importance of frozen semen evaluation in artificial insemination programs barth
TRANSCRIPT

Importance of Frozen Semen Evaluation in Artificial Insemination Programs
Albert BarthWestern College of Veterinary MedicineUniversity of Saskatchewan, Saskatoon, SK, Canada, S7N 5B4
The artificial insemination (AI) industry in is highly competitive and AI centers must strive to produce a high quality product to remain in business. Therefore, most frozen semen on the market is of high quality and performs well in the hands of experienced producers and AI technicians. In most countries, stringent federal regulations require quarantine facilities for all bulls and extensive testing for diseases transmissible in semen combined with the regulations from importing countries, ensure that frozen semen will be free of specific pathogens. However, there usually there are no government regulations or uniform AI industry standards for semen quality traits. Minimum standards for post-thaw viability, sperm abnormalities or numbers of viable sperm per dose are largely based on field experience with individual bulls and thus may vary not only between AI centers but also between bulls within an AI center. For example, sperm numbers for one insemination dose from a highly fertile bull may be too low for other bulls. Furthermore, since to some degree each AI center has developed it's own methods of evaluating semen quality traits and because the measurement of these traits is often subjective, adoption of uniform industry standards hasn't occurred. The AI industry has strived diligently to find a method of evaluating frozen semen which would accurately predict its performance in the field. Because of various degrees of inaccuracy and subjectivity associated with semen evaluation as well as the measurement of actual fertility by the non-return rate method, correlations between semen tests and fertility have often been low. Furthermore, even highly sophisticated methods using computer-assisted analysis have not improved the ability to accurately predict the performance of frozen semen in the field. This is not to say that evaluating frozen semen is useless. In general, frozen semen evaluation using minimum quality standards are used regularly at all AI centers to discard substandard quality semen and to monitor effects of semen processing (process quality control). In the case of beef bulls, AI centers may need to discard up to 1/3 of all ejaculates due to insufficient quality. Nevertheless, semen of unacceptable quality may inadvertently enter the market. Some reasons for poor quality semen entering the market are:
1. Semen quality of certain bulls can vary dramatically over short periods of time and sudden changes could be missed by tests that are semi-routine. Laboratory personnel are usually in an assembly line type of production and time constraints may not permit intensive testing of all ejaculates.
2. There is a great deal of marketing pressure on AI centers to freeze and distribute semen from popular bulls, some of which produce low quality semen. This is particularly true for beef bulls in custom semen production where the bull is not owned by the center. Yearling beef bulls are often pressed into semen production before completion of postpubertal maturational changes and older beef bulls frequently become obese. The show ring does not select for fertility and often champion bulls have testicular deficiencies. Some breeders of purebred cattle desire the genetics of a low fertility bull badly enough to accept or overlook low quality semen. AI centers are often under pressure to release substandard semen on the understanding that it will not be distributed or sold. Nevertheless, once the semen is released to the bull owner, the AI center has lost control of it.
3. Semen in field storage may have been mishandled. Repeated exposure of semen to ambient temperatures or to the warmer temperatures in the neck of the nitrogen refrigerator, has a cumulative, negative effect on post-thaw viability of the sperm.

Veterinarians are often asked to evaluate frozen semen, but most lack the equipment and expertise to do a valid examination. However, many veterinarians and particularly those involved in embryo transfer and estrous synchronization programs, might find it economically feasible to develop this capability. Veterinarians involved in embryo transfer, because of costs involved, are most acutely aware that low semen quality may be a cause of fertilization failure. In fact, there is evidence which suggests that superovulated cows require higher quality semen and a higher sperm dose than single ovulating cows to reach their reproductive potential (1,2).
It is absolutely imperative that veterinarians who evaluate frozen semen understand that good equipment and a consistent, meticulous effort is necessary to obtain meaningful results. Frozen semen evaluations by veterinary practitioners may not be as accurate as those of more qualified laboratories; however, they would reduce the risk of failure in embryo transfer and AI programs. If, in the eyes of the examiner, semen is found to be of poor quality, an inquiry to the AI center that produced the semen should be made to obtain a history of the particular bull in question and to discuss the current findings. All results must be kept in confidence between the owner, the veterinarian and the AI center.
Some or all of the methods of evaluation described in this paper are used by all AI centers, however, the techniques used may vary somewhat and other tests may also be used. Due to the subjectivity of laboratory tests, and human, animal and environmental factors that influence fertility, AI organizations have not adopted uniform industry standards. The National Association of Animal Breeders has developed a position paper on laboratory tests for evaluating bovine semen which discusses how laboratory tests can be utilized as part of an overall monitoring of semen quality, and also to point out some of their limitations (3). The methods described here are those most likely to be practical to veterinary practitioners and are proposed as the standard method of frozen semen evaluation recommended by the Society for Theriogenology.
Methods Of Frozen Semen EvaluationEquipment
Evaluations must be done in a warm and clean laboratory environment. Student microscopes that find their way into veterinary practices often have a poor light source and low quality objectives. They usually cannot be upgraded and a veterinarian wishing to do frozen semen evaluations may have to realize a considerable cash outlay for a new microscope. A high quality microscope with a capability of 1000 X bright field, phase contrast at 200-400 X and 1000 X and a mechanical warm stage are necessary. Differential interference contrast (DIC) is very expensive and is not a necessity, however, it has advantages over phase contrast for sperm morphology and acrosomal integrity examination in wet mounts. In addition a slide warmer and a water bath, or other equipment for maintaining semen temperature, are essential. Slides and cover slips must be new, clean and warmed to 37 oC.Semen Traits to be Evaluated
Basically, at least three semen quality parameters must be evaluated:1. Post-thaw viability2. Sperm morphology3. Number of motile cells per dose(4. Microbial identification)
In most cases the fourth category of microbial pathogen assays would be unnecessary, however, it should be considered when a history of infertility implicates a possible infectious cause or when normally fertile females fail to settle even though the semen has good viability, good morphology and adequate dose.
If possible, three doses of semen from each freeze date should be thawed and examined. All doses may be combined or evaluated separately. For sperm morphology, one straw or unit is sufficient. When semen is very expensive one straw may be evaluated and if the semen quality is satisfactory, no further evaluation should be necessary. However, when the evaluation of one dose is unsatisfactory, more semen should be evaluated before drawing any conclusions, particularly regarding viability.
It is usually most practical to thaw semen, whether packaged in straws or ampules, in a 37 oC water bath (4). The straws are then dried and emptied into a 1 or 2 ml tube which maintained at 37 oC water bath for the duration of the semen evaluation. On occasion it seems that some batches of tubes contain a toxic residue. For each new batch of tubes, a semen sample should be incubated in a serum tube for two hours and compared to the same semen incubated within an unopened straw. Care must also be taken to ensure that slides and cover slips remain free from potentially spermacidal contamination.
1. Post-Thaw ViabilityPost-thaw viability reflects the recovery of sperm from the freeze-thaw process. It is assessed
by determining the percentage of progressively motile spermatozoa, the vigor of progression and a direct examination of the acrosomal membranes for their integrity. Membrane damage may not be fully expressed immediately after thawing, however, when semen is incubated at 37 oC for several hours (stress test) loss of viability may occur indicating the full extent of freeze-thaw damage. Although different time periods of incubation for the stress test have been reported (5,6), we propose the use of a 2 - hour stress test as a uniform standard for practitioners. It should be recognized, however, that extenders differ in their ability to support viability at 37 oC. Since sperm do not remain in extender following insemination, this difference may not be interpreted as important to fertility when comparing semen in different extenders. Again, a positive (good) incubation quality is indicative of good semen viability. On the contrary, poor incubation quality should be rechecked or additional information on the bull sought.
(a) Motility examination.Many different methods of assessing motility have been developed ranging from a visual
estimate for percent motility to use of sophisticated equipment. The use of computer technology for rapid determination of motility and other semen traits has been adopted by many AI centers. At the present time, however, visual microscopic assessment of motility is probably the most acceptable method for veterinary practitioners.
The percent of progressively motile spermatozoa and their vigor of progression (rate) should be determined immediately after thawing and after 2 hours of incubation. Straws (1/2 mL) require a little over 30 seconds to reach a water bath temperature of 37 oC and motility is usually fully expressed within 2 minutes after thawing. Contents of straws should be emptied into a tube by pushing the cotton plug through the straw using a wooden or metal rod. A small drop of semen which would spread barely to the edges of the cover slip is transferred to a warm slide. The number of cells moving progressively in a field is counted followed by a count of the number not moving progressively and the percent of motile spermatozoa is determined. More than one wet mount should be examined and at least 500 cells in 10-15 fields should be counted in order to obtain repeatability. A subjective evaluation of the rate of progression of spermatozoa could be made using the following scoring system.
0 = no movement1 = slight tail undulation or vibration without progression
2 = slow progression, including stop and start motion3 = strong progressive motion 4 = very rapid progressive motion (tails often look fan-shaped)
Spermatozoa will be moving at different speeds and the score assigned will pertain to the rate of the majority of spermatozoa.
The percent of motile spermatozoa immediately after thawing multiplied by the total number of spermatozoa per dose will determine the number of viable spermatozoa inseminated. The number of viable spermatozoa inseminated would likely be a more important semen trait than the percentage of motile spermatozoa. However, in as much as percentage of motile spermatozoa reflects the viablity of semen which went into the freezing process as well as the fortitude of spermatozoa to survive the freeze thaw process, it is a useful measure of semen quality in itself. Minimum standards for motility have not previously been suggested. The Society for Theriogenology has adoptd a minimum standard for motility as follows:
0 hr = 25motile at a rate of 32 hr = 15motile at a rate of 2
A higher standard is desirable for superovulated cows.
(b) Percent Intact Acrosomes (PIA)Determination of the PIA is a morphologic method of measuring post-thaw viability
that is also correlated to fertility (6). It is a valuable addition to motility estimates in determining the viability and potential fertilizing capacity of spermatozoa since not all immotile cells are necessarily dead, whereas, sperm without acrosomes are irreversibly damaged. To examine the acrosome, cell motion must be stopped. This may be accomplished by mixing the semen with 0.2buffered glutaraldehyde which fixes the membranes and prevents further deterioration (7). Mixing may be done on the slide by placing a small drop of semen next to a small drop of 0.2glutaraldehyde, mixing and applying a cover slip. The amount of fluid on the slide must be sufficient so that it barely reaches the edges of the coverslip to minimize the depth of field, otherwise, examination of the acrosomes will be difficult due to constant focusing adjustments on each spermatozoon. It is particularly important to make the coverslip preparation very thin when semen is extended in milk as the milk fat globules tend to obscure the spermatozoa.
Acrosomes are examined at 1000 X magnification with phase contrast or DIC. Acrosomes are often difficult to evaluate with phase contrast when semen has been extended in milk and in this regard, DIC is superior to phase contrast. With phase contrast, acrosomes that are intact will have a dark ridge at the apex of the spermatozoon. Swollen acrosomes lose the dark ridge and are not counted as intact. Acrosomes with broken membranes will usually show as a faint ruffled line just ahead of the apex of the sperm nucleus. With DIC, light will appear to come from an angle, usually from the 11 or 4 o'clock position. When the apex of a spermatozoon points away from the light source, the intact acrosome will have a dark ridge at it's apex but when the spermatozoon points toward the light source it will have a bright white ridge which resembles the edge of a pumpkin seed. Non-intact acrosomes lack a ridge or show a ruffled membrane separated from the apex of the nucleus.
Two hundred cells should be examined and the first and second counts of 100 should be compared. If these counts are within 5 of each other no further counts are necessary. The Giemsa(8), Wells-Awa(9) and Spermac(10) staining techniques have been reported to be useful for studying the acrosome with ordinary light microscopes lacking phase contrast or DIC capabilities. However, all of these staining techniques involve drying and washing steps that will vary in efficiency with semen in different extenders giving potentially unreliable results. Acrosome counts are done immediately after

