importance of trace elements in public health
TRANSCRIPT

Trace elements
DR. BHUSHAN KAMBLE
MODERATOR: DR. ANITA KHOKHAR
PROFESSOR,
DEPT. OF COMMUNITY MEDICINE,
VMMC & SJH

Outline of presentation
Definitions
Classification
Various trace elements
Body content
Requirement
Sources
Functions
Deficiency/ Excess
Control
Iodine
Iron
Zinc
Selenium
Copper
Molybdenum
Chromium
Manganese
Flourine
Nickel
Boron
Definitions
Element: An element is a chemical substance that is made up of a
particular kind of atoms and can not be broken down or
transformed by a chemical reaction into a different element
Trace element: Those elements which occur or function in living
tissues in concentrations most conveniently expressed in µg/l
Trace elements in human nutrition, WHO, 1973
Arbitrarily, the term "trace" has been applied to concentrations of
element not exceeding 250 µg per g of extracellular matrix.
Trace elements in human nutrition and health, WHO, 1996

Trace element*: A naturally occurring, homogeneous, inorganic
substance required in humans in amounts less than 100 mg/day
Bioavailability of minerals are low in vegetarian diet.
Excess amounts are injurious to health
*Department of clinical nutrition, university of Illinois at chicago
Classification (WHO, 1996)
Essential trace elements
Iodine, Zinc, Selenium, Copper, Molybdenum, Chromium,
Cobalt, Iron
Trace elements that are probably essential
Manganese, Nickel, Silicon, Boron, Vanadium
Potentially toxic elements with possible essential functions in low
doses
Fluoride, Lead, Cadmium, Mercury, Arsenic, Lithium, Tin,
Aluminium

Iodine

Iodine
Body content: 50mg Blood conc: 8-12mcg/dl
Sources of iodine
i. Seafood ii. Vegetables grown on iodine-rich soils
iii. Milk products iv. Eggs
v. Cereal grains vi. Legumes
vii. Green leafy vegetables
Water contains traces of iodine which may contribute to as much
as 10% of total iodine intake
Functions :
Iodine is an integral component of the thyroid hormones thyroxine
(T4) and tri-iodothyronine (T3).
In foetus and neonate normal protein metabolism in the CNS requires
iodine
Iodine
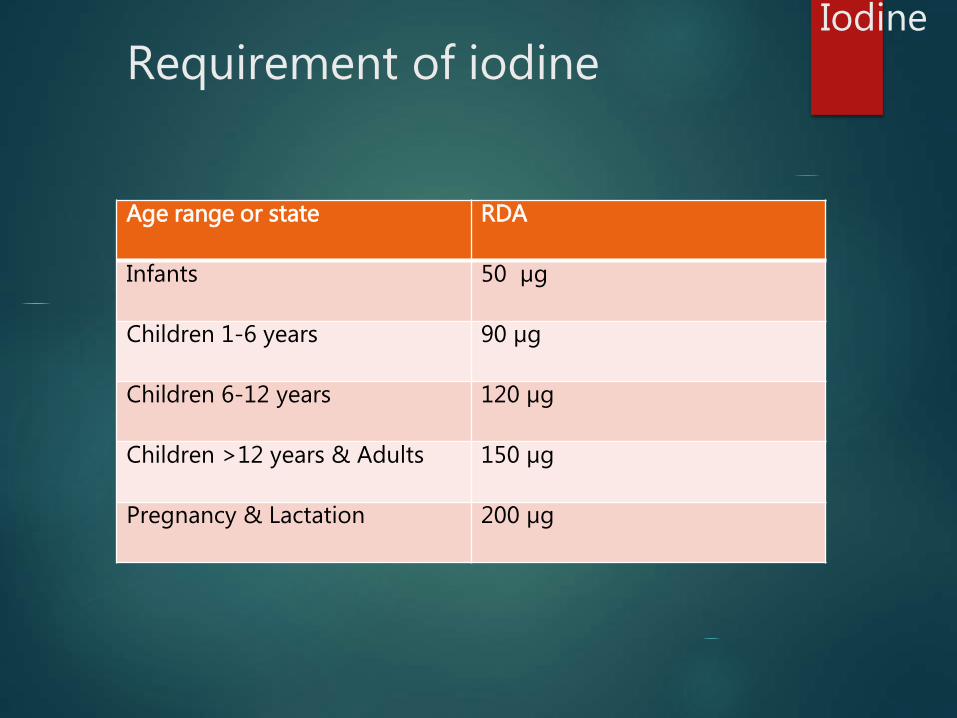
Age range or state RDA
Infants 50 µg
Children 1-6 years 90 µg
Children 6-12 years 120 µg
Children >12 years & Adults 150 µg
Pregnancy & Lactation 200 µg
Requirement of iodine

Iodine cont..
Absorption :
Dietary iodine absorbed from the small intestine.
Approximately 30 % used by the thyroid gland for the synthesis
of thyroxine hormone; rest excreted in urine
Goitrogens :
Vegetables of Brassica group (cabbage, cauliflower and radish)
contain goitrogens -thiocyanates and cynoglycosides.
Consumption of large quantities of these may lead to development
of goiter by making the iodine present in food unavailable to the
body.
Goitrogens inactivated by heating
Iodine

IODINE DEFICIENCY DISORDERS
Spectrum of disorders that result from deficiency of
iodine in body
IDD seen across all ages
Most profound effect of deficiency during periods of
rapid growth: fetus, neonate, infants, pregnancy
Iodine

IDD cont…Iodine

Assessment of status of IDD: Indicators
Goitre prevalence:
Seen in school children
Various levels of prevalence indicate the severity of IDD as a
public health problem
Prevalence of Goitre in School Age Children
Severity of IDD
5.0-19.9% Mild
20.0-29.9% Moderate
>=30% Severe
Iodine

Assessment of status of IDD: Indicators cont..
Urinary iodine levels:
School age children
Can be used as an indicator in 2 ways
Median urinary iodine levels to classify severity of IDD
population with median UI levels<100mcg: district endemic
Mean UI levels in mcg Severity of IDD
>= 300 TOXIC
299-200 EXCESSIVE: AT RISK OF TOXICITY
100-199 ADEQUATE
99-50 MILD DEFICIENCY
20-49 MODERATE DEFICIENCY
<20 SEVERE DEFICIENCY
Iodine
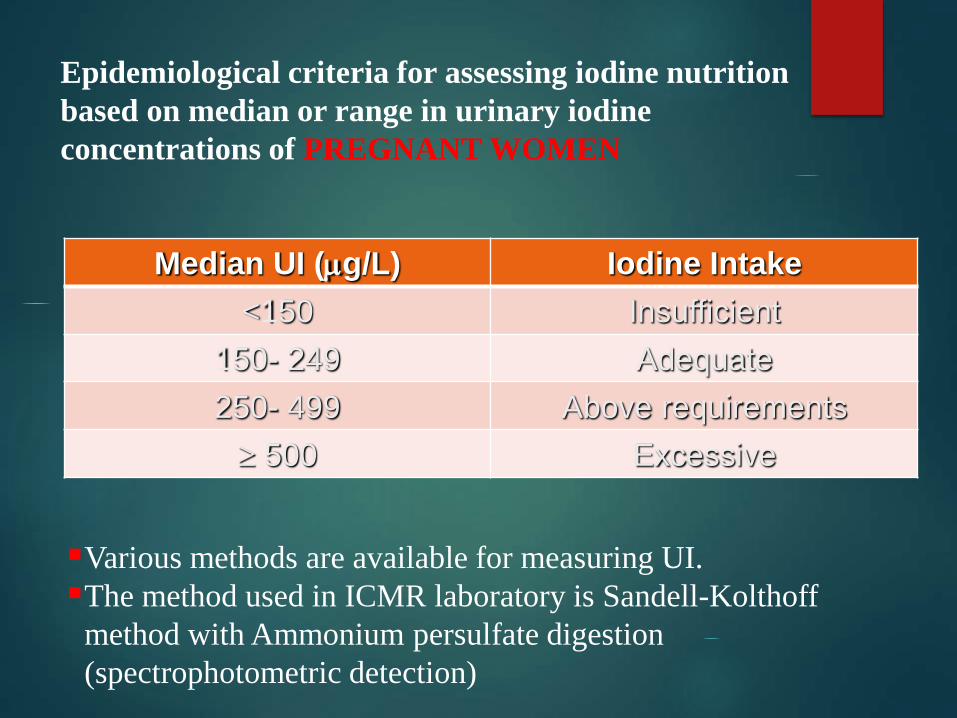
Epidemiological criteria for assessing iodine nutrition
based on median or range in urinary iodine
concentrations of PREGNANT WOMEN
Median UI (g/L) Iodine Intake
<150 Insufficient
150- 249 Adequate
250- 499 Above requirements
500 Excessive
Various methods are available for measuring UI.
The method used in ICMR laboratory is Sandell-Kolthoff
method with Ammonium persulfate digestion
(spectrophotometric detection)

