident prevention, therefore, is gaining an
understanding of the nature, timing and causes of error. One of the important and
unique characteristics of error, distinguishing it from other factors involved in
incidents, is that error is a normal part of behaviour. Error plays a fundamental role
in learning new skills and behaviours and in maintaining those behaviours. Through
testing the boundaries of interactions with the environment, and consequently
making errors, humans learn just what the boundaries are. This is essential not only
for learning a new skill but also for updating and maintaining ones they have already
learned. The degree to which humans test the boundaries of their skills is related to
the level of risk that they are prepared to accept.
It seems that errors are a constant feature of all behaviour. Studies show also that
they occur in the causes of approximately two-thirds of work-related fatal incidents.
It is essential therefore to develop some ideas about the form they are likely to take,
and when and why they might occur. While there are many aspects of human error
that are not yet understood, our current level of understanding allows some
predictions to be made about error types. Knowledge of these types of error will, it is

to be hoped, guide our efforts to prevent error or at least to modify the adverse
consequences of error.
One of the most important features of the nature of error is that it is not a unitary
phenomenon. Even though traditional incident analysis often treats error as if it were
a singular entity which cannot be dissected further, there are a number of ways that
errors can occur. Errors differ depending on the information-processing function
being challenged.
A second characteristic of errors is that they are not novel or random. Error forms
are limited. They take similar forms in all types of functions. This means that the
error forms that occur in everyday life in the kitchen, for example, occur in the same
manner in the most high-risk industries. The consequences of these errors, however,
are very different and are determined by the setting in which the error occurs, rather
than by the nature of the error itself.
These categorizations of error distinguish between those occurring during skilled
behaviour (slips, lapses or unintended acts) and those occurring during unskilled or
problem-solving behaviour (mistakes).
Slips or skill-based errors are defined as unintended errors occurring when the
behaviour is a highly practiced routine or automatic in nature.
Mistakes have been further categorized into two types:
� rule-based errors, which occur when the behaviour requires the application of rules
� knowledge-based errors, which occur during problem solving when the person has
no skill or rule to apply.
This means that knowledge-based errors occur through lack of expertise, rule-based
Elaboration of the involvement of human factors other than human error in the
circumstances immediately surrounding the incident represents a major advance in
understanding incident genesis. While there is no question that error is present in
most incident sequences, human factors are also involved in a broader sense, taking
the form, for example, of standard operating work procedures and the influences that
determine the nature and acceptability of work procedures, including the earliest
decisions of management.
The conventional view of incidents as a number of things suddenly going wrong at
the time and the place of the incident, concentrates attention on the overt
measurable event at the time of the incident.
Thus, to understand how incidents occur, how people contribute to them and why
they behave the way that they do, it is necessary to ensure that analysis does not

begin and end with the circumstances that most directly and immediately lead to
harm.
In acknowledging the potential aetiological significance of the wider circumstances
surrounding the incident, the model best describing incident causation has to take
into account the relative timing of elements and how they relate to each other.
First, causal factors vary in terms of their causal importance, and also in terms of
their temporal importance. Furthermore, these two dimensions can vary
independently; that is, causes can be important because they occur very close in
time to the incident and therefore they reveal something about the time of the
incident, or they can be important because they are a prime cause underlying the
incident, or both. Second, incidents are generally agreed to be multicausal. Human,
technical and environmental components in the work system can interact in critical
ways. Third, these two considerations, the nature of the event and the nature of its
contribution to the incident, interact. Although multiple causes are always present,
they are not equivalent in role.
Effective prevention would be best served if it were targeted towards the latent
underlying causes, rather than the immediately precipitating factors. This level of
understanding of the causal network and how it influences outcome is possible only
if all types of factors are included for consideration, their relative timing is examined
and their relative importance is determined.
The first is the notion that people have a target level of risk—that is, the level of risk
they accept, tolerate, prefer, desire or choose. The target level of risk depends on
perceived benefits and disadvantages of safe and unsafe behaviour alternatives, and
it determines the degree to which they will expose themselves to safety and health
hazards.
The second premise is that the actual frequency of lifestyle-dependent death,
disease and injury is maintained over time through a closed-loop, self-regulating
control process. Thus, fluctuations in the degree of caution people apply in their
behaviour determine the ups and downs in the loss to their health and safety.
Moreover, the ups and downs in the amount of actual lifestyle-dependent loss
determine the fluctuations in the amount of caution people exercise in their
behaviour.
Finally, the third premise holds that the level of loss to life and health, in so far as
this is due to human behaviour, can be decreased through interventions that are
effective in reducing the level of risk people are willing to take—that is, not through
measures of the “safe cigarette” variety or other such efforts towards a
“technological fix” of the problem, but by means of programs that enhance people’s
desire to be alive and healthy.

