in the name of god. how to deal with infected total knee arthroplasty mohsen mardani-kivi assistant...
TRANSCRIPT

In the name of God

How to deal with Infected Total Knee
Arthroplasty
Mohsen Mardani-KiviAssistant Professor, Orthopedic Department, Guilan University of Medical Sciences

Background
• Total joint replacement is one of the most commonly performed and successful operations in Orthopaedics as defined by clinical outcomes and implant survivorship*
*

Incidence
• Infection has occurred in 1% to 2% of primary TKA surgeries and has been the leading cause of failure following TKA.
• The rate of peri-prosthetic infection has been declining over the last two to three decades, mostly due to operating room environments and operative techniques

Risk Factors for Infected Arthroplasty
• Prior surgery• Surgery time > 2.5 hours• Compromised immune status• Poor nutrition• Diabetes mellitus• Obesity • Smoking

Risk Factors for Infected Arthroplasty
• Chronic renal insufficiency• Diabetes • Neoplasm requiring chemo• Tooth extraction• Skin ulcerations / necrosis• Rheumatoid Arthritis• Recurrent UTI• Oral corticosteroids

Surgical Techniques
HemostasisProlonged operating time

Surgical Techniques
Avoid skin bridges Avoid creation of
skin flaps

Clinical Course
Pain #1SwellingFeverWound breakdown
drainage
Windsor et alWindsor et alJBJSJBJS; 1990; 1990

Work-Up
• Wound History• Physical Exam• Serial Radiographs• Lab/sed rate/CRP (returns
to normal level 3 wk post op.)
• Bone scan / Indium scan• Serum interlukine-6
(100%sensitivity & 95%specifity)

Arthrocentesis
• Gold standard for infection diagnosis:
WBC Cell count more than 2500 cells/mm3 & 60% PMN
Protein high Glucose low
Arthrocentesis
•direct smear•gram strain•Aerobic•Anaerobic•acid fast•fungi

Microbacterial
• Majority of infections : Staphylococci
• Acute hematogenous infections:– Staphylococcus aureus – Beta-hemolytic streptococci – Enterococcus species
• Gram-negative bacilli and anaerobes are also seen in chronic infections but uncommon...

Staphylococcus aureus
Common cause of musculoskeletal infections:
• Early postoperative infection
• Late chronic infection
• Acute hematogenous infection at the site of a prosthetic joint

Staphylococcus aureus
Susceptibility to methicillin treated most effectively with
• Antistaphylococcal penicillin (e.g., nafcillinor oxacillin)
• First-generation cephalosporin.

MRSA: Methicillin-resistant Staphylococcus aureus
• first described in 1961
• Extra penicillin-binding protein (PBP2a) which results in a low affinity for beta-lactam antibiotics such as the penicillins and cephalosporins

MRSA
• poor clinical outcome because of the limited effectiveness of antibiotics.
• Increase cost for treatment.

MRSA
• Increasing trend in MRSA infection
• Staphylococcus aureus (MRSA) from the nosocomial setting and its emergence as a cause of community-acquired infection.

Staphylococcus 64
S. aureus, penicillin sensitive 14 S. aureus, penicillin resistant 28 S. epidermis 22
Gram negative 12 Pseudomonas 7 Escherichia coli 5
Anærobic 6
Other 17
OrganismOrganism PercentPercent
Infection TKR

Treatment of prosthetic infection
• Long-term antibiotic suppression• Surgical débridement with retention of the
prosthesis • Resection arthroplasty• Arthrodesis• One-stage re-implantation procedure• Two-stage re-implantation procedures• Amputation
Treatment of prosthetic infection
• Two-stage reconstruction is the standard practice for treating patients with infected total joint arthroplasty.
• The success rate of two-stage reimplantation has ranged from 80-100%

Treatment Options
– Long-term antibiotic suppression– Surgical débridement with retention of the
prosthesis – Resection arthroplasty– Arthrodesis– One-stage re-implantation procedure– Two-stage re-implantation procedures– Amputation

Antibiotic suppression
Indicated in:– med compromised patients that prosthesis
removal is not feasible– The prosthesis is not loose– Low virulence micro-organism
Duration: life long

Treatment Options
– Long-term antibiotic suppression– Surgical débridement with retention of the
prosthesis – Resection arthroplasty– Arthrodesis– One-stage re-implantation procedure– Two-stage re-implantation procedures– Amputation

Surgical Debridement
• Debridement with antibiotic suppression therapy
– Limited success and Arthroscopic irrigation is not effective
– < 3 weeks

