improving timeliness - cihi · improving timeliness of discharge abstract database data canadian...
TRANSCRIPT

Canadian Institute for Health Information
IMPROVING TIMELINESS
of Discharge Abstract Database Data

IMPROVING TIMELINESSof Discharge Abstract Database Data

Contents of this publication may be reproduced in wholeor in part provided the intended use is for non-commercialpurposes and full acknowledgement is given to the CanadianInstitute for Health Information.
Canadian Institute for Health Information377 Dalhousie StreetSuite 200Ottawa, OntarioK1N 9N8
Telephone: (613)241-7860Fax: (613)241-8120www.cihi.ca
ISBN 1-896104-29-0
© 2000 Canadian Institute for Health Information

Table of Contents
Timely Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
What is the DAD? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
What We Did to Get the Facts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2What We Got Back . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2How the Facts are Organized . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3What We Could Have Done Better . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
The Facts, Just the Facts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Documentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Organizational Policies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Education of Physicians . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Data Collection and Submission Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Submission Timeframes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13CIHI Data Edits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Let's Re-cap What We Learned . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Staffing Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Coding and Abstracting Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16What Can We Do From Here . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
AppendicesAppendix 1: Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Appendix 2: The Questionnaire . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21

1
I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Timely Data"You cannot manage what you cannot measure" was the opening statement made by theCanadian Institute for Health Information's (CIHI) Board Chairperson Michael Decterat the launch of CIHI's Annual Health Report, 2000. This statement serves as a guidingprinciple for CIHI in its efforts to develop Canada's health information databases.Implied in this statement is the fact that access to timely information is critical to ensur-ing the effective management of our health systems. Late in the fall of 1998, the CIHIBoard identified the timeliness of data—specifically, the Discharge Abstract Database(DAD) data—as an issue. Initial analysis of the data management pathway indicatedpotential areas for improvement in processes related to data submission, correction,compilation, analysis, reporting and dissemination. Of these, reducing data submissiontime delays and improving the efficiency of examining the error correction process heldthe most potential for improving timeliness of DAD data.
What is the DAD?The Discharge Abstract Database is a national database for information related to hospi-tal inpatient and day surgery events. Currently, over four million records are submittedto the DAD annually. Inpatient records submitted to DAD represent 85% of all inpa-tient discharges in Canada. Each record in the DAD captures a standard clinical, demo-graphic and administrative data set on a patient-specific basis. The database, in its pres-ent form, includes data from fiscal years 1979/1980 to 1999/2000.
The DAD was originally developed in 1963 to collect data on hospital discharges inOntario. Over time, it has expanded to provide national coverage (excluding rural hos-pitals in Manitoba and all of Quebec). Information from the DAD is used by a variety ofagencies and facilities for planning, evaluation and hospital funding. Hospitals also usethe data to support facility-specific utilization management decisions and administrativeresearch. Governments use the data for funding and system planning and evaluation.Given these uses, a consistent concern expressed by CIHI stakeholders was the timeli-ness of DAD data. Recently, CIHI identified within its data quality framework timeli-ness, accuracy and comprehensiveness as key data quality attributes that determine theoverall fitness for use of data. Consequently, an initiative to understand the factors thatcontribute to, and improve the timeliness of this data, was needed.
In 1999, a national survey was developed and conducted among Canadian acute carefacilities in selected provinces regarding the timeliness of data submission by hospitals tothe DAD. The purpose of the survey was to examine data collection and submissionprocesses in hospitals to determine what variation exists in practices related to thesesuch as documentation and coding required to complete the DAD abstract. Objectives ofthe timeliness survey were to identify best practices in the timely submission of data and,based on the results, to initiate a nationally oriented change process in data submissionand reporting.
This document describes the survey’s purpose, objectives, methodology, results and out-lines a process that will develop recommendations that, if accepted, will enhance theavailability of timely DAD data. It is hoped that a data submission and collection

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
framework will emerge from discussions of these findings that can be applied across all ofCIHI's data holdings. It is also hoped that the implementation of recommendations willlead to action that will result in timely access and use of health information leading toeffective management of our facilities, and therefore, benefiting Canadians.
What We Did To Get the FactsA project team was established consisting of two CIHI managers, a coordinator and anexternal researcher along with external consultants hired at different phases of thisproject. Provincial/territorial quality committees were invited to provide expert adviceand feedback during the design phase of the survey. (Please see Appendix 1 for detailson project team members).
Project staff wanted to involve all facilities submitting data to the DAD to contribute tothe process of discovering best practices. Therefore, all facilities registered with CIHI ascontributors to the DAD were included in the survey.
CIHI stakeholders from across Canada, provincial and territorial data quality commit-tees, CIHI staff and researchers were consulted in developing the survey. Pre-tests of thesurvey were conducted and a final version was developed and disseminated in May 1999.
The survey questionnaire was sent with an accompanying cover letter and a tracking sys-tem for monitoring response rates was implemented. Respondents were given threemonths to respond which included reminder letters and additional copies of questionnairesbeing mailed out with a closing date of July 1999.
What We Got BackA total of 616 facilities were included in the sample frame. This represents the numberof individual DAD submitting facilities as of the summer 1999. During the period ofthe questionnaire’s distribution, five facilities merged with another facility, with theother facility assuming all administrative functions including health records coding(and responding to surveys), or facilities closed. These changes reduced the sampleframe to 611. Responses were received from 468 of these facilities for an initialresponse rate of 77%.
Forty-one of these responses were not usable for various reasons. For example, for manyof these facilities, the health records coding had been assumed by another facility alto-gether, while others were no longer providing acute care and therefore declined to com-plete the questionnaire. Other questionnaires were returned blank. The final responserate therefore, was 70% or 425 facilities. Returns by province are listed in Table 1.
2

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Table 1: Response Rate by Province and Size of Hospital
How the Facts are OrganizedThe survey was designed to support an exploratory study, therefore there were noresearch hypotheses to be tested. Descriptive analyses were conducted using SPSS tocategorize average responses.
Responses were separated for analysis into three groups by size of facility defined byabstract volume because the size of hospitals is related to both variations in servicedemands and differing resources.
1. The "small" group included 328 facilities with an annual abstract volume of ≤15,000 abstracts;
2. The "medium" group included 55 facilities with an annual abstract volume of>15,000 to ≤30,000; and
3. The "large" group included 42 facilities with an annual abstract volume of >30,000.
These distinctions are used throughout the "Results" section that follows.
What We Could Have Done BetterDespite the extensive consultations and pre-tests completed, a number of areas with miss-ing data and some "out-of-range" responses that could not be coded easily resulted. In hind-sight, the project team realized that, some question response categories were not mutuallyexclusive as initially intended. Consequently, respondents replied to all alternativespresented instead of choosing one from the list provided, making interpretation difficult.
3
Province Number of SurveysReturned
Percent of OverallResponse Rate
Small Medium Large
NWT 3 0.7 1 2YK 1 0.2 1NUV 1 0.2 1NF 21 4.9 18 2PEI 4 0.9 4NS 22 5.2 21 1NB 17 4.0 12 3 2PQ 0 0 0 0 0ON 150 35.1 101 27 21MN 5 1.2 3 2SK 57 13.3 52 3 2AB 76 17.8 72 2 2BC 70 16.4 47 10 13TOTAL 425 100 328 55 42

