improving patient safety background & legislation impact of iom report “to err is human...
TRANSCRIPT

Improving Patient SafetyBackground & Legislation
Impact of IOM report “To Err is Human (1999)
The National Quality Forum NQF Safe Practices for Better Health Care
(2003) The Quality Choir-Joint Commission,
Institute for Healthcare Improvement, Agency for Health Research & Quality, National Quality Forum, the LeapFrog Group & Centers for Medicare & Medicaid (CMS)

Reportable Adverse Events (Never Events)SITUATION:Treatment for some “hospital acquired conditions” will not be paid by CMS and some private payors. These conditions are generally known as reportable adverse events or “never events.”
BACKGROUND: REPORTABLE ADVERSE EVENTS (NEVER EVENTS):• In May of 2006, CMS (Center for Medicare and Medicaid Services) issued a list of non- covered events scheduled for a gradual phase in with the initial eight being scheduled for 2008 implementation.
• In January 2008, following a request from Governor Gregoire, all hospitals which are members of the Washington State Hospital Association, adopted a voluntary agreement which states that “when an adverse event occurs, no patient will be required to pay for care related to the event by the physician or facility directly involved in care.” This is effective now and includes all the adverse events listed on the next pages.

Adverse Health Events1. Surgery performed on the wrong body part.
2. Surgery performed on the wrong patient.
3. Wrong surgical procedure performed on a patient.
4. Unintended retention of a foreign object in a patient after surgery or other procedure.
5. Intraoperative or immediately post-operative death in an ASA Class 1 patient.
6. Patient death or serious disability associated with the use of contaminated drugs, devices, or biologics provided by the healthcare facility.
7. Patient death or serious disability associated with the use or function of a device in patient care in which the device is used or functions other than as intended.
8. Patient death or serious disability associated with intravascular air embolism that occurs while being cared for in a healthcare facility.
9. Infant discharged to wrong person.
10. Patient death or serious disability associated with patient elopement (disappearance).
11. Patient suicide or attempted suicide resulting in serious disability, while being cared for in a healthcare facility.
12. Patient death or serious disability associated with a medication error (e.g. errors involving the wrong drug, wrong dose, wrong patient, wrong time, wrong rate, wrong preparation or wrong route of administration.
13. Patient death or serious disability associated with a hemolytic reaction due to administration of BO/HLA-incompatible blood or blood products.
14. Maternal death or serious disability associated with labor or delivery in a low risk pregnancy while being cared for in a healthcare facility. Includes events that occur within 42 days post-delivery.