Surgical Debridement
• Debridement with antibiotic suppression therapy
– Strep/staphepi -- best– Avoid repeated attempts– Frozen tissue section– Suction drains– 6 week antibiotic-therapy– Polyethylene exchange


Treatment Options
– Long-term antibiotic suppression– Surgical débridement with retention of the
prosthesis – Resection arthroplasty– Arthrodesis– One-stage re-implantation procedure– Two-stage re-implantation procedures– Amputation

Two-stage Re-implantation
Most successful treatment
•Procedure of choiceProcedure of choice

Two-Stage Re-implantation

Two-Stage Reimplantation
Stage I
remove prosthesis / cement
thorough debridement


Two-Stage Reimplantation
Stage I create antibiotic spacer impregnated with antibioticswound closure








Two-Stage Re-implantation
• Spacer Antibiotic Regimen
• Tobramycin 2.4 gm/3.6 gm per 40 gms of PMMA
• Vancomycin > 0.5 gm to 1 gm per 40 gms of PMMA


Antibiotic Impregnated Spacer
Cidal levels of antibiotic
Spacer to preserve tissue tension
Facilitates re-implant and wound exposure

Local Delivery of Antibiotics
• Antibiotic cemen bead/spacer
• local levels of antibiotics that far exceed those attained with systemic antibiotic therapy.

Local Delivery of Antibiotics
• Antibiotic bead - difficulty in removing after implan
tation.
• Antibiotic impregnated spacers
- minimizes limb-shortening
- limits scar formation
- facilitates reimplantation
Antibiotic for cement spacer
• Microbial Sensitivity
• Bactericidal
• Heat stable
• Powder form

Antibiotic for cement spacer
• Gentamycin
• Tobramycin
• Vancomycin
• Fosfomycin

MRSA
• VancomycinVancomycin is first choice in MRSA
• Vancomycin bead/cement space
• Intravenous vancomycin

Block spacers
1. Simple tibio-femoral block
2. Molded arthrodesis block
3. Articulating mobile spacers (especially in bilateral infected TKAs)

Block spacers
• Simple tibio-femoral block

Block spacers
• Molded arthrodesis block

Block spacers
• Articulating mobile spacers (especially in bilateral infected TKAs)
• Multiple Techniques

Mobile spacer technique

Prosthesis removal

Removal of debris and cement
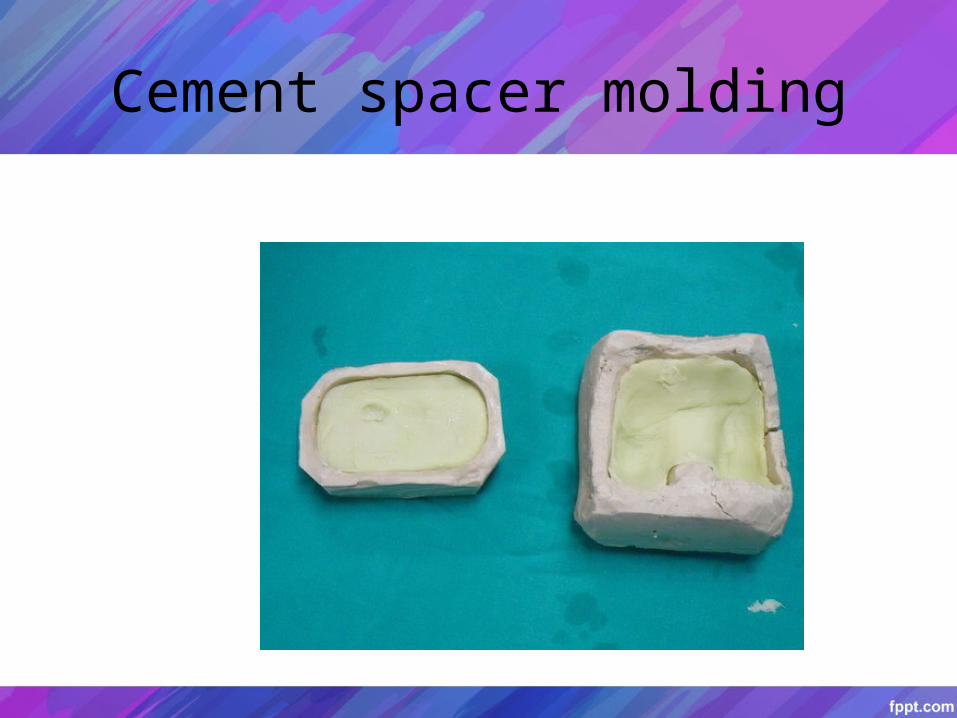
Cement spacer molding

