in the name of god. frontal sinus fractures cummings otolaryngology 2015 chapter 23 –...
TRANSCRIPT

IN THE NAME OF GOD

Frontal Sinus Fractures
Cummings Otolaryngology 2015
CHAPTER 23 – Maxillofacial Trauma
Dr .Akhtar Kavan

Introduction
• The term maxillofacial trauma is generally used to refer to the injuries of the facial skeleton
• Craniomaxillofacial trauma might be a better term because the anterior wall and floor of the anterior cranial fossa are included in these injuries
• management of these injuries is sometimes thought of as “facial orthopedics.”

Embryology
• Absent at birth
• Doesn’t begin development until about 2 years
• Radiographically evident at about 8 years
• Adults size at about 12 years ; but pneumatization continues slowly until 40 years
• Consists of one or more compartments
• Irregular shapes & asymmetric

Embryology
• Lined by respiratory epithelium
• Intimate relation with cranial fossa
• Volume approx 5 - 15 mls
• Ant. wall thickers / stronger than post. wall
• Dura adheres to deep surface of post. table
• Mucosal lining continous with ethmoidal air cells & Nasofrontal ducts
Embryology
• Foramina of Breschet = venous drainage of mucosa are site of potential intracranial spread of infection
• Mucosa deeply invaginates foramina

Anatomical Variation
• 10 % unilateral
• 5 % rudimentary
• 4 % absent
• 20 % of people “abnormal frontal sinus anatomy
Nasofrontal Duct
• Drains frontal sinus
• Located posteromedial floor of sinus
• Very variable course
• True duct is absent in 85% people
• - FS drains indirectly via ethmoidal air cells to middle meatus

Anatomy
• The face can be divided into 3 sections
• the frontal bones are generally considered the upper third of the face
• The maxillae, zygomas, and orbits comprise the middle third, or midface, which may include the nose
• The mandible is considered the lower third

Physiology
• Upper Third
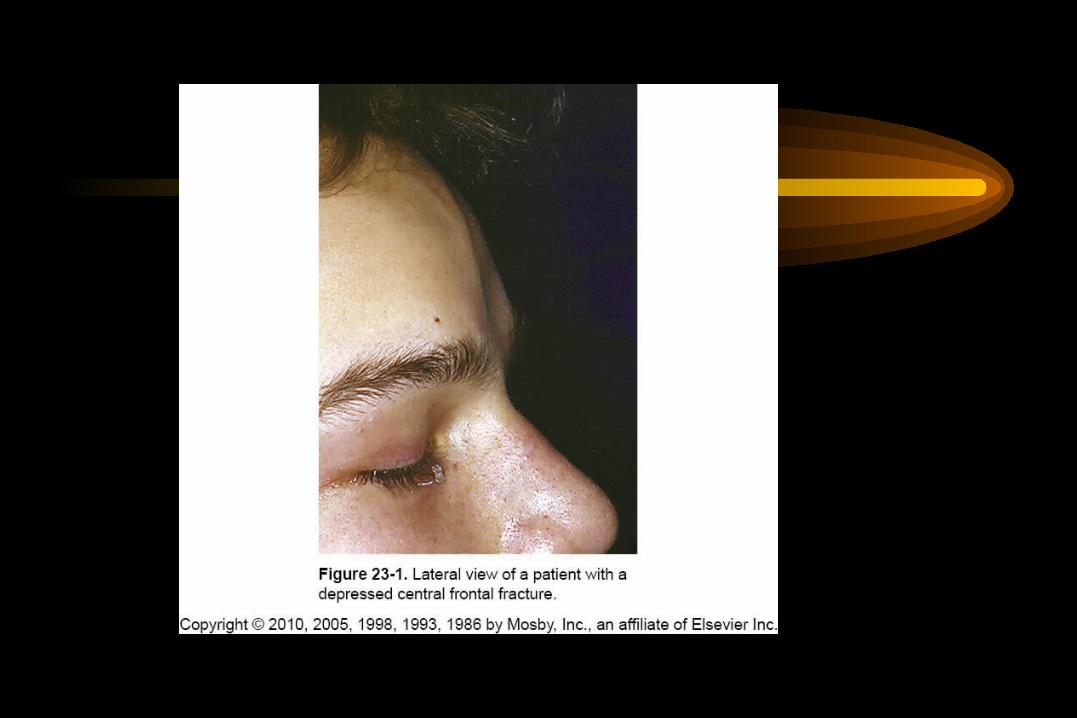
• Displaced fractures of Frontal bone can create various deformities, the most common of which is a central forehead depression (Fig. 1).

