in compliance with accme standards for commercial support ... · complexity of differentiating...
TRANSCRIPT

In Compliance with ACCME Standards for Commercial Support of CME activities…
John K. Maesaka, MD1.
Advisory board—Pfizer, Inc., Otsuka
Pharmaceutical US
2.
Research grant-
Otsuka
Pharmaceutical US

Complexity of differentiating cerebral-renal salt wasting (RSW) from SIADH, emerging importance of determining fractional urate excretion
John K. Maesaka, MD

Hyponatremia is in a state of flux
Confusion in the literatureInability to differentiate RSW from SIADHPresent approach does not seem to be workingPropose a new approach to hyponatremia

Traditional Approach to Hyponatremia
1. Euvolemia2. Hypovolemia3. Hypervolemia (edema)
RSW
Rare - internists and nephrologists. It’s all SIADH!
Textbooks nephrology/medicineReview Articles

RSW
Common by:neurosurgeons critical careneurologists

Why Such a Diagnostic Discrepancy?
Largely an inability to assess volume. Are they euvolemic or hypovolemic?

Therapeutic Dilemma
SIADH-actually hypervolemic, water-loaded
-Water restrictSalt Wasting-hypovolemic
-Salt and water supplementation

Diagnostic Dilemma SIADH vs RSW
Both characterized by:Association with intracranial diseasesHyponatremiaConcentrated urineUrinary [Na] usually> 20 mEq/LNormal renal/adrenal/thyroid functionNonedematousHypouricemia, Increased FEurateOnly difference is volume status
So, let us review pertinent volume studies

Volume Studies-Neurosurgical Patients gold standard radioisotope dilution methods
BV BV UNaRSW SIADH mEq/L
Nelson-HN 10 (83%) 2 41-203Wijdicks-SAH
HN 8 (89%) 1 -NN 8 (67%) 4
SivakumarHN 17/18 (94%) 43-210
RSW much more common than SIADH in neurosurgical patients.

Chronic Hyponatremia Associated with Falls
122 chronic hyponatremics115-132 mEq/L
Falls in 21.3% hyponatremics vs 5.3% controls. i.e. 4X increase in falls
SAME FREQUENCY OF FALLS REGARDLESS OF LEVEL OF HYPONATREMIA- 115-132 mEq/L
Renneboog et al. Am J Med. 2006; 119: 711-718.
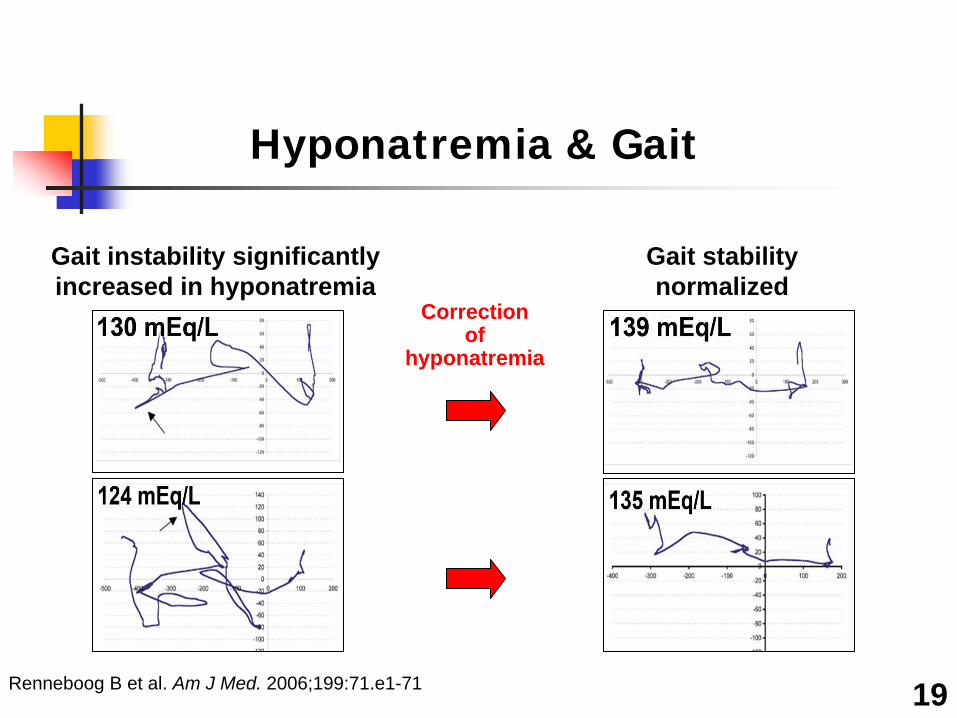
Renneboog B et al. Am J Med. 2006;199:71.e1-71 19
Hyponatremia & Gait
Gait instability significantly increased in hyponatremia
Gait stability normalized
Correction of
hyponatremia