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
The Facts, Just the FactsThe survey instrument was divided into five sections. Sections 1 and 2 obtained profileinformation on the responding facility, asking questions such as average number of sepa-rations by care type and abstracting software vendor. Section 2 obtained detail informa-tion about the coding and abstracting staff within the responding facility such as years ofexperience and work patterns. Sections 3 and 4 asked questions about coding andabstracting practices within the facility as well as physician practices where both eithercontribute to or inhibit timely submission of DAD data. Finally, Section 5 asked ques-tions pertaining to the key factors impacting timely data submission. It is recommendedthat readers refer to the survey instrument in Appendix 2 in conjunction with theirreview of the results section that follows as specific questions are referred to throughoutthe presentation of the findings.
Section 1: Facility ProfileQuestion 1.6 of the survey instrument asked respondents to estimate the number of sep-arations per month for their facility. Across all care types such as inpatient, day surgery,emergency to chronic or long term care, on average, small facilities reported a total of1,638; medium 4,314 and large 13, 679 separations per month. The responses to thisquestion for each facility were validated against CIHI's billing information provided byits Finance Department to ensure that facilities classified as small, medium and large inthis survey were also similarly classified for billing purposes which also uses abstract vol-umes. Where discrepancies emerged, we reclassified the responding facility using thebilling information provided by CIHI's Finance Department. In total, 10 hospitals out ofthe 425 that responded were reclassified as small from medium using their individualresponses to question 1.6. CIHI's billing information was deemed more reliable as it isbased on the actual number of abstracts submitted to CIHI during the study period.
According to question 1.7 which asked about the name of abstracting software vendors,78% of all responding facilities had electronic abstracting software systems to facilitatedata submission (see Table 2).
Table 2: Percent Distribution of Responding Facilities with Electronic AbstractingSystems (Q 1.7)
4
Name of Abstracting Software Vendor Percent of Responding FacilitiesMed 2020 41%MediTech 12%3M/3M with CodeFinder 11%Cactus Health Systems 4.3%Encom 2.7%Phoenix Solutions 2.4%P.A.S.S. Group 2.4%PRISM/Med 2020 2.2%No system 7%Non response 15%Total 100%

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Section 2: Coding/Abstracting Staff ProfileThis section of the survey instrument obtained detailed profile information about thecoding and abstracting staff within the responding facility such as years of experienceand work patterns. Question 2.1 asked about the average number of Full-timeEquivalent (FTE) coding/abstracting staff (regardless of where they are assigned andincluding management staff who code) by care type. As would be expected, the greaterthe volume of abstracts, the more dedicated coding and abstracting staff existed withinthe facility. On average, the number of full-time equivalent staff tripled between small tolarge facilities (see Table 3). As well, when asked in question 2.2: "Are the majority ofyour coding/abstracting staff responsible for more than acute care coding?", 83% of small, 62%medium and 56% of large facilities answered affirmatively.
Table 3: Average Number of FTE Coding/Abstracting Staff (Q 2.1)(number indicates number of responses)
When asked about the years of experience of certified Health Records Technicians(HRT) or Health Records Administrators (HRA), by size of facility, on averageHRT/HRA with three or more years of experience were more likely to be employed in amedium or large-sized facility. With respect to work practices, well over 90% of staffregardless of the size of facility both code and abstract charts.
During initial construction of the questionnaire, interviews with health records directorssuggested that illness, vacation or maternity leave were potential factors that impactedon the timely submission of DAD data. This hypothesis was not supported by the data.Question 2.5 asked respondents to indicate: "How frequently does extended (more than 5days) illness, vacation, or maternity leave in your coding/abstracting area impact on the timeli-ness of data submission to CIHI?" The responses showed that over 90% of small, mediumand large facilities respectively felt that DAD data submissions were never or rarelydelayed due to illness (see Table 4).
Table 4: Data Submission Delayed Due to Illness (Q 2.5.1)
5
Response Categories Small(avg FTE)
Medium(avg FTE)
Large(avg FTE)
Acute 1.2 2.7 5.7Day Surgery 1.1 1.3 1.6Emergency 1.2 1.3 2.3Chronic/LTC 1.0 1.2 1.5Clinics 1.1 1.0 2.0Other 1.6 1.0Overall FTE Average 1.2 1.8 3.3
Response Categories Smalln=313
Mediumn=55
Largen=41
Never 33% 18% 22%Rarely 61% 71% 71%At least once a month 4% 11% 7%At least once a week 1% 0% 0%More often 1% 0% 0%

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
As Table 5 shows, the large majority of respondents felt that rarely or never did vacationsresult in delays for DAD data submission.
Table 5: Data Submission Delayed Due to Vacation(s) (Q 2.5.2)
As Table 6 shows, the large majority of respondents felt that rarely to never did maternityleave for staff result in delays for DAD data submission.
Table 6: Data Submission Delayed Due to Maternity Leave (Q 2.5.3)
To obtain information in conjunction with the responses received around potentialdelays due to illness, vacation or maternity leave, question 2.6 asked whether facilities"hired casual relief staff for extended (more than 5 days) illness, vacation, or maternity leave?"Again the patterns were similar to those found in question 2.5. The large majority,approximately 80% of facilities, regardless of size, rarely to never hired casual relief stafffor illness or vacation. Interestingly, medium and small facilities never to rarely hiredcasual relief staff for maternity leave but a quarter of large facilities (24%) routinelyhired casual relief staff for maternity leaves for their regular staff.
When asked about the frequency of overtime hours incurred to meet submission dead-lines (Q 2.7), the majority of small (87%), medium (92%), and large (78%) "never torarely" worked overtime to meet submission deadlines (see Table 7). The last question (Q 2.8) in Section 2 asked whether coding staff were unionized and the majority ofrespondents regardless of hospital size answered affirmatively.
6
Response Categories Smalln=304
Mediumn=50
Largen=40
Never 19% 14% 13%Rarely 67% 74% 55%At least once a month 13% 10% 28%At least once a week 0% 0% 0%More often 1% 2% 5%
Response Categories Smalln=311
Mediumn=53
Largen=41
Never 72% 64% 42%Rarely 23% 34% 51%At least once a month 2% 2% 5%At least once a week 0% 0% 0%More often 1% 0% 2%