Homeostatic model relating changes in incident loss to changes in operator
behaviour and vice versa, with the target level of risk as the controlling variable
In principle, there are four ways in which workers and drivers may be motivated to
lower their target level of risk:

� Reduce the expected benefits of risky behaviour alternatives.
� Increase the expected costs of risky behaviour alternatives.
� Increase the expected benefits of safe behaviour alternatives.
� Decrease the expected costs of safe behaviour alternatives.
While some of these approaches have been found to be more effective than others,
the notion that safety may be enhanced by acting upon motivation has a long history,
as is obvious from the universal presence of punitive law.
Punishment
Although enforcement of punitive law is one of society’s traditional attempts at
motivating people towards safety, the evidence for its effectiveness has not been
forthcoming. First is the “self-fulfilling prophecy” effect of attribution. For example,
labelling people with undesirable characteristics may stimulate individuals to
behave as if they had these characteristics. Treat people as if they were
irresponsible and eventually some will behave as if they were.
Second, the emphasis is on process controls; i.e., on specific behaviours such as
using a piece of safety equipment or obeying the speed limit, instead of focusing on
the end result, which is safety. Process controls are cumbersome to design and
implement, and they can never totally encompass all undesirable specific behaviours
of all people at all times.
Third, punishment brings negative side-effects. Punishment creates a dysfunctional
organizational climate, marked by resentment, uncooperativeness, antagonism and
even sabotage. As a result, the very behaviour that was to be prevented may in fact
be stimulated.
Encouragement
In contrast to punishment, incentive programs have the effect for which they are
intended, as well as the positive side-effect of creating a favourable social climate .
Behavioural Adaptation
According to risk homeostasis theory, the incident rate per person-hour of task
performance or the annual incident rate per head of population do not primarily
depend upon a person’s ability to be safe, nor upon the opportunity to be safe, but
instead upon that person’s desire to be safe.
Humans play important roles in most of the processes leading up to incidents and in
the majority of measures aimed at incident prevention. Therefore, it is vital that

models of the incident process should provide clear guidance about the links
between human actions and incidents. Only then will it be possible to carry out
systematic incident investigation in order to understand these links and to make
predictions about the effect of changes in the design and layout of workplaces, in
the training, selection and motivation of workers and managers, and in the
organization of work and management safety systems.
Individual problem solving in the face of danger
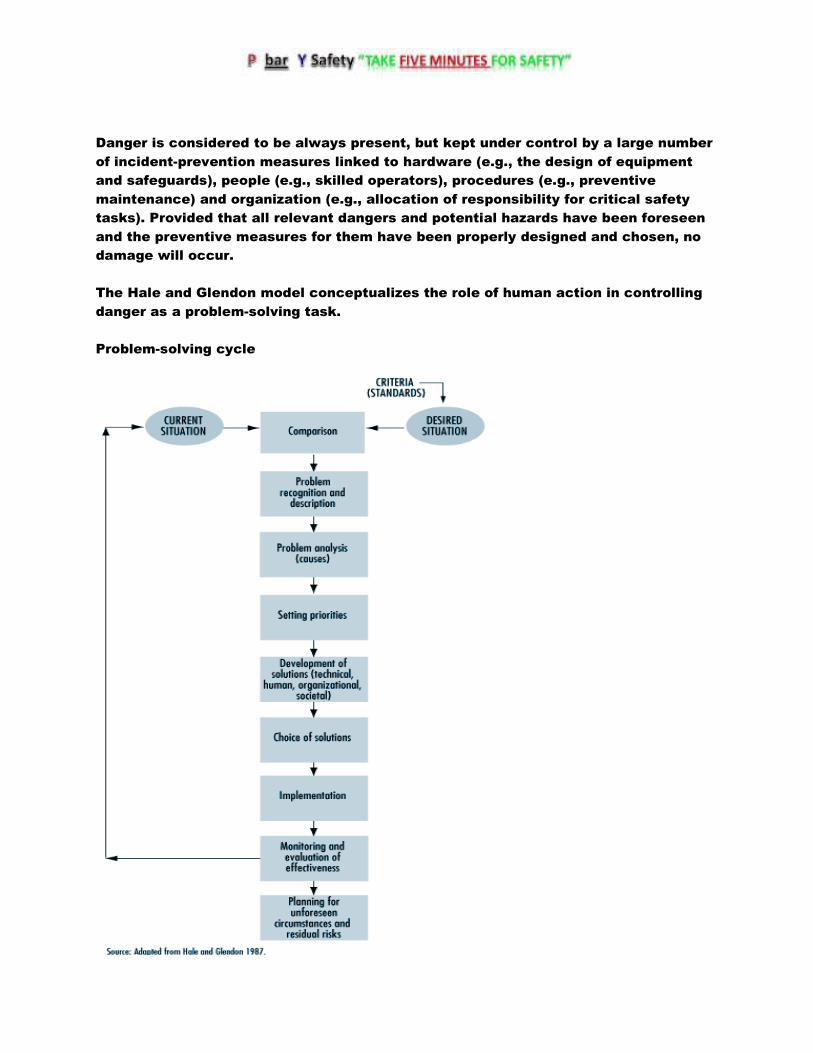
Danger is considered to be always present, but kept under control by a large number
of incident-prevention measures linked to hardware (e.g., the design of equipment
and safeguards), people (e.g., skilled operators), procedures (e.g., preventive
maintenance) and organization (e.g., allocation of responsibility for critical safety
tasks). Provided that all relevant dangers and potential hazards have been foreseen
and the preventive measures for them have been properly designed and chosen, no
damage will occur.
The Hale and Glendon model conceptualizes the role of human action in controlling
danger as a problem-solving task.
Problem-solving cycle

Hence safety management systems can be modelled in a consistent way with human
behaviour, allowing the designer or evaluator of safety management to take an
appropriately focused or a wide view of the interlocking tasks of different levels of
an organization.
Behaviour in the face of danger

