improving medicines safety at transfers of care … · improving medicines safety at transfers ......
TRANSCRIPT

Improving medicines safety at transfers
of care across Greater Manchester
Improving Medicines Safety and Transfer of Care: A Quality Improvement Programme in Greater Manchester
Jane Macdonald
Director of Nursing and Improvement
Greater Manchester Academic Health Science Network (GM ASHN)

Click to edit Master title style
This programme has been commissioned by the Greater Manchester Academic Health Science Network (GM AHSN) and is delivered in partnership by Haelo, an innovation and improvement science centre based in Salford, Manchester
Declaration of interest
Transfers of Care: A Quality Improvement programme
How to approach improve medicines safety at transfers of care for vulnerable patients

30/05/2017 4
GM AHSN Membership
AHSN footprint
4 Universitie
s
1 Ambulance Service

Click to edit Master title style
Achieving safe medicines management during transfer of care was identified as a healthcare priority that affects many patients
Our solution: To create a collaborative quality improvement programme across multiple healthcare systems, teams and individuals in Greater Manchester
Introduction and objectives
Today’s presentation will:
• Share our I.H.I. Break Through Series Collaborative model and show how a using a ‘plan-do-study-act’ approach helped build effective cross-organisational teams and projects
• Report the outcomes of the programme against our ambition to achieve 95% ‘defect-free’ medicines care
• Provide individual exemplars of success from project teams and share what we learned

30/05/2017 6
Receiving safe medicines on transfer of care should be every patient’s expectation…

30/05/2017 7
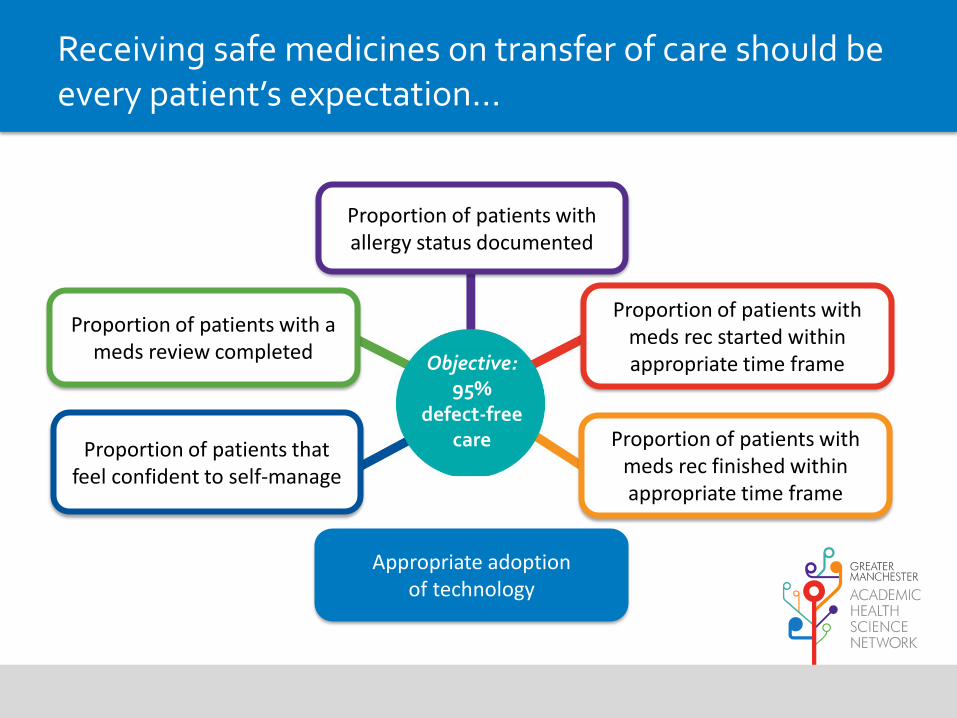
Receiving safe medicines on transfer of care should be every patient’s expectation…
Objective: 95%
defect-free care

30/05/2017 8
Receiving safe medicines on transfer of care should be every patient’s expectation…
Baseline: 26.6%
30/05/2017 9
Receiving safe medicines on transfer of care should be every patient’s expectation…
Baseline: 26.6%
Objective: 95%
defect-free care
Proportion of patients with allergy status documented
Proportion of patients with meds rec started within appropriate time frame
Proportion of patients with meds rec finished within appropriate time frame
Proportion of patients with a meds review completed
Proportion of patients that feel confident to self-manage
Appropriate adoption of technology

30/05/2017 10
Using the Breakthrough Series (BTS) collaborative model

30/05/2017 11
Using the Breakthrough Series (BTS) collaborative model
9/14 Health economies participated
Teams from Manchester Mental
Health and Social Care and HMP Manchester
reviewed medicines reconciliation for newly
transferred patients
Wrightington, Wigan and Leigh pharmacy team improved documentation and effectively used patient / public involvement to improve patient discharge
Salford Royal collaborated with Heartly Green Care
Home to improve transfer from
acute hospital to intermediate care homes

30/05/2017 12
Using the Breakthrough Series (BTS) collaborative model
Page 30 of 32
Posters produced by More than Minutes at Learning Session 2 of each of the
participating teams
East Lancashire (refertopharmacy) and began to share learning with one another through
knowledge exchange sessions.
Resources from the second Learning Session, including a film summary of the event are
available online.
Following the event teams were encouraged to undertake rapid PDSA cycles linked to the
driver diagram, building on change ideas developed in Learning Session 2. Teams were
requested to submit data and progress reports on a monthly basis.
At this stage in the project, the majority of teams utilised site visits as an opportunity to
receive coaching support to tackle issues affecting progress. Common issues were around
difficulties in collecting sufficient data and addressing the need to be fully documenting all
PDSA cycles. Some teams raised issues around losing key staff involved in the project
through various staff changes.