thawing and after a 2-hour stress test. Minimum standards for percent intact acrosomes have not been previously suggested. The Society for Theriogenology has adopted minimum values for percent intact acrosomes as follows:
0 hr = 60intact acrosomes2 hr = 40intact acrosomes
2. MorphologyAll semen has some abnormal spermatozoa. The purpose of examining sperm morphology is
to determine the proportion and type of sperm abnormalities. The difficult questions are: 1. What type of aberrations are truly abnormalities which contribute to infertility? 2. What level of abnormality is tolerable?The system of categorizing sperm abnormalities as primary (1o) or secondary (2o) has been
widely accepted. By definition, a primary abnormality is one that originates during spermatogenesis - within the testicle. A secondary abnormality is one that originates within the epididymis (11,12). All head abnormalities, including knobbed acrosomes, microcephalic sperm, pyriform heads, nuclear vacuoles etc., would thus be primary. Some tail abnormalities, notably the Dag defect and distal midpiece reflexes develop in the epididymis and might be considered secondary. However, if these abnormalities developed in the epididymis because of a weakness in structure which occurred during spermatogenesis they should be classified as primary abnormalities. Following this line of reasoning, there would be very few secondary abnormalities.
The definitions of 1o and 2o abnormalities, based on origin, may have little to do with the seriousness of sperm abnormalities with regard to the usefulness of the semen, but more often tells much about the health of a bull's testicles. These definitions would serve well for the evaluation of breeding soundness of bulls. In frozen semen evaluation, when we are attempting to determine the quality of frozen semen for use in single-ovulating or superovulating females, we may not be very interested in a particular bull's semen production capability, but rather in whether the type and number of sperm abnormalities pose any problem to fertility. Many AI centers categorize sperm abnormalities as 1o, 2o and tertiary (3o) based on " location (type)" rather than "origin"; thus, head abnormalities are primary, proximal protoplasmic droplets are secondary and tail defects are tertiary (13). Since information regarding the significance to fertility for specific sperm abnormalities within categories is incomplete, the categories do not necessarily denote seriousness.
Another system devised by Blom classifies sperm abnormalities as "major" if they have been associated with infertility and "minor" if they have not been associated with infertility (12,14). In general, it has been empirically accepted that primary or major abnormalities should not exceed 15 to 20 percent for a satisfactory classification. The tolerable level of secondary or minor abnormalities has never been very clear, however, it is generally accepted that at least 70 of cells should be normal. In general, a certain number of live normal spermatozoa must be inseminated in order to optimize the possibility of a spermatozoon finding the ovum, penetrating the zona pellucida and fertilizing the ovum. More spermatozoa than this number should not result in any further improvement in fertility. This concept is somewhat complicated by the proportion of abnormal spermatozoa that can penetrate the zona pellucida of an ovum, thereby causing a zona block to other normal sperm, but are unable to initiate or sustain embryonic development. For example, if a semen had 20diadem defects, it would make no difference to fertility whether 10 million, 100 million or a billion cells were inseminated because the chance of an abnormal sperm initiating a zona block would always be 20 On the other hand, spermatozoa unable to penetrate the zona pellucida, such as those with knobbed acrosomes or bent tails, would be unable to block normal spermatozoa from fertilizing the ovum. It has shown that the cervix and uterotubal junction act as "filters" to some types of abnormal spermatozoa (15,16). Abnormal spermatozoa which are not transported to the oviduct and those that are transported, but are not capable of penetrating the zona pellucida, may be compensated for by increasing the sperm

numbers inseminated ("compensable defects"). Abnormal sperm that are not "filtered" and are able to initiate a zona block cannot be compensated for ("non-compensable") (17). Classification of sperm defects as compensable and non-compensable would be particularly well suited to artificial insemination since the number of spermatozoa inseminated is controlled and the semen is delivered into the uterus. However, at this point, a great deal of research is necessary to determine to what extent the many different abnormalities are compensable or uncompensable. On the other hand, due to a lack of strong research support, there is controversy and many assumptions are currently being made with regard to the significance of sperm abnormalities classified as primary and secondary or major and minor. In this regard, one could argue equally in favor of using a system based on a compensable-uncompensable classification based on limited data and theory. Thus, until clarification is provided by further research it is suggested that non-compensable abnormalities should not exceed 15-20 as previously suggested for "primary" or "major" abnormalities and at least 70of all spermatozoa should be normal.
The examination of sperm morphology must always be done at a magnification of 1000 X. Morphology may be examined in wet mounts using phase contrast or DIC. These methods tend to be more tedious than those using stained smears because in wet mounts, usually the entire spermatozoon under scrutiny is not within one focal plane and frequent focal adjustments are necessary for each sperm examined. It is the opinion of the author that two staining methods should be routinely employed in every examination of morphology. A morphology stain such as the eosin-nigrosin stain, which has no washing steps, is essential because everything that is in semen will show up on the smear. The Feulgen staining method for DNA allows closer scrutiny of nuclear defects such as vacuolation and abnormality in shape. Semen which is extended in milk usually cannot be adequately examined for morphology with eosin-nigrosin stain because the milk fat globules obscure the spermatozoa. The process of Feulgen staining removes the fat globules allowing a clear visualization of sperm. The Feulgen technique is as follows:1. Allow semen smears to dry at least 6-24 hours to prevent the loss of sperm from the slide during washing.2. Place slides into 5 N HCl for 30 minutes.3. Wash slides by running water into the corner of a staining dish containing the slides for 30 seconds.4. Place slides into Schiff's reagent for 45 minutes.5. Wash as in step 3 and allow to dry.6. Examine under oil at 1000 X magnification with phase contrast.
A differential count of 100 cells is satisfactory when there are few sperm abnormalities. When a large number of sperm defects are present 300 to 500 cells may need to be counted in order to obtain an accurate spermiogram.
3. Number of Motile Spermatozoa Per DoseEarlier workers have established the generally accepted AI industry standard of 10 million
motile spermatozoa per dose immediately after thawing (18). In bulls of lower fertility, improvement in fertility may occur with an increase in dose (19). Usually, the minimum number of normal motile spermatozoa per dose is determined by AI centers based on an individual bull's performance in the field. Semen from highly fertile bulls may perform well when as low as 4 million motile sperm immediately after thawing are inseminated.
The method of counting the number of sperm cells per dose, for most veterinarians, would be done with a hemacytometer. Some veterinarians may have access to a laboratory with a automated equipment (20,21); however, the accuracy of hemacytometer counts is comparable when a meticulous