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Table 7: How frequently does coding staff work overtime to meet data submissiondeadlines? (Q 2.7)
Section 3: Coding and Abstracting PracticeSection 3 of the survey instrument asked questions about coding and abstracting prac-tices within the facility. As expected, a high percentage (over 95%) of coding andabstracting occurs within health records departments across facilities regardless of size. Asmall percentage (approximately 11%) of responding facilities indicated that coding andabstracting also occurred in patient care areas.
When asked about the nature and type of electronic coding software and associatedpractices for use of this software, two-thirds of those who responded to question 3.4 andwho were from small facilities indicated they felt "automated software (compared to ICDclassification books) facilitated timely DAD data submission". One-third of those whoresponded to question 3.4 and who were from large facilities felt "automated software(compared to ICD classification books) facilitated timely submission of DAD data".
When respondents were asked in Q 3.6 if they "abstracted directly into their abstractingsoftware", approximately two-thirds (63%) of those who responded from small, 72% of medium and 78% from large facilities indicate that they directly abstract into their software.
Interface with Admission Discharge and Transfer (ADT) systems and online accessexisted for all respondents regardless of facility size, although the likelihood was greaterfor large facilities to have online access to other systems. Nearly, two-thirds (61%) ofthose who responded to Q 3.5 from small facilities, 96% of medium and 93% of largefacilities indicated that abstracting systems were interfaced with the facility's ADT sys-tem. Online access to reports was more likely for large facilities than for respondentsfrom small facilities (see Table 8).
Table 8: Does your coding staff have electronic online access to (Q 3.7)*number is count of yes responses for total of that category, based on valid responses only
7
Response Categories Smalln=319
Mediumn=54
Largen=40
Never 54% 31% 33%Rarely 33% 61% 45%At least once a month 10% 6% 10%At least once a week 1% 2% 4%More often 2% 0% 8%
YES Small n* Medium n* Large n*
Discharge summaries 23% 69/304 38% 18/51 33% 18/40
Operative reports 21% 64/301 38% 18/51 33% 18/40
Lab data 13% 38/302 41% 19/51 33% 21/42
Radiology reports 19% 56/299 47% 22/51 44% 22/42
I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
A particular concern identified by data quality staff contacted during survey design wasthe frequency of abstracts being submitted to CIHI based on incomplete charts. Theresults are not presented here due to the poor numbers that responded to the question.However, large numbers of respondents indicated that while abstracts are submitted toCIHI based on incomplete charts, a "follow-up process was in place in their facility to verifyand update diagnoses and procedures from incomplete charts". Of those who responded toquestion 3.8, which asked: "If you code from incomplete charts, is there a follow-up process inplace to verify and update diagnoses and procedures once the charts are complete?", 79% ofsmall, 90% medium and 92% of large facilities answered affirmatively.
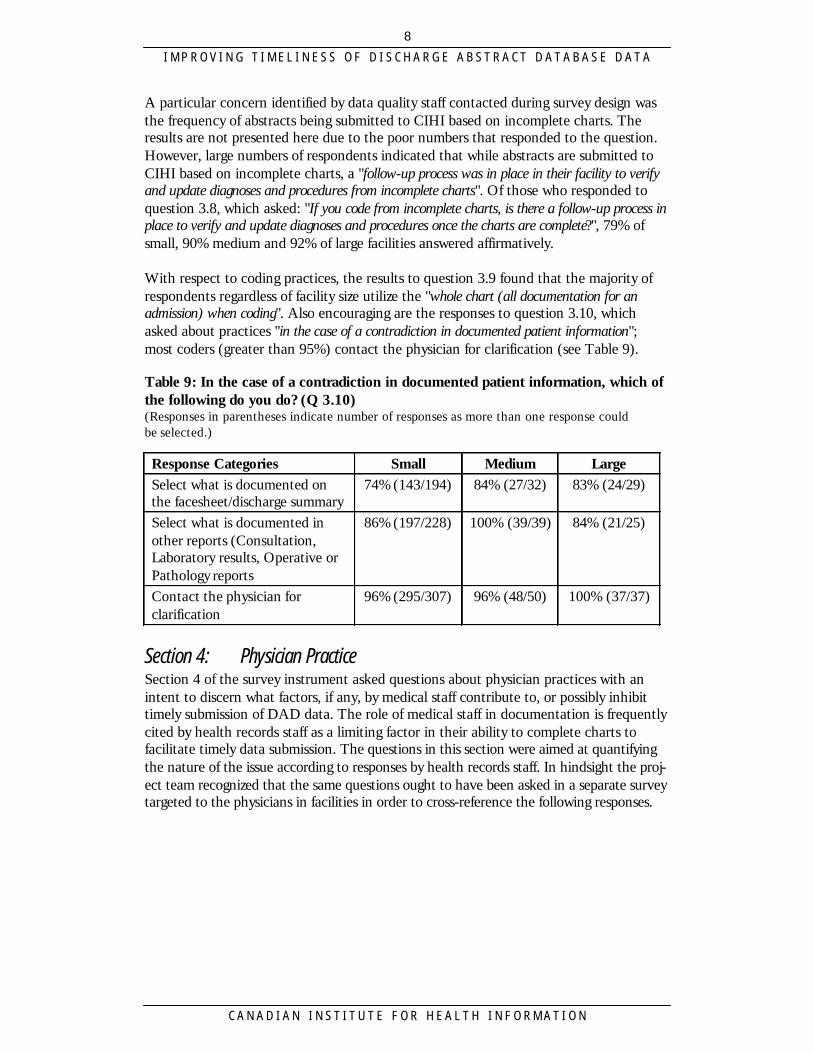
With respect to coding practices, the results to question 3.9 found that the majority ofrespondents regardless of facility size utilize the "whole chart (all documentation for anadmission) when coding". Also encouraging are the responses to question 3.10, whichasked about practices "in the case of a contradiction in documented patient information";most coders (greater than 95%) contact the physician for clarification (see Table 9).
Table 9: In the case of a contradiction in documented patient information, which ofthe following do you do? (Q 3.10)(Responses in parentheses indicate number of responses as more than one response could be selected.)
Section 4: Physician PracticeSection 4 of the survey instrument asked questions about physician practices with anintent to discern what factors, if any, by medical staff contribute to, or possibly inhibittimely submission of DAD data. The role of medical staff in documentation is frequentlycited by health records staff as a limiting factor in their ability to complete charts tofacilitate timely data submission. The questions in this section were aimed at quantifyingthe nature of the issue according to responses by health records staff. In hindsight the proj-ect team recognized that the same questions ought to have been asked in a separate surveytargeted to the physicians in facilities in order to cross-reference the following responses.
8
Response Categories Small Medium LargeSelect what is documented onthe facesheet/discharge summary
74% (143/194) 84% (27/32) 83% (24/29)
Select what is documented inother reports (Consultation,Laboratory results, Operative orPathology reports
86% (197/228) 100% (39/39) 84% (21/25)
Contact the physician forclarification
96% (295/307) 96% (48/50) 100% (37/37)