These situations of imminent danger are rare in most industries, and it is normally
desirable to activate workers to control danger when it is much less imminent.
To ensure the appropriate quality of alertness, they must accustom themselves to
recognize potential incident scenarios—that is, indications and sets of indications
that could lead to loss of control and so to damage. This is partly a question of
understanding webs of cause and effect, such as how a process can get out of
control, how noise damages hearing or how and when a trench can collapse.
Just as important is an attitude of creative mistrust. This involves considering that
tools, machines and systems can be misused, go wrong, or show properties and
interactions outside their designers’ intentions. It applies “Murphy’s Law” (whatever
can go wrong will go wrong) creatively, by anticipating possible failures and
affording the opportunity of eliminating or controlling them. Such an attitude,
together with knowledge and understanding, also helps at the next step—that is, in
really believing that some sort of danger is sufficiently likely or serious to warrant
action.
Skill-based. The skill-based level is highly reliable, but subject to lapses and slips
when disturbed, or when another, similar routine captures control. The responses
are so automatic that workers may not even be aware that they are actively
controlling danger with them.
Rule-based. The rule-based level is concerned with choosing from a range of known
routines or rules the one which is appropriate to the situation—for example,
choosing which sequence to initiate in order to close down a reactor which would
otherwise become overpressurized, selecting the correct safety goggles to work
with acids (as opposed to those for working with dusts ), or deciding, as a manager,
to carry out a full safety review for a new plant rather than a short informal check.
Errors here are often related to insufficient time spent matching the choice to the
real situation, to relying on expectation rather than observation to understand the
situation, or to being misled by outside information into making a wrong diagnosis.
Knowledge-based. The knowledge-based level is engaged only when no pre-existing
plans or procedures exist for coping with a developing situation. This is particularly
true of the recognition of new hazards at the design stage, of detecting unsuspected
problems during safety inspections or of coping with unforeseen emergencies.

Surry’s model
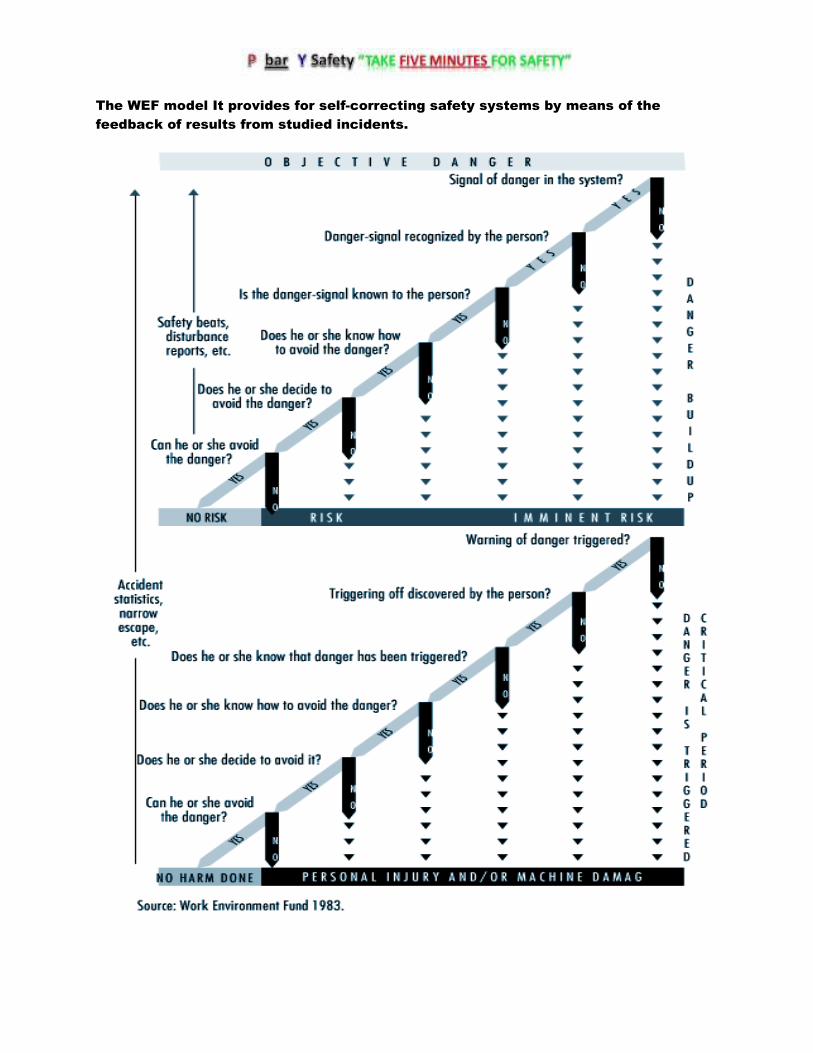
The WEF model It provides for self-correcting safety systems by means of the
feedback of results from studied incidents.

Hence, it becomes irrelevant and misleading to ask whether people know how to
avoid (and choose to avoid) something which is not really avoidable unless they
decide to quit their job.
� The model provides no insight into the important issue of why the dangerous
activity was necessary to begin with, and why it was performed by the specific
individual. Sometimes dangerous tasks can be made unnecessary; and sometimes
they can be performed by other, more appropriate persons with greater skills.
� The analysis is restricted to a single person, but many incidents occur in
interaction between two or more persons. However, it was suggested that this
deficiency could be overcome by combining the results of parallel analyses, each
made from the perspective of one of the different individuals involved. A tentative
comprehensive model, based on Surry’s original design and including these
additional elements, Tentative comprehensive model on incident causation