30/05/2017 13
Case Study 1: Salford team embedding medicines reconciliation in Intermediate Care
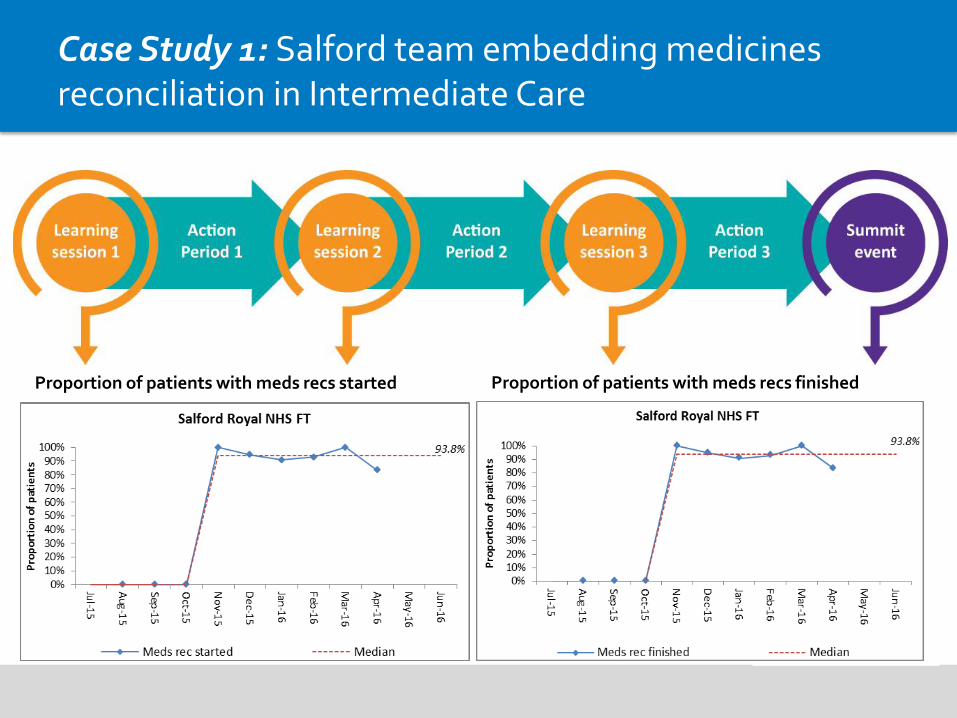
• The Salford team looked at how they could improve medicines processes for patients discharged to intermediate care
• An in-house pharmacy technician was introduced at a pilot intermediate care home
• It immediately impacted the number of patients who had medicine reconciliations within 72 hours: from 0% to 93.8%
• The introduction of an onsite medicines stock cupboard reduced omitted or delayed doses
• A business case has now been approved to introduce pharmacy technicians to all intermediate care units in Salford
30/05/2017 14
Case Study 1: Salford team embedding medicines reconciliation in Intermediate Care
Proportion of patients with meds recs started Proportion of patients with meds recs finished
30/05/2017 15
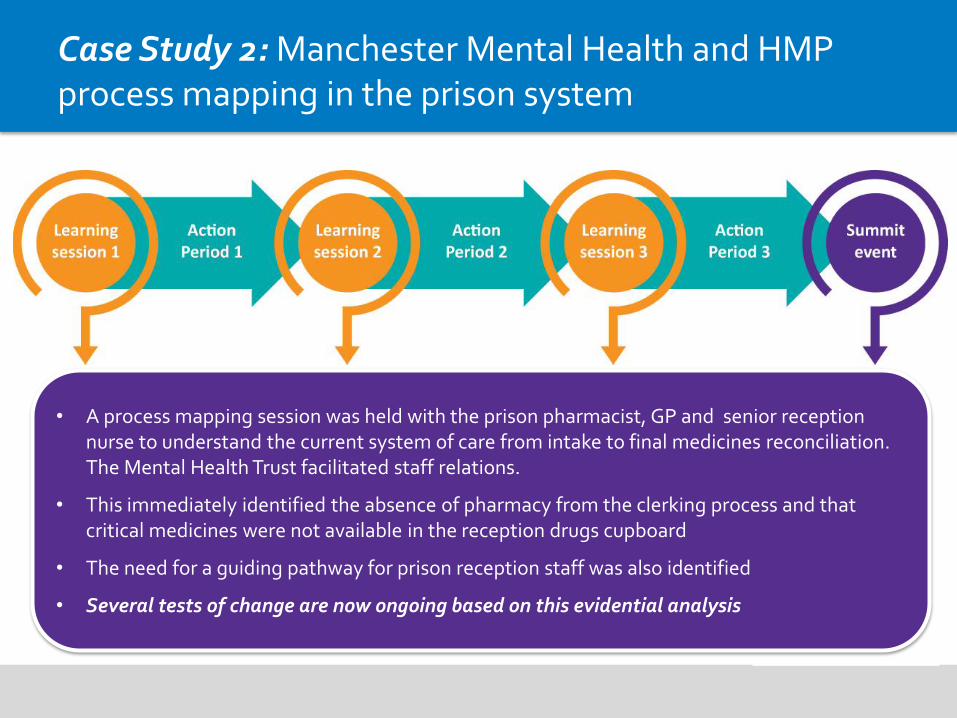
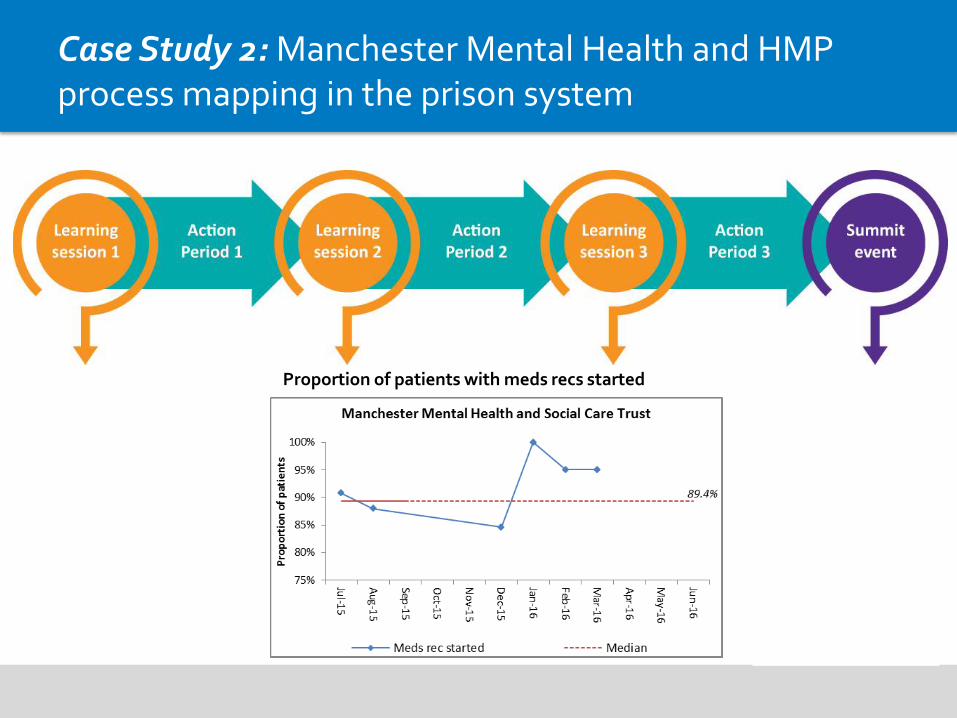
Case Study 2: Manchester Mental Health and HMP process mapping in the prison system
• A process mapping session was held with the prison pharmacist, GP and senior reception nurse to understand the current system of care from intake to final medicines reconciliation. The Mental Health Trust facilitated staff relations.
• This immediately identified the absence of pharmacy from the clerking process and that critical medicines were not available in the reception drugs cupboard
• The need for a guiding pathway for prison reception staff was also identified
• Several tests of change are now ongoing based on this evidential analysis
30/05/2017 16
Case Study 2: Manchester Mental Health and HMP process mapping in the prison system
Proportion of patients with meds recs started