Pathophysiology
• Frontal bone fractures may involve only the anterior sinus walls, in which case the fractures are significant only for sinus function and cosmesis
• or they may involve the posterior wall of the sinus or extend beyond the sinus, in which case they are true skull fractures and become neurosurgical concerns as well

Pathophysiology
• The supraorbital rims and roofs are also part of the frontal bones, which are therefore also related to the orbits, and fractures can thus affect orbital and ocular functions.
• This thick glabellar bone protects the underlying frontal outflow tracts and the cribriform plates, which house the branches of the olfactory nerves
Pathophysiology
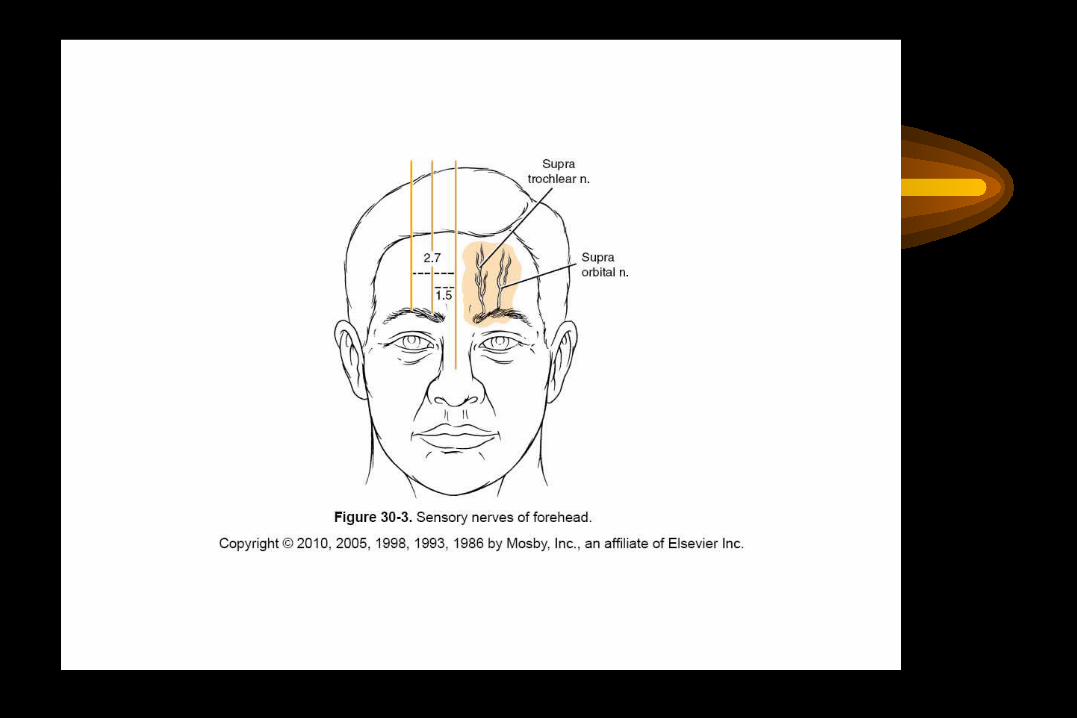
• The supraorbital and supratrochlear nerves pass through notches or foramina in the supraorbital rims and can be injured from trauma or, more commonly, from surgical manipulation.