Assessment of status of IDD: Indicators cont..
Thyroid gland volume:
School children
Measured as proportion of children having thyroid volume
>97 percentiles (2.9 to 4.1 ml)
Measured by USG
Proportion of School Age Children with thyroid volume> 97th precentile
Severity of IDD
5.0-19.9% Mild
20.0-29.9% Moderate
>=30% Severe
Iodine

Assessment of status of IDD: Indicators cont..
Serum thyroglobulin
Both children and adults
Thyroglobulin levels indicate the severity of IDD as follows
Median thyroglobulin ng/ml Severity of IDD
10-19.9 Mild
20-39.9 Moderate
>=40 Severe
Iodine

Assessment of status of IDD: Indicators cont..
Serum TSH
Neonates
Measured as proportion with serum TSH levels >5mU/l
Proportion of neonates with TSH > 5mU/l
Severity of IDD
10-19.9% MILD
20-39.9% MODERATE
>=40% SEVERE
Iodine
Other indicator used: salt iodine content
Salt iodine content
Recommended 15ppm at HH level
Can be measured by RAPID test kits: INEXPENSIVE KITS
Method: iodometric titration
100gm loose salt or full packet taken for analysis
50 samples to be collected per month per district
25 rural households
15 urban households
7 rural retailers
3 urban retailers
Iodine
CONTROL OF IDD
1956-1968: study conducted in Kangra district of Himachal
Pradesh to understand the magnitude of problem in India.
Rural community based study.
District divided into 3 zones: A B & C
Baseline survey in 1956
Salt distributed to three zones
Zone A : Salt + Potassium iodide
Zone B : Plain salt
Zone C : Salt + Potassium iodate
15 gms of salt/person/day
So as to ensure 200 µg of iodine/person/day
Iodine
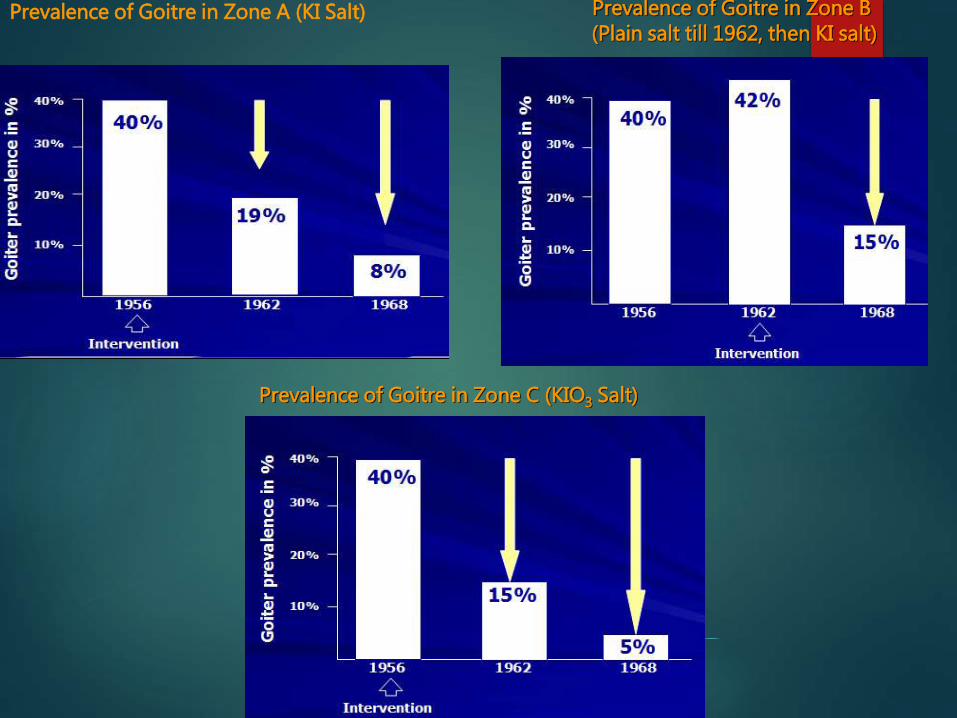
Prevalence of Goitre in Zone A (KI Salt) Prevalence of Goitre in Zone B(Plain salt till 1962, then KI salt)
Prevalence of Goitre in Zone C (KIO3 Salt)

Introduction of Iodized Salt in India – study
(1956-62)
40 40 4042
19
15
0
10
20
30
40
50
60
Plain salt Salt + Potassium iodide Salt + Potassium iodate
Goitre
pre
vale
nce (
%)
1956 1962
Iodine
CONCLUSION FROM KANGRA STUDY:
Iodine supplementation in the form of iodised salt on a
regular and continuous basis reduces goitre
prevalence
Iodine
In 1962, National Goitre Control Programme (NGCP) was
launched by GOI.
In 1986, the GOI adopted the policy of Universal Salt
Iodization
Iodine
National Goitre Control Programme(NGCP) 1962
1) Survey to identify endemic areas
2) Production & Supply of iodized salt to endemic areas
3) Impact assessment surveys after five years
24
Iodine

4 Phases of NGCP
Phase I 1962 – 1980
Phase II 1980 - 1990
Phase III 1990 - 2000
Phase IV 2000 onwards
IN 1992, renamed as National Iodine Deficiency Disorder
Control Programme( NIDDCP)
25
Iodine

PHASE I: NGCP
Iodized salt to Endemic districts Only
Interruptions in the supply of Iodized Salt
Surveys to find endemic districts
Iodine

Phase II: NGCP
1981-1982: pilot surveys: screening of neonates for hypothyroidism with filter paper techniques
Incidence of NH in Areas with Varying Goitre Prevalence
District Goitre Cretinism Incidence of NH Prevalence Prevalence (per thousand births)
___________________________________________Deoria 80% 3-5% 133Gorakhpur 70% 0-5% 85Gonda 60% 0-4% 75Delhi 29% Nil 6__________________________________________
Iodine
PHASE II: NGCP cont..
Such studies established the presence of iodine deficiency in Extra -
Himalayan Regions also.
1983: Ministry of Social Welfare sponsored project for
intensification of NGCP through Nutrition Foundation of India
1984-1986: multiple studies conducted by ICMR
EPIDEMIOLOGICAL SURVEY OF ENDEMIC GOITRE AND
ENDEMIC CRETINISM
14 Districts, 9 States
Pooled prevalence
Goitre: 21.1%
Cretinism: 0.7%
Iodine

Phase II: NGCP cont..
Other NGCP surveys:
Districts surveyed 282
District Endemic: 242
1983 : Iodized salt Production Opened to Private
Sectors
1984: Policy Decision Universal Salt Iodization (USI)
Compulsory Iodization all Edible Salt in Entire Country
Iodine

