in-patient dental anesthesia major oral and fasciomaxillary surgery classifications: major...
TRANSCRIPT
In-Patient Dental Anesthesia Major oral and fasciomaxillary surgery
Classifications:
Major Orthognathic Surgery (late teenage& adults)
Tumor surgery (elderly) Palate Surgery (infants&children)
In-Patient Dental Anesthesia
Problems:
Major problem: Airway Management Extensive, long operations Significant blood loss Poor nutritional status Micro-vascular surgery
In-Patient Dental Anesthesia Airway Management
IMPORTANT POINTS
NEVER PARALYSE UNTILL POSSIBLE VENTILATION HAS BEEN ESTABLISHED
RECENT SUCCESSFUL INTUBATION DOESNOT MEAN FUTURE POSSIBLE INTUBATION
FULL RANGE EF DIFICULT INTUBATION EQUIPMENT MUST BE AVAILABLE
In-Patient Dental Anesthesia Airway Management
Choice of the technique depends on several factors:
Patient safety Experience of the anesthetist Known difficult airway Requirements: nasal or oral Post operative jaw wiring
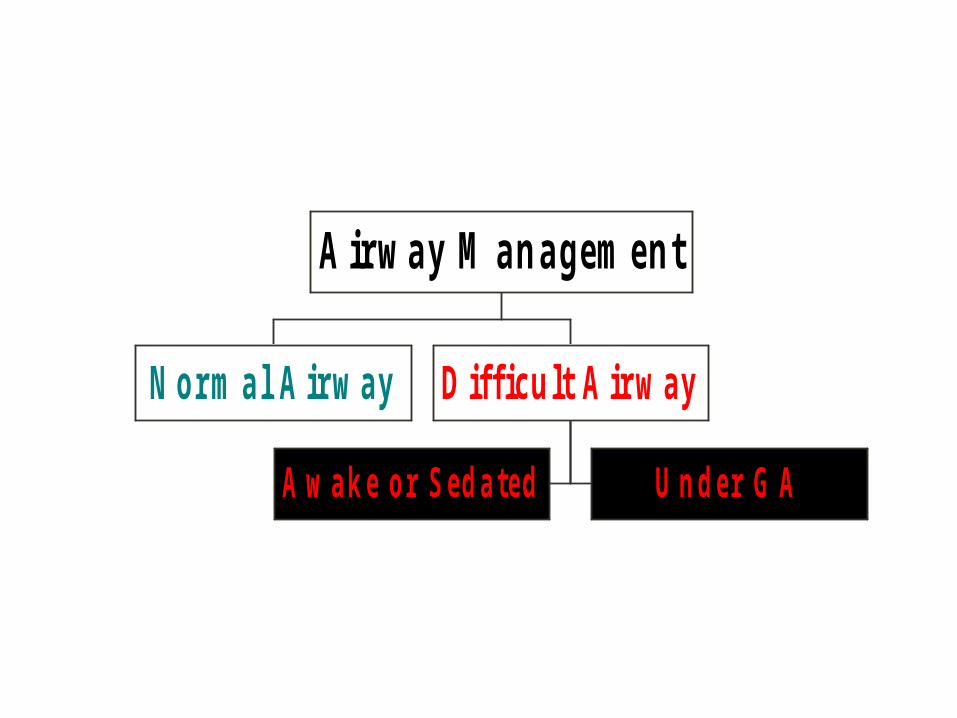
N orm al A irw ay
A w a k e o r S e d a te d U n d e r G A
D iff icu lt A irw ay
A ir w a y M a n a g em e n t
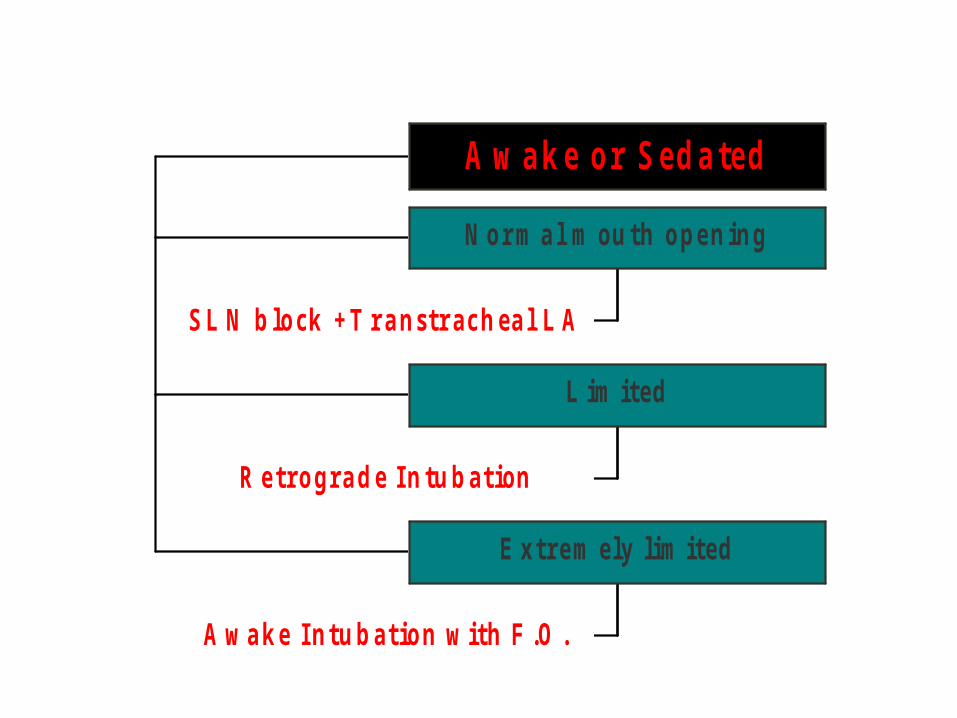
A w a k e o r S e d a te d
S L N b lo ck +T r a nstr ac h ea l L A
N o r m a l m ou th o pe n ing
R e tro g ra d e In tu b at ion
L im ited
A w a ke In tu b at io n w ith F .O .