Evaluation and Diagnosis
• Physical Examination
• performing a good physical examination.
• the initial assessment must address the ABCs and any other potentially life-threatening injuries
Evaluation and Diagnosis
• In the upper third of the face, the forehead is evaluated for sensation and motor function.
• In some cases, fractures may be visible as depressions (see Fig.1) or palpable as step-offs, although typically these fractures are more readily seen on CT scans.

Radiographic Evaluation
• With some exceptions, the CT scan has replaced other forms of radiographic imaging for the assessment of craniomaxillofacial injuries.
• The exception here is for simple nasal fractures (simple meaning without evidence of involvement of other facial bones)
Radiographic Evaluation
• For frontal fractures, a high-resolution axial CT gives good information about the anterior and posterior walls
• When the posterior wall is displaced (regardless of the degree of displacement), and there is soft tissue density within the sinus, the inside of the sinus be visualized



Associated injuries
• Neurological
• Closed head injury
• Pneumocephalus
• Cerebral contusions
• Hematomas
• Open brain

Associated injuries
• Ophthalmological
• - Up to 25 %
• Full ophthalmological examination mandatory

Associated injuries
• Maxillofacial injuries
• - NOE
• - ZMC
• - Le Fort fractures
• - Panfacial fractures

Classification Schema
• Many classification system
• Can get very detailed classification ;
• However not useful clinically
• most useful classification, which predicts the likelihood of disruption of the frontal sinus drainage passages, was presented by Stanley and Becker.

Classification Schema
• They separated frontal sinus fractures into linear horizontal and linear vertical and comminuted anterior and posterior walls, with and without NEC or supraorbital rim fractures


Clincal Classification
• Anterior Table
• - Displassed
• - un -displaced
• Posterior Table
• - Displaced
• - Un- displaced

• Anterior & Posterior Table
• - Displaced
• - Un - displaced
• Nasofrontal duct
• - Involved
• - Un involved
Clincal Classification

Simplified Clinical Classification
• 1- Fracture of anterior table
• 2- Fracture with disruption of posterior wall
• 3- Fracture involving floor of sinus
Management
• General
• Antibiotic treatment should be initiated at the time the patient initially presents
• Typically, antibiotics that cover oral organisms such as penicillins, cephalosporins, or clindamycin are selected

Management
• Many surgeons have suggested that surgery should be delayed until swelling resolves
• Certainly, logic seems to suggest that early intervention to restore the hard and soft tissues to their normal anatomic positions would be beneficial
Surgical Access
• There is also an additional challenge in craniomaxillofacial surgery, which is the inability to make incisions directly over most fractures,
• because unacceptable scars and facial nerve injuries would result