Phase III: NGCP
GOI –Unicef Project : 1992-97
NIDDCP High Priority
Increase in Production of Iodized Salt
National , State and District Levels Advocacy and Trainings
State Plan of Action for Prevention of IDD
Adequate Resources were Provided : Salt Department
Iodine
1992 :Goiter Control Program (NGCP)
Re-named
National Iodine Deficiency Disorders Control Program
1997:National ban Notification—Banning Sale of Edible Non-
Iodized salt
Iodine
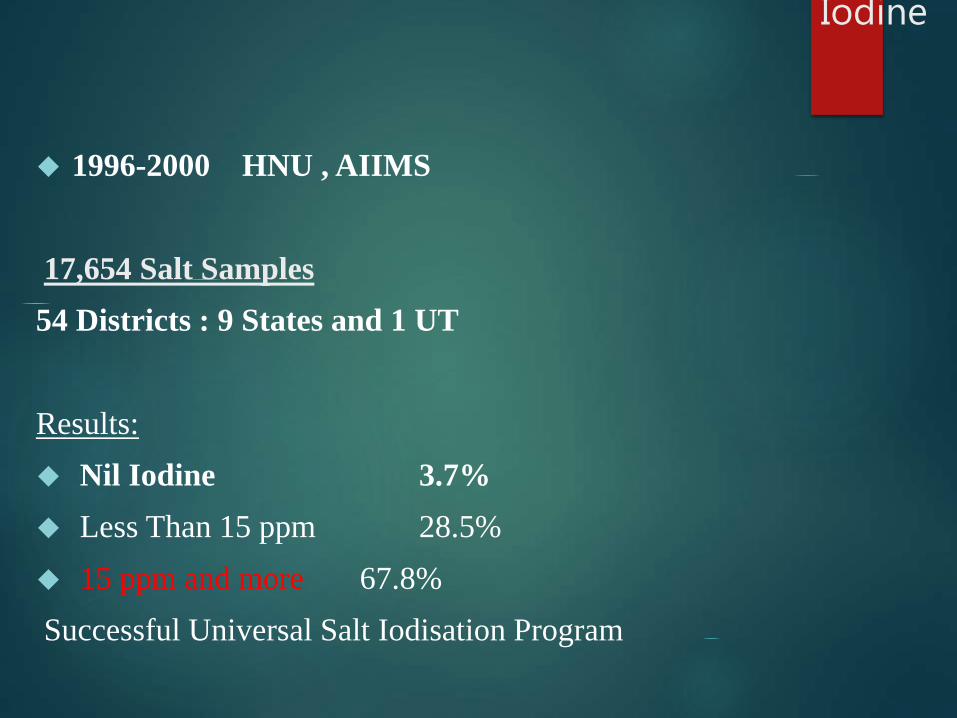
1996-2000 HNU , AIIMS
17,654 Salt Samples
54 Districts : 9 States and 1 UT
Results:
Nil Iodine 3.7%
Less Than 15 ppm 28.5%
15 ppm and more 67.8%
Successful Universal Salt Iodisation Program
Iodine
PHASE IV: 2000 ONWARDS
Objectives under NIDDCP:
Surveys to assess the magnitude of the Iodine Deficiency
Disorders.
Supply of iodated salt in place of common salt.
Resurvey after every 5 years to asses the extent of Iodine
Deficiency Disorders and the Impact of iodated salt.
Laboratory monitoring of iodated salt and urinary Iodine
excretion.
Health education. & Publicity
Iodine
Production and distribution of iodised salt intensified
Multiple studies conducted by ICMR to study the change after
introduction of iodised salt.
notification banning the sale of non-iodated salt for direct
human consumption in the entire country with effect from 17th
May, 2006 under the Prevention of Food Adulteration Act
1954.
Iodine

Results: district nutrition project
0.04
0.92
1.56
3.6
4.46
9.86
0.15
0.2
0.78
8.56
12.95
0.13
4.78
0.02
31.02
0.02
0 3 6 9 12 15
BADAUN
MAINPURI
BARAMULLA
MANDI
LAKHIMPUR KHERI
SRINAGAR
BIKANER
DEHRADUN
BISHNUPUR
NAGAON
GAYA
PATNA
DIBRUGARH
MEHBOOB NAGAR
RAIGARH
ALL DISTRICTS
NORTHERN DISTRICTS EASTERN DISTRICTS SOUTHERN DISTRICT
WESTERN DISTRICT ALL DISTRICTS
35
PREVALENCE (%) OF GOITRE AMONG CHILDREN
(6-< 12 YEARS)
Iodine
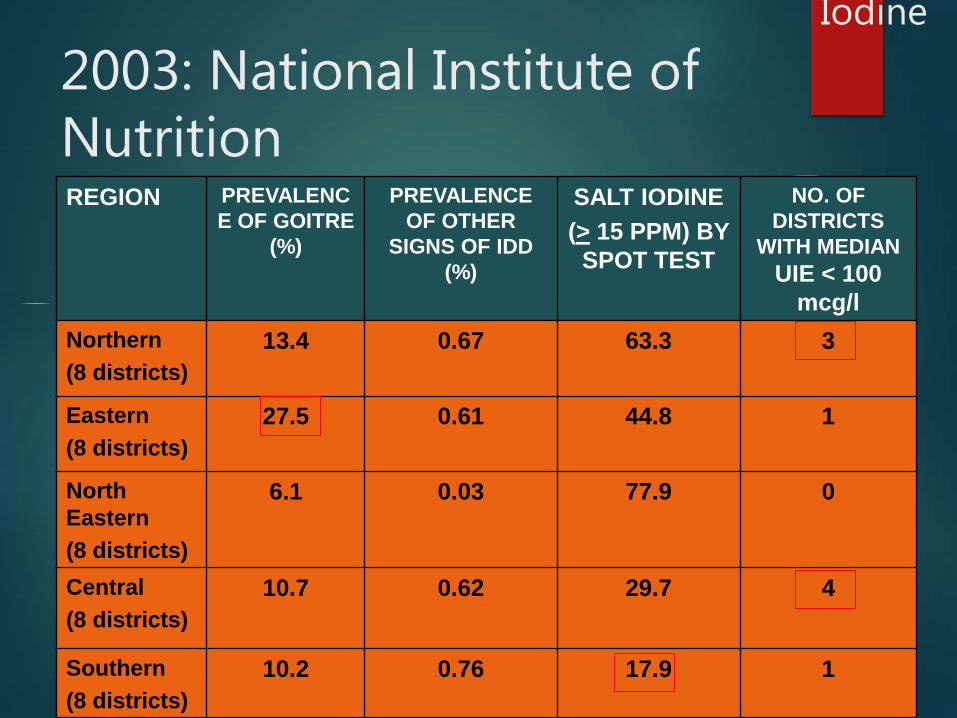
2003: National Institute of NutritionREGION PREVALENC
E OF GOITRE
(%)
PREVALENCE
OF OTHER
SIGNS OF IDD
(%)
SALT IODINE
(> 15 PPM) BY
SPOT TEST
NO. OF
DISTRICTS
WITH MEDIAN
UIE < 100
mcg/l
Northern
(8 districts)
13.4 0.67 63.3 3
Eastern
(8 districts)
27.5 0.61 44.8 1
North
Eastern
(8 districts)
6.1 0.03 77.9 0
Central
(8 districts)
10.7 0.62 29.7 4
Southern
(8 districts)
10.2 0.76 17.9 1
Iodine

STANDARDS FOR IODATED SALT
Moisture Not more than 6.0% by weight of the sample salt
Sodium Chloride Not less than 96.0 % by weight on dry basis
Matter soluble In water Not more than 1.0% by weight on dry basis
Matter Soluble In water other than Sodium chloride Not more than
3.0 % by the weight on dry basis
IODINE CONTENT AT
a. Manufacturing Level Not less than 30 parts per million (ppm) on dry
weight basis.
b. Distribution Not less than 15 parts per million on dry weight basis.
Iodine

PACKING OF IODATED SALT
BULK PACKING
50kg bags
Polyethylene lined jute bags
Retail packing for sale:
500gms or 1 kg packs
Following legends on packet:
Name of manufacturer
Month and year of packing
Iodine content (when packed)
Net weight
Batch number
Iodine
Iodine
Iodised oil
For moderate to severe prevalence of IDD
Mass level programmes carried out in China, South America,
Zaire, Papua New Guinea using iodised oil for injection
Iodised oil can also be given by mouth, but effects last for half
the time as compared to by injection.
Fortification of bread, rice and wheat was also done in various
trials.