Hyponatremia, Fractures & Falls
Falls and fractureshyponatremics -13.6% controls -3.9%
4.16 adjusted OR for fracture after fall
Gankam Kengne FG et al. Q J Med. 2008;101:583-588. Sandhu HS et al. Int Urol Nephrol. 2009;41:733-737.
21

Symptomatic Hyponatremia
Increasing awareness that even mild hyponatremia induces symptomsEditorial Does ‘asymptomatic hyponatremia’ exist?(Schrier R. Nature Rev. 2010)
Movement to treat all hyponatremics, creating an urgency to resolve the diagnostic dilemma

SIADH-Uric Acid and Hyponatremia
Beck, LH. NEJM 301:528-530, 1979
14-
12-
Serum 10-
Urate 8-
mg/dl 6-4-
2-
SIADH Other Hyponatremia
Beck, L.H. NEJM 301:528-530;1979
Beck’s Proposal
Coexistence of hyponatremia and hypouricemia (<4mg/dL) differentiates SIADH from most other causes of hyponatremia
Beck, LH. NEJM 301:528-530, 1979

SIADH FEurate before and after correction of hyponatremia
Patient FEurateN=5-10%
%1. Before 14.1
After 8.52. Before 24.2
After 9.93. Before 38.0
After 6.3
Beck, LH. NEJM 301:528-530, 1979

SUA, FEUA and SNa Before and After Correction of hyponatremia 4 papers published on this subject
SIADH
FEurateSNaSUA
Before AfterCorrection-hyponatremia

Insight Case-RSW
40 y.o.m, Adenocarcinoma-LungPE- postural hypotension
responsive to saline-No edema Serum: Na 116, Cr 0.6, urate 2.6 Urine: Osm 323, Na 41, FEurate 26.5%

Insight Case-RSW
Must be SIADH-no cerebral disease (-) CT scan of brain. He had hyponatremia and hypouricemia (Beck-SIADH)
Convinced he had RSW-postural hypotension-responsive to saline.

Proposal: Increased FEurate will persist after correction of hyponatremia by water restriction
SIADH vs RSW
FEurateSNa
Before AfterCorrection-hyponatremia

Insight Case-RSW
Fluid restriction-More wt loss, lethargic, weak, somnolent, postural dizziness, unsteady gait, slurred speech, postural hypotension.
Serum Na 138, uric acid 2.2, FEurate 14.7%, UNa 181
All signs and symptoms of volume depletion corrected with saline. T3, T4, Cortisol and ACTH stimulation test normal.

Serum Sodium, urate, FEurate, UNa Before and After Correction of Hyponatremia
Patient Serum Na Serum Urate FEurate Urine Na (mEq/L) (mg/dL) % mEq/L
1. Before 121 1.1 34.2 99After 138 1.5 30.0 156
2. Before 120 2.0 26.5 42After 138 2.2 14.7 181
3. Before 130 2.1 22.6 73After 139 2.5 22.6 130
4. Before 126 2.1 - 96After 135 2.8 16.1 37
5. Before 130 2.2 - -
After 139 2.1 29.8 114

Increased FEurate ± Hyponatremia
Described in:Neurosurgical diseases of multiple etiologiesAIDSAlzheimer’s diseaseDisseminated CryptoBronchogenic carcinoma metastatic to brain
Without cerebral diseaseMetastatic pancreatic carcinomaBronchogenic carcinomaHodgkins Disease