30/05/2017 17
Case Study 3: Wrightington, Wigan and Leigh pharmacy team improving discharge communications
• The pharmacy team identified variations in the quality of patient communications in different healthcare settings
• The objective was to make patient medication information of equal quality at discharge as it is at admission
• A group of patient representatives, district nurses and CCG pharmacists collaborated to develop seven key tests of change
• The most effective solution was a discharge summary sheet that is sent to the community pharmacy to support all discharge prescriptions

30/05/2017 18
Case Study 3: Wrightington, Wigan and Leigh pharmacy team improving discharge communications
Proportion of patients confident to self-manage

30/05/2017 19
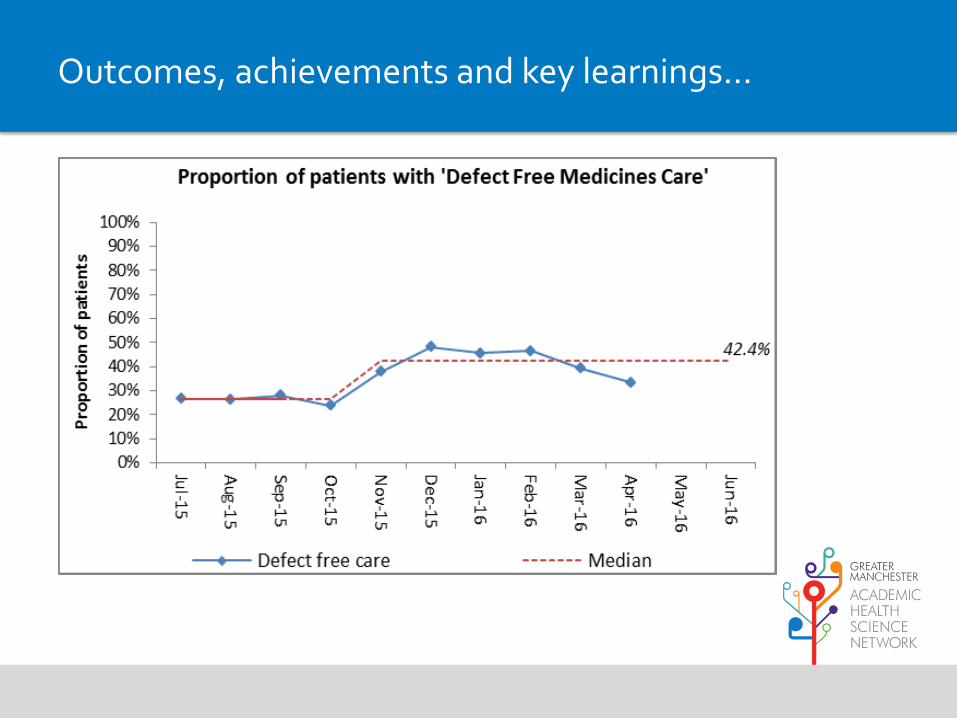
Outcomes, achievements and key learnings…
Objective: 95%
defect-free care

30/05/2017 20
Outcomes, achievements and key learnings…
Baseline: 26.6%

30/05/2017 21
Outcomes, achievements and key learnings…
One-year outcome:
42.4%

30/05/2017 22
Outcomes, achievements and key learnings…
58% improvement
30/05/2017 23
Outcomes, achievements and key learnings…

30/05/2017 24
Outcomes, achievements and key learnings…

30/05/2017 25
Outcomes, achievements and key learnings…
The project established critical relationships across
health economies
We gained a better, evidential understanding of systems and
opportunities for improvement
Participants reported personal benefits for their training and
development
Patient / public involvement kept us asking the question
“Is this good enough?”
More teams would have liked to engage executive level
sponsors / chief pharmacists
Data collection and outcomes measurement was a key
challenge

30/05/2017 26
Outcomes, achievements and key learnings…

30/05/2017 27
Outcomes, achievements and key learnings…
Did we make Manchester the safest place to take medicines..?
..no, but we did make it safer

Outcomes from its first 18 months

Why refer to Community pharmacy?
• New Medicine Service: ↑10% in medicines adherence
• Discharge Medication Review: every £1 spent saves £3
• Patient Safety: sharing the right information when it matters
↓Waste
↓ED attendance
↓(re)admissions
↑Safety