technique is used. Accuracy can be improved by repeating counts and this should be done in cases where the number of sperm cells per dose is found to be unacceptably low.
References1. Saacke RG, Nebel RL, Karabius DS, Bame JH, Mullins J. Sperm transport and accessory sperm evaluation. Proc 12th Tech Conf Artif Insem Reprod. The National Association Of Animal Breeders, Columbia, p7-14, 1988.2. Hawk HW, Conley HH, Wall RJ, Whitaker RO. Fertilization rates in superovulating cows after deposition of semen on the infundibulum, near the uterotubal junction or after insemination with high numbers of sperm. Theriogenology 29: 1131-1142, 1988.3. The National Association Of Animal Breeders Technical Committee. Laboratory tests for evaluating bovine semen. Proc 11th Tech Conf Artif Insem Reprod. The National Association Of Animal Breeders, Columbia, p102-104, 1986.4. Barth AD, Bowman PA. Determination of the best practical method of thawing bovine semen. Can Vet J 29: 366-369, 1988.5. Pickett BW, MacDonald WA, Gosslee DG, Cowan WA. Correlation between certain laboratory tests and fertility of frozen bovine spermatozoa. J Dairy Sci 44:1134 -1140, 1961.6. Saacke RG, White JM. Semen quality tests and their relationship to fertility. Proc 2nd Tech Conf Artif Insem Reprod. The National Association Of Animal Breeders, Columbia, p22-27, 1972.7. Johnson L, Berndtson WE, Pickett BW. An improved method for evaluating acrosomes of bovine spermatozoa. J An Sci 42: 951-954, 1976.8. Watson PF. Use of a giemsa stain to detect changes in acrosomes of frozen ram spermatozoa. Vet Rec 97: 12-15, 1975.9. Wells ME, Awa DA. New technique for assessing acrosomal characteristics of spermatozoa. J Dairy Sci 53: 227-232, 1970.10. Oettle EE. Using a new acrosome stain to evaluate sperm morphology. Vet Med 81: 263-266, 1986.11. Anderson J. Investigations on the semen of fertile and sterile bulls.
The Veterinary Journal 95: 457-473, 1939.12. Blom E. Sperm morphology with reference to bull infertility. First All India Symp Anim Reprod, Ludhiana, p.61-81, 1977.13. Mitchell JR, Hanson RD, Fleming WN. Utilizing differential interference contrast microscopy for evaluating abnormal spermatozoa. Proc 7th Tech Conf Artif Insem Reprod, The National Association Of Animal Breeders, Columbia, p 64-67, 1978.14. Blom E. Ultrastrukturen af nogle karakteristiske spermiedefekter og forslag til et nyt klassificerings-system for tyrens spermiogram. Nord Vet Med 25: 383-391, 1973.15. Karabinus DS, Saacke RG. Selection of spermatozoa across the bovine cervix.
J Dairy Sci 70 (Suppl. 1): 248,1987.16. Mitchell JR, Senger PL, Rosenberger JL. Distribution and retention of spermatozoa with acrosomal and nuclear abnormalities in the cow genital tract. J Anim Sci 61: 956-967, 1985.17. Saacke RG, Nebel DS, Karabinus JH, Mullins J. Sperm transport and accessory sperm evaluation. Proc 12th Tech Conf Artif Insem Reprod. The National Association Of Animal Breeders, Columbia, p7-14, 1988.18. Pickett BW, Berndtson WE. Preservation of bovine spermatozoa by freezing in straws: a review. J Dairy Sci 57: 1287-1301, 1974.19. Sullivan JJ. Sperm numbers required for optimum breeding efficiency in cattle. Proc 3rd Tech Conf Artif Insem Reprod. The National Association Of Animal Breeders, Columbia, p36, 1970.20. Amann RP, Hammerstedt RH. Validation of a system for computerized measurements of spermatozoal velocity and percentage of motile sperm. Biol Reprod 23: 647, 1980.21. O'Connor MT, Amann RP, Saacke RG. Comparisons of computer evaluations of spermatozoal motility with standard laboratory tests and their use for predicting fertility.
J An Sci 53: 1368-1376, 1981.
--------------------------------------
ADENITIS VESICULAR EN TOROS
Martínez M.1, Arteaga A2, Chirino-Trejo M.3, Palmer C.4, Barth A.41Instituto de Reproducción Animal Córdoba. 2Davis-Rairdan Embryo Transplants Ltd. Departments of 3Veterinary Microbiology 4Large Animal Clinical Sciences and, Western College of Veterinary Medicine, University of Saskatchewan.
IntroducciónLa enfermedad de las glándulas vesiculares en el toro ha sido una preocupación de veterinarios clínicos, produccionistas y científicos desde hace mucho tiempo. El presente manuscrito es un breve resumen de la ubicación, etiología, epidemiología, patogénesis, y posibles tratamientos de la inflamación de las glándulas. Se incluyen también un algunos trabajos realizados tendientes comparar algunas estrategias de la terapia antibiótica. Al mismo tiempo, se espera que la presentación de los resultados obtenidos sea un estímulo para continuar la investigación que permita mejorar el tratamiento, el control y la prevención de esta enfermedad en toros.
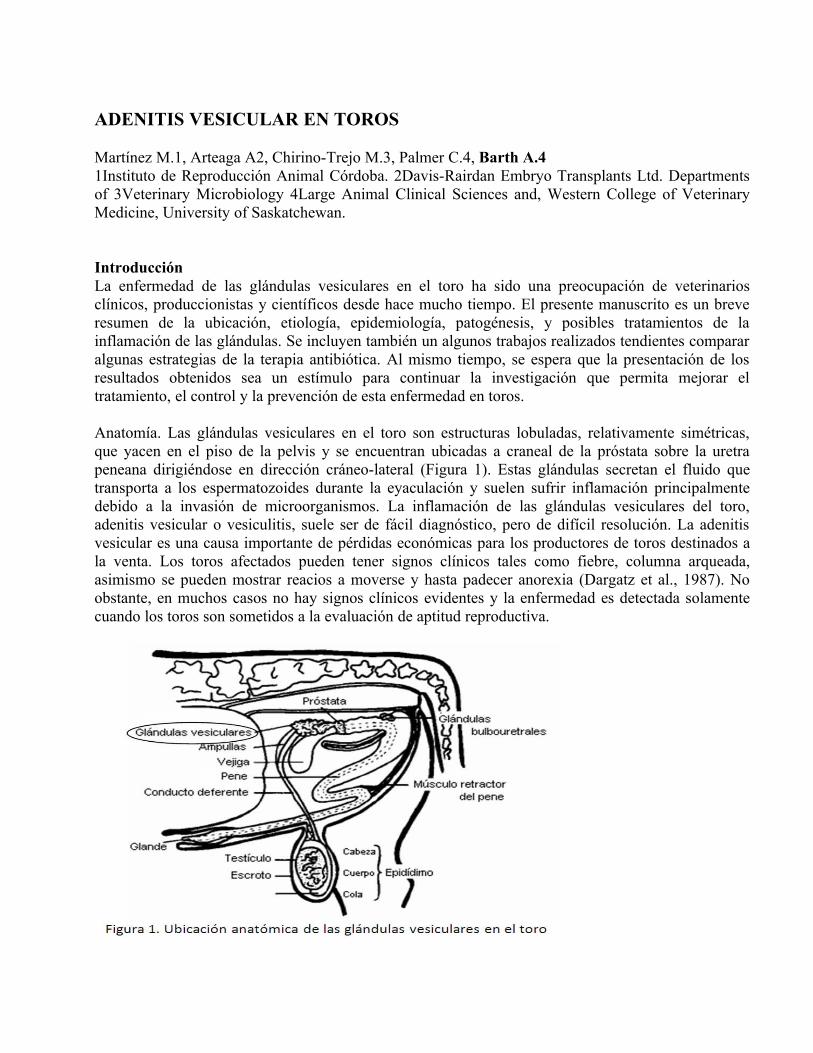
Anatomía. Las glándulas vesiculares en el toro son estructuras lobuladas, relativamente simétricas, que yacen en el piso de la pelvis y se encuentran ubicadas a craneal de la próstata sobre la uretra peneana dirigiéndose en dirección cráneo-lateral (Figura 1). Estas glándulas secretan el fluido que transporta a los espermatozoides durante la eyaculación y suelen sufrir inflamación principalmente debido a la invasión de microorganismos. La inflamación de las glándulas vesiculares del toro, adenitis vesicular o vesiculitis, suele ser de fácil diagnóstico, pero de difícil resolución. La adenitis vesicular es una causa importante de pérdidas económicas para los productores de toros destinados a la venta. Los toros afectados pueden tener signos clínicos tales como fiebre, columna arqueada, asimismo se pueden mostrar reacios a moverse y hasta padecer anorexia (Dargatz et al., 1987). No obstante, en muchos casos no hay signos clínicos evidentes y la enfermedad es detectada solamente cuando los toros son sometidos a la evaluación de aptitud reproductiva.

Epidemiología. La vesiculitis ha sido encontrada en porcentajes que varían del 0.85 al 10de los toros en las evaluaciones de fertilidad de los mismos (Cavallieri y Van Camp, 1997). En más detalle, se han publicado las prevalencias en diferentes lugares del mundo. Para comenzar el 0.85fue encontrado luego de la revisación de 2000 toros en Dinamarca (Blom and Christensen, 1965), 2.5de 7359 toros en Colorado, USA (Ball et al., 1968), 4.2 de 828 toros en Holanda (Van der Sluis, 1953), 4.6de 343 toros en New York, USA (McEntee, 1962). a prevalencia de adenitis vesicular clínica y subclínica en especímenes de matadero fue tan alta como el 49(Ball et al., 1968). Aunque la inflamación bilateral ha sido publicada, los casos unilaterales son los más comunes (Dargatz et al., 1987). En cuanto a la edad, la prevalencia ha sido reportado por Ball et al. (1968), la cual fue de 5.9en toros de un año, en un rango de 0 al 2en toros de 2 a 8 años, de 4.8en toros de 9 años y de 6.6en aquellos de ≥10 años. En Canadá es de 3en toros de un año.Etiología. Una gran variedad de microorganismos han sido asociados a la adenitis vesicular (Galloway, 1964), incluyendo numerosos tipos de bacterias, virus, mycoplasmas, ureaplasmas y chlamydias (Cavallieri y Van Camp, 1997). En lugares donde la brucelosis no ha sido controlada, Brucella abortus es la causa primaria de adenitis vesicular. Arcanobacterium pyogenes es uno de los microorganismos aislados más frecuentemente (Carroll et al., 1968; Hoover, 1979; Dargatz, 1987; Phillips, 1993; Mickelsen et al., 1994; Cavallieri y Van Camp, 1997; Carson, 2000). Histophilus somni también ha sido aislado de toros con adenitis vesicular durante revisaciones de rutina (Grotelueschen et al., 1994).Patogénesis. En la literatura se han publicado diferentes teorías sobre la patogénesis de esta enfermedad. Sin embargo, estas teorías aún no han sido totalmente demostradas (Cavallieri y Van Camp, 1997). Las diversas hipótesis planteadas por diferentes autores hablan de la infección de las glándulas vesiculares ocurriendo potencialmente mediante el ascenso por el tracto genito-urinario, por el descenso desde el tracto urinario o reproductivo superior, por vía hematógena o por la invasión directa desde algún órgano cercano, mientras que las anomalías congénitas predisponen a la ocurrencia de la enfermedad.1) Infección ascendente. La ruta de ascenso por la uretra no sería posible ya que la misma es frecuentemente lavada durante la micción. Cuando se intentó la reproducción de adenitis vesicular por instilación repetida de Arcanobacterium pyogenes profundamente en la uretra peneana no se pudo conseguir el objetivo deseado (Galloway, 1964). El único microorganismo que se supone que asciende por la uretra y que fue aislado en las glándulas vesiculares ha sido Tritrichomonas foetus (Cavallieri y Van Camp, 1997); pero se deberìa tener en cuenta que éste es un parásito con movilidad propia.2) Infección descendente. La ruta de descenso es posible ya que la adenitis vesicular se ha encontrado como patología secundaria a pielonefritis, epididimitis u orquitis. En los casos de adenitis vesicular causada por A. pyogenes, otras partes del tracto reproductivo también se encontraron afectadas (Dargatz et al., 1987; Cavallieri y Van Camp, 1997).3) Vía hematógena. En un estudio postmortem, se encontró que el 50de los toros con adenitis vesicular habían tenido problemas de salud no reproductivos tales como endocarditis vegetativa, broncopneumonía crónica, poliartritis, y reticuloperitonitis traumática (Linhart y Parker, 1988). Por lo que todas estas condiciones pueden ser la fuente hematógena de infección de las glándulas vesiculares. También, la adenitis vesicular ha sido asociada a la alimentación con dietas de alta energía (Cavalieri y Van Camp, 1997). Muchos toros, especialmente aquellos de un año y en preparación para la venta o para exposiciones, son mantenidos con raciones similares a aquellas de animales de “feedlot”. En este caso, la infección de las glándulas sería el resultado de una bacteriemia secundaria a rumenitis. Es preciso recordar que los aislamientos bacterianos más comunes de abscesos hepáticos en animales de “feedlot” son aquellos en los que A. pyogenes y/o bacteria gram-negativas
anaeróbicas están presentes. Por lo tanto, debido a que A. pyogenes es el microorganismo más comúnmente obtenido de las infecciones de las glándulas vesiculares, debe debería considerarse una infección “metastásica” de las glándulas.4) Anomalías congénitas. Si bien éstas pueden representar una pequeña proporción de animales, pueden ser causas predisponentes de vesiculitis y jugar un papel importante de la patogénesis de esta enfermedad. Las anomalías congénitas de los túbulos de las glándulas vesiculares y de los colículos seminales fueron observadas en toros con vesiculitis (Blom, 1979a, b). Entre otros elementos que predisponen a la infección y la enfermedad, se halla la oclusión de los conductos grandes de las glándulas vesiculares por acumulación de material proteináceo y residuos epiteliales causando una distensión de los alvéolos glandulares (Ball et al., 1968).Tratamiento. Hay evidencia que algunos toros se recuperan espontáneamente de esta enfermedad, especialmente los toros jóvenes (Larson, 1997). Existen dos tipos de tratamiento, uno quirúrgico y otro médico. Muchos intentos quirúrgicos de remoción glandular han sido publicados; no obstante, no han tenido un resultado aceptable para glándulas fibrosadas al tejido adyacente (Hooper et al., 1994), ya que hubo problemas en la viabilidad del semen después de la congelación (Hoover et al., 1979). El tratamiento médico es el más usado. Este incluye la terapia con antibióticos, anti-inflamatorios no esteroidales, etc. (Cavalieri y Van Camp, 1997). Pero el método más común es la inyección parenteral de antibióticos, que ha tenido resultados variables (Phillips, 1993). Además, ha habido publicaciones anecdóticas a cerca de la inyección intraglandular de agentes esclerosantes (Hoover, 1974). Sin embargo, el uso intraglandular de antibióticos no ha sido publicado todavía.Al presente, no hay publicaciones que comparen las tasas de casos de adenitis vesicular clínica tratados con aquellas de no tratados. Sin embargo, algunos casos clínicos reportados indican una tasa de recuperación muy pobre luego del tratamiento con antibióticos aún cuando las bacterias aisladas fueron sensitivas al antibiótico elegido (Phillips, 1993). Parece ser que los métodos de tratamiento de rutina no resultan en niveles tisulares de antibióticos suficientes como para inhibir el crecimiento bacteriano. En general, las recomendaciones para elegir un antibiótico para el tratamiento de adenitis vesicular (Phillips, 1993; Cavalieri and Van Camp, 1997; Hooper et al., 2002) han derivado de estudios de próstata en humanos (Winningham et al., 1968). Estas recomendaciones son una serie de propiedades, tales como una alta solubilidad en lípidos, un pKa favorable, baja unión a proteínas y un pH más alcalino que el del fluido seminal (Cavalieri and Van Camp, 1997). De esta manera, se ha usado la eritromicina, trimetoprim, o gentamicina por largos periodos de tiempo, pero con resultados inciertos (Phillips et al., 1993).
Estudios sobre tratamiento de la adenitis vesicularEn las siguientes secciones del presente manuscrito se incluyen experimentos de concentración plasmática y tisular de antibióticos y tratamientos antibióticos parenterales o intraglandulares en toros sanos o afectados con vesiculitis.
Concentración de antibióticos en plasma y glándulasComo se dijo anteriormente, los tratamientos con antibióticos para la adenitis vesicular han tenido una eficacia variable. La falta de efectividad cuando se conoce que las bacterias aisladas son sensitivas al tratamiento usado puede ser debido a una inadecuada distribución del antibiótico en el tejido. Al respecto, se diseñaron dos experimentos con el objetivo de comparar la inhibición de crecimiento bacteriano in-vitro por concentraciones de antibióticos en plasma o en tejido glandular luego de la administración parenteral de algunos antibióticos comúnmente usados (Prescott, 2002a, b, c, d). En el Experimento 1, toros Hereford (2-3 años; peso = 703.9 ± 24.8 kg; n=25) fueron aleatoriamente asignados a grupos de tratamiento para recibir ceftiofur (1 mg/kg IM), florfenicol (20 mg/kg IM), oxitetraciclina (20 mg/kg IM; control negativo), penicilina G procaínica (22000 IU/kg IM) o