Rapid Test Kit-Salt iodinedetection
Iodine levels in salt can be measured in the laboratory using a standard titration test or in the field using a rapid-test kit.
In NFHS-3, interviewers measured the iodine content of cooking salt in each interviewed household using a rapid-test kit.
The test kit consists of ampoules of a stabilized starch solution and of a weak acid-based solution and a colour chart

The interviewers were instructed to squeeze two drops of the starch solution onto a sample of cooking salt obtained from the household. If the colour changed (from light blue through dark violet), the interviewer matched the colour of the salt as closely as possible to a colour chart provided with the test kit and recorded the iodine level as <15 or >15 ppm.
If the initial test was negative (no change in colour), the interviewer was required to conduct a second confirmatory test, adding an acid-based solution in addition to the starch solution.
This test is necessary because the starch solution will not show any colour change even on iodized salt if the salt is alkaline or is mixed with alkaline free-flow agents.
If the colour of the salt does not change even after the confirmatory test, the salt is not iodized.


Titration Method It is most commonly used quantitative method, still remains the
reference method for determining the iodine concentration in salt
It requires the use of a small laboratory equipped with some basic instruments, such as precision scale, a burette, glassware, and pipettes
titration involves the preparation of four solutions and a standard solution(Na2S2O3, H2SO4,KI, Starch soln)
The iodine content of salt is determined by liberating iodine from salt and titrating the iodine with sodium thiosulfate using starch as an external indicator.
mg/kg (ppm) iodine = titration volume in ml x 21.15 x normality of sodium thiosulfate x 1000 / salt sample weight in g
ADMINISTRATIVE SET UP
1. The Central Nutrition and IDD Cell at D.G.H.S. is
responsible for the implementation of NIDDCP in the
country.
2. The Salt Commissioner’s Office under the Ministry of
Industry is responsible for licensing, production and
distribution of iodated salt to States/Uts.
3. Each State Government has an IDD Control Cell which
carries out periodic surveys regarding the prevalence of
IDD and reports to D.G.H.S. 31 States/UTs have
established such Cells.
4. A National Reference Laboratory for monitoring IDD at the
Bio-Chemistry & Biotechnology division, NICD, Delhi.
5. Four regional IDD monitoring laboratories
6. Each State has been sanctioned one IDD monitoring laboratory for
the monitoring of iodine content of salt and urine. 21 States/UTs have
established such laboratories.
Lab Region
the National Institute of Nutrition Hyderabad South
All India Institute of Hygiene & Public Health, Kolkata East
All India Institutes of Medical Sciences New Delhi west
National Institute for Communicable Diseases, Delhi North

Iron
Iron
Total body content of iron: 3-4 gm
1-1.5 gm Hb
2-2.5 gm storage iron
Sources:
Haem Iron Sources: nonvegetarian sources of iron e.g. meat,
fish and eggs. Milk a poor source of iron but breast milk an
efficient source for the infant.
Non-haem Iron Sources : vegetarian sources, namely cereals,
dark green leafy vegetables, pulses, nuts and dry fruits.

Absorption and bioavailability
Factors in food that increase absorption of iron:
Vitamin C
Amino Acids
Factors in food that decrease iron absorption
Phytates
Oxalates
Tannins
Phosphates
IRON

IRON
Absorption varies with type of cereal in the diet
Maximum for rice based diet and minimum for wheat
based diet
Dietary iron Absorption varies person to person
Adult men, children and adolescent boys: 3%
Adult women, lactating women, adolescent girls: 5%
Pregnant women: 8%
Basal loss through GI tract , sweat and urine:
Average basal loss across all age groups and gender for India : 14 mcg/kg/day
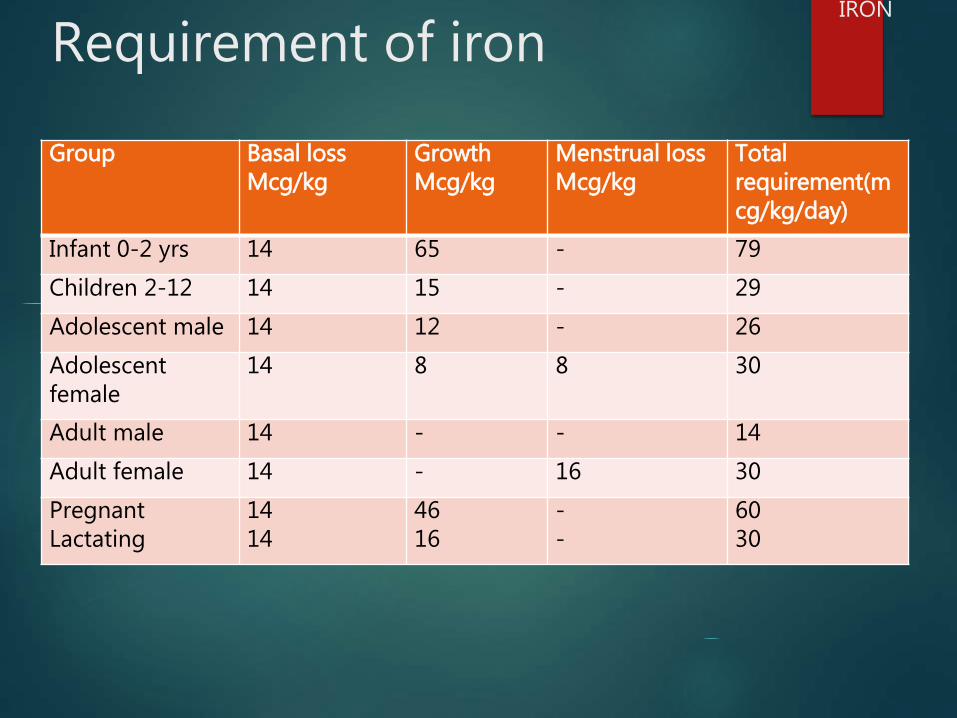
Requirement of iron
Group Basal lossMcg/kg
GrowthMcg/kg
Menstrual lossMcg/kg
Total requirement(mcg/kg/day)
Infant 0-2 yrs 14 65 - 79
Children 2-12 14 15 - 29
Adolescent male 14 12 - 26
Adolescent female
14 8 8 30
Adult male 14 - - 14
Adult female 14 - 16 30
PregnantLactating
1414
4616
--
6030
IRON