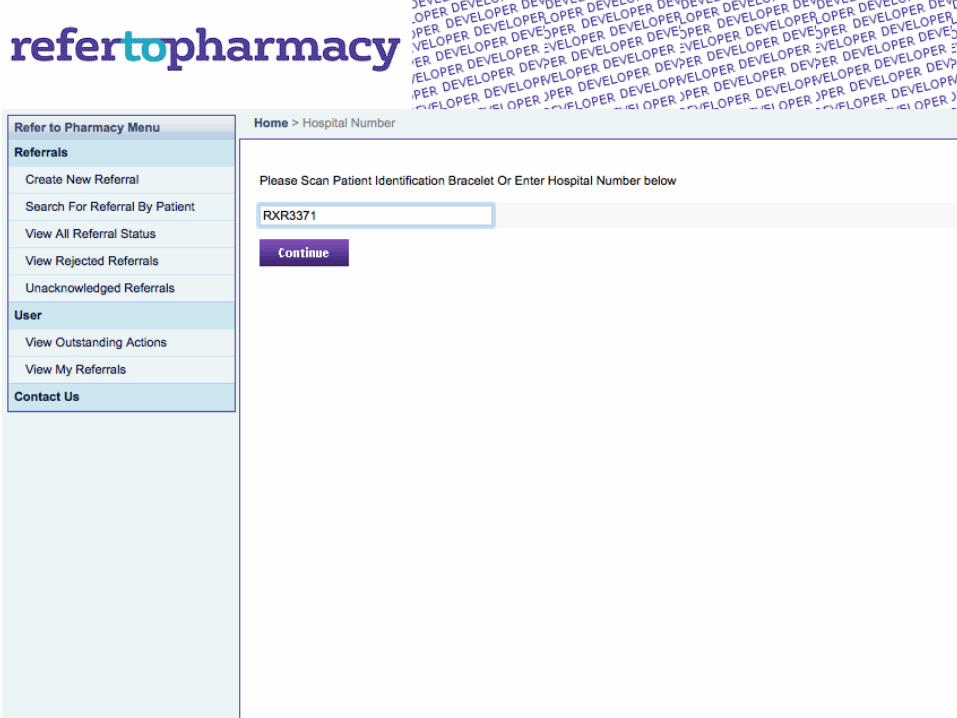
World’s first fully integrated pharmacy
referral system:
• Fast
• E-discharge letter attachment
• Secure
• Auditable
• Two-way communication
• Adaptable