E x tre m ely lim ited
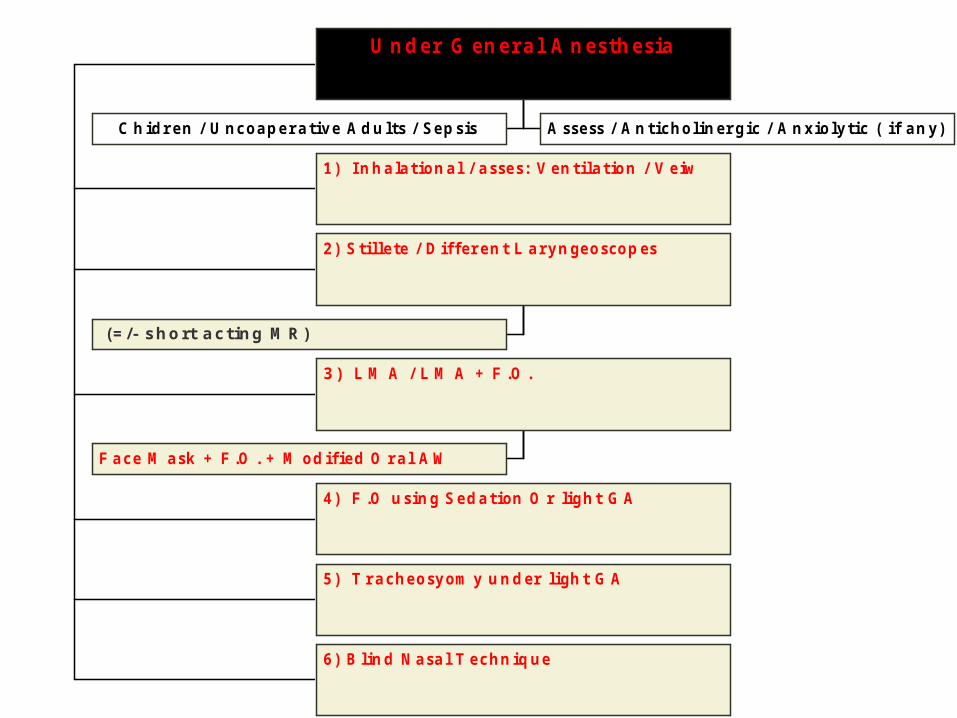
C h idr e n / U nc o a pe r a tiv e A d u lts / Se p s is A sse ss / A n t ic ho lin er g ic / A n xio ly tic ( if a n y)
U n d e r G e n e r a l A n e sth e s ia
1 ) In h a la t io n a l / a sse s : V e n t ila t io n / V e iw
(= /- short acting M R)
2 ) S tille te / D if f er e n t L a ry n ge o sco p es
F a c e M a sk + F .O . + M o d if ie d O r a l A W
3) L M A / L M A + F .O .