Functions :
component of haemoglobin and myoglobin.
constituent of important enzymes like cytochromes, catalase,
peroxidase,etc.
important functions in oxygen transport and cellular
respiration.
involved in cellular immune response for functioning of
phagocytic cells
IRON
Iron deficiency anaemia
Causes of iron deficiency
Inadequate ingestion
Increased requirement
Inadequate absorption
Inadequate utilization
Increased blood loss or excretion
Defects in release from stores
Signs & symptom:
fatigue
Headache
Weakness
Lack of concentration
Irritation
dizziness
IRON
Public Health problem
Categorized as one of the top ten most serious health problems in the modern world (WHO)
Globally – 41.8% pregnant women and 30.2% of non-pregnant are anaemic i.e 524 million women worldwide
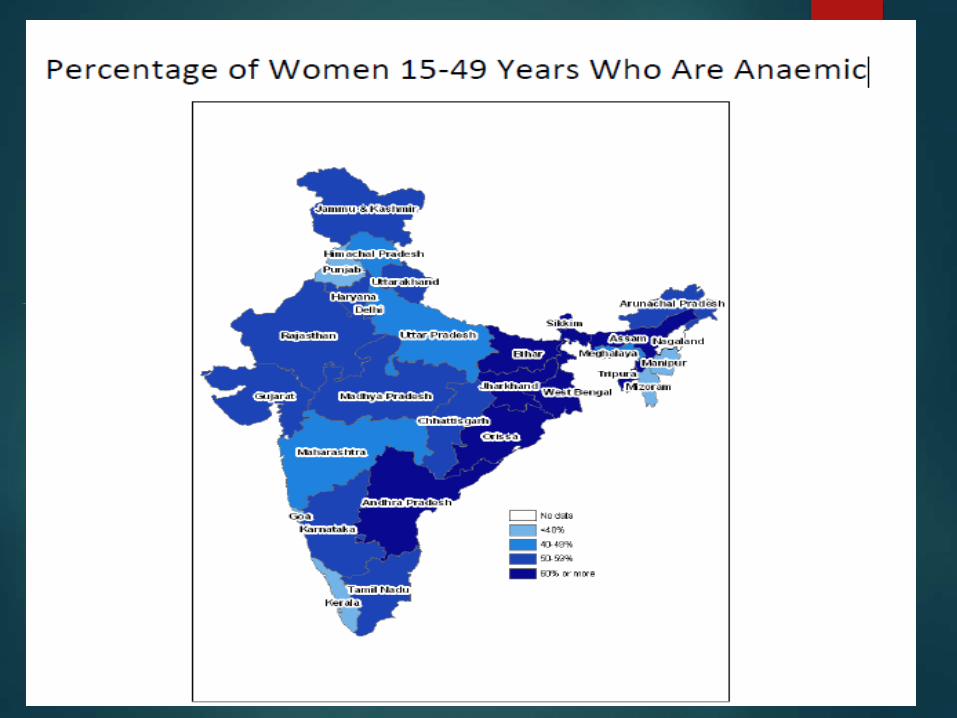
Prevalence of anaemia in India is among the highest in the world
56% Adolescent girls are anaemic
7 out of every10 children age 6-59months are anaemic in india
According to a survey conducted by NFHS, the prevalence of anaemia in young girls aged between 15-24 years is 56% with higher rates in rural than in urban India
More than 1,000 severely anemic young women die every week in the perinatal period because of inadequate iron status
Who report :1993-2005
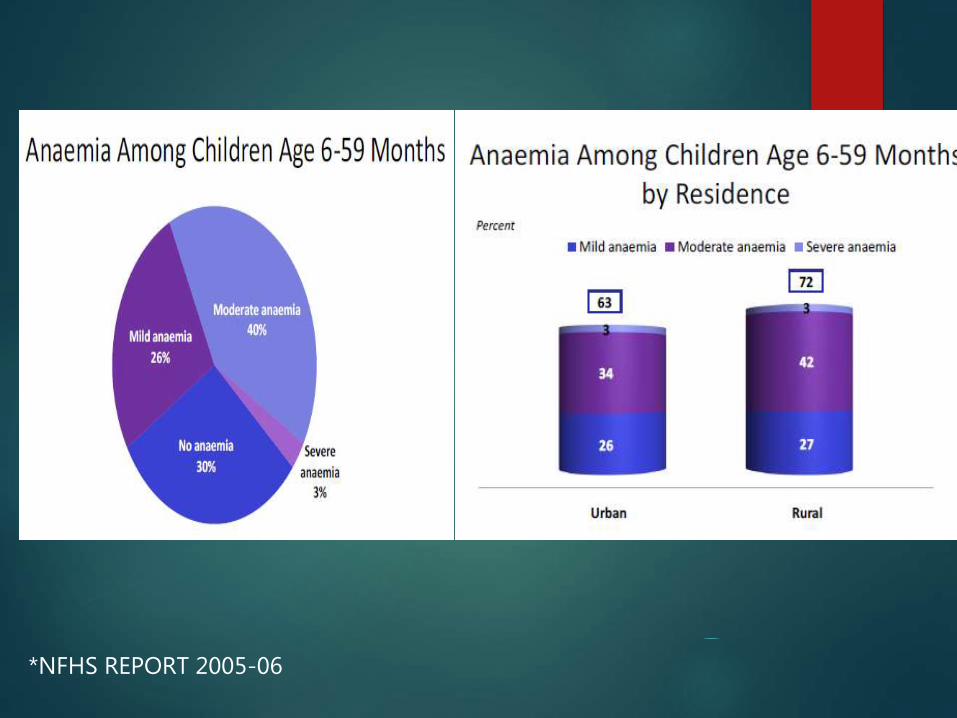
*NFHS REPORT 2005-06

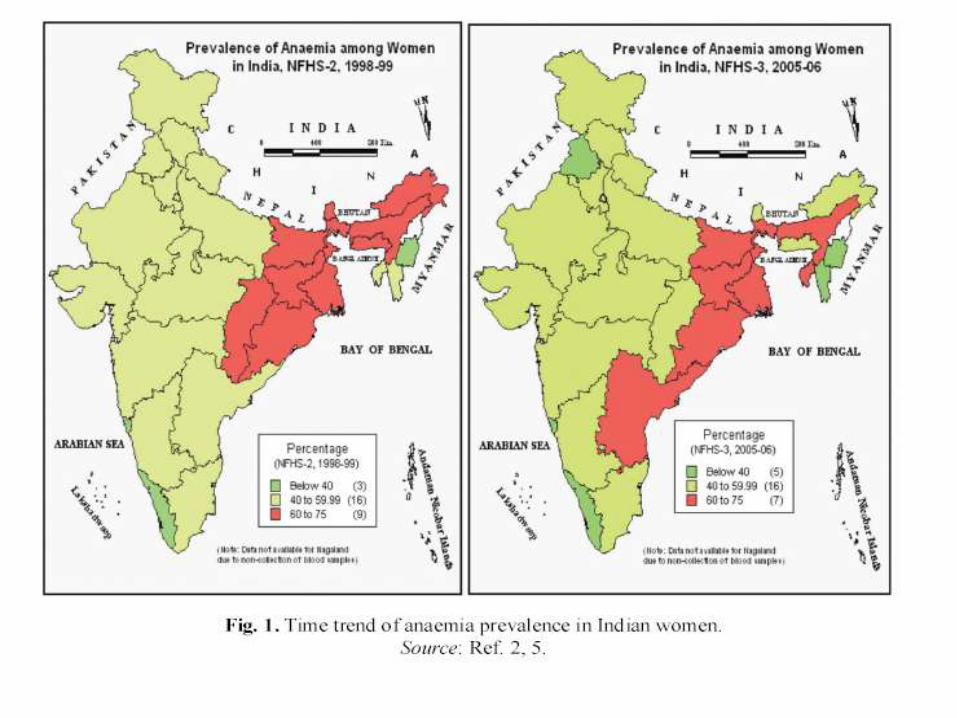
Iron deficiency anaemia: current status
35
15
2
52
39
16
2
56
Mild Moderate Severe Any anaemia
NFHS-2 NFHS-3
IRON
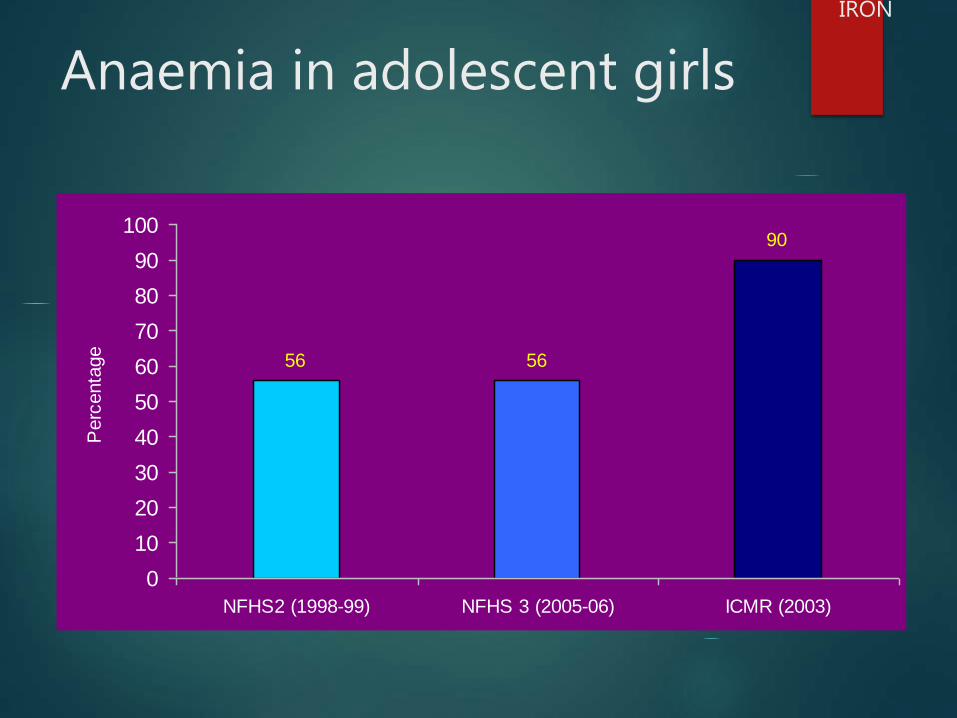
Anaemia in adolescent girls
56
90
56
0
10
20
30
40
50
60
70
80
90
100
NFHS2 (1998-99) NFHS 3 (2005-06) ICMR (2003)
Perc
enta
ge
IRON

Anaemia Testing in NFHS
The HemoCue system (Hb 201+) was used for Anaemia testing in the NFHS-3.
This system consists of a battery-operated photometer and a disposable microcuvette, coated with a dried reagent that serves as the blood-collection device. The test is performed using a drop of blood taken from a person’s fingertip.