tilmicosin (10 mg/kg SC). Se colectaron muestras de sangre inmediatamente antes (0 h), 6 y 12 h después del tratamiento. En el Experimento 2, los mismos toros fueron ubicados al azar en cuatro grupos para recibir ceftiofur, penicilina, tilmicosin o para no recibir tratamiento (control). Las dosis y rutas de administración fueron como en el Experimento 1. Se tomaron muestras de sangre y biopsias de las glándulas vesiculares entre 6 y 12 h después del tratamiento. Bacterias que habían sido aisladas de toros afectados con adenitis vesicular (Histophilus somni y Arcanobacterium pyogenes cepas 901359 y 662141), y de conocida sensibilidad a los antibióticos usados (excepto oxitetraciclina), fueron expuestas a plasma y/o extracto de tejido glandular en cultivo in-vitro. En Experimento 1, la penicilina plasmática a las 6 y 12 h resultó en la mayor inhibición de todas las bacterias y correspondió al número más alto de toros (P-0.05; Tabla 1). La concentración plasmática de ceftiofur a las 6 y 12 h inhibió el crecimiento de H. somni, mientras que la de tilmicosin inhibió el crecimiento de A. pyogenes cepa 901359. El florfenicol y la oxitetraciclina (control negativo) no inhibieron el crecimiento bacteriano in vitro. En el Experimento 2 (Tabla 2), la penicilina plasmática pero no la penicilina del tejido glandular inhibió el crecimiento bacteriano. Mientras que las concentraciones plasmáticas y tisulares de tilmicosin inhibieron el desarrollo de ambas cepas de A. pyogenes (P-0.05). Estos resultados favorecerían al tilmicosin como antibiótico de elección para el tratamiento de la adenitis vesicular en toros.
Tabla 1. Número de muestras de plasma tomadas 6 a 12 h después del tratamiento de toros previamente tratados con ceftiofur, florfenicol, oxitetraciclina, penicilina o tilmicosin (Hora 0) que inhibieron el desarrollo in-vitro de H. somni o A. pyogenes cepas 901359 y 662141.
abc Valores con diferentes superíndices dentro de las columnas difieren (P - 0.001).Nota: el número de toros fue cinco en cada grupo de tratamiento. La oxitetraciclina fue considerada como control negativo.
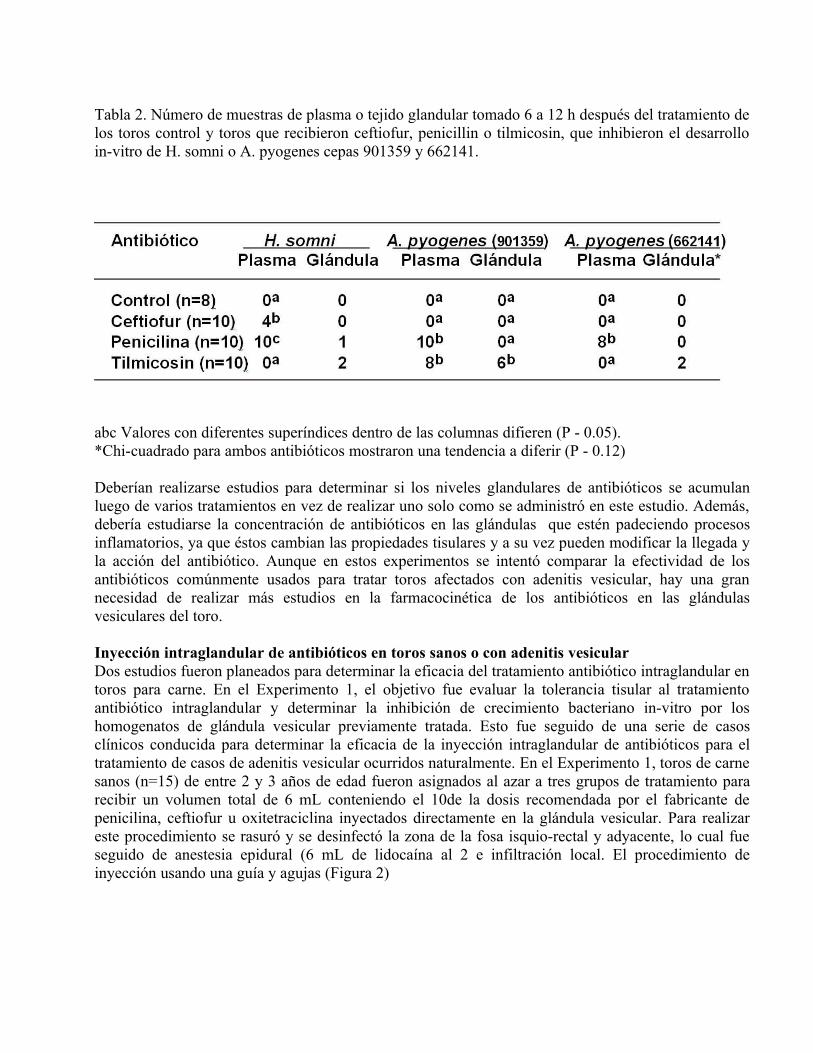
Tabla 2. Número de muestras de plasma o tejido glandular tomado 6 a 12 h después del tratamiento de los toros control y toros que recibieron ceftiofur, penicillin o tilmicosin, que inhibieron el desarrollo in-vitro de H. somni o A. pyogenes cepas 901359 y 662141.
abc Valores con diferentes superíndices dentro de las columnas difieren (P - 0.05).*Chi-cuadrado para ambos antibióticos mostraron una tendencia a diferir (P - 0.12)
Deberían realizarse estudios para determinar si los niveles glandulares de antibióticos se acumulan luego de varios tratamientos en vez de realizar uno solo como se administró en este estudio. Además, debería estudiarse la concentración de antibióticos en las glándulas que estén padeciendo procesos inflamatorios, ya que éstos cambian las propiedades tisulares y a su vez pueden modificar la llegada y la acción del antibiótico. Aunque en estos experimentos se intentó comparar la efectividad de los antibióticos comúnmente usados para tratar toros afectados con adenitis vesicular, hay una gran necesidad de realizar más estudios en la farmacocinética de los antibióticos en las glándulas vesiculares del toro.
Inyección intraglandular de antibióticos en toros sanos o con adenitis vesicularDos estudios fueron planeados para determinar la eficacia del tratamiento antibiótico intraglandular en toros para carne. En el Experimento 1, el objetivo fue evaluar la tolerancia tisular al tratamiento antibiótico intraglandular y determinar la inhibición de crecimiento bacteriano in-vitro por los homogenatos de glándula vesicular previamente tratada. Esto fue seguido de una serie de casos clínicos conducida para determinar la eficacia de la inyección intraglandular de antibióticos para el tratamiento de casos de adenitis vesicular ocurridos naturalmente. En el Experimento 1, toros de carne sanos (n=15) de entre 2 y 3 años de edad fueron asignados al azar a tres grupos de tratamiento para recibir un volumen total de 6 mL conteniendo el 10de la dosis recomendada por el fabricante de penicilina, ceftiofur u oxitetraciclina inyectados directamente en la glándula vesicular. Para realizar este procedimiento se rasuró y se desinfectó la zona de la fosa isquio-rectal y adyacente, lo cual fue seguido de anestesia epidural (6 mL de lidocaína al 2 e infiltración local. El procedimiento de inyección usando una guía y agujas (Figura 2)

se realizó en la fosa isquio-rectal, como se puede apreciar en la Figura 3.
Las bacterias usadas en este experimento fueron resistentes a oxitetraciclina, por lo tanto, los toros tratados con clorhidrato de oxitetraciclina fueron considerados como controles negativos. Una biopsia de la glándula fue tomada entre las 6 y 12 h después del tratamiento antibiótico. Se realizó ecografía antes, inmediatamente después y a las 24, 48 y 168 h después de la inyección intraglandular. El tamaño y dureza de la glándula vesicular que recibió oxitetraciclina fueron mayores (P-0.01) que en aquellas que recibieron ceftiofur (Figura 4). Las muestras de glándulas vesiculares de toros tratados con ceftiofur resultaron en la inhibición de desarrollo bacteriano (H. somni) en 2 de 5 toros y la penicilina resultó en la inhibición del crecimiento de todas las bacterias en sólo un toro y de H. somni y A. pyogenes (901359) en otro. El nivel de intensidad de píxeles aumentó significativamente (P-0.01) después del tratamiento con antibióticos, especialmente después del tratamiento con oxitetraciclina o penicilina (Figura 5).

Figura 4. Gráfico “box-plot” del volumen de las glándulas vesiculares siete días después del tratamiento intraglandular con ceftiofur, oxytetraciclina o penicilina in toros de carne sanos. El grupo Control es representado por aquellas glandulas que no recibieron tratamiento. X representa los “outliers” (datos que están más allá de dos desvíos estándar de la media) de acuerdo con el programa estadístico SPSS. Las cajas están compuestas por el primero y el tercer cuartil mientras que los puntos de arriba y abajo de las líneas centrales representan los valores mínimo y máximo.
Figure 5. Porcentaje de cambio de la intensidad e píxel promedio respecto a la ecografía de cada toro realizada al comienzo del experimento.