Deviations
The definition of deviations in relation to specified requirements coincides with the
definition of nonconformities in the International Organization for Standardization’s
ISO 9000 series of standards on quality management . The value of a systems
variable is classified as a deviation when it falls outside a norm. Systems variables
are measurable characteristics of a system, and they can assume different values.
Norms
There are four different types of norms. These relate to: (1) specified requirements,
(2) what has been planned, (3) what is normal or usual and (4) what is accepted.
Each type of norm is characterized by the way it has been established and its degree
of formalization.
Safety regulations, rules and procedures are examples of specified requirements. A
typical example of a deviation from a specified requirement is a “human error”,
which is defined as a transgression of a rule. The norms that relate to what is
“normal or usual” and what is “accepted” are less formalized. They are typically
applied in industrial settings, where the planning is oriented to outcome and the
execution of the work is left to the discretion of the operators.
The Time Dimension
Time is a basic dimension in the deviation model. An incident is analysed as a
process rather than as a single event or a chain of causal factors. The process
develops through consecutive phases, so that there is a transition from normal
conditions in the industrial system to abnormal conditions or a state of lack of
control. Subsequently, a loss of control of energies in the system occurs and the
damage or injury develops.
Analysis of an incident at a construction site on the basis of the OARU model

A distinction is made between corrective and preventive actions. Correction of
deviations coincides with the first order of feedback in Van Court Hare’s hierarchy of
feedback, and does not result in any organizational learning from the incident
experiences. Preventive actions are accomplished through higher orders of feedback
that involve learning.
Examples of taxonomies for the classification of deviations
Theory or model and variable Classes
Process model
Duration Event/act, condition
Phase of the incident sequence Initial phase, concluding phase, injury phase
Systems theory
Subject-object (Act of) person, mechanical/physical
condition
Systems ergonomics Individual, task, equipment, environment
Industrial engineering Materials, labour power, information,
technical, human, intersecting/parallel
activities, stationary guards, personal
protective equipment
Human errors
Human actions Omission, commission, extraneous act,
sequential error, time error
Energy model
Type of energy Thermal, radiation, mechanical, electrical,
chemical
Type of energy control system Technical, human
Consequences
Type of loss No significant time loss, degraded output
quality, equipment damage, material loss,
environmental pollution, personal injury
Extent of loss Negligible, marginal, critical, catastrophic

Application of the Deviation Model
The coverage of different tools for use in safety practice
For example, Safety sampling is a method for the control of deviations from safety
rules through performance feedback to the workers. Positive effects of safety
sampling on safe performance, as measured by the risk of incidents, have been
reported.
THE MERSEYSIDE INCIDENT INFORMATION MODEL
MAIM, the Merseyside Incident Information Model, which is most naturally adapted
to the second purpose—recording and storing incident information. Following an
outline of the rationale for MAIM, some early studies evaluating the model are
described. The article ends with recent progress with MAIM, including the use of
“intelligent software” to collect and analyses information on injury incidents.
A simple example illustrates the problem. A worker slips on a patch of oil, falls and
strikes his or her head on a machine and suffers a concussion. We can easily
distinguish the (immediate) cause of the incident (slipping on oil) and the cause of
the injury (hitting the head on the machine). Some classification systems, however,
include the categories “falls of persons” and “striking against objects”. The incident
could be allocated to either of these, although neither describes even the immediate
cause of the incident (slipping on oil) or causal factors (such as how did the oil get
on the floor).

The MAIM Incident Model
The behaviour of the equipment or person is described by the general activity at the
time and a more specific description of the type of corporal movement when the first
event occurred.

The example of a worker who slips on a patch of oil, falls and hits his or her head
provides an illustration. The first event is “foot slipped”—instead of remaining still,
the foot acquires kinetic energy. The second event is “fell”, when further kinetic
energy is acquired. This energy is absorbed by the collision of the worker’s head with
the machine when the injury occurs and the sequence ends. This can be “plotted”
onto the model as follows:
1. 1st event: foot slipped on oil.
2. 2nd event: person fell.
3. 3rd event: head struck against machine.
A number of principles guide the selection and implementation of prevention
measures in a public health approach to injury control. These include:
(1) The importance of basing prevention measures on prior assessment and
evaluation. The first principle acknowledges the importance of selecting
interventions that are targeted to have a high impact on community health status
and are likely to be successfully implemented. Thus, interventions selected on the
basis of a thorough assessment phase, rather than merely common sense, are more
likely to be effective. Interventions that have been demonstrated as effective in the
past are even more promising.
(2) The relative importance of control measures that automatically protect the
worker. The second principle emphasizes the continuum between active and passive
protection. Active protection is that which requires constant repetitive individual
action; passive protection offers relatively automatic protection. For example, seat-
belts require individual action to initiate protection each time someone gets into a
vehicle. An air bag, on the other hand, bestows protection on a vehicle occupant
without any initiating action—it automatically protects that person. Active
interventions require modifying and sustaining individual behaviour change, which
has been the least successful of injury prevention strategies to date. This principle is
similar to the traditional hierarchy of controls in occupational safety which
emphasizes the importance of engineering controls over administrative controls,
personal protective equipment and training.
(3) The importance of behaviour modification rather than education. The third
principle recognizes the importance of behaviour modification and that not all
hazards can be engineered out of the environment at the manufacturing stage.
Modification of the behaviour of employers, managers and employees is central, not
only to the installation and maintenance of passive protection, but to most other
occupational injury control strategies as well. Another important aspect of this
principle is that classroom instruction, posters, pamphlets and other forms of
education that merely seek to increase knowledge, usually have little effect on
behaviour when used alone.