Surgical Access
• Coronal flap preferable
• Generally avoid using laceration or local incisions
• Avoid “ Gull Wing “ & “ Open Sky “ approaches
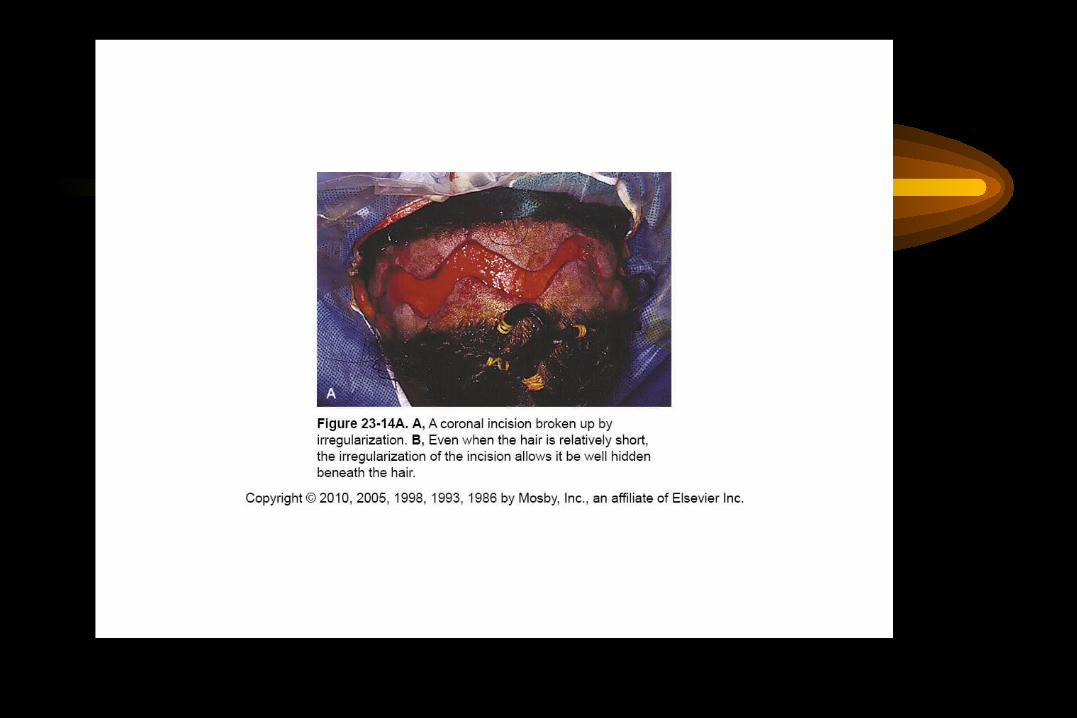
• In the patient with hair, irregularizing the incision with a running W or a wavy line



Surgical Access
• Shaving the hair is not required
• When full exposure of the zygomas is required, the incision begins in the preauricular crease
• When zygomatic exposure is not needed, the incision starts above the auricle
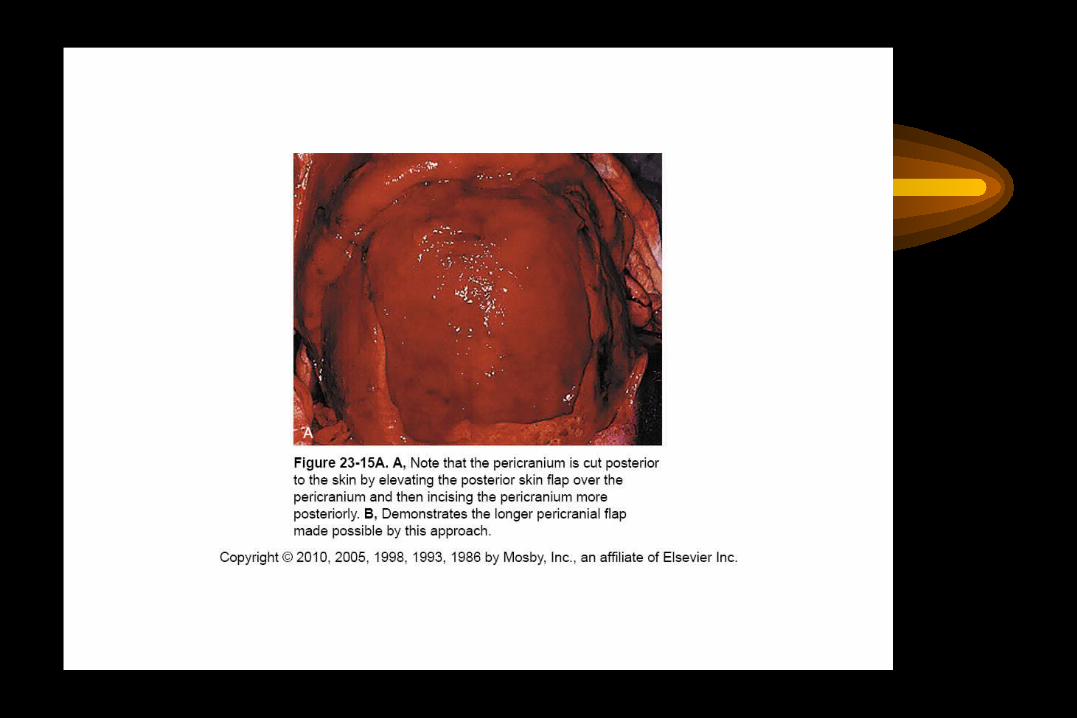
• When a long pericranial flap is needed , the incision should not violate the pericranium



