improving outcome for musculoskeletal tumours in a developing country
TRANSCRIPT

IMPROVING OUTCOME FOR MUSCULOSKELETAL TUMOURS:
The Journey So Far
SEYI IDOWU FWACS FMCS
Based on a presentation at the ISOLS/MSTS Conference in Orlando, Florida Oct 2015.
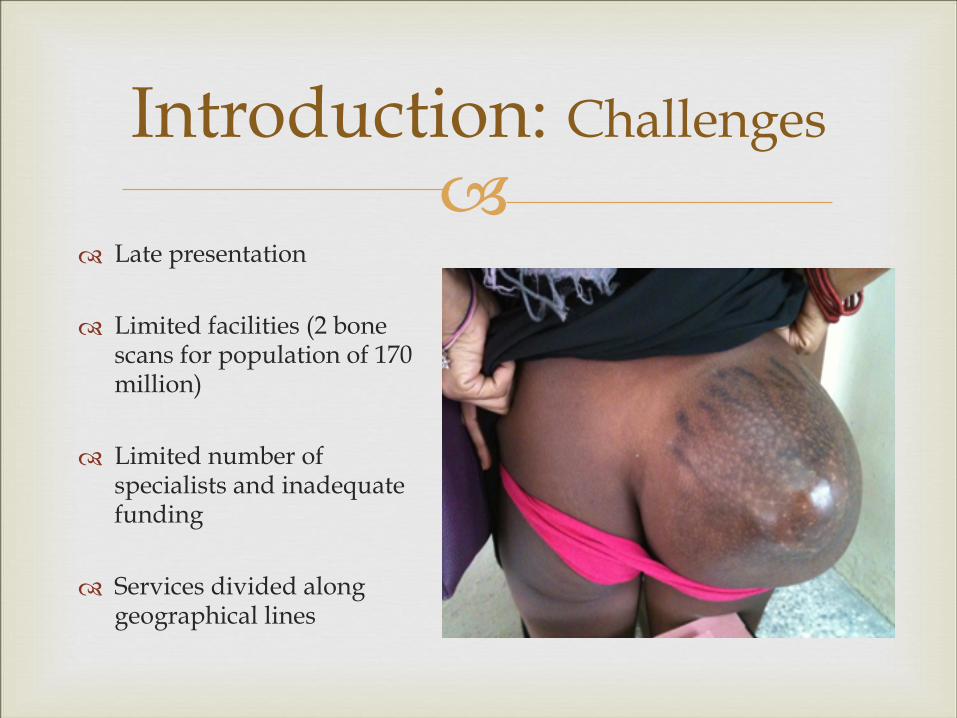
!Introduction: Challenges
" Late presentation
" Limited facilities (2 bone scans for population of 170 million)
" Limited number of specialists and inadequate funding
" Services divided along geographical lines

!" Coastal city along west
Africa Coast
" Most populous city in Africa
" 17 million people (10% of Nigerian population)
" No dedicated sarcoma MDT prior to 2012
Introduction - Lagos

LAMON
LAgos Muscoskeletal Oncology Network A model for Cancer Care in
Resource Poor Countries

LAMON

!AIMS OF LAMON
" Improve the care pathway for patients with sarcoma
" Improve efficient use of scarce resources
" Encourage adherence as much as possible to published national and international guidelines
" Decisions for holistic care plan – diagnosis, radiotherapy, chemotherapy, surgery and timing of interventions