HemoCue microcuvette :The
microcuvette is a plastic disposable unit that serves as both a reagent vessel and a
measuring device
The HemoCue Hb 201+ photometer: It measures light absorption and presents the results on a display. ambient temperature and protect it from direct sunlight. The HemoCue Hb 201+ analyzer has an internalelectronic “SELFTEST”.The sensitivity and the specificity of Hemocue Hb201+® were 95.1% and 65.3% respectively.
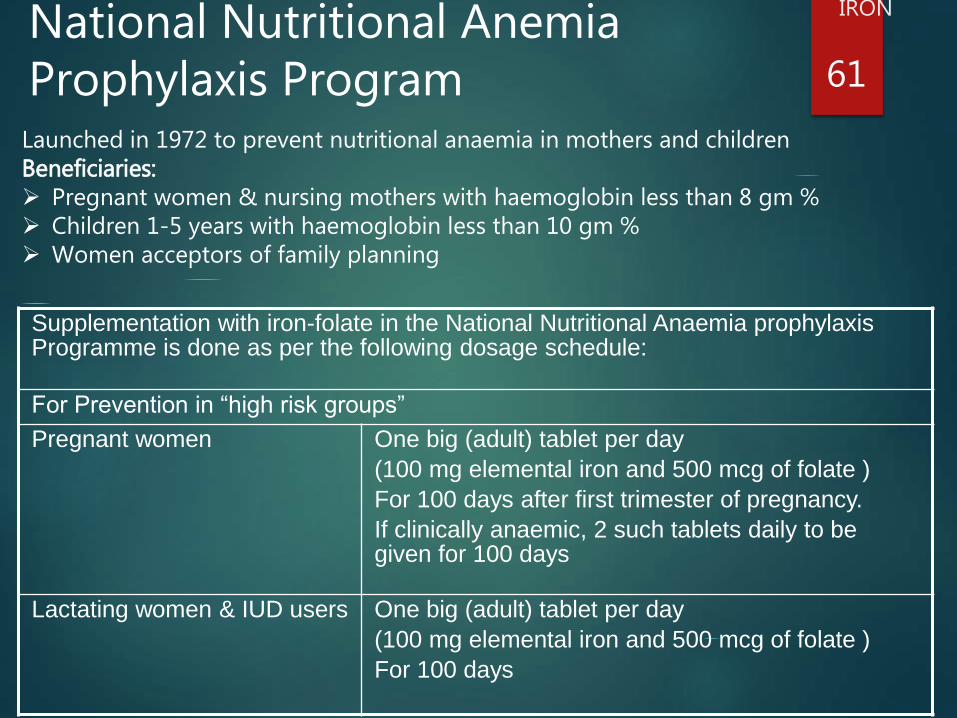
National Nutritional Anemia Prophylaxis Program
Supplementation with iron-folate in the National Nutritional Anaemia prophylaxis Programme is done as per the following dosage schedule:
For Prevention in “high risk groups”
Pregnant women One big (adult) tablet per day
(100 mg elemental iron and 500 mcg of folate )
For 100 days after first trimester of pregnancy.
If clinically anaemic, 2 such tablets daily to be given for 100 days
Lactating women & IUD users One big (adult) tablet per day
(100 mg elemental iron and 500 mcg of folate )
For 100 days
61
IRON
Launched in 1972 to prevent nutritional anaemia in mothers and childrenBeneficiaries: Pregnant women & nursing mothers with haemoglobin less than 8 gm % Children 1-5 years with haemoglobin less than 10 gm % Women acceptors of family planning

Supplementation with iron-folate in the National Nutritional Anaemia Prophylaxis Programme is done as per the following dosage schedule:
Pre-school children 6-60 months
One small (paediatric) tablet (20 mg elemental iron and 100 mcg of folate )
Biweekly throughout the period of 6-60 months
School children 5-10 years 45mg elemental iron + 400 ug folic acid weekly, throughout the entire period of 5-10 years
Adolescent 10-19 years One big(adult) tablet
(100mg elemental iron +500 mcg of folate)
weekly throughout the entire period of 10-19 years
women in reproductive age group (15-45 years)
One big(adult) tablet weekly throughout the reproductive period
(100 mg elemental iron +500 mcg of folate )
62
IRON
12 X 12 INITIATIVE
LAUNCHED ON 23rd APRIL,2007 AT AIIMS ,NEW
DELHI
Organized by DEPARTMENT OF OBSTETRICS &
GYNECOLOGY OF AIIMS in collaboration with WHO ,
UNICEF AND FOGSI.
OBJECTIVE---Ensuring every child at least 12gm%
Hemoglobin by 12 yrs of age.
GOALS --- 1)To determine the prevalence of anemia in
adolescence to ensure healthy parenthood.
2)To increase awareness among adolescents
regarding anemia and appropriate nutrition.
SPECIFIC ACTIVITES
Hb testing camps at various cities/towns of India under the banner of 12X12 initiatives.Program coverage
The camps are conducted in schools for the student’s of 5th to 7th level primarily focusing girl child.
formal presentation on anaemia (giving focus on importance of Hb
Lab technicians performs the Hb testing on students.
A Health card is maintained for each student .
a literature on anaemia is also provided to each student.
The students with low Hb (<11.5 gm) are provided 5-10 days course of Orofer XT tablets or suspension.
Till now we have conducted such camps in 40 cities/towns of India and covered a population of over 100,000 students.
IRON FORTIFICATION NATIONAL INSTITUTE OF NUTRITION,Hyderabad showed that simple
addition of ferric ortho-phosphate or ferrous sulphate with sodium bisulphate was enough to fortify salt with iron.
Commercial production of iron fortified salt was started in 1985.
In 2005, NIN, Hyderabad evolved the concept of fortification of iodized salt with iron (double fortified salt, DFS) for controlling IDD and IDA as 'one intervention controlling two problems'
The Prime Minister's Office on April 2011 issued instructions for the introduction of DFS in ICDS, MDM and PDS in phased manner
DFS is being supplied at Orissa in the open market and in MDM programmes of Karnataka, Chhattisgarh, Jharkhand & Haryana
Iron Fortified Wheat Flour (Atta) and Rice: Doubts have been raised about bio-availability of iron from wheat 'atta’ because of high phytate(inhibitor of absorption) content.

Zinc
Zinc is present in small amounts in all tissues of the body.
Total content of the body is 1.4 to 2.3 g.
Sources :
Meat
Whole grains
Legumes.
Nuts

Absorption and Bioavailability
Zinc absorbed mainly from jejunum
Absorption affected by
Phytates in diet
Proteins in diet
Total zinc content
Calcium and other divalent ions in diet
Chronic iron supplementation decreases zinc absorption
Fermentation of food digests phytates: zinc availability
increases
Zinc