Adverse Health Events (continued)
15. Patient death or serious disability associated with hypoglycemia, the onset of which occurs while the patient is being cared for in a healthcare facility.
16. Death or serious disability (kernicterus) associated with failure to identify and treat hyperbilirubinemia neonates.
17. Stage 3 or 4 pressure ulcers acquired after admission to a healthcare facility.
18. Patient death or serious disability due to spinal manipulative therapy.
19. Patient death or serious disability associated with electric shock or elective cardioversion while being cared for in a healthcare facility.
20. Any incident in which a line designed for oxygen or other gas to be delivered to a patient contains the wrong gas or is contaminated by toxic substances.
21. Patient death or serious disability associated with a burn incurred from any source while being cared for in a healthcare facility.
22. Patient death or serious disability associated with a fall while being cared for in a healthcare facility.
23. Patient death or serious disability associated with the use of restraints or bedrails while being cared for in a healthcare facility.
24. Any instance of care ordered by or provided by someone impersonating a physician, nurse, pharmacist, or other licensed healthcare provider.
25. Abduction of a patient of any age.
26. Sexual assault on a patient within or on the grounds of a healthcare facility.
27. Death or significant injury of a patient or staff member resulting from a physical assault (i.e. battery) that occurs within or on the grounds of a healthcare facility.
28. Artificial insemination with the wrong donor sperm or egg.
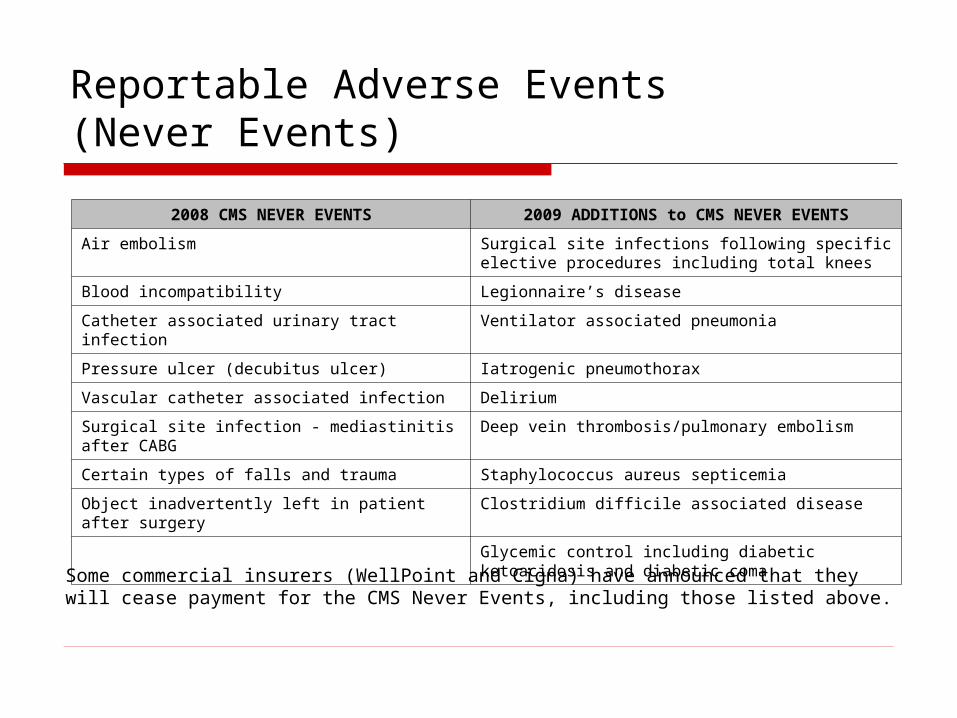
Reportable Adverse Events (Never Events)
2008 CMS NEVER EVENTS 2009 ADDITIONS to CMS NEVER EVENTS
Air embolism Surgical site infections following specific elective procedures including total knees
Blood incompatibility Legionnaire’s disease
Catheter associated urinary tract infection Ventilator associated pneumonia
Pressure ulcer (decubitus ulcer) Iatrogenic pneumothorax
Vascular catheter associated infection Delirium
Surgical site infection - mediastinitis after CABG
Deep vein thrombosis/pulmonary embolism
Certain types of falls and trauma Staphylococcus aureus septicemia
Object inadvertently left in patient after surgery
Clostridium difficile associated disease
Glycemic control including diabetic ketoacidosis and diabetic coma
Some commercial insurers (WellPoint and Cigna) have announced that they will cease payment for the CMS Never Events, including those listed above.

Reportable Adverse Events (Never Events)ASSESSMENT: Reportable Adverse of “Never” events reporting will require that processes be established to identify whether these events were present on admission. Critical Access Hospitals (CAH’s) are currently exempt from “present on admission” reporting. However, due to the adoption by the State of Washington of the 28 “never events” list and the anticipated impact of the Recovery Audit Contactor (RAC) surveys, critical access hospitals should be updating their systems to capture this data (conditions present on admission).
PRESENT ON ADMISSION INFORMATION: Beginning in 2007, prospective payment system hospitals were required to submit a “present on admission” indicator for every inpatient diagnosis. “Present on Admission” is defined as:
• Any condition present at the time of the physician order for inpatient admission
• Any condition that develops during an outpatient encounter (including Emergency Department, observation or outpatient surgery) and still present at time of inpatient admission.
“Present on Admission” applies to all inpatient diagnosis codes, both principal and all secondary diagnoses.
Improving Patient SafetyBackground & Legislation
Why Adverse Event Reporting An important goal--the reporting law drives
quality improvement in facilities as part of a broader statewide vision of creating patient safety
Adverse event reporting systems enhance both accountability and transparency
The true strength of the adverse event reporting system is the focus on learning, sharing information about root causes and best practices for prevention and increased awareness of about adverse events.
Improving Patient SafetyBackground & Legislation
27 States receive adverse event reports-26 mandatory & 1 voluntary
12 States and District of Columbia use NQF list of adverse events, or modified version
14 States use a state defined list
Source: National Academy for State Health Policy, 2007 Guide to State Adverse Event Reporting Systems/Download this publication at www.nashp.org/Files/shpsurveyreport_adverse2007.pdf