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DocumentationQuestion 4.1, asked respondents to "estimate how often chart information was complete whenfacilities were ready to submit data to CIHI". Chart information in this question pertained toa) face sheet, b) discharge summary, c) operative reports, d) pathology reports, e) physi-cian's orders, f) progress notes, g) consults, h) diagnostic investigations or i) other. Onaverage, respondents from small facilities reported that 90% of chart documentation wascomplete by the time facilities were ready to submit to CIHI. Similar percentages werefound from respondents from medium-sized facilities. The proportion dropped somewhatfor large-sized facilities, to approximately 70% on average.
Question 4.2 asked: "What physician practices cause charts to be incomplete?" and providedan open-ended, free text field for response in the survey instrument (see Table 10).
Table 10: "What physician practices cause charts to be incomplete?"
Organizational PoliciesHealth records staff during the construction of the survey instrument indicated to the projectteam that they lack authority to ensure compliance by the medical staff to complete charts,which inhibits timely submission to the DAD. Consequently, questions were created for the sur-vey regarding organizational policies that help to ensure compliance for chart completion.Question 4.3 asked: "Does the Health Records Department or hospital have policies to promote atimely completion of patients' charts by physicians within a specific time period?" The responses weresomewhat surprising given the project team's original reason for including such a question.Approximately, 93% of respondents from small, 98% of medium and 98% of respondents fromlarge facilities indicate that policies existed in their facility to promote timely chart completion.
Additional questions were asked in the survey instrument around the nature of associatedsanctions for not adhering to policies for timely completion. The questions probed aroundenforcement of sanctions for failing to complete charts. Generally, policies in hospitalssupported suspension of physician privileges for admission, on call, patient treatment, andsurgery privileges for failing to complete charts. Question 4.4 asked: "What percentage ofthe time are physician privilege suspension policies for incomplete charts enforced in your facility?"On average, large facilities are twice as likely as small facilities to suspend physician privi-leges for incomplete charts. Approximately 19% of those respondents who answered thequestion from small facilities, 38% from medium and 47% of respondents from large facili-ties indicated that their facility had suspended physician's privileges for incomplete charts.However, question 4.6 asked whether "physician privilege suspensions are generated automati-cally?" and 9% of small, 25% of medium and 11% of respondents from large facilitiesanswered affirmatively.
9
Coded Responses Number of Respondents"Just not dictating discharge summaries on a timely basis" 222“Physician turnover, holidays and other absences” 53“A lack of consistency in dictating/ signing habits” 40“Health records staff lack authority to make them get thematerial or signatures completed”
27
“A problem with documentation (i.e. failure to indicatefinal Diagnosis or Most Responsible Diagnosis)”
26

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Question 4.10 asked: "If there are hospital policies about physician suspension, within whichtimeframe must the discharge summary be completed and signed?" Nearly two-thirds ofrespondents from small size facilities indicated less than 14 days while almost one-half ofmedium to large-sized facilities indicated the same (see Table 11).
Table 11: If there are hospital policies about physician suspension, within whichtime frame must the discharge summary be completed and signed? (Q 4.10)*number is based on valid responses only and more than one answer was sometimes given
Finally, when asked in question 4.11: "How long does it usually take following the dischargedate for physicians to complete charts for submission to the Discharge Abstract Database?",approximately one-half of respondents indicated between 15 to 30 days (see Table 12).
Table 12: How long does it usually take following the discharge date, for physiciansto complete charts for submission to the Discharge Abstract Database? (Q 4.11)*number is based on valid responses only and more than one answer was sometimes given
Education of Physicians More than two-thirds of all respondents regardless of the size of facility, indicated thatphysicians are educated about submission timeframes. Approximately 81% of those whoresponded to Q 4.7 from small, 65% from medium and 73% from large facilities indicat-ed that "physicians in their facility are educated about submission timeframes". The trainingmechanisms used in facilities vary from orientation booklets, memorandums to roundsand other presentations. Memorandums were the most likely training mechanism used,with more than 90% of respondents indicating they had used these as part of educating physicians about submission timeframes.
10
Response Categories Small *n=290
Medium *n=55
Large *n=35
Less than 14 days 61% 49% 46%15 to 30 days 29% 40% 43%More than 30 days 3% 9% 3%No time limit 3% 2% 9%Not known 4% 0% 0%
Response Categories Small *n=311
Medium *n=54
Large *n=38
Less than 14 days 26% 13% 0%15 to 30 days 48% 45% 54%More than 30 days 24% 31% 46%No time limit 6% 4% 0%Not known 4% 0% 9%

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Section 5: Submission of Abstracts to CIHISection 5 of the survey instrument asked questions pertaining to the key factors impact-ing timely data submission of DAD abstracts. It was hoped by the project team that thissection would yield results or insights in regards to the appropriate action that could betaken within a change process. In general, staffing issues, chart issues and vendor issueswere the most commonly cited factors identified by health records staff as impactingtimely submission of DAD data. These findings were relatively consistent regardless ofhospital size, with minor variations (see Table 13).
Question 5.1 asked: "What key factors at your facility impact the timeframe for submittingdata to the Discharge Abstract Database at CIHI?" Eighteen suggested items divided intosix different subject areas were offered for respondents to select. The six subject areasincluded: 1) staffing issues, 2) inexperienced staff, 3) staff required to work in otherareas of the department, 4) incomplete charts at time of coding, 5) computer issues and6) other issues. For each of the total of 18 items in these six areas, respondents wereable to choose among three responses: "very important", "somewhat important" and"not important". The following summarizes the results by hospital size using an arbitrarythreshold of 70% of respondents that indicated somewhat to very important for the item.
Table 13: "Somewhat to Very Important" Factors affecting submission of DAD datato CIHI by Small, Medium and Large Size Hospitals (Q 5.1)*numbers indicate minimum and maximum of those who responded
Hospitals—LargeThose who responded to question 5.1 and were from large-sized hospitals reported insuf-ficient transcription staff (79%), insufficient coding staff (82%), insufficient abstractingstaff (72%), incomplete charts at time of coding (100%), vendor issues (72%), softwareissues (78%), and charts required for readmission (76%) as somewhat to very importantfactors at their facility that impact the timeframe for submitting data to the DAD.
11
IssueSmall *
min=253max=278
Medium *min=46max=53
Large *min=33max=41
Insufficient transcription staff 59% 73% 79%Insufficient coding staff 71% 81% 79%Insufficient abstracting staff 69% 83% 72%Staff required to work in other areas ofthe department
70% 56% 39%
Incomplete chart at time of coding 79% 98% 100%Vendor issues 51% 54% 72%Software issues 54% 57% 78%Charts required for readmission 54% 57% 75%