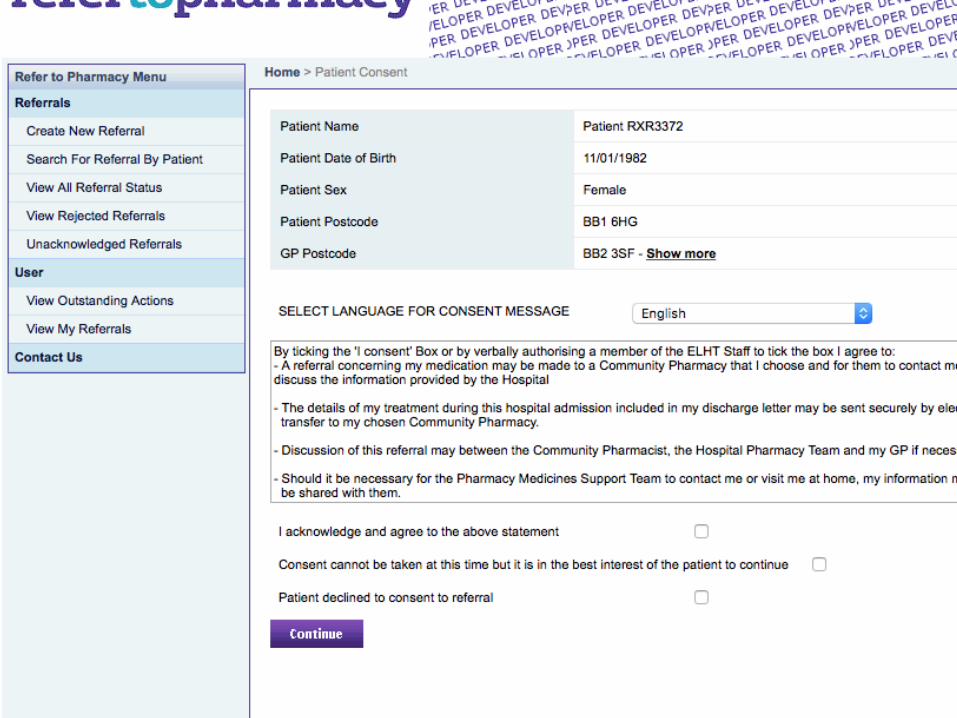
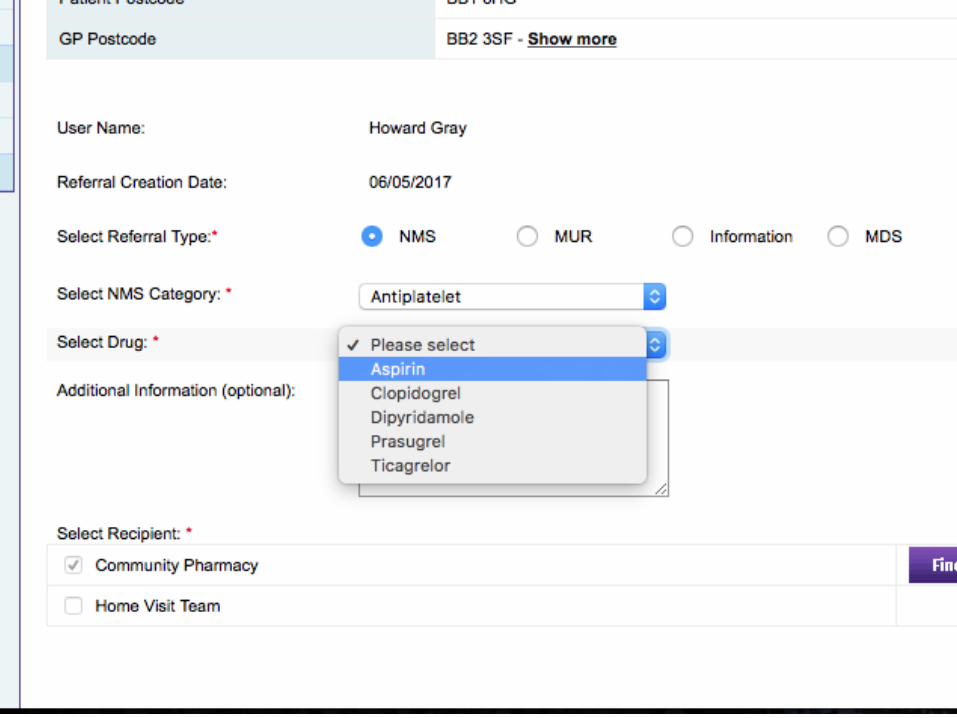
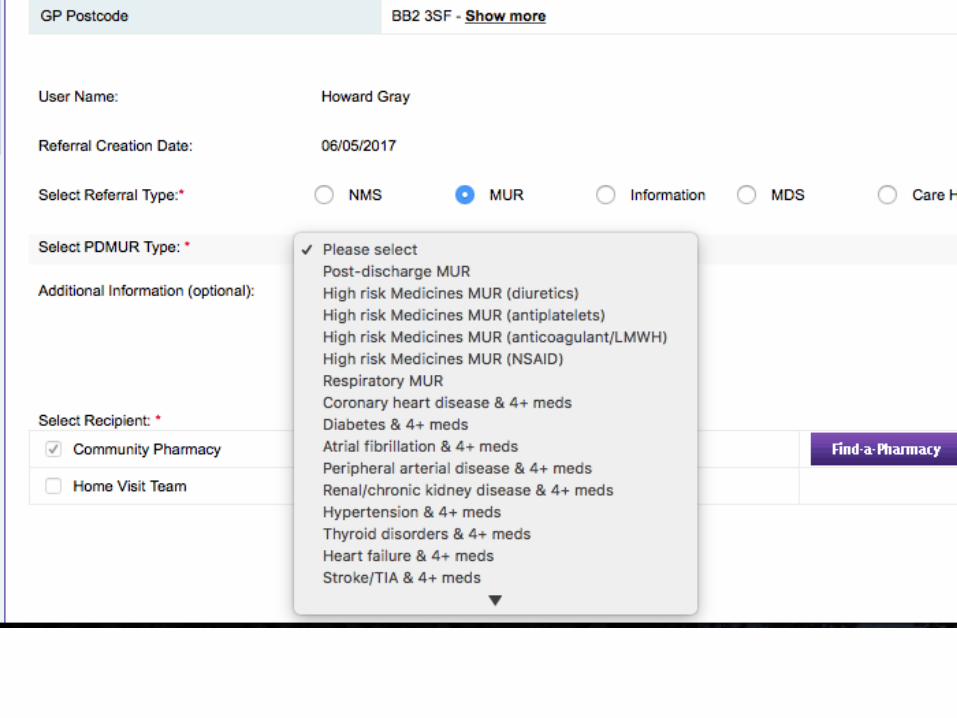
How it works on hospital wards
Every Eligible Patient: Referred
• Consultation-referral – NMS & MURs
• Information-referral – MDS, Care Home, Information
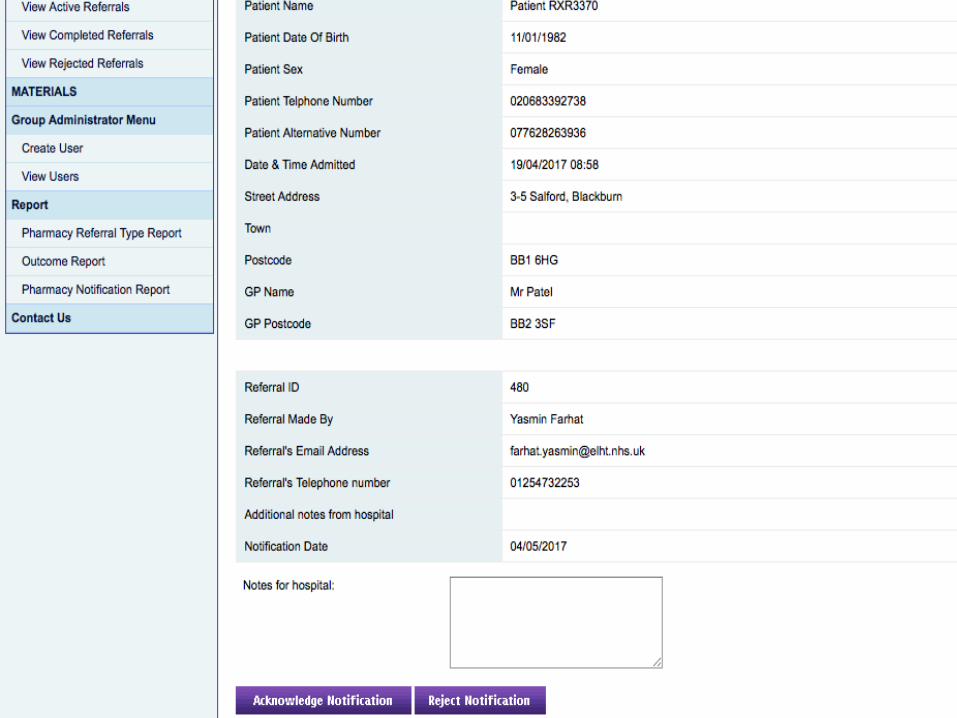
• Hospital Admission Notification – when appropriate
• Home Visit referral – Domiciliary Medicines Support Teams