Improving Patient SafetyBackground & Legislation
70.56 RCW Adverse Event Reporting Became law on June 5, 2006 & amended in 2008 Quality Improvement Focus not Regulatory Definitions from NQF Serious Reportable Events Adverse Event Notification within 48 hours of
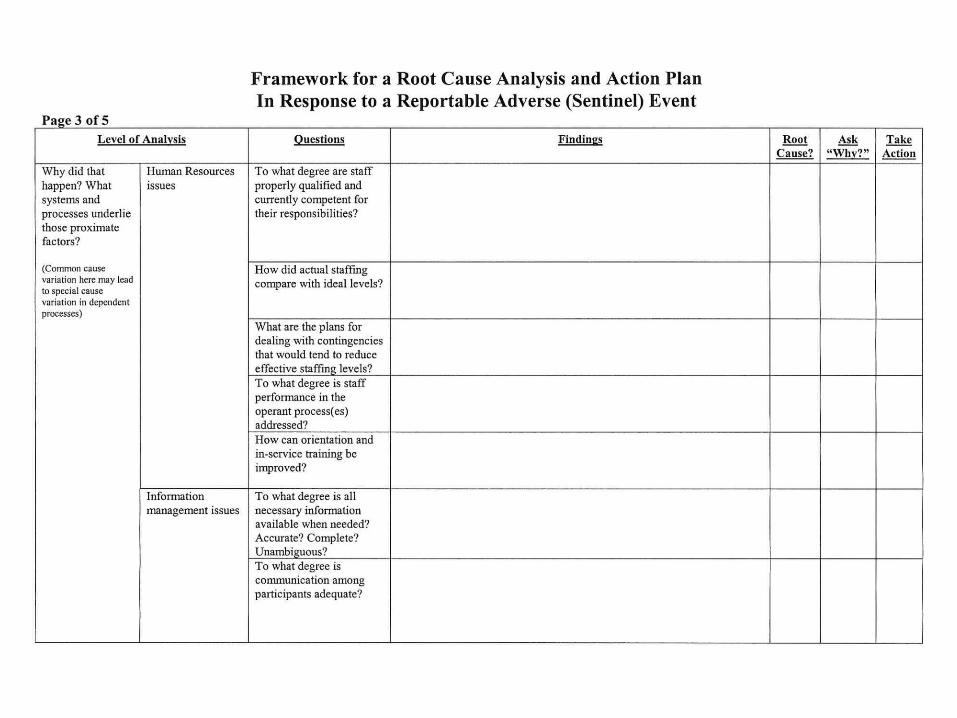
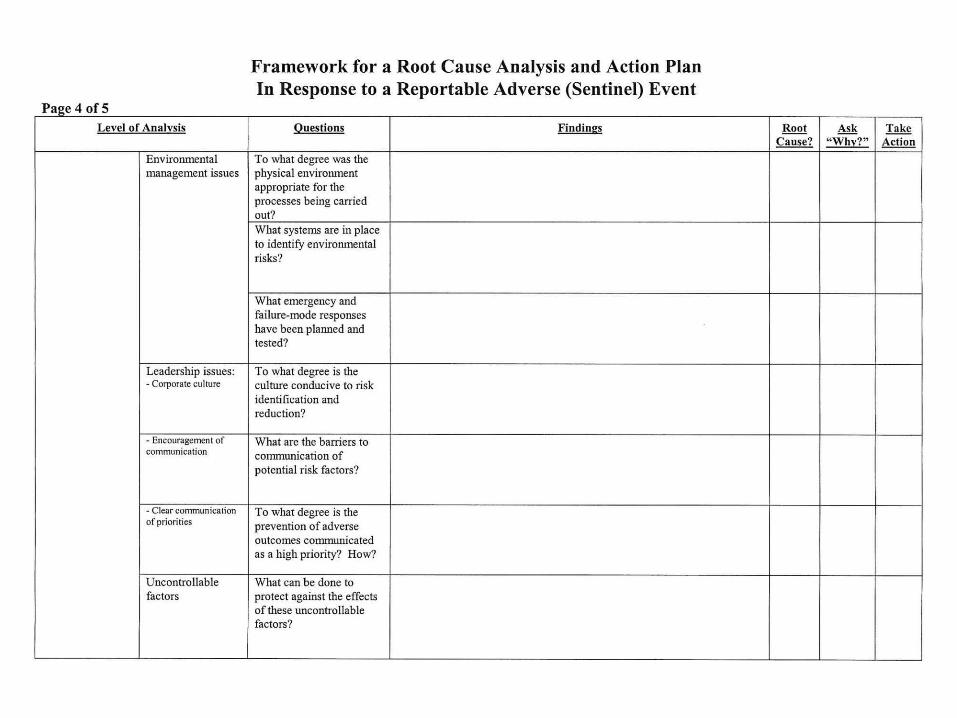
confirmation and may include contextual information Root Cause Analysis with Action Plan to DOH within
45 days. DOH provides review and consultation for RCA’s Public disclosure of adverse event notifications
permitted Report/RCA’s not subject to public disclosure
Improving Patient Safety:Background & Legislation
70.56 RCW Adverse Event ReportingDepartment of Health Role Receive & Investigate, where necessary,
adverse event notifications, root cause analyses, and corrective action plans and communicate the department’s conclusions to facilities
Consultation Visits initiated through RCA review or by request
Improving Patient Safety:Background & Legislation
70.56 RCW Adverse Event ReportingDepartment of Health Role Developed the Root Cause Analysis Evaluation Tool 1
PSAE Program—Review of 300+ RCA’s utilizing Root Cause Analysis Evaluation Tool 1
Reference: 1. Adapted from Joint Commission Sentinel Event Methodology and Maryland
Department of Health & Mental Hygiene, Office of Health Care Quality

Improving Patient Safety: General Findings from RCA Reviews
Definition for Root Cause Analysis: An analytic tool that can be used to perform a comprehensive, system based review of critical incidents and adverse health events.