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Hospitals—MediumThose who responded to question 5.1 and were from medium-sized hospitals reportedinsufficient transcription staff (73%), insufficient coding staff (81%), insufficientabstracting staff (83%) and incomplete charts at time of coding (98%) were somewhat tovery important factors at their facility that impact the timeframe for submitting data tothe DAD.
Hospitals—SmallThose who responded to question 5.1 and were from small-sized hospitals reported insuf-ficient coding staff (71%), staff required to work in other areas of the department (70%)and incomplete charts at time of coding (79%) were somewhat to very important factorsat their facility that impact the timeframe for submitting data to the DAD. Table 13 showsthat the key factors which prevent a health records department from timely submission tothe DAD are quite similar across facilities regardless of size.
Interestingly, an internal validity check built into the survey asked later on in the instru-ment in question 5.5: "What factors could assist you in submitting data to CIHI in a moretimely fashion without compromising data quality?" The responses to this question did gen-erally support the findings in question 5.1 above. One hundred and twenty-sevenrespondents requested better physician compliance, 112 identified the need for addition-al staff , 88 respondents want electronic links to CIHI, 49 wanted better internal systems(i.e. transcription, abstracting), 16 cite vendor problems, and 11 respondents wantedbetter timeliness from CIHI with respect to updates for abstracting software. Thoughasked differently in question 5.5 than in question 5.1, the responses are generally consis-tent in that the key factors affecting timely DAD data submission include: staffing issues,chart issues and vendor issues.
The remaining questions in Section 5 asked about the submission practices at therespondent's facility and submission timeframes for their facility.
Data Collection and Submission PracticesWhen asked in question 5.2 about their personal knowledge of data submission policies,most respondents regardless of facility size indicated they were knowledgeable about hos-pital level policies and CIHI policies but were less sure about regional or provincial poli-cies regarding data submission. On average, 90% of respondents who answered question5.2 were knowledgeable about hospital or CIHI policies regarding data submission.However, these percentages fell to between 36% to 76% of respondents who felt theywere knowledgeable about regional or provincial policies.
Question 5.3 asked whether respondents in their facilities collected more data than wassubmitted to CIHI. Approximately 83% and 79% of medium and large-sized facilitiesrespectively collected more data than was submitted to CIHI while only 44% of small-sized facilities did the same.
12

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
At the time the survey was conducted, which was the spring 1999, the majority of small-sized facilities were using rudimentary methods of data submission delivery to CIHI.According to question 5.4, on average, 63% of small-sized facilities indicated they sub-mitted abstracts to CIHI via mail or courier of diskettes. Approximately 49% and 41% ofmedium and large-sized facilities, respectively, used mail or courier. Only one-quarter(27%) of small-sized facilities compared to 40% and 52% of medium and large-sizedfacilities, respectively, used a modem to transmit electronically DAD abstracts to CIHI.Recognizing that CIHI had announced in that same period that for all abstracts effectiveApril 2001, data would only be accepted electronically, it is anticipated that the samequestion if asked today would yield dramatically different results.
Submission TimeframesThe combination of results from questions 5.6 to 5.9 of the survey that ask about submis-sion timeframes represent the core of the survey's objectives. Question 5.6 asked: "Howquickly could you submit data to CIHI without compromising data quality?" On average respons-es indicated: 26 days for small, 26 days for medium and 25 days for large-sized facilities.
Questions 5.7 asked whether the respondent's provincial Ministry of Health require datato be submitted to CIHI within certain timeframes. Respectively, 70%, 89% and 90% ofrespondents from small, medium and large-sized facilities answered affirmatively. Whenthose who answered affirmatively were then asked in question 5.8 “in what timeframe?”,most respondents regardless of facility indicated within a 60 day period after month-end.CIHI and provincial Ministry of Health data submission timeframe policies are presentedin Table 14.
Table 14: Provincial Policies for DAD Data Submission for those Provinces withKnown Policies
*Note: Year-end is typically March 31
13
Province Existing Data Submission Policy
Newfoundland 90 days post year-end*
Nova Scotia 30 days after month-end
Ontario 3 months after year-end (June 30)
Saskatchewan 60 days after month-end
Alberta 90 days after month-end
CIHI DAD database year-end close is July 15for production of comparative reports(i.e. CHAP)

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Respondents were then asked within what timeframes they felt they could comply with aMinistry of Health requirement for data submission. The majority of respondents regard-less of size of facility felt they could comply with a Ministry of Health data submissionrequirement of 30 to 45 days after month-end (see Table 15).
Table 15: Could you comply with a ministry requirement to submit data within thefollowing timeframe? (Q 5.9)*number is based on valid responses only. Percentages reflect proportion that checked that celland more than one cell was often checked by the same respondent.
In hindsight, the project team recognized the need to have clearly stated: "Please selectonly one option" for the above question. However, taking an aggregate view, more thanhalf of all respondents (47% small; 66% medium and 96% large-sized facilities) felt theycould comply with a ministry requirement to submit within 60 days after month-end.
This is very encouraging but has not been supported by past practice. Figure 1, takenfrom CIHI management information generated on fiscal year 1998/1999 data on hospitalsubmission times, indicates that the majority of hospitals regardless of size or provincetypically submit data to the DAD more than 120 days after month-end. This is doublethe time which respondents indicated in question 5.9 they felt they could meet ifrequired to by their respective Ministry of Health.
Figure 1: Hospital Submission Timeframes for Discharge Abstract Database FY 1997/1998 to 1998/1999
14
YES Small Medium LargeWithin 30 days aftermonth end
44% (84/189) 39% (15/38) 39% (13/33)
Within 45 days aftermonth end
28% (93/151) 39% (23/37) 68% (13/39)
Within 60 days aftermonth end
47% (155/170) 66% (36/39) 96% (25/26)
Not known 18/19 1/2 2/2
0
20
40
60
80
100
<31 31-60 61-90 91-120 > 120
Days Elapsed From CIHI CHAP Due Date
% H
ospi
tals
Sub
mitt
ing
1997/98
1998/99