Differentiation of SIADH from RSW Works with hypertonic saline to correct hyponatremia
SIADH RSW
FEUA
SNa
Before After Before AfterCorrection of Hyponatremia

Insight Case
74 y.o.f. non-edematous, hip fracture. No Cerebral Disease
Na-129, Creatinine-0.8, uric acid-3.4 UNa 6 mEq/L, Uosm 362
FEurate 29.6%
Maesaka JK et al. (2007) Kidney Int,71,pp.822-826

Insight Case
7.1% decreased blood volume-radioisotope dilution-plasma and RBC volumes↑renin and ↑aldosteroneNormal adrenal and thyroid function
Maesaka JK et al. (2007) Kidney Int,71,pp.822-826

Saline infusion (125 ml/hr)
Maesaka JK et al. (2007) Kidney Int,71,pp.822-826

Plasma ADH levels in RSW
Time ADH-pg/ml
Baseline- 2.5
Dilute urine- Undetectable
Maesaka JK et al. (2007) Kidney Int,71,pp.822-826

Regulation of AVP Secretion
Increased plasma osmolality and decreased blood volume stimulate AVP secretion, but volume stimulus is more potent than osmolality.
AVP=arginine vasopressin.Stricker et al. In: Fundamental Neuroscience. 2nd ed. 2003;1011-1029.
-30 -20 -10 0 10 200
5
10
15
20
25
Plas
ma
Vaso
pres
sin
(pg/
Plas
ma
Vaso
pres
sin
(pg/
mL
mL ))
Percent ChangePercent Change
Plasma osmolality
Basal
Blood pressure/volume

Persistent increase in FEurate after correction hyponatremia-RSW
Maesaka JK et al. (2007) Kidney Int,71,pp.822-826

‘Is it cerebral or renal salt wasting’Change cerebral salt wasting to renal salt wasting
Mini-review-Kidney International-2009
Maesaka JK et al. Mini-review. Kidney Int. 2009 76:934-8

New Insight Case
83 Y.O. F-Colon Ca, HTNSerum Na-124, Cr-0.4, urate-2.8Uosm-336, UNa-43FEurate-9.6%, repeated x 3 <10%
Not consistent with SIADH or RSW!!Uosm 115 mosm/kg on random urine, reset osmostat!!Proved by water-loading test-Uosm 99 mosm/kg

Hyponatremia with Normal FEurate
Reset Osmostat (RO) (Imbriano et al J Nephrol 2012)
14 consecutive patients with hyponatremia and normal FEurate had RO (8 -Uosm < 200 mosm/kg-random urine, 6-normal water-loading test-ADH unmeasurable)8 hypouricemia, urate < 4 mg/dL, all had normal FEurate.FEurate is superior to serum urate!!

RO pathophysiologically different from SIADH
Normal FEuratePredictable, suppressible ADH

Types of the Syndrome of Inappropriate Antidiuresis (SIAD)
Ellison D, Berl T. N Engl J Med 2007;356:2064-2072

Study of Nonedematous Hyponatremia FEurate and Water Volume
About half of admissions to hospital have ROSIADH more common than RSW outside of neurosurgical unitMore RSW without cerebral diseaseAll patients with RO and SIADH have increased total (deuterium) and extracellular (sodium bromide) water volumes

Traditional Approach to Hyponatremia
1. Euvolemia2. Hypovolemia3. Hypervolemia (edema)

Assessing Volume Status in Hyponatremia
Extremely inaccurate SIADH and RO are not euvolemic. Hypervolemic!Some unwilling to treat SIADH and RO with V2 receptor blockers because they will become hypovolemic.Propose new algorithm that eliminates need to assess volume, UNa, renin, aldosterone or BNP
Renin, Aldosterone and BNP not useful—too many factors that affect them!