Patient engagement film
www.elht.nhs.uk/refer

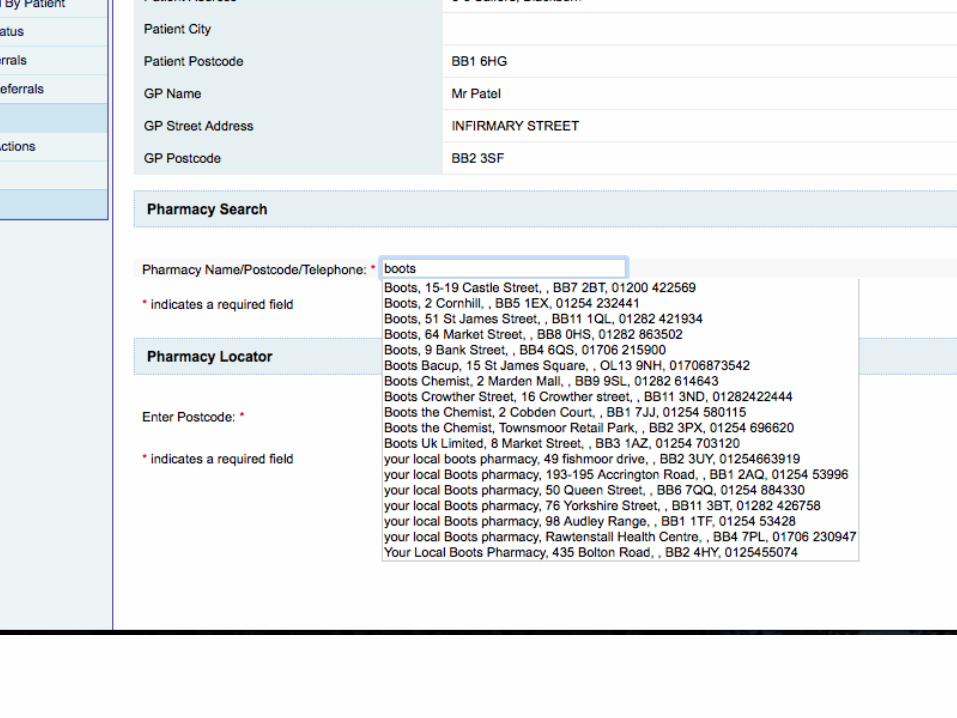
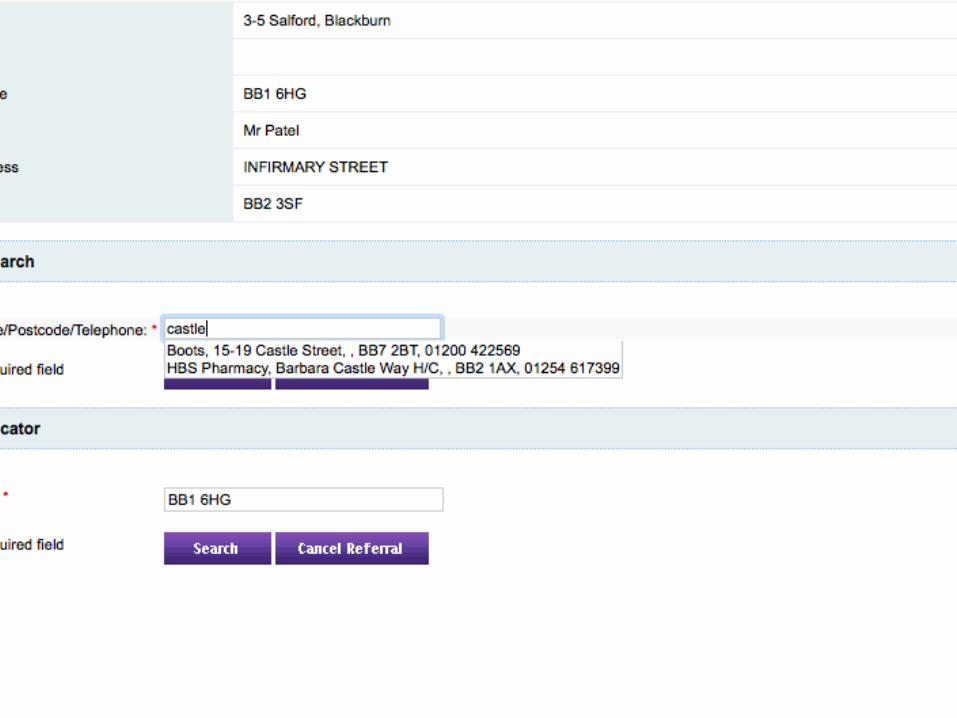
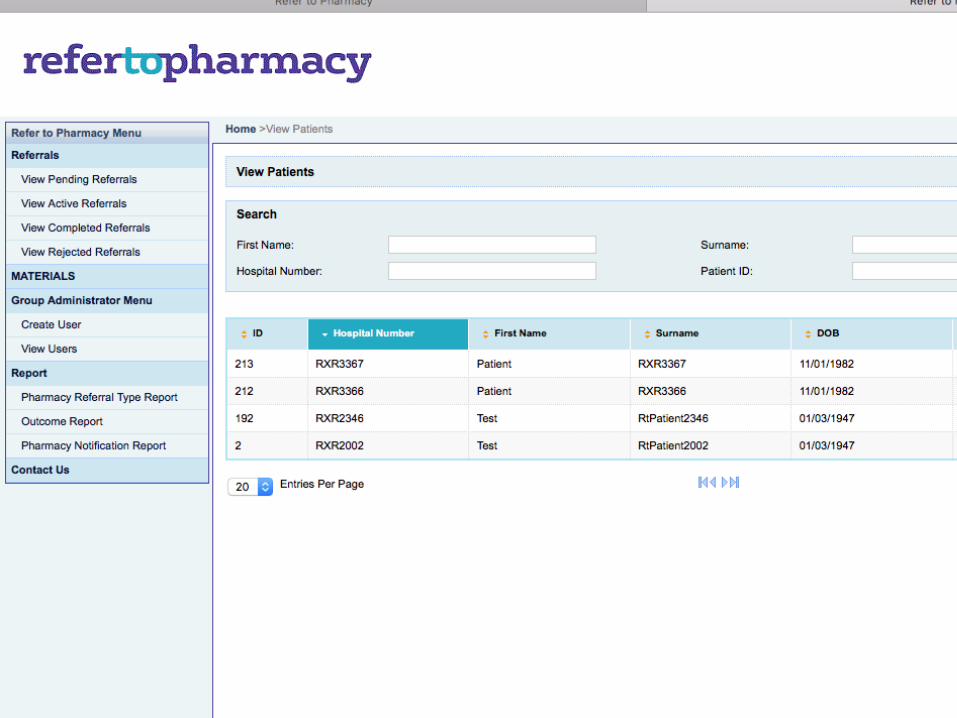
How it works in Community Pharmacy