!" 212 patients reviewed in 1st 30 months
"Definitive histological diagnosis in 192 patients (91%)
"Age range: 3 – 95 years
"Tumour Locations: ! Extremity 82% Central: 18%
LAMON" Diagnosis
! Osteosarcoma – 22%; ! Giant cell tumour – 13% ! Soft tissue sarcoma – 11% ! Metastatic bone disease – 8% ! Other benign lesions
" Limb preservation rate 67%
" Local recurrence rate 8.5%
!
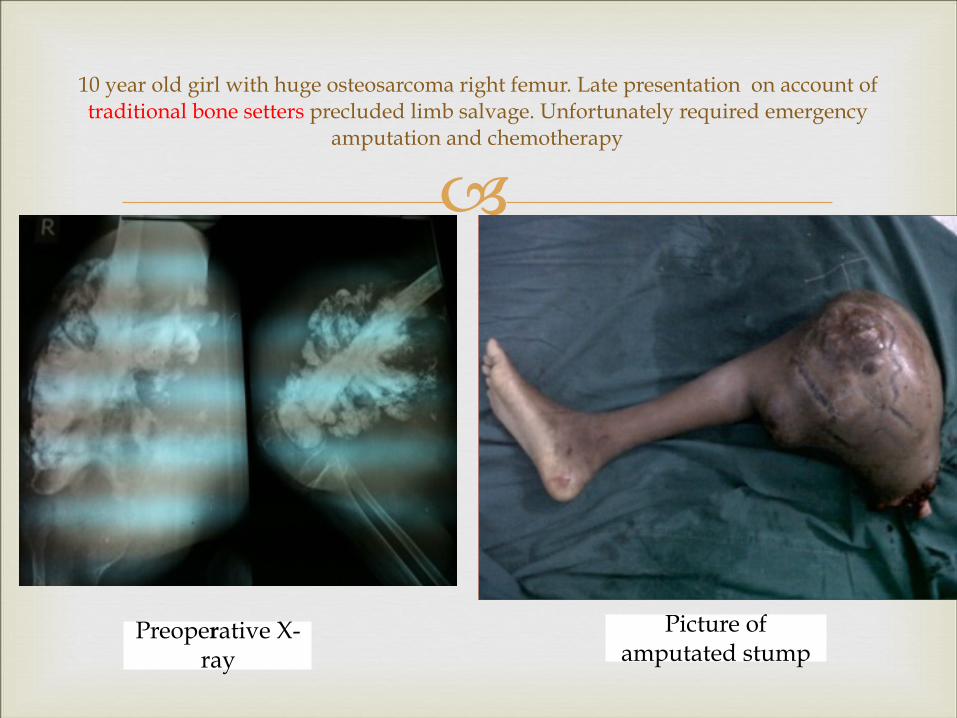
10 year old girl with huge osteosarcoma right femur. Late presentation on account of traditional bone setters precluded limb salvage. Unfortunately required emergency
amputation and chemotherapy
Picture of amputated stump
Preoperative X-ray

!
30 yr old lady with recurrent GCT distal femur



!ID AGE IN YRS SEX INDICATIONS SYMPTOMS
INTERVAL IN MONTHS
RESECTION LENGTH IN CM
PROSTHESIS COMPLICATIONS MSTS SCORE IN %
1 82 F non union hip # with osteolysis
5 12 RESTOR PFEPR none 60
2 54 F failed DHS for hip # 24 18 RESTOR PFEPR SSI 96
3 58 M pathological # hip secondary to C.A.P
4 14 RESTOR PFEPR none 70
4 68 M fibrous dysplasia 3 14 RESTOR PFEPR none 96
Proximal Femoral Endoprosthetic Replacement

!ID AGE YRS SEX INDICATION SYMPTOMS INTERVAL IN MONTHS
RESECTION LENGTH IN CM
TYPE OF PROSTHESIS
COMPLICATIONS
MSTS SCORE IN %
1 28 F GCT 60 17 RESTOR DFEPR SSI 86
2 32 M GCT TENDON SHEATH
6 15 IMPOL DFEPR NONE 93
3 4 M PLASMACYTOMA
84 24 IMPOL DFEPR POPLITEAL ARTERY THROMBOSIS . WOUND DEHISCENCE. A/K AMPUTATION
24
4 55 M NON UNION DISTAL FEMORAL # WITH BONE LOSS
18 20 RESTOR DFEPR DVT 86
Distal Femoral Endoprosthetic Replacement

!ID AGE YRS SEX INDICATION SYMPTOMS INTERVAL IN MONTHS
RESECTION LENGTH IN CM
TYPE OF PROSTHESIS
COMPLICATIONS
MSTS SCORE IN %
1 63 M INFECTED TKR 14 12 RESTOR PTEPR NONE 93
2 21 M OSTEOSARCOMA
6 24 RESTOR PTEPR LOOSENING OF THE HINGE MECHANISM
86
Proximal Tibial Endoprosthetic Replacement