RDA- ZINC
RDA
ADULT MALE 15mg
ADULT FEMALE 12mg
PREGNANCY 15mg
LACTATION 20mg
INFANT 5mg
CHILDREN 10mg
Zinc

Zinc
Functions :
Part of over 100 enzymes
Protein and carbohydrate metabolism,
Bone metabolism
Oxygen transport.
Immune response and gene expression.
Structural constituent of leucocytes
Role in the synthesis of nucleic acids
Lymphoid tissue contains zinc.
Efficient storage of insulin in pancreas.
Powerful antioxidant.
Zinc- deficiency The principal clinical features of severe zinc deficiency in humans are
Growth retardation
A delay in sexual and skeletal maturation
The development of orificial and acral dermatitis
Diarrhoea
Alopecia
A failure of appetite/ affects voluntary food intake
Appearance of behavioural changes.
An increased susceptibility to infections (reflects the development of
defects in the immune system)
Altered taste
Delayed wound healing
Restricts utilization and storage of vitamin A
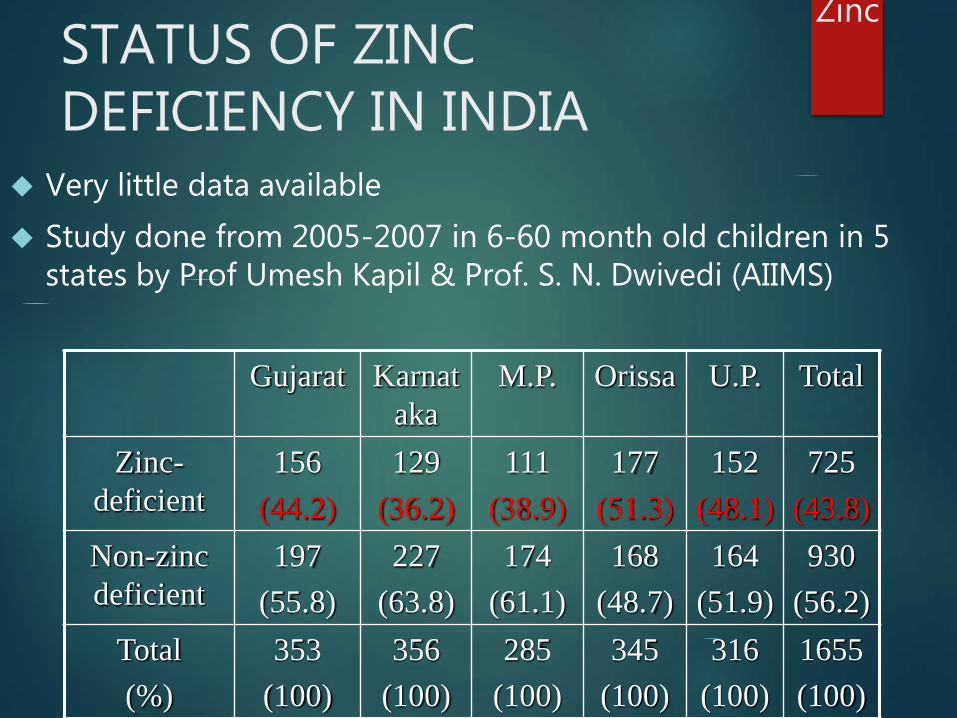
STATUS OF ZINC DEFICIENCY IN INDIA
Very little data available
Study done from 2005-2007 in 6-60 month old children in 5 states by Prof Umesh Kapil & Prof. S. N. Dwivedi (AIIMS)
Gujarat Karnat
aka
M.P. Orissa U.P. Total
Zinc-
deficient
156
(44.2)
129
(36.2)
111
(38.9)
177
(51.3)
152
(48.1)
725
(43.8)
Non-zinc
deficient
197
(55.8)
227
(63.8)
174
(61.1)
168
(48.7)
164
(51.9)
930
(56.2)
Total
(%)
353
(100)
356
(100)
285
(100)
345
(100)
316
(100)
1655
(100)
Zinc

Other studies conducted in 1998- 2004 suggested that a 10- to 14-day therapy of zinc treatment can considerably reduce the
1. Duration and severity of diarrhoeal episodes,
2. Decrease stool output, and
3. Lessen the need for hospitalization.
4. May also prevent future diarrhea episodes for up to next three months.
Zinc
WHO and UNICEF recommend daily 20 mg zinc supplements
for 10–14 days for children with acute diarrhoea, and 10 mg
per day for infants under six months old
Government adopted policy of use of Zinc in treatment of
diarrhoea in National Rural Health Mission in children < 5
years from the year 2008.
Zinc
Zinc
Acute zinc poisoning:
after ingestion of 4-8 g of zinc.
nausea, vomiting, diarrhoea, fever and lethargy
Long-term exposure to high zinc intakes result in interference
with the metabolism of other trace elements.
Copper utilization is especially sensitive to an excess of
zinc.
Copper/zinc interaction may cause copper deficiency::
deliberately exploited to control copper accumulation in
Wilson disease .
Changes in serum lipid patterns and immune response have
also been associated with zinc supplementation
Zinc toxicity

Selenium

Selenium
It is present in all body tissues except fat.
Sources : Meat, fish, nuts and eggs are good
sources. vegetarians and vegans may be at risk of
deficiency.
Functions :
Selenium is an integral part of over 30
selenoproteins; the most important of which are
glutathione peroxidases and iodothyronine
deiodinases.

SELENIUM
Requirements : Recommended daily intake is 70 µg (WHO)
ICMR recommends:
RDA
Infants 6-12 mcg
Children 20-30 mcg
Adult 50mcg
Deficiency :
Its deficiency is associated with increased coronary artery
disease.
Keshan disease (endemic cardiomyopathy) in China
Kashin Beck syndrome, an osteo-arthropathy in children of 05-
13 years age is seen in selenium deficient areas
SELENIUM

The major histopathological feature of Keshan disease is a
multifocal myocardial necrosis.
Coronary arteries unaffected.
Membranous organelles, such as mitochondria or
sarcolemma, affected earliest.
Once the disease is established, selenium is of little or no
therapeutic value.
Treatment generally follows the standard procedures
employed in cases of congestive heart failure.
SELENIUM
Selenium
Kashin-Beck disease: an endemic osteoarthropathy linked
with low selenium status.
Primarily affects children between the ages of 5 and 13 years
living in certain regions of China
Advanced cases of the disease are characterized by
enlargement and deformity of the joints.
The principal pathological change is multiple degeneration and
necrosis of hyaline cartilage tissue.
Some studies have suggested that selenium may prevent
Kashin-Beck disease, but this work needs further confirmation
SELENIUM TOXICITY
Chronic selenium poisoning
loss of hair and changes in fingernail morphology.
skin lesions (redness, blistering)
nervous system abnormalities (paresthesia, paralysis,
hemiplegia)
In animals, particularly rats, liver damage is a common feature
of chronic selenosis but evidence less convincing in humans .
SELENIUM

Copper
Copper
An essential trace element:
component of many metallo-enzyme systems
Role in iron metabolism
The amount of copper in the adult body is estimated to be 80 -
100mg.
Sources : Meat, nuts, cereals and fruits are good sources

Copper
Functions : Many metalloenzymes contain Copper.
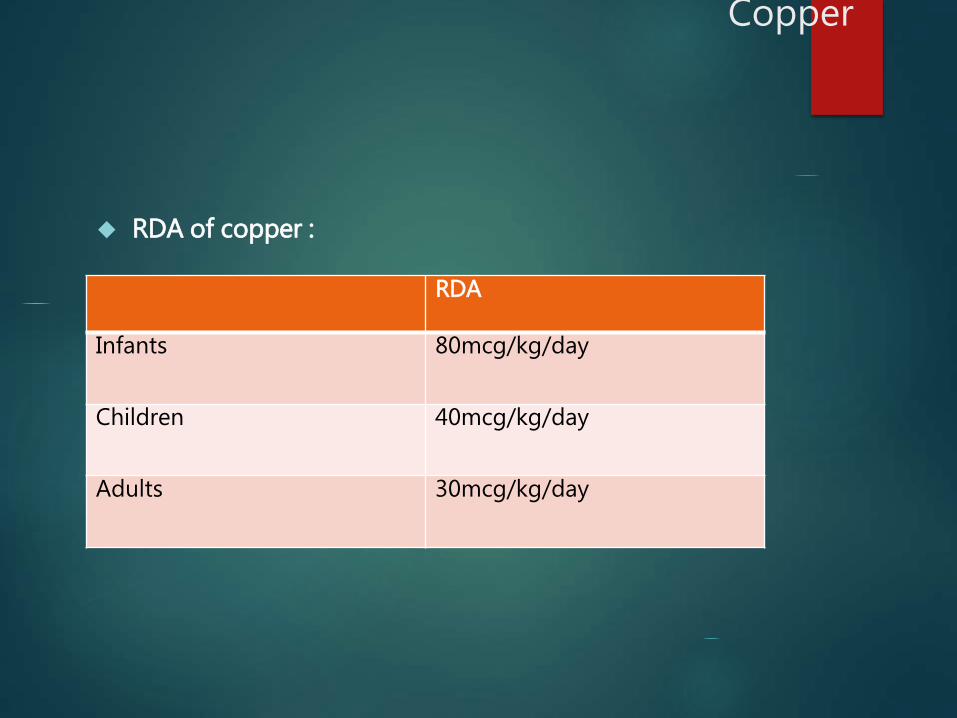
RDA of copper :
RDA
Infants 80mcg/kg/day
Children 40mcg/kg/day
Adults 30mcg/kg/day
Copper
Copper Deficiency
Deficiency : Copper deficiency is rare.
Hypocupraemia : serum copper level <= 0.8mcg/ml
in patients with nephrosis
Wilson’s disease and
protein energy malnutrition.
Neutropaenia - commonest abnormality of copper deficiency.
Infants, especially premature, may develop copper deficiency
usually presenting as chronic diarrhoea. Neutropaenia and
later anaemia develop and they do not respond to iron.
Copper deficiency may be a risk factor for coronary heart
disease as it has been associated with raised plasma
cholesterol levels and heart-related abnormalities
Copper