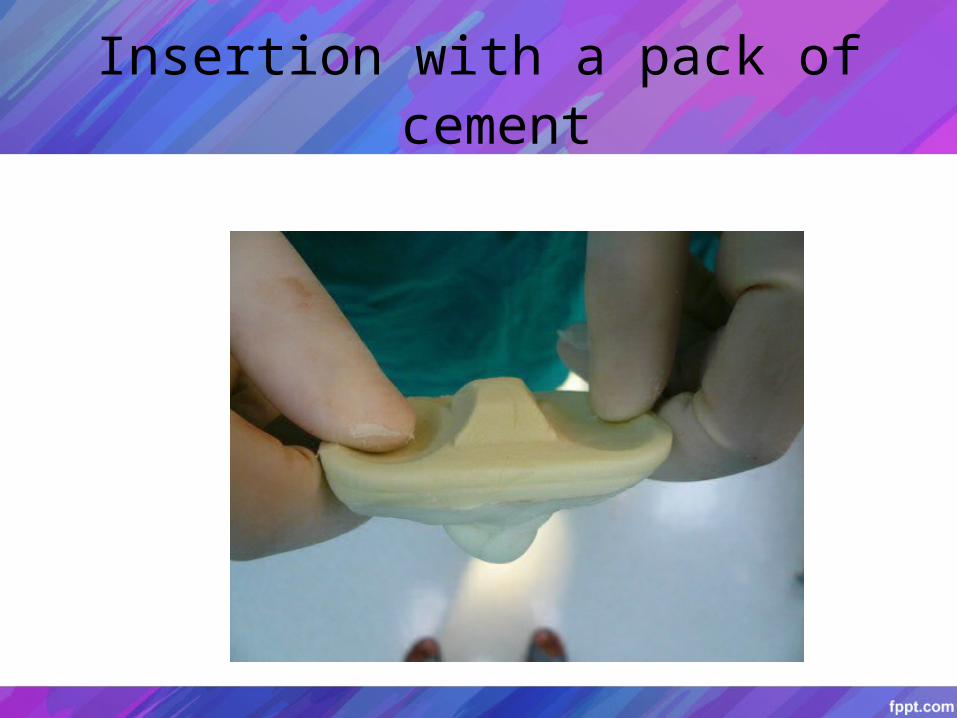
Insertion with a pack of cement

Final implantation

Postoperative x- ray

PROSTALAC COMPONENTs

PROSTALAC COMPONENTs

• Haffmann’s Procedure:– Using of the patients own prosthesis

Stage II – Antibiotic Treatment Hickman catheter
MIC 1:8 / 6 wks
Patient should use knee brace
In mobile articulating spacers patient is allowed up to 50% PWB and is encouraged ROM
Infections About TKRInfections About TKR

Stage III – Reimplantation
Serial aspirations Pre-op planning Bone scan / Sed rate

• Intra-operative Frozen Section
< 5 PMN’s per HPF – no infection
> 10 PMN’s per HPF – infection

Treatment Options
– Long-term antibiotic suppression– Surgical débridement with retention of the
prosthesis – Resection arthroplasty– Arthrodesis– One-stage re-implantation procedure– Two-stage re-implantation procedures– Amputation

Resection Arthroplasty
Removal all components
Remove all cement
Effective in medically compromised patient

Treatment Options
– Long-term antibiotic suppression– Surgical débridement with retention of the
prosthesis – Resection arthroplasty– Arthrodesis– One-stage re-implantation procedure– Two-stage re-implantation procedures– Amputation

Arthrodesis Indications
Extensor mechanism disruption Resistant bacteria Inadequate bonestock Inadequate soft tissues Young patient

Advantages
DefinitiveDefinitive treatment
Little chance of recurrence

Disadvantages
Difficulty with transfers / small spaces
Increase energy requirements

Algorithm
• TKA
• Clinical Sepsis
(GRAM + (GRAM + Organism) Organism)
< 3 wks< 3 wks > 3 wks> 3 wks
DebridementDebridementAntibiotics (6 wks)Antibiotics (6 wks)
2-Stage2-StageReplantReplant
Infections About TKRInfections About TKR