En una serie de casos clínicos, toros de un año de edad con adenitis vesicular clínica (n=14) fueron remitidos al Western College of Veterinary Medicine (Universidad de Saskatchewan) para ser tratados. Ocho toros tenían adenitis vesicular unilateral y seis tenían adenitis vesicular bilateral. La bacteria más comúnmente aislada fue Arcanobacterium pyogenes, mientras que otro hallazgo fue Corynebacterium pseudotuberculosis en un toro (Tabla 3). Los toros fueron sujetos a palpación rectal y ecografía de las glándulas vesiculares, seguidas de colección de semen por electroejaculación y tratamiento intraglandular con ceftiofur (n=13) y de ser necesario, un segundo tratamiento con penicilina (n=6). Un toro recibió sólo una inyección intraglandular inicial de penicilina. Los toros fueron evaluados una vez por semana durante 6 semanas por palpación de las glándulas, evaluación macro y microscópica del semen y cultivo bacteriológico del semen. Todos los toros se recuperaron de la adenitis vesicular luego de 3 ó 6 semanas.Hubo una diferencia significativa entre colecciones en la cantidad de pus (P=0.042), leucocitos (P-0.001) y sangre (P=0.003) presentes en los eyaculados de las muestras antes del tratamiento y las muestras de semen tomadas 3 semanas después del mismo (Figura 6). La distribución de la intensidad de píxeles en las imágenes ecográficas de las glándulas sanas o afectadas, ya sea tratadas o no, no cambiaron con el paso del tiempo. No se encontró efecto del estado de salud de la glándula (enferma o sana), tiempo (días de recuperación), o de la interacción estado de salud por tiempo en el nivel de intensidad de píxel promedio (P=0.3, P=0.46, y P= 0.64, respectivamente) o en heterogeneidad de imagen (P=0.16, P=0.77, y P= 0.20, respectivamente). La inyección intraglandular de ceftiofur vía fosa isquio-rectal fue muy efectiva para el tratamiento de la adenitis vesicular en los toros de carne estudiados.
Tabla 3. Bacterias aisladas de toros jóvenes (alrededor de un año de edad) afectados con adenitis vesicular1.
.Toro No Principal aislamiento Aislamiento concomitante----------------------------------------------------------------------------------------------------------------1 Arcanobacterium pyogenes Corynebacterium sp., Pasteurela sp.2 Acinetobacter sp.3 Corynebacterium sp. Pasteurella sp.4 Corynebacterium pseudotuberculosis Corynebacterium sp.5 Acinetobacter sp.6 Streptococcus sp.7 Arcanobacterium pyogenes Corynebacterium sp., Bacilos G (-)8 Bacilos G (-)9 Arcanobacterium pyogenes Bacilos G (-)10 No hubo aislamiento11 No hubo aislamiento12 No hubo aislamiento13 Bacilos G (-)14 Arcanobacterium pyogenes------------------------------------------------------------------------------------------------------------------Todas las bacterias fueron sensitivas a ceftiofur, florfenicol, oxitetraciclina, penicilina y tilmicosin. Una cepa aislada de A. pyogenes (Toro No. 1) y una cepa de Corynebacterium sp. (Toro No. 3) fueron resistentes y parcialmente resistentes a enrofloxacin, respectivamente, mientras que una cepa de A. pyogenes (Toro No. 14) fueron parcialmente resistente a enrofloxacina y tetraciclina.
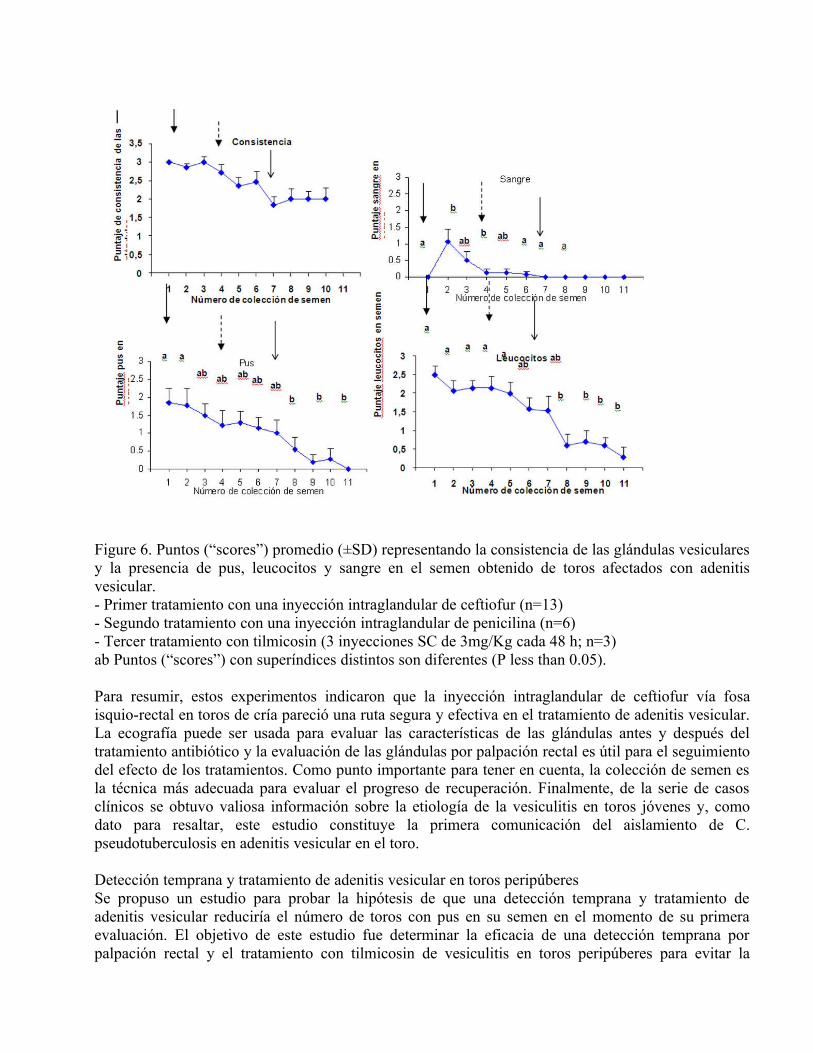
Figure 6. Puntos (“scores”) promedio (±SD) representando la consistencia de las glándulas vesiculares y la presencia de pus, leucocitos y sangre en el semen obtenido de toros afectados con adenitis vesicular.- Primer tratamiento con una inyección intraglandular de ceftiofur (n=13)- Segundo tratamiento con una inyección intraglandular de penicilina (n=6)- Tercer tratamiento con tilmicosin (3 inyecciones SC de 3mg/Kg cada 48 h; n=3)ab Puntos (“scores”) con superíndices distintos son diferentes (P less than 0.05).
Para resumir, estos experimentos indicaron que la inyección intraglandular de ceftiofur vía fosa isquio-rectal en toros de cría pareció una ruta segura y efectiva en el tratamiento de adenitis vesicular. La ecografía puede ser usada para evaluar las características de las glándulas antes y después del tratamiento antibiótico y la evaluación de las glándulas por palpación rectal es útil para el seguimiento del efecto de los tratamientos. Como punto importante para tener en cuenta, la colección de semen es la técnica más adecuada para evaluar el progreso de recuperación. Finalmente, de la serie de casos clínicos se obtuvo valiosa información sobre la etiología de la vesiculitis en toros jóvenes y, como dato para resaltar, este estudio constituye la primera comunicación del aislamiento de C. pseudotuberculosis en adenitis vesicular en el toro.
Detección temprana y tratamiento de adenitis vesicular en toros peripúberesSe propuso un estudio para probar la hipótesis de que una detección temprana y tratamiento de adenitis vesicular reduciría el número de toros con pus en su semen en el momento de su primera evaluación. El objetivo de este estudio fue determinar la eficacia de una detección temprana por palpación rectal y el tratamiento con tilmicosin de vesiculitis en toros peripúberes para evitar la