More FEurate in hyponatremias
Unequivocal cases of:Addison’s Disease—FEurate 2% and 3%
Myxedema—FEurate 29% and 30%

NF probably affects sodium transport in the proximal tubule
70% Na reabsorption
30% Na to distal tubule
0.4% Na in urine

Tubular handling of urate
90-95% urate reabsorption
5-10% presented to DT
No distal tubule urate transport
5-10% filtered urate excreted in urine
0.4% Na in urine

Urate/Lithium transported only in PT
Lithium transported 1:1 with Na in proximal tubule
30% Li/Na to distal tubule-No Li transport in distal tubule
5-10% of filtered urate excreted in urine

Serum urate and FEurateEffect of plasma on Na transport in rats
control, multi-infarct dementia and Alzheimer’s

Effect of plasma infusions on sodium excretion rates in rats
IC=intracranial diseases-Increased FEurate-normonatremiaTime 0 represents end of plasma infusion 4 h after firstexposure to plasma.

Studies in myxedematous rats
DiScalaHypertonic saline increased sodium excretion 3.4 fold
45% vs 12 %36% reduction in GFR17.1% reduction in ECV-inulin space
Papper—Micropuncture study30% and 32% reduction in GFR and renal plasma flow28% reduction in proximal tubule Na reabsorption4.3 and 2.3 fold increase in FE sodium and water excretion in urine.

Myxedematous patients are salt wasters!!
Volume depletion due to salt wastingRAT STUDIESDecreased ECVDecreased GFRMajor decrease in proximal tubule sodium reabsorptionHUMAN DATASupported by increased FEurate of 30% in hyponatremic-myxedematous patient.

Approach to Hyponatremia
Hyponatremia Normonatremia
FEurate < 11% FEurate > 11%Hypertonic saline
Psychogenic Polydipsia NormonatremiaReset OsmostatPrerenal azotemia
ECV depletion Addison’s Disease
Congestive heart failure Cirrhosis Nephrosis
FEurate < 11% FEurate > 11%
SIADH RSWHypothyroidism

New manuscript in press
“Failure of Volume Approach to Hyponatremia: A new Algorithm”

Current Status of RSW
It is not rareEstablished to be more common than SIADH in neurosurgical patients.Encountering more RSW patients without clinical cerebral disease.Investigate cause of RSW Demonstrated presence of circulating natriuretic factor (NF) in RSW



Protocol to study hypothyroidism Identify them-we will do the rest
IRB-approved protocol for studyStudy any hypothyroid patient before treatmentObtain informed consent to do study
Collect blood and urine Na, K, Osmolality, creatinine, urate, phosphorus
Perform total and extracellular water volume—deuterium and sodium bromideSave plasma 5 cc at -80°C

Question is whether we repeat studies after successfully treating these patients if they are salt wasters.

Developing a protocol to demonstrate NF in RSW
Preferable to expose luminal and basolateral surfaces of tubule cell because it may require a receptor for endocytosis. Decided to do clearance studies in ratsCan expose both sides of cell to NF

Demonstrating Natriuretic Factor in RSW
Because uric acid is transported only in the proximal tubule, we postulated that the NF was probably a protein that acted on proximal tubule

Lithium excretion rates in rats treated with plasma from Alzheimer’s disease and multi-infarct dementia and
mini mental state examination score

Other pertinent data in neurosurgical and Alzheimer diseases
GFRs and blood pressures were similar in all groups of rats
Age and gender-matched controlsMulti-infarct dementiaNeurosurgical patientsAlzheimer’s disease
Data inconsistent with effect of ANP/BNPNatriuretic factor is not ANP/BNP

Attempts to isolate NF
Extreme difficulty to identify NF by rat clearance studies.Needed an in-vitro bioassayPlasma given IP induced salt wasting in ratsMust be a small protein that can be filtered at glomerulus, saturate any receptors present and excreted in urine.

Ammonium Sulfate Precipitation of Urine Proteins
Neurosurgical patients with:increased FEurate and normonatremiaNormal FEurate and normonatremia
SIADHIncreased FEurate and hyponatremia

SIADH Neurosurg.
FEUA
SNa
Before After Before AfterCorrection of Hyponatremia

Ammonium Sulfate Precipitation of Urine Proteins


22Na Urine Protein

Inhibition of transcellular sodium transport (positive in red)
Neurosurgical patients with:increased FEurate-normonatremiaNormal FEurate-normonatremia
SIADHIncreased FEurate-hyponatremia