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Further investigation is clearly warranted between what respondents believe to be reasonabletimeframes for data submission versus what actually transpires.
CIHI Data EditsA common suggestion that most facilities and representatives from the vendor commu-nity have raised to CIHI is that CIHI ought to share with vendors their data edits toenable a clean data submission of abstracts from source which would in turn reduce timespent on data corrections. CIHI has announced that as of April 2001, a copy of the editlogic used throughout the Discharge Abstract Database would be made available to allvendors and facilities submitting data to the DAD. However, based on communicationsbetween CIHI and vendors, most abstract software vendors in an attempt to add valueto their products have taken CIHI error report messages and developed edit logic whichthey have then built into their products. Many hospitals have extended this need byrequesting facility-specific edits be incorporated into their version of the vendor'sabstracting software. This was clearly supported by the findings in questions 5.10 (see Table 16).
Table 16: Do you have most CIHI edits (Q 5.10.1) and/or facility-specific (Q 5.10.2) edits in your electronic abstracting system?
Let's Re-cap What We LearnedTaking into consideration the data limitations outlined earlier, there are findings in thedata that are worth considering as a basis for policy change to improve timeliness ofDAD data submission.
Staffing Issues1. In general there is a monotonic relationship between facility size and the number of
available coding staff (Q 2.1). Large facilities have more staff than do medium sizefacilities that have more than small facilities. This trend appears to weaken withrespect to staff that is coding for day surgery and emergency areas. The same num-bers of coders are available, on average, in both small and medium-sized facilities.However, these numbers are still less than that available in large facilities, but per-haps there is an irreducible minimum number of staff to be effectively deployed in acoding area.
2. There is an inverse relationship between facility size and whether the majority ofcoding/abstracting staff is responsible for more than acute care coding (Q 2.2). Thesmaller the facility the more staff works beyond acute care. Larger facilities havemore experienced staff (Q 2.3) and most health records staff both code and abstractcharts. There is no difference by facility size.
15
YES Smalln=259
Mediumn=51
Largen=42
CIHI edits 94% 92% 86%Facility-specific edits 42% 86% 88%

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
3. More delays in coding/abstracting are reported in large hospitals due to illness, vacationand particularly due to maternity leave (Q 2.5) even though the large facilities moreoften hire casual relief staff (Q 2.6). Moreover, health records staff in large hospitalsmore frequently work overtime to meet data submission deadlines (Q 2.7).
4. More large facility HRTs are unionized than in medium or small facilities. FewerHRAs are unionized in small facilities than are reported to be in medium or largefacilities (Q 2.8).
5. Almost all coding and abstracting is done in Health Records departments in all facil-ities (Q 3.1). However, more large facilities have coding and abstracting occurring inpatient care areas than do small and medium-sized facilities.
6. Fewer small facilities have electronic online access to necessary data (Q 3.7) such asdischarge summaries, operative reports, lab data, and radiology reports.
Coding and Abstracting Practices7. Large facilities submit data to CIHI with significantly less complete information than
do small and medium-sized facilities (Q 4.1). All reporting facilities however, regard-less of size, report having policies to promote timely physician completion of patientcharts (Q 4.3). However, large facilities are much more likely to enforce their policy(Q 4.4).
8. There is a facility size differential in the manner in which physician privileges aresuspended (Q 4.5). Admission and surgical privileges are less likely to be suspendedin small hospitals. On call and patient treatment privileges are more likely to be sus-pended in medium hospitals. On call privileges are least likely to be suspended in largehospitals. Medium-sized facilities are most likely to automatically suspend privileges (Q 4.6). However, they also have the most time latitude in their policy (Q 4.10).
9. All facilities report educating their physicians about submission timelines (Q 4.7).Small hospitals are least likely to use orientation booklets for that purpose and largefacilities more likely to use rounds and other presentations (Q 4.8).
10. Key factors impacting the timely submission to CIHI vary slightly by facility size (Q 5.1). Large and medium facilities indicate insufficient and inexperienced staff asvery important impediments. Small hospitals have more trouble with staff requiredto work in other areas of the department. Incomplete charts at coding are reportedas an important factor more often by medium-sized facilities. Large facilities havemore problems with computer issues. Absent charts, charts required for readmissionor audit review are more problematic in large facilities.
11. The transmission method to CIHI appears to vary by facility size (Q 5.4). More smallfacilities mail in data; more medium-sized use couriers and fewer small facilities useelectronic means. Almost all (90%) of medium-sized facilities have the CIHI edits intheir abstracting systems. Only 78% of small and large facilities report the same.
16

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
What Can We Do From HereThis project began with the objective of improving the timeliness of DAD data collec-tion and submission processes. The summary suggests a number of possible policy direc-tions. Encouraging is the fact that many of the findings fail to represent insurmountableobstacles. Most can be addressed through process changes at the local level that wouldbe facilitated by hospital or provincial policies around data submission that are enforced.
CIHI recently established a Provincial and Territorial Steering Committee for theDAD/Hospital Morbidity Database. Members for this committee were selected from therespective provincial and territorial Ministries of Health and the key criterion for participa-tion was that members have decision making authority for matters related to DAD/Morbidity data collection. Facilities were consulted in the development of recommendationsfor Steering Committee members.
A first meeting of this Steering Committee is being scheduled for winter 2000 with anintent to discuss this survey and findings from its analysis as an agenda item.Recommendations therefore, were not included in this report as it is necessary to identi-fy the mechanisms for change through consultations with this Steering Committee.Within CIHI, it was felt that to await development of recommendations and then dissem-inate this report was not considered prudent. Instead, once recommendations from thiswork are identified, a process to share these with CIHI stakeholders and readers of thisreport will occur. As a starting point, reviewers of this report have suggested the followingminimum recommendations:
1. Encourage provinces and territories to establish policies requiring data suppliers tosubmit data and required corrections to CIHI within 31 days following the end ofthe period.
2. Encourage provinces and territories to establish financial incentives/penalties thatrelate to the submission of data within specified deadlines.
3. That CIHI revise the deadline for data submissions for comparative reports (i.e.CHAP reports) to 30 days (from 85) after the end of the first 3 quarters, with the 4thquarter remaining the same, and distribute reports 25 days (from 37 days) followingthe deadline.
4. CIHI should investigate the feasibility and advisability of revising its pricing struc-ture of core and non-core plan subscribers to include financial incentives for earlydata submission.
What is clear is that considerable further work must be done to describe and verify rele-vant "best practice" and supportive action that also recognizes differences in circum-stances across facilities. As well, designing a change process will have to involve leadersfrom the field, provincial champions and tenacity around some simple principles. First,however, there must be a decision amongst these leaders in partnership with CIHI abouthow to pursue actual change. It is hoped that feedback from readers of this report willgenerate ideas for how to do so.
17