The Haddon Matrix reveals that interventions targeted at humans, the vehicles
which can transfer damaging energy (e.g., cars, machinery), or the physical or
psychosocial environment may operate to control injury in the pre-event, event or
post-event phases.
The Haddon Matrix applied to motor vehicle injuries
Phases Factors
Human Vehicles and
equipment
Environment
Pre-event Educate public in the
use of seat-belts and
child restraints
Safe brakes and tires Improved road
design; restrict
alcohol advertising
and availability at
gas stations
Event Prevention of
osteoporosis to
decrease likelihood of
fracture
Air bags and a
crashworthy vehicle
design
Breakaway utility
poles and crash
barriers
Post-event Treatment of
haemophilia and other
conditions that result
in impaired healing
Safe design of fuel
tank to prevent
rupture and fire
Adequate emergency
medical care and
rehabilitation
Haddon’s Ten Countermeasure Strategies shows how these strategies can be
applied to controlling injury from falls in construction. As shown, not all strategies
will be applicable for specific problems.
Countermeasure Intervention (and relevant notes)
Prevent the creation of the hazard. Do not construct buildings—generally
not a practical option, to be sure.
Reduce the amount of the hazard
brought into being.
Lower the height of construction
project to below fatal levels—usually
not practical, but may be possible in
some work zones.
Prevent the release of the hazard. Install non-slip walking surfaces on
roofs and other heights.
Modify the rate of release of the
hazard from its sources.
Use safety lanyards. Use safety nets.
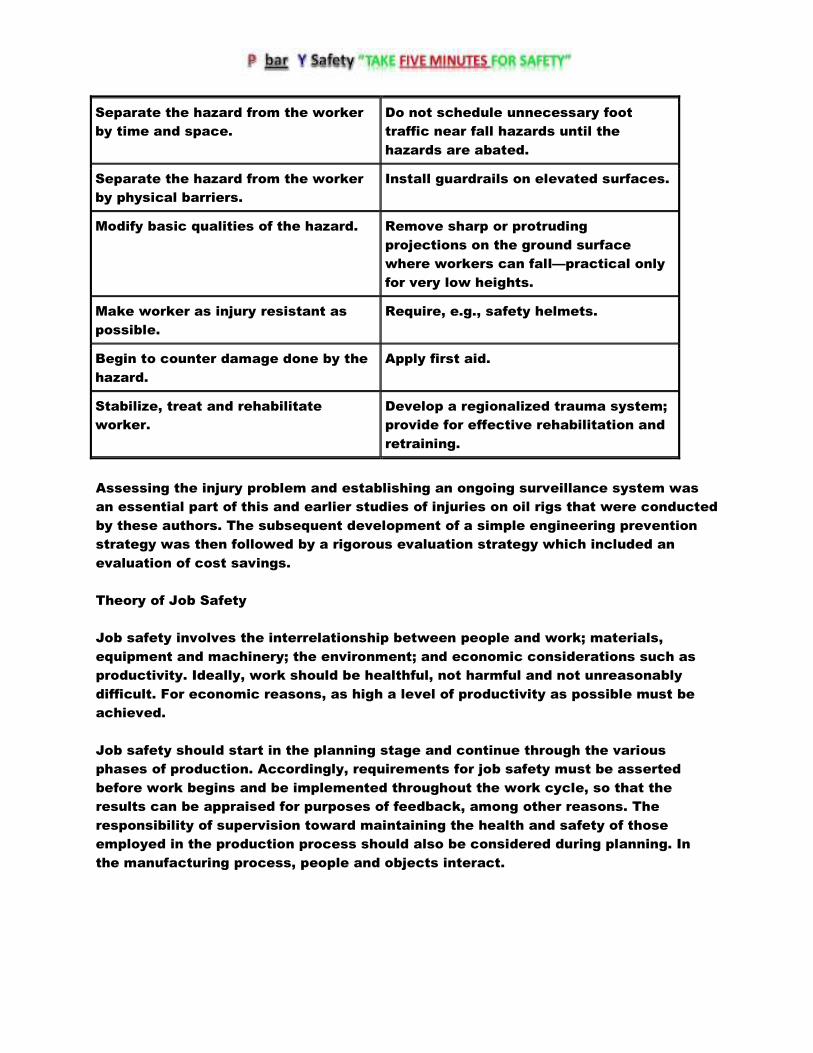
Separate the hazard from the worker
by time and space.
Do not schedule unnecessary foot
traffic near fall hazards until the
hazards are abated.
Separate the hazard from the worker
by physical barriers.
Install guardrails on elevated surfaces.
Modify basic qualities of the hazard. Remove sharp or protruding
projections on the ground surface
where workers can fall—practical only
for very low heights.
Make worker as injury resistant as
possible.
Require, e.g., safety helmets.
Begin to counter damage done by the
hazard.
Apply first aid.
Stabilize, treat and rehabilitate
worker.
Develop a regionalized trauma system;
provide for effective rehabilitation and
retraining.
Assessing the injury problem and establishing an ongoing surveillance system was
an essential part of this and earlier studies of injuries on oil rigs that were conducted
by these authors. The subsequent development of a simple engineering prevention
strategy was then followed by a rigorous evaluation strategy which included an
evaluation of cost savings.
Theory of Job Safety
Job safety involves the interrelationship between people and work; materials,
equipment and machinery; the environment; and economic considerations such as
productivity. Ideally, work should be healthful, not harmful and not unreasonably
difficult. For economic reasons, as high a level of productivity as possible must be
achieved.
Job safety should start in the planning stage and continue through the various
phases of production. Accordingly, requirements for job safety must be asserted
before work begins and be implemented throughout the work cycle, so that the
results can be appraised for purposes of feedback, among other reasons. The
responsibility of supervision toward maintaining the health and safety of those
employed in the production process should also be considered during planning. In
the manufacturing process, people and objects interact.