presencia de pus en su semen en el momento de su primera evaluación, y a la vez reducir el número de toros de un año descartados al momento de su primera evaluación de calidad seminal. Toros (n=2207) de 15 razas (Tabla 4) en 17 estaciones de prueba fueron examinados por palpación rectal a los 9-14 meses de edad y ubicados en tres grupos de tratamiento: (1) Grupo tratado positivo (toros con vesiculitis a la palpación) que recibió tres inyecciones subcutáneas de tilmicosin cada 48 h, (2) Grupo control no tratado positivo (con vesiculitis), y (3) Grupo control no tratado negativo (sin vesiculitis). Se realizó palpación rectal de las glándulas nuevamente al momento de la evaluación de semen, antes de la venta de los toros, entre los 28 y 70 días (media = 42.8 d) después del primer examen. El semen fue evaluado bajo microscopio óptico para determinar la presencia de pus y/o leucocitos.
Tabla 4. Razas de toros con adenitis vesicular detectada por palpación rectal que fueron asignadas a recibir un tratamiento antibiotico que consistió en una inyección subcutánea de tilmicosin (1 mL/30Kg) administrado tres veces cada 48 h.
Raza Número de toros Afectados--------------------------------------------------------------------------
Angus Negro 316 22Beef Booster 693 5Blonde D'Aquitaine 13 0Charolais 198 11Gelbvieh 38 1Hay Converters 2 0Hereford 27 0Limousin 38 0Maine Anjou 23 2Red Angus 737 47Salers 5 0Shorthorn 32 5Simmental 75 3South Devon 3 0Speckled Park 7 1
La proporción de toros con vesiculitis fue de 4.4(97/2207). Al momento de la evaluación de semen pre-venta, el número de toros con vesiculitis había disminuido a 1.3(29/2207); sin embargo, 7 de éstos fueron nuevos casos que se desarrollaron después del primer examen. Sólo 22 de los 97 casos permanecieron positivos o con vesiculitis. Por lo tanto, hubo una tasa de recuperación de 75/97 (77.3 en el grupo de toros original positivo a vesiculitis (Tabla 5). Al tiempo de la prueba de semen pre-venta, no hubo diferencia en la proporción de toros con glándulas inflamadas entre toros tratados positivos (15/66) y toros no tratados positivos (7/31). Dentro de los toros positivos (Tratados y Control), hubo una diferencia significativa entre el número de toros con glándulas agrandadas y el número de toros con pus en el semen (P = 0.001), mientras que el número de toros con glándulas agrandadas y toros con presencia de leucocitos en el semen tendió a diferir (P - 0.06). Por lo que desde el punto de vista del diagnóstico, los datos que aporta la evaluación del semen tienen más valor que aquellos de la palpación.Los toros con adenitis vesicular fueron detectados entre los 9 y 14 meses de edad, lo que coincide con el tiempo de rápido desarrollo de las glándulas vesiculares y también con el momento de la
alimentación con raciones de alta energía. No todos los toros con glándulas aumentadas de tamaño tuvieron pus en el semen lo que puede indicar que las infecciones se fueron eliminando en esos toros. El examen transrectal y el tratamiento podría ser beneficioso en rodeos de toros con un riesgo incrementado de la enfermedad, como por ejemplo en toros que están siendo preparados para exposición o venta.
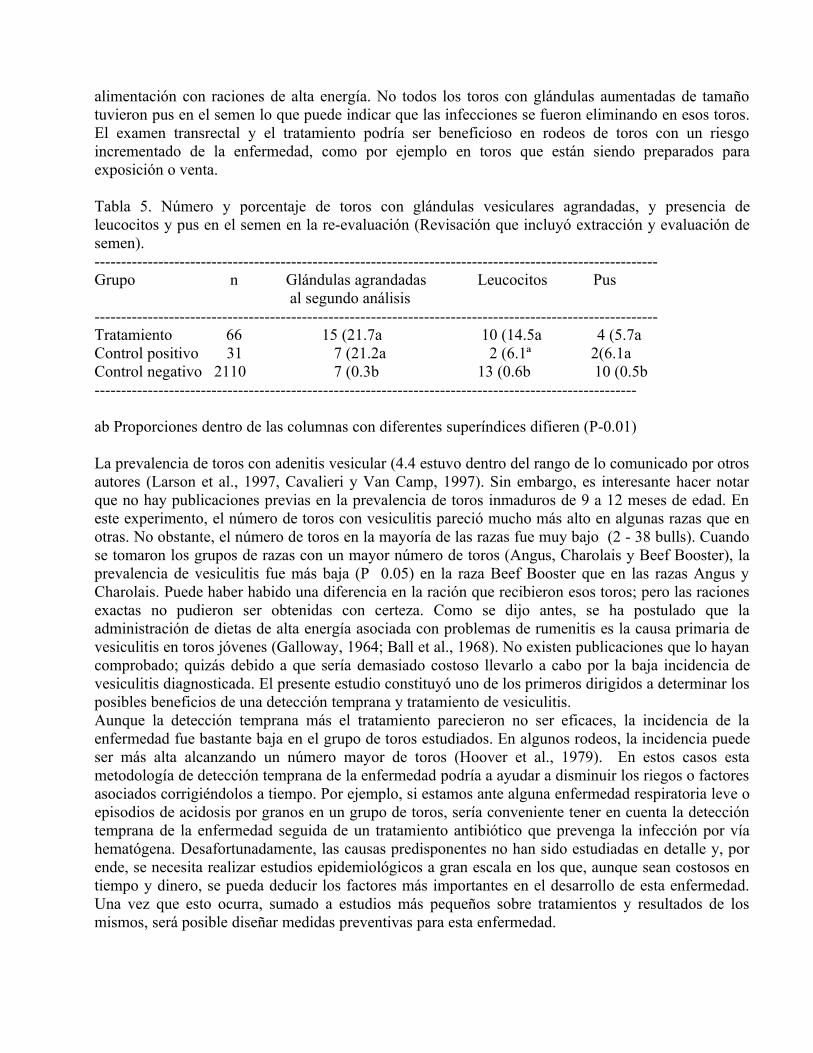
Tabla 5. Número y porcentaje de toros con glándulas vesiculares agrandadas, y presencia de leucocitos y pus en el semen en la re-evaluación (Revisación que incluyó extracción y evaluación de semen).----------------------------------------------------------------------------------------------------------Grupo n Glándulas agrandadas Leucocitos Pus
al segundo análisis----------------------------------------------------------------------------------------------------------Tratamiento 66 15 (21.7a 10 (14.5a 4 (5.7aControl positivo 31 7 (21.2a 2 (6.1ª 2(6.1aControl negativo 2110 7 (0.3b 13 (0.6b 10 (0.5b------------------------------------------------------------------------------------------------------
ab Proporciones dentro de las columnas con diferentes superíndices difieren (P-0.01)
La prevalencia de toros con adenitis vesicular (4.4 estuvo dentro del rango de lo comunicado por otros autores (Larson et al., 1997, Cavalieri y Van Camp, 1997). Sin embargo, es interesante hacer notar que no hay publicaciones previas en la prevalencia de toros inmaduros de 9 a 12 meses de edad. En este experimento, el número de toros con vesiculitis pareció mucho más alto en algunas razas que en otras. No obstante, el número de toros en la mayoría de las razas fue muy bajo (2 - 38 bulls). Cuando se tomaron los grupos de razas con un mayor número de toros (Angus, Charolais y Beef Booster), la prevalencia de vesiculitis fue más baja (P 0.05) en la raza Beef Booster que en las razas Angus y Charolais. Puede haber habido una diferencia en la ración que recibieron esos toros; pero las raciones exactas no pudieron ser obtenidas con certeza. Como se dijo antes, se ha postulado que la administración de dietas de alta energía asociada con problemas de rumenitis es la causa primaria de vesiculitis en toros jóvenes (Galloway, 1964; Ball et al., 1968). No existen publicaciones que lo hayan comprobado; quizás debido a que sería demasiado costoso llevarlo a cabo por la baja incidencia de vesiculitis diagnosticada. El presente estudio constituyó uno de los primeros dirigidos a determinar los posibles beneficios de una detección temprana y tratamiento de vesiculitis. Aunque la detección temprana más el tratamiento parecieron no ser eficaces, la incidencia de la enfermedad fue bastante baja en el grupo de toros estudiados. En algunos rodeos, la incidencia puede ser más alta alcanzando un número mayor de toros (Hoover et al., 1979). En estos casos esta metodología de detección temprana de la enfermedad podría a ayudar a disminuir los riegos o factores asociados corrigiéndolos a tiempo. Por ejemplo, si estamos ante alguna enfermedad respiratoria leve o episodios de acidosis por granos en un grupo de toros, sería conveniente tener en cuenta la detección temprana de la enfermedad seguida de un tratamiento antibiótico que prevenga la infección por vía hematógena. Desafortunadamente, las causas predisponentes no han sido estudiadas en detalle y, por ende, se necesita realizar estudios epidemiológicos a gran escala en los que, aunque sean costosos en tiempo y dinero, se pueda deducir los factores más importantes en el desarrollo de esta enfermedad. Una vez que esto ocurra, sumado a estudios más pequeños sobre tratamientos y resultados de los mismos, será posible diseñar medidas preventivas para esta enfermedad.
Los autores de este manuscrito agradecen la colaboración de L. Brito, Fei Huang, y a todo el personal de Animal Care and Goodale Research Farm, University of Saskatchewan, así como también a todos los veterinarios que colaboraron con los distintos estudios descriptos en el presente manuscrito. References
Ball, L., Young, S., Carroll, E.J., 1968. Seminal vesiculitis syndrome, lesions in genital organs of young bulls. Am. J. Vet. Res. 29, 1173-1184.Blom E., 1979a. Studies on seminal vesiculitis in the bull. I. Semen examination methods and post mortem findings. Nord. Vet. Med. 31, 193-205.Blom E., 1979b. Studies on seminal vesiculitis in the bull. II. Malformation of the pelvic genital organs as a possible predisposing factor in the pathogenesis of seminal vesiculitis. Nord. Vet. Med. 31, 241-250.Blom E. Christensen N.O., 1965. Seminal vesiculitis in the bull caused by Corynebacterium pyogenes. Nord. Vet.-Med. 17: 435-445.Carroll, E.J., Ball, L., Young, S., 1968. Seminal vesiculitis in young beef bulls. J. Am. Vet. Med. Assoc. 152, 1749-1757.Carson, R.L., 2000. Diseases of the male internal genitalia. Current Veterinary Therapy, Food Animal Practice. Ed by H. Smith, W Saunders Co., PA USA. Pp 602-603.Cavallieri, J., Van Camp, S.D. 1997. Bovine seminal vesiculitis. A review and update. Vet. Clin. North Am. Food. Anim. Pract. 13, 233-241.Dargatz, D.A., Mortimer, R.G., Ball, L., 1987. Vesicular adenitis of bulls, a review. Theriogenology 28, 513-521.Galloway, D.B., 1964. A study of bull with the clinical signs of seminal vesiculitis. Acta Vet. Scand. 5 (Suppl. 2), 1-122.Grotelueschen, D.M., Mortimer, R.G., Ellis, R.P. 1994. Vesicular adenitis syndrome in beef bulls. J. Am. Vet. Med. Assoc. 205, 874-877.Harris, F.W., Janzen, E.D., 1989. The Haemophilus somni disease complex, a review. Can. Vet. J. 30, 816-822.Hooper, R.N., Blanchard, T.L., Varner, D.D., 2002. Male reproductive disorders. In: Smith, B.P. (Ed.), Large animal internal medicine. 3rd Ed, Mosby, St Louis, pp. 1343-1344.Hooper, R.N., Taylor, T.S., Blanchard, T.L., Schumacher, J., Edwards, J.F., 1994. Ventral pararectal approach to the seminal vesicles of bulls. J. Am. Vet. Med. Assoc. 205, 596-599.Hoover, T.R., 1979. Bacterial seminal vesiculitis in bulls. Proceedings of the Society for Theriogenology, Mobile, Alabama, USA, pp. 92-98.Larson, L.L., 1986. Examination of the reproductive system of the bull. In: Morrow, D.A. (Ed.), Current Therapy in Theriogenology, W.B. Saunders Co., Philadelphia, pp.101-116.Linhart, R.D., Parker W.G., 1988. Seminal vesiculitis in bulls. Comp. Cont. Educ. 10, 1428-1432.McEntee K. 1962. Seminal vesiculitis in the bull. Proc. US Livestock San A., 66:160-167.Mickelsen, W.D., Weber, J.A., Memon, M.A., 1994. Use of transrectal ultrasound for the detection of seminal vesiculitis in a bull. Vet. Rec. 135, 154-155.Phillips, P.E., 1993. Seminal vesiculitis, New strategies for an old problem. Proceedings of the Society for Theriogenology Jacksonville, Florida, USA, pp. 59-66.Prescott, J.F., 2002a. Beta-lactam antibiotics, Cephalosporins and cephamycins. In: Prescott, J.F., Baggott, J.D., Walker, R.D. (Ed.), Antimicrobial therapy in veterinary medicine. 3rd Edition. Iowa State University Press, Ames, USA, pp. 134-159.
Prescott, J.F., 2002b. Beta-lactam antibiotics, Penam penicillins. In: Prescott, J.F., Baggott, J.D., Walker, R.D. (Ed.), Antimicrobial therapy in veterinary medicine. 3rd Ed., Iowa State University Press, Ames, USA, pp. 105-133.Prescott, J.F., 2002c. Chloramphenicol, thiamphenicol, and florfenicol In: Prescott, J.F., Baggott, J.D., Walker, R.D. (Ed.), Antimicrobial therapy in veterinary medicine. 3rd Ed., Iowa State University Press, Ames, USA, pp. 263-274.Prescott, J.F., 2002d. Lincosamides, macrolides, and pleuromutilins. In: Prescott, J.F., Baggott, J.D., Walker, R.D. (Ed.), Antimicrobial therapy in veterinary medicine, 3rd Ed., Iowa State University Press, Ames, USA, pp. 229-262.Van der Sluis L. 1953. Experiences with the examination into herd infertility. Proc 1st World Cong. On Fertil. and Steril., 2: 703-718.Winningham, D.G., Nemoy, N.J., Stamey, T.A., 1968. Diffusion of antibiotics from plasma into prostatic fluid. Nature 219, 139-143.