!ONGOING CHALLENGES

!
" Rising life expectancy of cancer patients
" Main factors include; 1. primary histology 2. potential instability 3. neural compression
" Multidsciplinary collaboration is required
" Median survival of patients with spinal metastatic disease is 10 months.
" The morbidity of spinal metastatic disease is important, especially in patients with paralysis and/or bowel and bladder involvement.
" Cord compression is normally seen as preterminal event.
" Median survival at that stage is about 3 months.
!
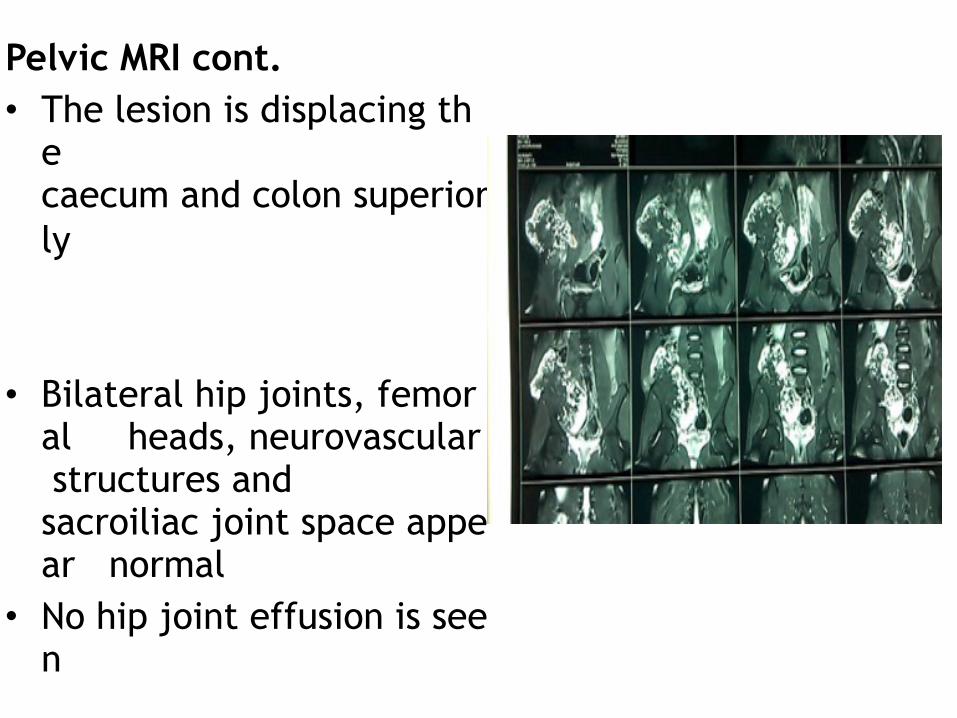
Pelvic MRI cont.
• The lesion is displacing the caecum and colon superior
ly
• Bilateral hip joints, femor
al heads, neurovascular
structures and
sacroiliac joint space appe
ar normal
• No hip joint effusion is see
n

!
• Pelvic MRI • Large lobulated expansile
lesion arising from the anter
ior cortex of the right iliac bone with extensive periosteal reaction and excessive bone formation
• It appears heterogenously
hyperintense on T2 and hypointense on T1 images
• It measures approximately 17.5x 9.0 x 17.4 cm..
• It invades the surrounding iliacus muscle and displacin
g it anteriorly

!" Establish a formal referral pathway: Grants
applications!!!
" Funding for MDT: NGO ——MONSUF
" Funding for investigations and specialist care
" Funding for specialist training
Ongoing challenges

!"The network resulted in improvement in diagnosis,
limb salvage rate and follow up care for musculoskeletal tumours and other conditions.
" Perhaps, with appropriate social and corporate support, communal tumour boards like LAMON may translate into model for multidisciplinary cancer care in resource poor countries
DISCUSSION