Worker-Job Relationships
The following three possible relationships within the manufacturing process indicate
how personal injury incidents (especially incidents) and harmful working conditions
are unintended effects of combining people and the objective working environment
for the purpose of production.
1. The relationship between the worker and the objective working environment is
optimal. This means well-being, job safety and labour-saving methods for the
employees as well as the reliability of the objective parts of the system, like
machines. It also means no defects, incidents, incidents, near misses (potential
incidents) or injuries. The result is improved productivity.
2. The worker and the objective working environment are incompatible. This may be
because the person is unqualified, equipment or materials are not correct for the job
or the operation is poorly organized. Accordingly, the worker is unintentionally
overworked or underutilized. Objective parts of the system, like machines, may
become unreliable. This creates unsafe conditions and hazards with the potential for
near misses (near incidents) and minor incidents resulting in delays in production
flow and declining output.
3. The relationship between the worker and the objective working environment is
completely interrupted and a disruption results, causing damage, personal injury or
both, thereby preventing output. This relationship is specifically concerned with the
question of job safety in the sense of avoiding incidents.
Principles of Workplace Safety
Because it is apparent that questions of incident prevention can be solved not in
isolation, but only in the context of their relationship with production and the
working environment, the following principles for incident prevention can be derived:
1. Incident prevention must be built into production planning with the goal of
avoiding disruptions.
2. The ultimate goal is to achieve a production flow that is as unhindered as
possible. This results not only in reliability and the elimination of defects, but also in
the workers’ well-being, labour-saving methods and job safety.
Some of the practices commonly used in the workplace to achieve job safety and
which are necessary for disruption-free production include, but are not limited to the
following:
� Workers and supervisors must be informed and aware of the dangers and potential
hazards (e.g., through education).

� Workers must be motivated to function safely (behaviour modification).
� Workers must be able to function safely. This is accomplished through certification
procedures, training and education.
� The personal working environment should be safe and healthy through the use of
administrative or engineering controls, substitution of less hazardous materials or
conditions, or by the use of personal protective equipment.
� Equipment, machinery and objects must function safely for their intended use, with
operating controls designed to human capabilities.
� Provisions should be made for appropriate emergency response in order to limit the
consequences of incidents, incidents and injuries.
The following principles are important in understanding how incident prevention
concepts relate to disruption-free production:
1. Incident prevention is sometimes considered a social burden instead of a major
part of disruption prevention. Disruption prevention is a better motivator than
incident prevention, because improved production is expected to result from
disruption prevention.
2. Measures to ensure workplace safety must be integrated into the measures used
to ensure disruption-free production. For example, the instructions on hazards must
be an integral part of the general directions governing the flow of production at the
workplace.
Incident Theory
An incident (including those that entail injuries) is a sudden and unwanted event,
caused by an outside influence, that causes harm to people and results from the
interaction of people and objects.
Often the use of the term incident in the workplace is linked with personal injury.
Damage to a machine is often referred to as a disruption or damage, but not an
incident. Damage to the environment is often called an incident. Incidents, incidents
and disruptions which do not result in injury or damage are known as “near
incidents” or “near misses”. So while it may be considered appropriate to refer to
incidents as cases of injury to workers and to define the terms incident, disruption
and damage separately as they apply to objects and the environment, in the context
of this article they will all be referred to as incidents.
The conceptual model for the term incident indicates that workplace incidents occur
from workers and objects interacting with each other through the release of energy.
The cause of an incident can lie in the characteristics of the injured worker (e.g., not
capable of performing the work safely) or of the object (e.g., unsafe or unsuitable
equipment). The cause can also be another worker (providing erroneous information),
supervisor (receiving incomplete job instructions) or trainer (receiving incomplete or
incorrect training). The following can be derived for incident prevention:
Potential Hazards and Risks
Although a hazard or danger may exist in an object, if the worker and the object are
so separate from one another that they cannot come into contact, no incident is
possible. The risks of incidents are different in various workplaces, under various
conditions. For example, the risks involved in drilling for oil, using the same workers
and identical equipment, differ widely depending on the geography (drilling on land or
off shore) and the climate (Arctic exploration or deserts). The level of incident risk
depends on:
� the anticipated frequency of error of the worker and the technology (number per 1
million hours, etc.)
� the probability of the errors resulting in incidents (incident: error = 1:x)
� the probability of the seriousness level of the incident.
The acceptance of incident risks also varies widely. High incident risk appears to be
acceptable in road traffic whereas a zero base tolerance is expected in the field of
nuclear energy. For purposes of incident prevention, it therefore follows that the
driving force is the smallest possible acceptance of incident risk.
Causes of Incidents
The occurrence of an incident requires classification on a scale from cause to effect.
Three levels must be differentiated:
� the level of the causes of possible and actual incidents
� the level of the incident’s origins
� the level of the incident’s consequences in the form of personal and material
damages.
Cause is the reason for the incident. Almost every incident has multiple causes such
as hazardous conditions, combinations of factors, courses of events, omissions and
so on. It is important to differentiate the factors associated with the production
process from the incident causes linked to workers (conduct of the immediate
operator), the organization (safe work procedures or policies) and technical incident
causes (environmental changes and object failures). However, in the final analysis,
every incident results from faulty conduct of people, because people are always at