UPDATE ON TREATMENT OF VESICULITIS IN BULLS
Rovay H, Barth AD, Chirino-Trejo M, Martínez MFWestern College of Veterinary MedicineUniversity of Saskatchewan, Saskatoon, SK, Canada, S7N 5B4
Abstract
Four experiments were done to determine: 1) the effectiveness of early detection and treatment of vesiculitis in bulls; 2) whether antibiotic treatment at recommended dosages will result in adequate vesicular gland tissue concentrations of antibiotics to prevent in vitro bacterial growth; 3) whether intraglandular injection of antibiotics can be a successful alternative to systemic antibiotic treatment; and 4) the effectiveness of tilmicosin versus tulathromycin for treatment of clinical vesiculitis. In Experiment 1, there was a high rate of spontaneous remission from vesiculitis detected at 9 to 12 mo of age. Furthermore, there was no advantage for early antibiotic treatment versus no treatment for bulls of this age. In Experiment 2, bacteria on agar plates were exposed to fluid extracted from vesicular gland biopsies after antibiotic treatment of normal, healthy bulls. Although inadequate concentrations of antibiotics were achieved to inhibit bacterial growth when recommended dosages of various antibiotics were administered, doubling the antibiotic dosage increased in vitro bacterial growth inhibition. In Experiment 3, relatively nonirritating antibiotics were injected directly into the glands of bulls with clinical vesiculitis, demonstrating that intraglandular injections of antibiotic could be used as a successful alternative to systemic antibiotic treatment. Experiment 4 was a clinical field trial to compare the efficacy of tilmicosin versus tulathromide at recommended dosages for the treatment of clinical vesiculitis. Although the results favored tulathromycin, both antibiotics resulted in clinical cures of vesiculitis.
Keywords: Seminal vesiculitis; Vesicular adenitis; Early detection; Antibiotics; Bulls 1. Introduction
Vesicular adenitis (vesiculitis) was detected in 0.85 to 10of yearling bulls during routine breeding soundness evaluations (BSE) [1]. However, there was a much higher incidence of clinical or subclinical vesiculitis (49 in abbatoir-derived specimens [2]. In the experience of the authors (unpublished), as many as 14 of 15 bulls on one farm were affected. A definitive pathogenesis for vesiculitis has not been determined; however, proposed routes of infection include infectious agents ascending the genito-urinary tract, agents descending from the upper urinary or reproductive tracts, hematogenous invasion, or direct invasion from local sources [3]. A hematogenous source of infection has often been favored as an explanation, since vesiculitis has been associated with high-energy diets [1]. In that regard, high-energy diets predispose to the development of rumenal acidosis, which may lead to rumenitis, followed by bacteremia. Arcanobacterium pyogenes and gram-negative anaerobic bacteria, the most common isolates from liver abscesses of feedlot animals, are also commonly isolated from vesicular gland infections [1,3]. However, bacterial and viral cultures of inflamed vesicular glands were often negative [4]. Congenital abnormalities of the ducts and vessels opening into the urethra at the colliculus seminalis [5], or a lack of synchrony in the ejaculatory process [6], may lead to reflux of semen and urine into the vesicular glands causing inflammation, but not necessarily bacterial infection. Vesiculitis has not been reported in feedlot steers that commonly suffer from rumenal acidosis and liver abscesses. Rapid development of the duct system of vesicular glands
during puberty may allow reflux of semen and urine to occur in young bulls; conversely, lack of development of the vesicular glands may spare steers from vesiculitis.
Many types of infectious agents have been isolated from inflamed vesicular glands. Although vesicular gland bacterial isolates are usually sensitive to antibiotics, anecdotal reports indicate a poor success rate for antibiotic treatment, especially with chronic vesiculitis [4]. Surgical removal of infected glands has been the final remedy for some cases. There are no reports that provide data on response to antibiotic treatment for vesiculitis in any age group of bulls. This article describes four experiments to determine the efficacy of antibiotic treatment for vesiculitis.
2. Experiment 1: Early detection and treatment of vesiculitis in bulls [7]
Nine veterinary practitioners examined 2207 bulls of 15 breeds at 17 performance test stations in western Canada. Bulls were examined by transrectal palpation at 9 to 12 mo of age and assigned to three groups as follows: 1) positive treated group, positive for vesiculitis and receiving subcutaneous injections of 1 mL/30 kg body weight of tilmicosin (Micotil, Provel/Elanco Animal Health, Guelph, ON, Canada), every second day for three treatments; 2) positive control group, positive for vesiculitis and not treated; and 3) negative control group, negative for vesiculitis and not treated. Bulls were considered to be positive for vesiculitis if one or both glands were enlarged and hardened. Transrectal palpation of the glands was done again at a pre-sale evaluation of semen 28 to 70 d (mean = 42.8 d) after the first examination. Semen was collected by electroejaculation and evaluated for the presence of pus and/or leukocytes by light microscopy. Bulls were considered to have elevated numbers of leukocytes in their semen when the average number of leukocytes was at least one per five microscope fields at a magnification of 1000X. The prevalence of vesiculitis among breeds was considered for comparison only in groups with 100 animals. The influences of location and veterinarian on the incidence of vesiculitis were analyzed by logistic regression. Proportions of bulls with vesiculitis at the first and second transrectal examinations was compared among groups by Chi-square.
2.1. Results
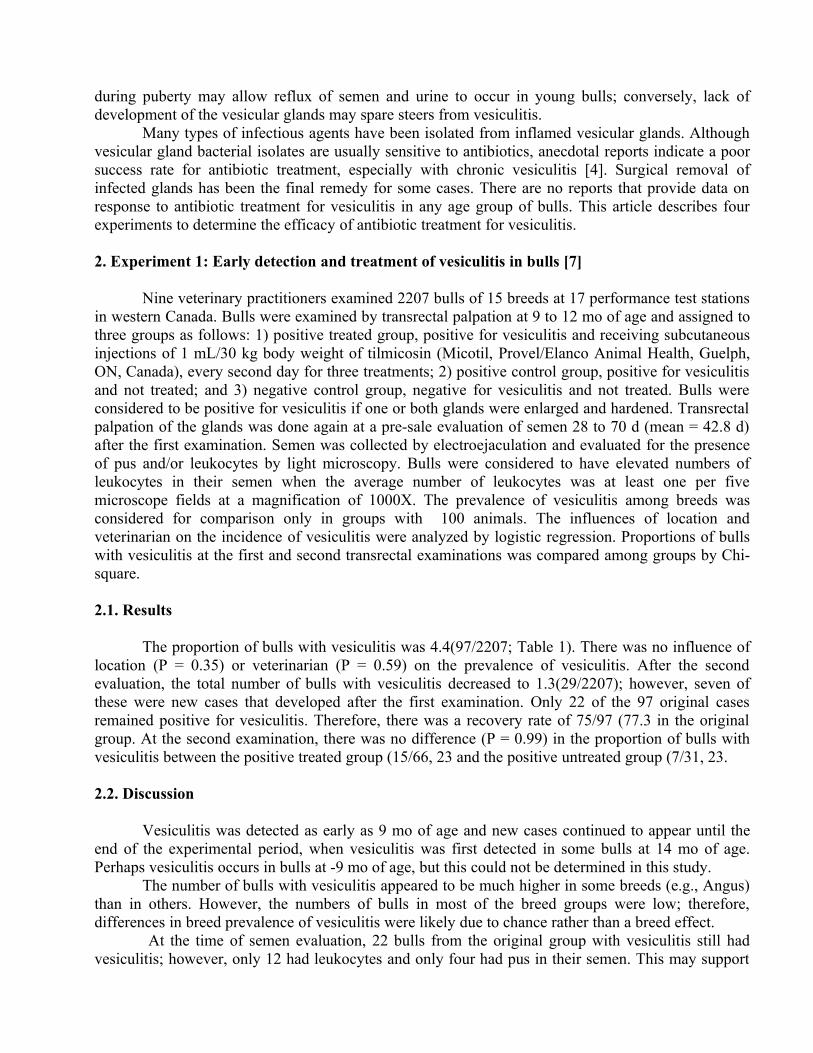
The proportion of bulls with vesiculitis was 4.4(97/2207; Table 1). There was no influence of location (P = 0.35) or veterinarian (P = 0.59) on the prevalence of vesiculitis. After the second evaluation, the total number of bulls with vesiculitis decreased to 1.3(29/2207); however, seven of these were new cases that developed after the first examination. Only 22 of the 97 original cases remained positive for vesiculitis. Therefore, there was a recovery rate of 75/97 (77.3 in the original group. At the second examination, there was no difference (P = 0.99) in the proportion of bulls with vesiculitis between the positive treated group (15/66, 23 and the positive untreated group (7/31, 23.
2.2. Discussion
Vesiculitis was detected as early as 9 mo of age and new cases continued to appear until the end of the experimental period, when vesiculitis was first detected in some bulls at 14 mo of age. Perhaps vesiculitis occurs in bulls at -9 mo of age, but this could not be determined in this study.
The number of bulls with vesiculitis appeared to be much higher in some breeds (e.g., Angus) than in others. However, the numbers of bulls in most of the breed groups were low; therefore, differences in breed prevalence of vesiculitis were likely due to chance rather than a breed effect.
At the time of semen evaluation, 22 bulls from the original group with vesiculitis still had vesiculitis; however, only 12 had leukocytes and only four had pus in their semen. This may support

the theory that vesiculitis begins due to reflux of semen and urine into the vesicular glands [6]. Conversely, when inflammation is associated with infection, as infectious organisms are eliminated from the tissue, fewer and fewer leukocytes and gradually less pus would be produced. In that regard, in treated bulls in our previous experiments [8], the numbers of leukocytes and the amount of pus diminished gradually over 2 to 3 wk after the end of treatment. It appeared that as bacterial infection was reduced, or eliminated by antibiotic treatment and/or natural defense mechanisms, there was a reduction in pus, leukocytes and gland hardness (in that order).
The proportion of bulls with vesiculitis in the positive-control and positive-treated groups was not significantly different at the time of semen collection. Therefore, it appears that under the conditions of this experiment, early detection and antibiotic treatment was not advantageous to reduce the prevalence of vesiculitis at the first semen evaluation. Although early detection and treatment appeared not to be efficacious, the overall incidence of the disease was quite low in this group of bulls. It is noteworthy that the incidence of vesiculitis can be extremely high in some herds [9]. Therefore, early transrectal examination and treatment may be useful in herds with an increased risk for development of the disease.
3. Experiment 2: Effectiveness of antibiotic concentrations in plasma and vesicular gland tissue for in-vitro bacterial growth inhibition
3.1. Experiment 2a
Twenty-five yearling Angus bulls were randomly assigned to five experimental groups (n = 5/group), to receive one treatment of 20 mL of saline IM (control group), Penicillin G procaine (22,000 IU/kg IM; Pen G Injection, Citadel Animal Health, Cambridge, ON, Canada); Ceftiofur (1 mg/kg IM; Excenel, Pharmacia and Upjohn Sante Animale, Orangeville, ON, Canada); Tilmicosin (10 mg/kg SC, Micotil); or Florfenicol (20 mg/kg IM, Nuflor, Schering-Plough Animal Health, Pointe Claire, PQ, Canada). Blood samples were taken before treatments, whereas blood samples and biopsy samples from the right vesicular gland, were taken between 8 and 12 h after treatment. Plasma and biopsies were stored at –40 oC until analyzed.
3.2. Experiment 2b
Eight weeks after the first experiment, the same bulls were randomly re-assigned to five experimental groups (n = 5/group), to receive one treatment of 40 mL of saline IM (control group), the recommended dose of Tulathromycin (2.5 mg/kg IM, Draxxin®, Pfizer Animal Health, Calgary, AB, Canada), or twice the recommended dose of Penicillin G procaine, Ceftiofur and Florfenicol. Blood samples were taken before treatments and blood samples and biopsy samples from the left vesicular gland were taken between 8 and 12 h after treatment. Plasma and biopsies were stored at –40 oC until analyzed.
3.3. Examination of vesicular glands
Vesicular glands were examined by transrectal palpation and ultrasonography before biopsy, on Days 1 to 5, and at 4 and 8 wk after the biopsy procedure. A crude estimate of vesicular gland volume was determined by length, width and depth measurements through the central region of the glands. A real-time, B-mode scanner (Model SSD-900; Aloka, Tokyo, Japan) equipped with a 7.5MHz linear-array transducer was used.