4 ) F .O u s in g S e d a t ion O r lig h t G A
5 ) T r a c he o sy om y u n d er ligh t G A
6 ) B lin d N a sa l T e c hn iq ue

Emergency Maxillofacial Surgery
Maxillofacial Trauma
Types of Injury
Fasciomaxillary Injury
Accompanied injury
Neck Injury Cervical Spine Injury Head Injury Closed Head Injury & Cervical Spine Injury
Fasciomaxillary Injury
One third of causalities Maxilla is the most common(24%) Followed by the mandible (18%) Most maxillary fractures are compound comminuted
Types Le Forte I: Transverse Fracture
Le Forte II Pyramidal Fracture
Le Forte III: Craniofacial Fracture
Neck Injury
10% are accompanied by carotid artery injuries
Presented with either severe hematoma or expanding neck hematoma
SymptomsDysphagiaConstant coughHemoptysisInspiratory stridorHoarseness of voiceSubcutaneous Emphysema
TypesOpen TraumaClosed Trauma
Cervical Spine, Spinal Cord Injury
Should always be considered
Involvement of C7
(or oedema of near by cervical spines)
Significant Hemodynamic Instability
Significant Respiratory Distress
Head Injury
17.5% with facial fractures (10% severe)
Early recognition
Loss of consciousness
Glascow Coma Scale
Secondary brain insult
Pre- Anesthetic AssessmentProblems
Airway Obstruction (early tracheostomy is not universal)
Difficult Intubations
Unstable Cervical Spine
AcuteAirway Problems:Aspired teethOral bleedingTrismusEpistaxisNasal CSF
leakage
Pre- Anesthetic AssessmentProblems
Blood loss in excess of patient blood volume
Full Stomach ( blood, debris, delayed emptying)
Large Air leaks, Risk of subcutaneous emphysema, pneumothorax
Pre- Anesthetic AssessmentProblems
CSF leaks with constant risk of meningitis
Increased ICP with secondary brain insult
Presence of co-existing disease (ASA)
Existing drug or alcohol intoxication

Anesthetic management
I) Specific Management
Facial Trauma Facial Trauma with Closed Head Injury Facial Trauma with Spinal Cord Injury Facial Trauma and Neck Injury
II) General
III) Airway
Anesthetic managementSpecific Management: Facial
Trauma
All facial traumas must be Suspected for IC and Spinal injuries
Airway
Hold tongue, head down, turned one side Nasopharyngeal airway (I&CI) Throat pack Scissors or wire cutter
Anesthetic managementSpecific Management:
Facial Trauma with closed head injury
Reduction of ICP is the Main Goal
Not a situation for blind nasal Head elevation 20o –30o
Control body temperature Prophylactic phenytoin Avoid hypervolemia and hypotonic fluids Avoid hypoglycemia and hyperglycemia
Anesthetic managementSpecific Management:
Facial Trauma with spinal cord injury
Not a situation for blind nasal ET intubation (technique) Respiratory dysfunction (up to 3 weeks) Spinal shock
Anesthetic managementSpecific Management:
Facial Trauma with neck Injury Airway Secure then control hemorrhageAirway
ETT through the wound Awake orotracheal intubation Avoid MR in uncertain airway
Respiration ( Risk of pneumothorax)
Avoid IPPV Avoid nitrous oxide Avoid sedation
Hypovolemia
Anesthetic managementGeneral Management
IV lines, Urinary catheters, stomach tubes Monitors Measure to reduce ICP Fluid therapy and replacement therapy FIO2 should be at maximum
Premedication Anticholinergics Avoid premedication Heavy premedication
Anesthetic managementGeneral Management
Important Points
Airway must be a priority (secondary brain insult)
Excitement is a sign of hypoxia rather than pain
Accidental extubation is a well recognized hazards
Anesthetic managementGeneral Management
Important Points
Decreasing level of consciousness is a reliable sign of head injury
Major surgery may be delayed until the patient’s neurological conditions has established
Important to differentiate between blood and CSF
Consider all patient full stomach
Anesthetic managementAirway
CHRACTERISTICS
TECHNIQUE (algorism)
Awake vs. anesthetized Nasotracheal vs. Orotracheal Blind vs. Visual Direct vs. Fiberoptic Antegrade vs. Retrograde Tracheostomy, Cricothyrotomy
Transtracheal Jet Ventilation
Anesthetic managementAirway :
CHRACTERISTICS
Dynamic not static All hypoxic All full stomach Unique optimum position for the airway
(semi prone, sitting up, leaning forward)
Anesthetic managementAirway :
Technique
Is there a possibility of concurrent basal skull fracture?
Nasotracheal intubation is absolute contraindication
Anesthetic managementAirway :
Technique
Is there a possibility of injury of cervical spine?