Algorithm
•DebridementAntibiotics
SuccessSuccess
2-stage 2-stage ReplantReplant
ArthrodesisArthrodesis
Infections About TKRInfections About TKR
No No SuccessSuccess
2-stage Replant2-stage Replant
SuccessSuccessNo No
SuccessSuccess
ResectionResectionArthroplastyArthroplasty

Result of treatment in MRSA infection
• Yogesh Mittal retrospective cohort study
• 37 TKA patients with MRSA or MRSE infection
• Two stage revision: success rate 76% at median duration of follow-up was 51 months (range, twentyfour to 111 months).
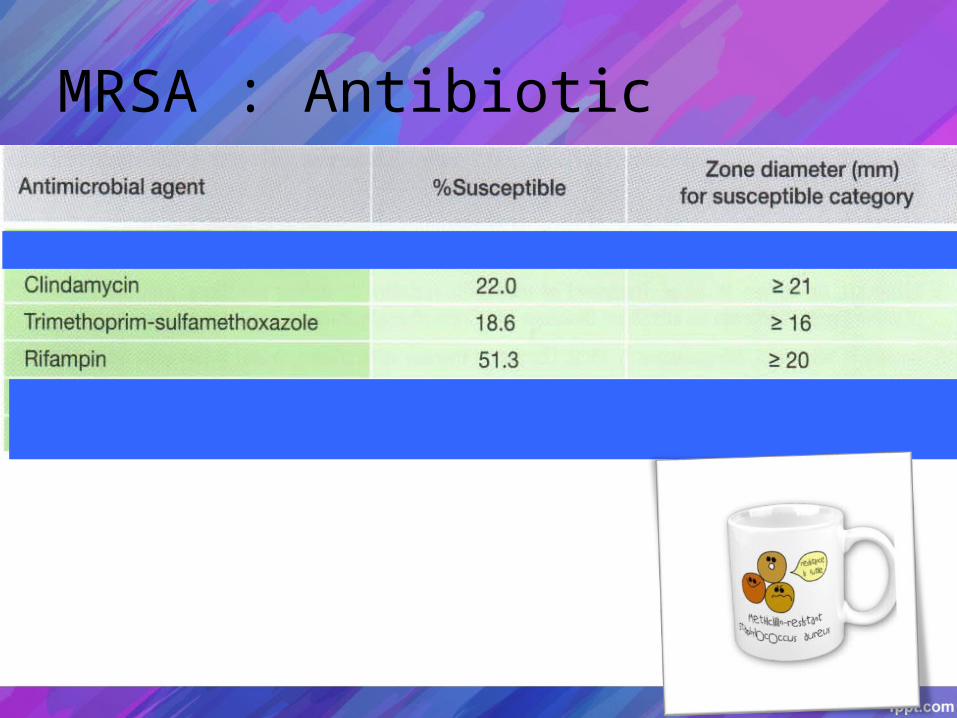
MRSA : Antibiotic
Alternate antibiotic
• Allergy to Vancomycin
• Pathogen resistance to Vancomycin
increase reports of decreasing susceptibility of S. aureus to vancomycin
Juan J . Picazo.Activity of daptomycin against staphylococci collected from bloodstream infections in Spanish medical centers.Diagnostic Microbiology and Infectious Disease.2009;64 ,448–451

MRSA sensitivity
Possible alternatives
• Teicoplanin
• Daptomycin
• Leinazolid
• Fosfomycin
Picazo JJ, Betriu C.Activity of daptomycin against staphylococci collected from bloodstream infections in Spanish medical centers.Diagn Microbiol Infect Dis . 2009 ;64(4):448-51.
Schintler MV,High fosfomycin concentrations in bone and peripheral soft tissue in diabetic patients presenting with bacterial foot infection . J Antimicrob Chemother . 2009 Jul 3.

Antibiotic cement in MRSA
Boonsin Buranapanithit : in vitro study
• Gentamycin , Cefalexin bead cannot inhibit MRSA
• Vancomycin , Fosfomycin bead effectively inhibit growth of MRSA
Boonsin Buranapanitkit.In vitro Elution Characteristics of Antibiotic Cement on MRSA organism.The journal of the asean orthopaedic association.2000, 13.33-36

Fosfomycin
• A synthetic broad spectrum antibiotic
• Bactericidal antibiotic
• Heat stable
• High concentration in bone
Boselli E, Allaouchiche B.Diffusion in bone tissue of antibiotics. Presse Med 1999; 28(40): 2265-76
Conclusions
• Prevension
• Adequate surgical debridement
• Staged revision
• Adequate &Susceptibility antibiotic