Improving Patient Safety: General Findings from RCA Reviews
Goals of an RCA What happened? Why did it happen? What can be done to reduce the likelihood of
recurrence?

Improving Patient Safety: General Findings from RCA Reviews
RCA Models US Veteran Affairs National Center for
Patient Safety Joint Commission Sentinel Events Canadian Root Cause Analysis Framework Other Models OK with DOH Permission

Improving Patient Safety: General Findings from RCA Reviews
Root Cause Analysis Evaluation Tool 1
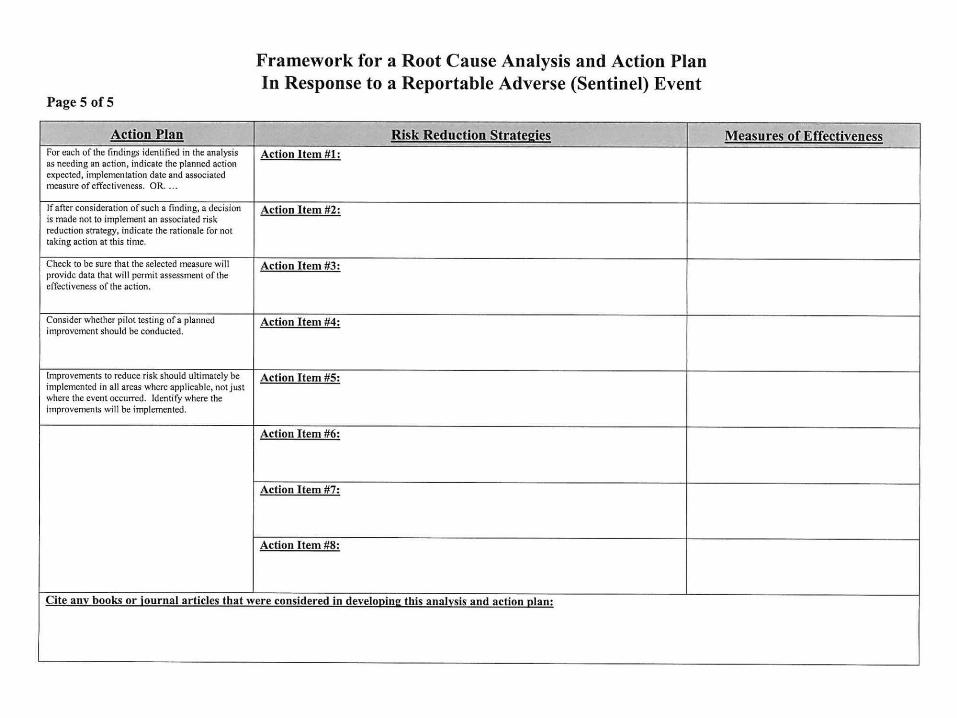
RCA Elements Determine that an adverse event
occurred Composition of RCA Team Conduct of RCA Develop an Action Plan Measure Effectiveness of Plan Relevant Literature

Improving Patient Safety: General Findings from RCA Reviews
Findings Composition of RCA Team
Team often developed by Nursing Department Lack representation from physicians, biomedical,
pharmacy, operations RCA teams provide an opportunity to create a
“culture of safety” Organization endorsements for RCA team
inconsistent

Improving Patient Safety: General Findings from RCA Reviews
Findings Conducting an RCA
Plans for what to review are inconsistent Review of medical records, policies, procedures, maintenance
logs, site inspections, staff interviews strengthen data collection
Short training session about how to conduct RCA for members can be helpful
Development of team member roles RCA’s can be accomplished in 3 meetings with good planning Review proximate factors at meeting Formulate specific causal statements
Improving Patient Safety: General Findings from RCA Reviews
Findings Outcome Measures
Improvements & changes are successful when processes become routine or habit or new employees demonstrate proper procedure after orientation
Communication plans are not always developed for internal and external release
Data analysis plan often unspecified Plans to include these findings in
administrative rounds or 24 hour reports reinforces “culture of safety”