Manual in line axial traction Bullard laryngoscope(It matches anatomy not to align the airway to match the blade)
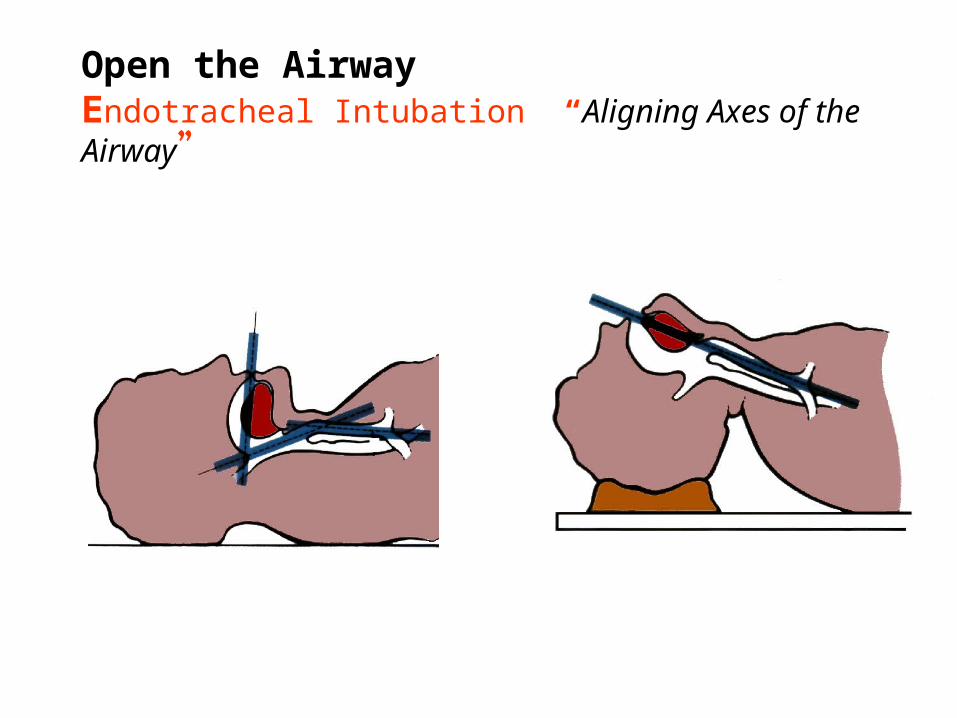
Open the AirwayEndotracheal Intubation “Aligning Axes of the Airway”
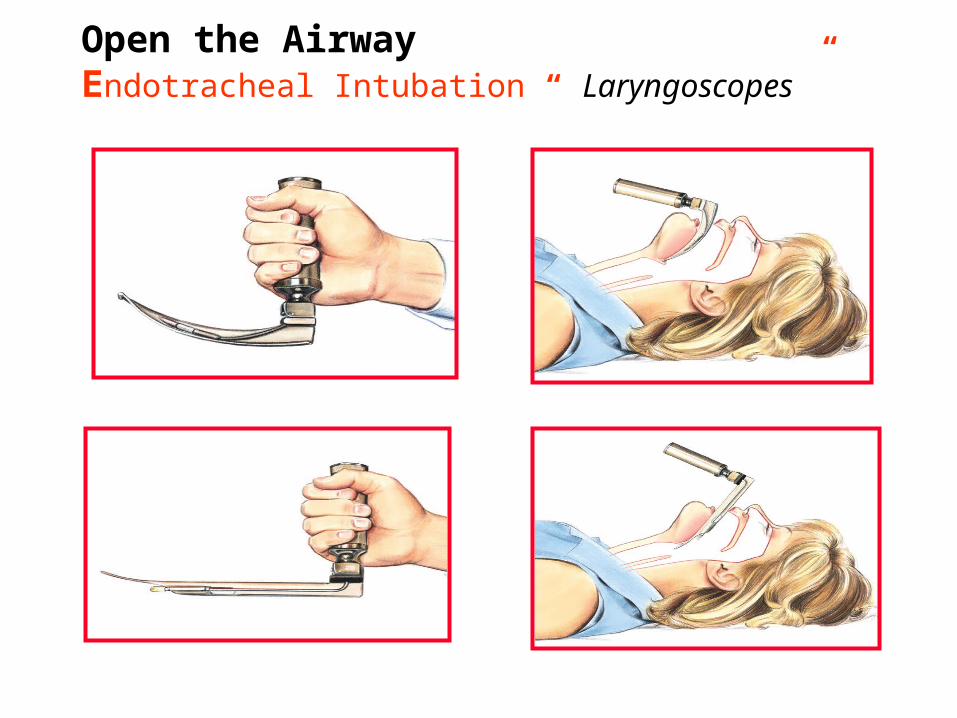
Open the AirwayEndotracheal Intubation “ Laryngoscopes ”
Anesthetic managementAirway :
TechniqueIs the patient is unable to open his mouth?Why?
Reflex spasm (I.e.Trismus) (Anesthesia may relief the spasm)
Mechanical dysfunction (i.e.TMJ) (Blind nasal intubation or Fiberoptic intubation)
Bimandibular fracture at the level of second or first molar

THANK YOU