the end of the causal chain. For example, if faulty material is determined to be the
cause of a boiler bursting, then improper conduct existed either on the part of the
builder, manufacturer, tester, installer or owner (e.g., corrosion due to inadequate
maintenance).
Effect of Strains and Demands
Mechanization and automation of production processes have advanced considerably
in recent years. It may appear that the causes of many incidents have shifted from
human error to those related to the maintenance of and interface with automated
processes. However, these positive consequences of technology are counterposed
to other, negative ones, particularly the increase in psychological strains and
corresponding ergonomic physical demands on workers in automated plants due to
the increased attention and responsibility required for overseeing the automated
operations process, impersonal working environment and monotony of work. These
strains and corresponding demands increase the occurrence of incidents and can be
harmful to health.
1. Strains are effects on workers which originate in the workplace, such as
environmental strains (temperature, heat, humidity, light, noise and air pollution), or
they can be static or dynamic strains originating directly from the work process
(lifting, climbing, chemical exposure and so on). Strain levels can be physically
measured (noise, force, atmospheric exposures and so on), whereas strain factors
are physically unmeasurable influences (fatigue, mental stress, plant
worker/management relationships and so on).
2. Demands on workers are dependent on the type and degree of the strain as well
as differing individual capability to withstand the strain. Effects of demands show up
physically and psychologically in the human body. The effects of the demands can be
desirable or undesirable, depending on the type and degree. Undesirable effects,
such as physical and psychological exhaustion, work aggravations, illness, lack of
coordination and concentration, and unsafe behaviour cause increased risk of
incident.
Near Incidents (Near Misses)
A large part of production loss results from disruptions in the form of near misses
(near incidents), which are the basis of occurrences of incidents. Not every
disruption affects work safety. Near incidents (near misses) are those occurrences
or incidents in which no injury or damage resulted, but if injury or damage had
occurred, they would be classified as incidents.
Incident Pyramid
Incidents are relatively rare occurrences, and usually the more serious the incident,
the more rare the occurrence. Near incidents form the bottom, or base, of the

incident pyramid, whereas fatal incidents stand at the top. If lost time is used as a
criterion for the seriousness of incidents, we find a relatively high degree of
correspondence with the incident pyramid. (There may be a slight deviation as a
result of the reporting requirements of different countries, companies and
jurisdictions.)
From the incident pyramid, it follows for purposes of incident prevention that:
1. Incident prevention begins with avoiding near incidents (near misses).
2. Eliminating minor incidents usually has a positive effect on eliminating serious
incidents.
Incident Prevention
The different paths of incident prevention for ensuring workplace safety are as
follows:
1. Eliminate the hazard or danger so that injury or damage is no longer possible.
2. Provide for separation between the worker (or equipment) and the hazard (equal to
elimination of the hazard). The danger remains, but an injury (or damage) is not
possible since we make sure that the natural zones of influence of workers
(equipment) and object (hazard or danger) do not intersect.
3. Provide shielding, such as fireproofing, protective clothing and respirators to
minimize the hazard. The hazard still exists, but the possibility of an injury or
damage is reduced by minimizing the chances of the hazard having an effect by
shielding the danger.
4. Adapt to the hazard by providing measures such as warning systems, monitoring
equipment, information about dangers, motivation for safe behaviour, training and
education.
Four Stages of the Incident Sequence
Task stage in incident sequence
Prior to task Routine task
performance
Abnormal task
conditions
Incident
conditions
Objectives
(Behavioural)
Educate and
persuade worker of
the nature and
level of risk,
precautions,
Instruct or
remind
worker to
follow safe
procedures
Alert worker of
abnormal
conditions.
Specify needed
actions.
Indicate
locations of
safety and first
aid equipment,
exits and

remedial measures
and emergency
procedures.
or take
precautions.
emergency
procedures.
Specify remedial
and emergency
procedures.
Example
sources
Training manuals,
videos or
programs, hazard
communication
programs, material
safety data sheets,
safety propaganda,
safety feedback
Instruction
manuals, job
performance
aids,
checklists,
written
procedures,
warning
signs and
labels
Warning
signals: visual,
auditory, or
olfactory.
Temporary
tags, signs,
barriers or
lock-outs
Safety
information
signs, labels, and
markings,
material safety
data sheets
First stage. At the first stage in the incident sequence, sources of information
provided prior to the task, such as safety training materials, hazard communication
program and various forms of safety program materials (including safety posters and
campaigns) are used to educate workers about risks and persuade them to behave
safely.
Second stage. At the second stage in the incident sequence, sources such as written
procedures, checklists, instructions, warning signs and product labels can provide
critical safety information during routine task performance.
Third stage. At the third stage in the incident sequence, highly conspicuous and
easily perceived sources of safety information alert workers of abnormal or
unusually hazardous conditions.
Fourth stage. At the fourth stage in the incident sequence, the focus is on expediting
worker performance of emergency procedures at the time an incident is occurring, or
on the performance of remedial measures shortly after the incident. Safety
information signs and markings conspicuously indicate facts critical to adequate
performance of emergency procedures (e.g., the locations of exits, fire
extinguishers, first aid stations, emergency showers, eyewash stations or
emergency releases). Product safety labels and SDSs may specify remedial and
emergency procedures to be followed.