Surgical Access
• As the flap is elevated anteriorly, care must be used to avoid injury to the temporal (frontalis) branches of the facial nerve
• The supraorbital and supratrochlear nerves are encountered as the flap is elevated to the supraorbital rims.
Biomechanics of the Facial Skeleton
• In the upper third, the anterior wall of the frontal sinus is thin and there are no significant forces acting on this area.
• The supraorbital rims and the frontal bones lateral and superior to the frontal sinuses are thicker , It requires more force to fracture these bones
Surgical Management
• Cranialization
• Vs
• Oblitration
Oblitration
• Frontonasal ducts oblitrated ,
• Mucosal lining removed And sinus “ packed “
• Various materials advocated :
• -Fat
• -Muscle
• -Bone
• -Hydroxyapatite

Fracture Repair
• Most repairs are performed using titanium plates and screws
• a variety of absorbable plates and screws are used as well
• there is no contraindication to the use of stainless steel wires when needed

Fracture Repair
• A number of algorithms have been published
• The key issues in frontal sinus trauma relate to two fundamental questions:
• (1) Is exploration necessary?
• (2) Is obliteration necessary?

Fracture Repair
• Keep in mind the purposes of the bone being repaired
• The sinus outflow tracts must function to drain the sinuses
• Thus pure anterior wall fractures that do not extend into the nasofrontal ducts are repaired for cosmetic purposes only.

Fracture Repair
• These should be explored if they are significantly depressed, because even in the absence of acute deformity, they are likely to lead to deformities when the swelling resolves.
• The smallest plates available are generally used, because there are little or no force
• Use of the endoscope may allow repair of selected anterior wall fractures with minimal incisions
Fracture Repair
• When the ducts are involved but the posterior wall is intact, judgment allows more than one option
• 1- Frontal sinus obliteration is always acceptable
• 2-Allow the sinus to function to see what happens

Fracture Repair
• A nondisplaced posterior wall fracture can be observed
• if the posterior wall is displaced, it is difficult to determine the status of the dura and underlying brain
• In the absence of apparent ductal injury, it is still wise to consider trephination and transcutaneous endoscopy

Fracture Repair
• In the absence of posterior wall displacement and with no soft tissue abnormalities associated with such a nondisplaced fracture, it is unclear that obliteration is mandatory
• Careful follow-up including interval CT scans will demonstrate whether or not aeration of the sinus ensues

Fracture Repair
• Numerous complications have been encountered using hydroxyapatite cements
• but in one series using it in combination with live pericranial flaps, no complications were seen
• they can be used to repair the frontal contour in the presence of severe comminution and/or bone loss of the anterior wall


Cranialization
• Frontal craniotomy
• Dural repair
• Removal of posterior wall
• Removal of mucosal lining
• Plugging of nasofrontal ducts
• Galeal flap placed

CSF Rhinorrhea
• CSF rhinorrhea is not rare and may occur via the frontal sinuses, or through the cribriform plate, ethmoid sinuses, and/or sphenoid sinuses
• Large defects should be repaired at the time of facial fracture repair.
• Small defects should be identified endoscopically and can usually be repaired using this approach

Skull Base Disruption
• Prophylactic Antibiotics
• Incidence of meningitis between 3-50%
• Mortality about 10%
• Usually pneumococcus spp.
• Prophylactic Antibiotics not recommended

CSF leak
• Fracture reduction often stops leak
• Most traumatic leaks close spontaneously
• Leak more than 72 h.= lumbar drain
• Surgical repair
• -Endoscopic
• -Intracranial

Skull Base Disruption
• The use of the Transglabellar Subcranial Approach may allow for earlier intervention
• It also allows direct visualization of the cribriform area without disarticulating it completely