Every Referred Patient: Accepted • Intuitive to use
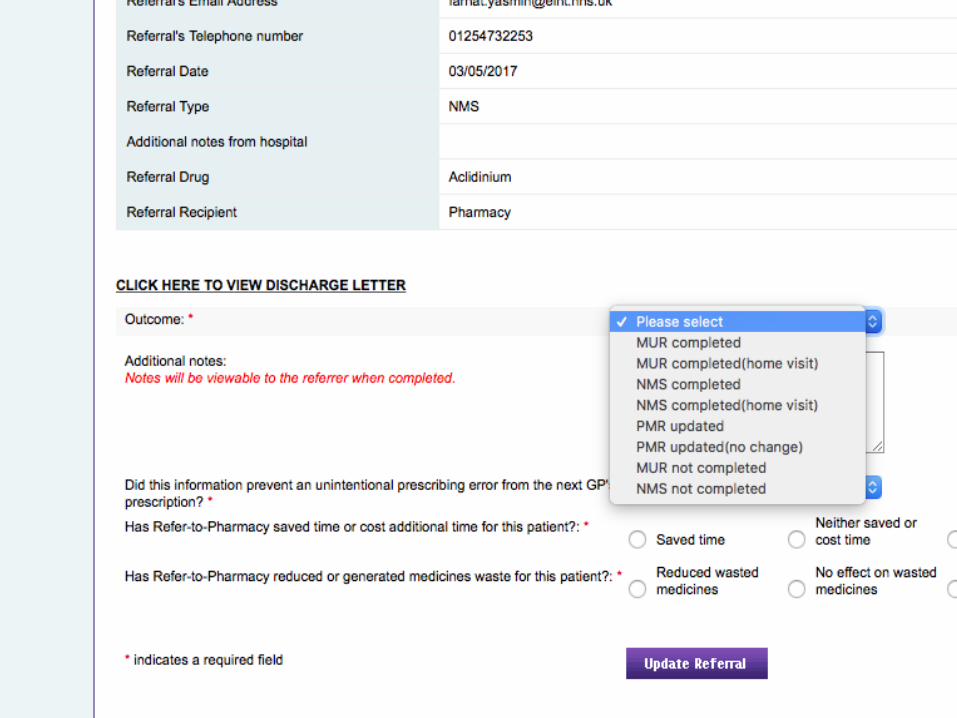
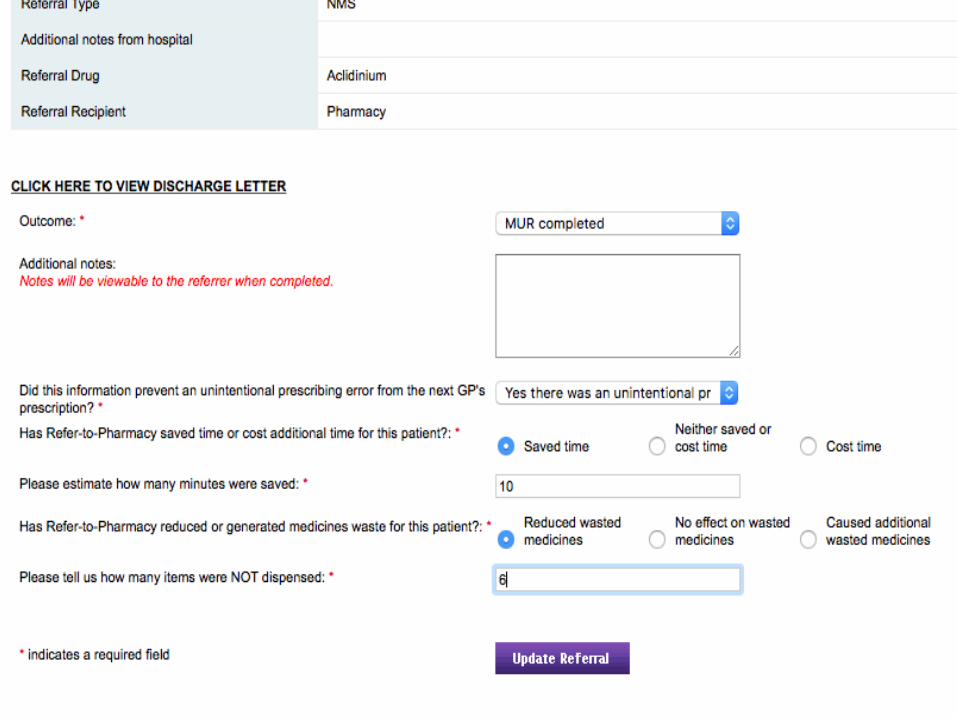
• Discharge letter reviewed
• Outcomes captured