Molybdenum

Molybdenum
Requirement 25 µg/day in adults
RDA: 500µg/day
The three principal molybdenum-containing enzymes
xanthine dehydrogenase
aldehyde oxidase
sulfite oxidase
A reduced tissue activity of xanthine oxidase has been associated with xanthinuria,
a genetic defect characterized by a low output of uric acid and high concentrations of xanthine and hypoxanthine in blood and urine.
Clinical manifestations: renal calculi formed or deposition of xanthine and hypoxanthine in muscles resulting in a mild myopathy
MOLYBDENUM
Other enzyme, sulfite oxidase,
responsible for the conversion of sulfite into inorganic sulfate,
Genetic "deficiency" of sulfite oxidase have been detected in early human infancy and have a lethal outcome at the age of 2-3 years.
The lesion results in severe neurological abnormalities, mental retardation and ectopy of the lens.

Molybdenum deficiency
A nutritional deficiency of molybdenum leading to decreased
activity of sulfite oxidase reported in those on prolonged total
parenteral nutrition.
The clinical symptoms included irritability followed by
tachycardia, tachypnoea and night blindness. Severe cases, coma
may be seen.
The clinical symptoms of molybdenum deficiency were totally
eliminated by supplementation with 300 µg of ammonium
molybdate (147 µg of molybdenum) daily.
Molybdenum toxicity
Molybdenum intoxication is accompanied by a secondary deficiency of copper.
Typical features of molybdenosis include
defects in osteogenesis leading to skeletal and joint deformities, spontaneous fractures, and mandibular exostoses .
Alkaline phosphatase activity decreases.
Due to copper deficiency: anaemia, cardiac hypertrophy, and achromotrichia arising from the development of defects in melanin synthesis in hair

Chromium

Chromium
Chromium is an essential nutrient that potentiates insulin
action and thus influences carbohydrate, lipid and protein
metabolism.
Sources
Processed meats, whole grain products, pulses and spices
are the best sources of chromium
while dairy products and most fruits and vegetables
contain only small amounts
Deficiency occurs if diets contain predominantly refined foods
Deficiency also associated in infants with PEM
Requirement: 33 µg/day

Chromium deficiency
Deficiency produces a state similar to diabetes mellitus
So far seen only in patients on long term parentral nutrition
Symptoms include:
impaired glucose tolerance and glucose utilization
weight loss
Neuropathy
elevated plasma free fatty acids,
depressed respiratory quotient
abnormalities in nitrogen metabolism.
All symptoms alleviated by chromium supplementation

Chromium toxicity
Toxicity not seen with excess intake of trivalent chromium.
Hexavalent chromium is much more toxic than the trivalent
form
oral administration of 50 µg/g diet has been found to induce
growth depression together with liver and kidney damage in
experimental animals
Not seen in humans so far

MANGANESE

Manganese
Sources:
Diets high in unrefined cereals, nuts, leafy vegetables and
tea will be high in manganese;
diets high in refined grains, meats and dairy products will
be low.
Functions: both an activator and a constituent of several
enzymes.
Activates: hydrolases, kinases, decarboxylases and
transferases, glycosyltransferase and xylosyltransferase.
Mn is a constituent of arginase, pyruvate carboxylase,
glutamine synthetase, and manganese superoxide
dismutase.

Manganese deficiency
Manganese deficiency has been produced in many species of
animals, but not, so far, in humans.
Signs of manganese deficiency include
impaired growth
skeletal abnormalities
disturbed or depressed reproductive function
ataxia of the newborn
defects in lipid and carbohydrate metabolism
Manganese toxicity
Manganese among the least toxic
The major signs in animals: depressed growth, depressed
appetite, impaired iron metabolism and altered brain function
Cases of human toxicity few.
Chronic inhalation of airborne manganese in mines, steel
mills and some chemical industries.
Signs of toxicity in Chilean manganese miners
severe psychiatric abnormalities, hyperirritability, violent
acts and hallucinations (manganic madness).
As the disease progresses, permanent crippling
neurological disorder of the extrapyramidal system similar
to Parkinson disease
Nickel
Sources:
Plant sources contain more nickel than animal sources
Approximately half the total daily intake of nickel is usually
derived from the consumption of bread and cereals
Milk, coffee, tea, orange juice, ascorbic acid depress absorption
Requirement : 100 µg/day.
Safe upper limit of consumption: 600 µg/day
Function:
four nickel-containing enzymes : urease, hydrogenase,
methylcoenzyme M reductase and carbon-monoxide
dehydrogenase

NICKEL
Nickel deficiency:
Deficiency rare in humans
Growth and haematopoiesis depressed, especially in those
with a marginal iron status.
Iron utilization impaired

Boron
Sources:
Foods of plant origin especially fruits, leafy vegetables,
nuts and legumes are rich sources.
Wine, cider and beer are also high in boron.
Meat, fish and dairy products are poor sources.
Requirement:0.75 mg/ day
Functions:
Affects steroid harmone metabolism
Studies suggest role in metabolism of other minerals like
aluminium and magnesium

BORON
Boron deficiency:
Dietary boron affects plasma and organ calcium and magnesium concentrations, plasma alkaline phosphatase, and bone calcification.
Boron deficiency causes
elevated urinary excretion of calcium and magnesium
depressed serum concentrations of lipo-estradiol and ionized calcium
lower plasma ionized calcium and serum 25-hydroxycholecalciferol
higher serum calcitonin and osteocalcin
Boron toxicity:
Osteoporosis
Two infants whose pacifiers were dipped into a preparation of borax and honey over a period of several weeks exhibited scanty hair, patchy dry erythema, anaemia and seizure disorders
Fluoride It is found in combined forms
96% of fluorides in the body found in bone and teeth.
An essential for normal mineralisation of bones and formation of dental enamel
Source:
Drinking water : Fluorine in the drinking water is 0.5 mg per ltr. Excess of fl > 3mg causes flourosis.
Foods: Sea fish, cheese, Tea
Dental fluorosis : chalky white teeth, transverse yellow bands on teeth
Skeletal fluorosis: severe pain and stiffness in joints , stiffness in neck and backbone, bow legs
Public health problem:
Fluorosis affects 25 million people and 66 million are at risk
Endemic in 275 districts of 20 states in india : AP, MP, ORRISA , BIHAR, CHATTISGARH,
National Programme for Prevention & Control of Fluorosis:2008-9
Preventive measures: providing defluoridated water, rain water harvesting , restrict intake of fluorine rich items: tobacco, supari, black tea and black salt, use of fluoride rich casmetics/drugs

References
WHO Technical Research Series no. 580, 1996
WHO Technical Research Series no. 532, 1973
Recommended Dietary Intakes for Indians. Report of an Expert Group,Final Draft . ICMR, New Delhi, 2010.
Nutrition India, NFHS 3 Report, 2005-06.
Park K, Textbook of Preventive and Social Medicine, 20th edition
Taneja D K, Health Policies and Programmes in India, 12th edition
Revised Policy Guidelines on National Iodine Deficiency Disorder Control Programme, Ministry of Health & Family Welfare, 2006
Kapil Umesh, et al. Process of implementation of National Iodine Deficiency Disorders Control Programme activities in Himachal Pradesh, India, Indian J Public Health. 1995 Oct;39(4):172-175

Thank you