Summary of recommendations within selected warning systems such as GHS
pictograms and standards in general for worker ease of understanding
System Signal words Colour
coding
Typograp
hy
Symbols Arrangement
ANSI Z129.1
Hazardous
Industrial
Chemicals:
Precautionar
y Labeling
(1988)
Danger
Warning
Caution
Poison
optional
words for
“delayed”
hazards
Not
specified
Not
specified
Skull-and-
crossbones
as
supplement
to words.
Acceptable
symbols for
3 other
hazards
types.
Label
arrangement
not specified;
examples given
ANSI Z535.2
Environment
al and
Facility
Safety Signs
(1993)
Danger
Warning
Caution
Notice
(general
safety)
(arrows)
Red
Orange
Yellow
Blue
Green
as above;
black and
white
otherwise
per ANSI
Z535.1
Sans
serif,
upper
case,
acceptabl
e
typefaces
, letter
heights
Symbols
and
pictographs
per ANSI
Z535.3
Defines signal
word, word
message,
symbol panels
in 1 to 3 panel
designs. 4
shapes for
special use.
Can use ANSI
Z535.4 for
uniformity.
ANSI Z535.4
Product
Safety Signs
and Labels
(1993)
Danger
Warning
Caution
Red
Orange
Yellow
per ANSI
Z535.1
Sans
serif,
upper
case,
suggeste
d
typefaces
, letter
heights
Symbols
and
pictographs
per ANSI
Z535.3; also
SAE J284
safety alert
symbol
Defines signal
word, message,
pictorial panels
in order of
general to
specific. Can
use ANSI
Z535.2 for
uniformity. Use
ANSI Z129.1 for
chemical
hazards.
NEMA
Guidelines:
NEMA 260
(1982)
Danger
Warning
Red
Red
Not
specified
Electric
shock
symbol
Defines signal
word, hazard,
consequences,
instructions,
symbol. Does

not specify
order.
SAE J115
Safety Signs
(1979)
Danger
Warning
Caution
Red
Yellow
Yellow
Sans serif
typeface,
upper
case
Layout to
accommoda
te symbols;
specific
symbols/
pictographs
not
prescribed
Defines 3 areas:
signal word
panel, pictorial
panel, message
panel. Arrange
in order of
general to
specific.
ISO
Standard:
ISO R557
(1967); ISO
3864 (1984)
None. 3
kinds of
labels:
Stop/prohibiti
on
Mandatory
action
Warning
Red
Blue
Yellow
Message
panel is
added
below if
necessar
y
Symbols
and
pictographs
Pictograph or
symbol is
placed inside
appropriate
shape with
message panel
below if
necessary
OSHA
1910.145
Specification
for Incident
Prevention
Signs and
Tags (1985)
Danger
Warning
(tags only)
Caution
Biological
Hazard,
BIOHAZARD,
or symbol
(safety
instruction)
(slow-moving
vehicle)
Red
Yellow
Yellow
Fluorescent
Orange/oran
ge-red
Green
Fluorescent
yellow-
orange and
dark red per
ANSI Z535.1
Readable
at 5 feet
or as
required
by task
Biological
hazard
symbol.
Major
message
can be
supplied by
pictograph
(tags only).
Slow-
moving
vehicle
(SAE J943)
Signal word and
major message
(tags only)
OSHA
1910.1200
(Chemical)
Hazard
Communicati
on (1985)
Per
applicable
requirements
of EPA, FDA,
BATF, and
CPSC; not
otherwise
specified.
In English Only as Material
Safety Data
Sheet
Westinghous
e Handbook
(1981); FMC
Danger
Warning
Caution
Red
Orange
Yellow
Helvetica
bold and
regular
Symbols
and
pictographs
Recommends 5
components:
signal word,

Guidelines
(1985)
Notice Blue weights,
upper/low
er case
symbol/pictogra
ph, hazard,
result of
ignoring
warning,
avoiding hazard
Cognitive guidelines
Design specifications, such as those discussed above, can be useful to developers of
safety information. However, many products and situations are not directly
addressed by standards or regulations. Certain design specifications may not be
scientifically proven, and, in extreme cases, conforming with standards and
regulations may actually reduce the effectiveness of safety information. To ensure
effectiveness, developers of safety information consequently may need to go beyond
safety standards.
A model for designing and evaluating product information

Workers who are the victims of work-related incidents suffer
from material consequences, which include expenses and loss of earnings, and from
intangible consequences, including pain and suffering, both of which may be of short
or long duration. These consequences include:
� doctor’s fees, cost of ambulance or other transport, hospital charges or fees for
home nursing, payments made to persons who gave assistance, cost of artificial
limbs and so on
� the immediate loss of earnings during absence from work (unless insured or
compensated)
� loss of future earnings if the injury is permanently disabling, long term or precludes
the victim’s normal advancement in his or her career or occupation
� permanent afflictions resulting from the incident, such as mutilation, lameness,
loss of vision, ugly scars or disfigurement, mental changes and so on, which may
reduce life expectancy and give rise to physical or psychological suffering, or to
further expenses arising from the victim’s need to find a new occupation or interests
� subsequent economic difficulties with the family budget if other members of the
family have to either go to work to replace lost income or give up their employment
in order to look after the victim. There may also be additional loss of income if the
victim was engaged in private work outside normal working hours and is no longer
able to perform it.
� anxiety for the rest of the family and detriment to their future, especially in the
case of children.
Workers who become victims of incidents frequently receive compensation or
allowances both in cash and in kind. Although these do not affect the intangible
consequences of the incident (except in exceptional circumstances), they constitute
a more or less important part of the material consequences, inasmuch as they affect
the income which will take the place of the salary. There is no doubt that part of the
overall costs of an incident must, except in very favorable circumstances, be borne
directly by the victims.

When passing from the abstract concept of an undertaking to the concrete reality of
those who occupy senior positions in the business (i.e., the employer or the senior
management), there is a personal incentive which is not only financial and which
stems from the desire or the need to further their own career and to avoid the
penalties, legal and otherwise, which may befall them in the case of certain types of
incident.