Demonstration











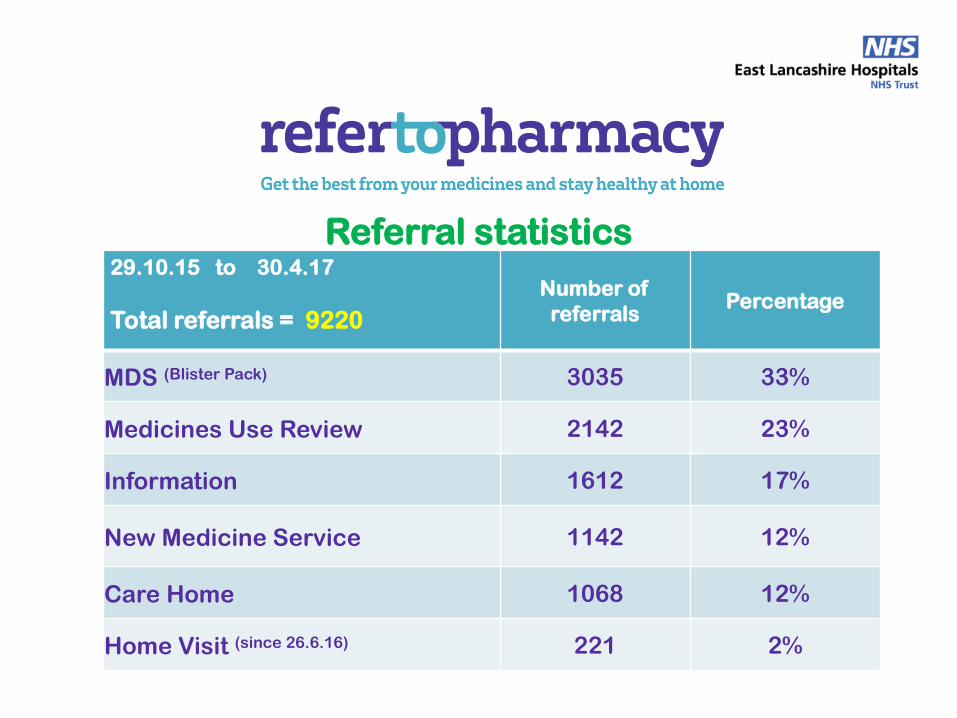
Referral statistics 29.10.15 to 30.4.17
Total referrals = 9220
Number of
referrals Percentage
MDS (Blister Pack) 3035 33%
Medicines Use Review 2142 23%
Information 1612 17%
New Medicine Service 1142 12%
Care Home 1068 12%
Home Visit (since 26.6.16) 221 2%

Referrals Number
Saved Dispensing Time 64 3954 minutes 65 hours (net)
Reduced Medicines Waste average item value £9.18 49 200 items (net)
= £1,836
Unintentional prescribing errors rectified 46
GP intentionally did not affect changes 9
Outcome statistics MARCH - APRIL 2017
•

An early SIGNAL: % readmissions for the same diagnosis from medical wards at 28 days
139 fewer people readmitted
in this 10 month period Lord Carter’s report: £3,500/patient episode
Period N
January – October 2015 590
January – October 2016 451

Making it work, aiding spread • Community Pharmacy support – CPPE
• Royal Pharmaceutical Society support
• R2P monthly newsletter
• Service evaluation: Manchester University

Multi-award winning

• Ward pharmacist works on same ward throughout working day
• Participates in Consultant-led ward round
• Greater patient contact: ↑ medicines adherence
• Every eligible patent referred to community pharmacist
Dedicated Ward Pharmacy

• Pharmacy technician time on ward increased
• Completes medicines reconciliation on ALL patients
• Prepares medicines sections of electronic discharge letter
• Ensures all medicines available before discharge
Dedicated Ward Pharmacy

• 5% increase in discharges by midday
• 18% increase in discharges by 5pm
• 16% decrease in discharges after 5pm
• Late finishes from pharmacy team virtually eliminated
• Dispensed items getting back to wards sooner
Dedicated Ward Pharmacy: Improved discharge times
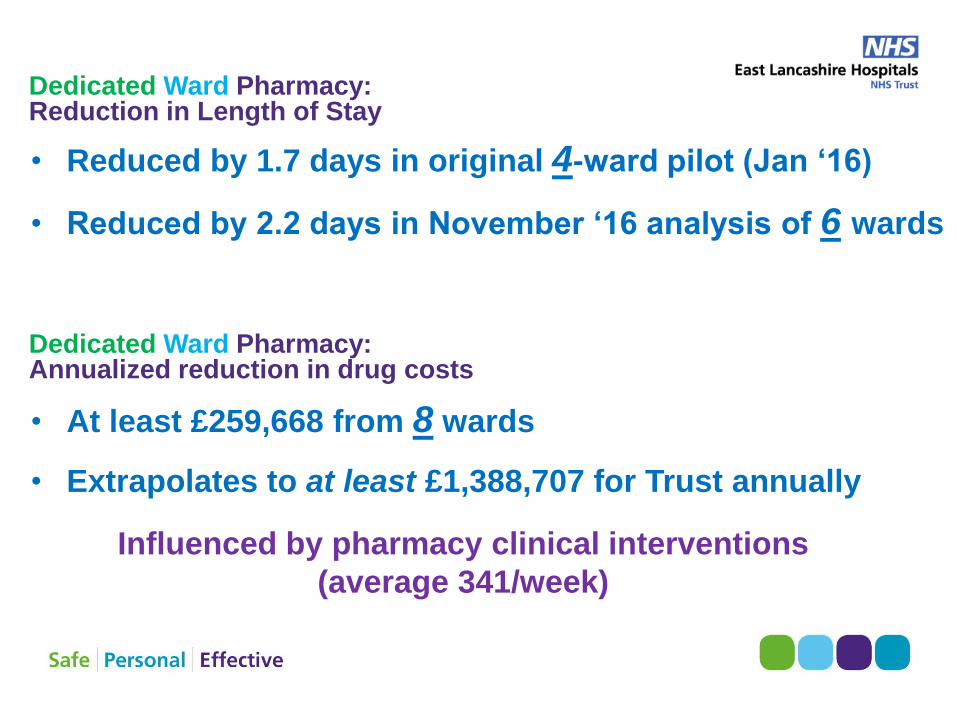
• Reduced by 1.7 days in original 4-ward pilot (Jan ‘16)
• Reduced by 2.2 days in November ‘16 analysis of 6 wards
Influenced by pharmacy clinical interventions
(average 341/week)
Dedicated Ward Pharmacy: Reduction in Length of Stay
• At least £259,668 from 8 wards
• Extrapolates to at least £1,388,707 for Trust annually
Dedicated Ward Pharmacy: Annualized reduction in drug costs
Dedicated Ward Pharmacy
Spreading good practice