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Appendix 1: Acknowledgements
Project Management Structure
Project Team Christine Fitzgerald, Director, Product ManagementNizar Ladak, Manager, Clinical and Administrative DatabasesDaria Parsons, Manager, Clinical RegistriesMicheline Mistruzzi, Coordinator, Discharge Abstract DatabaseAndrew Kmetic, External Consultant
External Research AdvisorDr. Carl van Walraven, Clinical Epidemiology Unit, Ottawa Civic Hospital
External Participation in Survey DevelopmentKaren Barker, Burnaby Hospital Site, British ColumbiaKathleen Addison, Calgary Regional Health Authority, Alberta Linda Miller, Alberta Health, AlbertaSheri McMann, Saskatchewan Health, Saskatchewan Diane French, St. Boniface Hospital, ManitobaHy Eliasoph, Ontario Hospital Association, OntarioChristine Pember, Ontario Hospital Association, Ontario Barbara Harvie, Nova Scotia Department of Health, Nova Scotia Charlotte Smith, Colchester Regional Hospital, OntarioMaureen Aucoin, QEII Health Sciences Centre, Nova ScotiaGlennis Nathanson, Cape Breton Regional Hospital, Nova ScotiaMarsha Wong, St. Martha's Regional Hospital, Nova ScotiaBeverley Dickie, Department of Health & Wellness, New Brunswick Faye Campbell, Department of Health & Social Services, Prince Edward Island Sandra Cotton, Newfoundland & Labrador Centre for Health Information, Newfoundland Pat Booth, Stanton Regional Health Board, Northwest Territories
19

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
Appendix 2: The Questionnaire
21
DAD Timeliness Survey
1. Institution Profile
This mailing label shows the information we currently have on file. Please make any corrections in the lines below.
Mailing label in here.
1.1 Name of Institution:
1.2 Name of Region:
1.3 Mailing Address:
1.4 Name of Director/Regional Leader of Health Records:
1.4.1 Contact Phone number:
1.4.2 Fax Number:
1.4.3 E-mail:
1.5 Number of active acute care beds:
1.6 Please indicate the average number of separations per month in the table below. (Include discharges,deaths, and stillbirths.)
Average Number of Separations per Month
TOTAL
Inpatient
Day surgery
Emergency
Clinics
Rehabilitation
Chronic/Long Term Care
Department of Veteran Affairs
1.7 Name of abstracting software vendor: _______________________________________________________

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DAD Timeliness Survey Page 2
22
2. Coding/Abstracting Staff
2.1 Total number of Full Time Equivalent (FTE) coding/abstracting staff (regardless ofwhere they are assigned and including management staff who code):2.1.1 acute __________
2.1.2 day surgery __________
2.1.3 emergency __________
2.1.4 chronic/Long term care (LTC) __________
2.1.5 clinics __________
2.1.6 other (Rehabilitation, Department of Veteran Affairs) _______________
2.2 Are the majority of your coding/abstracting staff responsible for more thanacute care coding? q YES q NO
2.3 Please indicate the experience level of coding staff in the tables below:
Table 2.3.1: Staff FTEs for Acute Care
Number of Staff Coding or AbstractingStaffing Categories Experience
(2 years or less) (3 years or more)
HRT/HRAClerical Staff
Nurse PractitionersPhysiciansOther (specify)
Table 2.3.2: Staff FTEs for Day Surgery
Number of Staff Coding or AbstractingStaffing Categories Experience
(2 years or less) (3 years or more)HRT/HRA
Clerical StaffNurse PractitionersPhysiciansOther (specify)
2.4 Does a staff member both code and abstract a chart? q YES q NO
2.5 How frequently does extended (more than 5 days) illness, vacation, or maternity leave in yourcoding/abstracting area impact on the timeliness of data submission to CIHI?
Delayed Due to Illness
Delayed Due toVacation
Delayed Due toMaternity Leave
q neverq rarelyq at least once a monthq at least once a weekq more often
q neverq rarelyq at least once a monthq at least once a weekq more often
q neverq rarelyq at least once a monthq at least once a weekq more often
Acute Care
Day Surgery

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DAD Timeliness Survey Page 3
23
2. Coding/Abstracting Staff (cont’d)
2.6 Do you hire casual relief staff for extended (more than 5 days) illness, vacation, or maternity leave?
Relief for Illness Relief for Vacation Relief for Maternity Leave
q never q rarely q at least once a month q at least once a week q more often
q never q rarely q at least once a month q at least once a week q more often
q never q rarely q at least once a month q at least once a week q more often
2.7 How frequently do coding staff work overtime to meet data submission deadlines?q neverq rarelyq at least once a monthq at least once a weekq more often
2.8 Are coding staff unionized? 2.8.1 HRTs q YES q NO
2.8.2 HRAs q YES q NO
2.8.3 others (i.e. clerical) q YES q NO
Note: This section refers to acute care and day surgery ONLY.
3. Coding and Abstracting Practice3.1 Indicate the percentage of coding and abstracting performed in the following locations:
3.1.1 Health Records Department %
3.1.2 patient care areas in your hospital %
3.1.3 off-site (i.e. home) %
3.2 Is your facility responsible for coding and abstracting data of a second site? q YES q NO
3.3 Do you usually use automated encoding software?q not knownq neverq sometimesq always
3.4 In your opinion, does the use of automated software (compared to ICD classificationcode books) facilitate timely submission to CIHI? q YES q NO
3.5 Is your abstracting software interfaced with your ADT (admission, discharge,transfer) system? q YES q NO
3.6 Does your coding staff code or abstract directly into your software (versus using worksheet)? q YES q NO3.7 Does your coding staff have electronic on-line access to:
3.7.1 discharge summaries q YES q NO
3.7.2 operative reports q YES q NO
3.7.3 lab data q YES q NO3.7.4 radiology reports q YES q NO

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DAD Timeliness Survey Page 4
24
3. Coding and Abstracting Practice (cont’d)
Estimate the percentage of abstracts initially submitted to CIHI based on incomplete charts? __________%
3.8 If you code from incomplete charts, is there a follow-up process in place to verify and update diagnosesand procedures once the charts are complete? q YES q NO
3.9 For coding purposes, do you usually:
q refer only to the facesheet
q refer to the facesheet, discharge summary and/or operative report
q refer to some other combination
q refer to the whole chart (all documentation for an admission)
3.11 In the case of a contradiction in documented patient information, which of the following do you do:(More than one response may be selected.)3.11.1 select what is documented on the facesheet/discharge summary q YES q NO
3.11.2 select what is documented in other reports (Consultation, Laboratory results, Operative orPathology reports) q YES q NO
3.11.3 contact the physician for clarification q YES q NO
3.11.4 other (specify) ____________________________________________________________
This section refers to acute care and day surgery ONLY.
4. Physician Practice4.1 Estimate how often the following chart information is complete when you are ready to submit data to CIHI.
Table 4.1.1: Complete Chart Information
Chart Information % Complete Information % Signed
Face sheet
Discharge summary
Operative report
Pathology report
Physician's orders
Progress notes
Consults
Diagnostic investigations
Other (specify)
4.2 What physician practices cause charts to be incomplete?
4.3 Does the Health Records Department or hospital have policies to promote a timelycompletion of patients’ charts by physicians within a specific time period? q YES q NO

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DAD Timeliness Survey Page 5
25
4. Physician Practice (cont’d)
4.4 What percentage of the time are physician privilege suspension policies for incomplete charts enforced inyour facility? ____________%
4.5 Which physician privileges are suspended for incomplete charts?4.5.1 admission q YES q NO
4.5.2 on call q YES q NO
4.5.3 patient treatment q YES q NO4.5.4 surgery privileges q YES q NO
4.5.5 other (specify) ______________________________________________________________4.6 Are physician privilege suspensions generated automatically? q YES q NO
4.7 Are physicians educated about submission timeframes? q YES q NO (Please go to # 4.9)
4.8 Which training mechanisms have been used to educate physicians about submission timelines?
4.8.1 orientation booklets q YES q NO
4.8.2 memos q YES q NO
4.8.3 rounds, other presentations q YES q NO
4.9 Are the completion and suspension policies standardized across all facilities in your region?q YES q NO q NOT KNOWN
4.10 If there are hospital policies about physician suspension, within which time frame must the dischargesummary be completed and signed?4.10.1 q < 14 days
4.10.2 q >15 to <30 days4.10.3 q > 30 days4.10.4 q no time limit
4.10.5 q not Known
4.11 How long does it usually take following the discharge date for physicians to complete charts forsubmission to the Discharge Abstract Database?4.11.1 q < 14 days
4.11.2 q <15 to <30 days
4.11.3 q > 30 days4.11.4 q no time limit4.11.5 q not Known
4.12 What percentage of the following fields on the facesheet is complete? (Estimate if necessary.)
4.12.1 Most Responsible Diagnosis __________%
4.12.2 Pre-admit Co-morbidities __________%
4.12.3 Post-admit Co-morbidities __________%
4.13 In your opinion, when the facesheet is complete, how reliable are the following?
4.13.1 Most Responsible Diagnosis q Always q Usually q Sometimes q Never
4.13.2 Pre-admit Co-morbidities q Always q Usually q Sometimes q Never
4.13.3 Post-admit Co-morbidities q Always q Usually q Sometimes q Never

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DAD Timeliness Survey Page 6
26
Note: This section refers to acute care and day surgery ONLY
5. Submission of Abstracts to CIHI5.1 What key factors at your institution impact the timeframe for submitting data to the Discharge Abstract
Database at CIHI? Please place a check (v) in the appropriate boxes in the chart below.
Very Important SomewhatImportant
Not Important
Staffing Issues§ Insufficient number of clerks§ Insufficient number of transcription
staff§ Insufficient number of coding staff§ Insufficient number of abstracting staff§ Insufficient number of quantitative
analysis staffInexperienced staff
Staff required to work in other areas ofdepartment
Incomplete charts at time of coding
Computer Issues
§ Hardware limitations§ System downtime§ Vendor issues§ Software issuesOther Issues
§ Coding process is viewed as a lowpriority
§ High demand for special studies orresearch
§ Submission to CIHI through theprovincial Ministry of Health
§ Charts unavailable in department(e.g. research projects outsidedepartment)
§ Charts required for readmission§ Charts required for audit review§ Other (specify)

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DAD Timeliness Survey Page 7
27
5. Submission of Abstracts to CIHI (cont'd)5.2 Do you know the policies for data submission to the following levels?
5.2.1 hospital q YES q NO
5.2.2 regional (if applicable) q YES q NO
5.2.3 provincial q YES q NO
5.2.4 CIHI q YES q NO
5.3 Do you collect more data elements than you submit to the CIHI Discharge Abstract Database?q YES q NO
5.4 Which method of delivery is used by your hospital to submit abstracts to CIHI?
q mailq courierq modemq other (specify) ______________________________________________________________________
5.5 What factors could assist you in submitting data to CIHI in a more timely fashion without compromisingdata quality? (List below.)
5.6 How quickly could you submit data to CIHI without compromising data quality?__________________________ calendar days
5.7 Does your provincial Ministry require submission of data? q YES q NO q NOT KNOWN
5.8 If YES, within what timeframe?
5.8.1 q within 30 days after month end
5.8.2 q within 45 days after month end
5.8.3 q within 60 days after month end
5.8.4 q other (specify)
5.8.5 q not known
5.9 Could you comply with a Ministry requirement to submit data within the following time frames?
5.9.1 q 30 days after month end q YES q NO
5.9.2 q 45 days after month end q YES q NO
5.9.3 q 60 days after month end q YES q NO
5.9.4 q not known
5.9.5 q other (specify)
5.10 If you have edits for electronic abstracts:
5.10.1 Do you have most CIHI edits in your abstracting system?q YES q NO
5.10.2 Do you have facility specific edits in place in addition to CIHI edits?q YES q NO
5.11 For fiscal year 1998/99, did you submit the majority of your corrections to CIHI before the: production ofquarterly reports in the:5.11.1 first quarter q YES q NO
5.11.2 second quarter q YES q NO
5.11.3 third quarter q YES q NO
5.11.4 fourth quarter q YES q NO

I M P R O V I N G T I M E L I N E S S O F D I S C H A R G E A B S T R A C T D A T A B A S E D A T A
C A N A D I A N I N S T I T U T E F O R H E A L T H I N F O R M A T I O N
DAD Timeliness Survey Page 8
28
Comments____________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________________
________________________________________________________________________________
Please provide the following information for person completing this survey.
Name: __________________________________________________________
Title: __________________________________________________________
Tel: ____________________ Fax: __________________ E-mail: _______________________
Thank you for your time in completing this survey.