3.4. Biopsy procedure
After the rectum was manually evacuated, the pararectal region was clipped and scrubbed with 1povidone-iodine solution. Local analgesia was achieved by caudal epidural injection of 5 mL of 2lidocaine HCl (Bimeda-MTC Animal Health Inc., Cambridge, ON, Canada) and by infiltration of the subcutaneous tissue of the ischiorectal fossa with 6 mL of lidocaine. A 1-cm stab incision was made in the skin of the ischiorectal fossa and equine uterine biopsy forceps was pushed through the incision and passed parallel to the rectum toward the vesicular gland. The caudal reflection of the peritoneum was bluntly perforated with the forceps to gain to access the vesicular gland. The vesicular gland was fixed by one hand in the rectum, while the forceps was manipulated with the opposite hand. A single glandular tissue sample (10 x 5 mm) was obtained. No sutures were placed after the procedure was completed. Bulls in the Control group had not been previously treated with an antibiotic; therefore, these bulls were given a single injection of procaine penicillin G at the recommended dose and route after the biopsy was obtained. Bulls in the other groups did not receive any further treatment, since they had already been treated with their respective antibiotic.
3.5. Bacteriological culture
Isolates of A. pyogenes and Histophilus somni from clinical cases of vesicular adenitis were used for in vitro sensitivity testing. These isolates were known to be sensitive to the antibiotics used in these experiments, with the exception that H. somni was resistant to tilmicosin and tulathromycin. Bacterial suspensions were cultured until a turbidity of 0.5 MacFarland standard was reached and then swabbed on blood agar in 94-mm plates. A. pyogenes and H. somni were inoculated in different plates as described for the standard disk diffusion method [10]. A well was punched in the middle of the agar as a receptacle for plasma or glandular tissue fluid suspensions. Undiluted plasma samples (20 µL) were directly deposited into agar wells. Biopsies of vesicular gland tissue were trimmed to a standard weight (1 g) and homogenized in 40 µL of saline; 20 µL of the resulting suspension was placed in agar wells. As laboratory controls, sterile 6 mm paper discs with antibiotics (Becton, Dickinson and Co, Sparks, MD, USA) were placed on the inoculated agar surface. All procedures were performed under sterile conditions. Plates were incubated at 37 °C with 7CO2 for 24 h, and the diameter of zones of bacterial growth inhibition were measured.
3.6. Results None of the bulls displayed any signs of discomfort at any time after the biopsy procedure.
However, in 5 of 25 bulls in Experiment 2a, hematomas were palpable in the pelvic cavity; all resolved spontaneously within approximately 3 wk. In four of the bulls, the hematomas were estimated to be 5 to 7 cm in diameter and 3 cm deep. In one of the bulls, the hematoma was approximately 20 cm in diameter and 7 cm deep. In Experiment 2b, when the biopsy procedure was repeated in bulls on the opposite gland, none of the bulls developed hematomas. No adverse effects on the biopsied vesicular glands were detected by transrectal palpation or ultrasonography in any of the bulls during Experiments 2a and 2b.
Although bacteria were sensitive to the antibiotics used (as determined by antibiotic disk sensitivity tests), after administration at the recommended dose (Experiment 2a), neither serum nor tissue concentrations of penicillin, ceftiofur, or florfenicol inhibited growth of H. somni in any of the bulls. Serum penicillin inhibited growth of A.pyogenes in 3 of 5 bulls, and serum tilmicosin inhibited growth of A.pyogenes in 5 of 5 bulls. Only tilmicosin achieved sufficient concentrations in vesicular gland tissue to inhibit growth of A.pyogenes in 4 of 5 bulls (Table 2).

When twice the recommended dose of penicillin, ceftiofur or florfenicol was used, there was an increase in the number of serum and tissue samples that achieved concentrations sufficient to inhibit growth of H. somni and A. pyogenes (Table 3). Serum penicillin inhibited growth of H. somni and A. pyogenes in 5 of 5 bulls. Serum ceftiofur inhibited H. somni in 5/5 and A. pyogenes in 0 of 5 cases. Serum florfenicol inhibited H. somni in 1/5 and A. pyogenes in 1/5 cases. Serum tulathromycin at the recommended dose inhibited A. pyogenes in 5/5 cases. Only ceftiofur achieved sufficient tissue concentrations to inhibit H. somni (3/5 cases). However, inhibitory tissue concentrations for A. pyogenes were achieved in some cases by all antibiotics: 2/5, 1/5, 1/5 and 2/5 cases for penicillin, ceftiofur, florfenicol and tulathromycin, respectively.
3.7. Discussion
The biopsy procedure in Experiment 2a resulted in hematoma formation in some of the bulls, but none of the bulls developed hematomas in Experiment 2b. A possible reason for the difference is that in Experiment 2a, the bulls were younger and their glands were smaller; therefore, a proportionately larger sample was taken from their glands. Secondly, in Experiment 2a, samples were taken from the gland near to the urethra, whereas, in Experiment 2b, biopsy samples were taken from the middle of the gland. Thus, the size of the gland at the time of biopsy and the location of the biopsy might explain the difference in the number of hematomas that developed. In an earlier experiment (unpublished), 50 vesicular gland biopsies taken from 25 older bulls did not cause any hematomas. Semen samples were collected by electroejaculation from all bulls used in this experiment, approximately 5 wk after the last vesicular gland biopsy was performed. At that time, none of the bulls had any detectable adverse effect of the biopsy procedure. Therefore, the biopsy procedure appeared to be a safe and effective means for obtaining vesicular gland tissue samples from healthy bulls.
The antibiotics administered to the bulls in these experiments resulted in serum or gland concentrations with varying effects on in-vitro growth of H. somni or A. pyogenes; however, paper discs containing the antibiotics were effective for growth inhibition of both types of bacteria used in this study (with the noteable exception that H.somni was resistant to tilmycosin and tulathromycin). The differences in bacterial growth inhibition among plasma and tissue fluid concentrations of antibiotics were likely influenced by concentrations of antibiotic achieved, pharmacokinetic characteristics, and sensitivity of bacteria.
The paper disks for sensitivity testing contained high concentrations of antibiotic and demonstrated only whether high concentrations would inhibit bacterial growth in-vitro. At 8 to 12 h after treatment, it was expected that adequate concentrations of the antibiotics used would be present in serum tissues to inhibit bacterial growth if infection was present. However, due to dilution of antibiotics within the blood, inhibition of in-vitro growth by serum samples should not necessarily be expected.
Based on Experiment 2a, recommended dosages of penicillin, ceftiofur and florfenicol may not achieve sufficient concentrations in vesicular gland tissue to inhibit growth of the strains of H. somnii and A. pygenes used in these experiments. The H. somni strain used in this experiment was resistant to tilmicosin, therefore, tilmicosin did not inhibit in vitro growth of H. somnii, but concentrations were sufficient to inhibit A. pyogenes in 4 of 5 cases. Therefore, tilmicosin might be an antibiotic of choice for treatment of vesiculitis involving these bacteria.
In Experiment 2b, using twice the recommended dosage of antibiotics improved the chance of bacterial growth inhibition in vesicular gland tissue for all antibiotics tested. Perhaps treatment failures in clinical cases of vesicular adenitis are due to inadequate concentrations of antibiotics developing within the gland tissue. Field trials are needed to study the treatment responses of clinical

cases of vesiculitis to the recommended dose of various antibiotics, as well as the use of these antibiotics at doses exceeding label recommendations.
4. Experiment 3: Intraglandular injection of antibiotics for the treatment of vesicular adenitis [8]
In an earlier experiment, intraglandular injection in normal healthy bulls of 10of the daily recommended parental dose of procaine penicillin G (22000 IU/kg IM), or ceftiofur (1 mg/kg kg IM), dissolved in saline (final volume, 6 mL), caused minimal tissue reaction without any prolonged ill effect to the vesicular glands. The method of intraglandular injection of antibiotics was as follows. Preparation of the region of the pararectal fossa was similar to that for vesicular gland biopsy. After stab incision was made in the skin of the ischiorectal fossa, a custom-made, blunt, 4-mm o.d. needle guide was pushed through the incision and passed pararectally up to the vesicular gland. The caudal reflection of the peritoneum was bluntly perforated with a short jab. The vesicular gland was fixed by one hand in the rectum, while the needle guide was manipulated with the opposite hand. A 44-cm long 18-gauge needle containing antibiotic (to avoid injecting air into the gland) and connected to a syringe with antibiotic was directed through the needle guide into the gland. The antibiotic was slowly injected into the gland.
Fourteen untreated beef bulls with clinical vesicular adenitis were used in this experiment. Eight bulls had unilateral vesiculitis (left, n=3; right, n=5) and six bulls had bilateral vesiculitis. Since the bull owners were unwilling to leave their bulls untreated, a period of 3 wk from the time of diagnosis in the field until experimental treatments were commenced was considered to be a control period for these bulls. The 14 bulls were then treated by an intraglandular injection of an antibiotic.
Semen for bacterial culture was collected by electroejaculation at the initial evaluation. After penile protrusion, the glans penis was grasped with a sterile surgical sponge and the tip of the penis was swabbed with betadine and dried with a sterile sponge. A spurt of semen was directed into a sterile vial held horizontally near the penis. Semen was swabbed on sheep blood agar and MacConkey agar. All plates were incubated at 37 °C in an atmosphere of 7CO2. Biochemical characterization and antimicrobial sensitivity tests for bacteria isolated were performed following the National Committee for Clinical Laboratory Standards M31-A recommendations [10].
Bulls were subjected to transrectal palpation and ultrasonography of the vesicular glands and semen collection by electroejaculation before treatment and every 4 d (11 times) after treatment.
Ceftiofur was injected into affected glands as the initial treatment in 13 of the 14 bulls; in the absence of evidence of recovery within 3 wk, a second intraglandular treatment with penicillin (n=6) was done. One bull was treated only once with an initial injection of penicillin. Three bulls that did not recover from vesiculitis after two intraglandular antibiotic injections (ceftiofur and penicillin) received three treatments of tilmicosin subcutaneously (Micotil, 10 mg/kg) at the recommended dose, 48 h apart.
Recovery from vesiculitis was deemed to have occurred when two or more consecutive semen samples were free of blood and pus, and semen smears had less than one leukocyte per five microscope fields at 1000X magnification. The presence of blood, pus and leukocytes in the semen, and vesicular gland hardness were scored from 0 to 4. For blood: 0 = absence, 1 = slight tinge, 2 = pink, 3 = red, and 4 = dark red p clots. For pus: 0 = absence, 1 = a few 1 mm diameter flakes, 2 = a few 2 mm diameter curds, at the bottom of the semen column after a settling period of 5 min, 3 = - 0.5 mL, and 4 = 0.5 mL of pus at the bottom of the semen column immediately after semen collection. For detection of leukocytes, semen was allowed to settle for 5 min, and then semen was sampled from the bottom of the semen column for preparation of an eosin-nigrosin stained semen smear. The leukocyte score was: 0 = absence, 1 = -2 leukocytes per 1000x field on microscopy, 2 = 2 to 5 leukocytes per field, 3 = 5 to 10 leukocytes per field, and 4 = 10 leukocytes per field. The hardness of

the vesicular glands was subjectively scored by transrectal palpation as 1 = consistency of a normal gland, 2 = slightly increased firmness, 3 = moderately hard, and 4 = hard.
4.1. Ultrasound imaging
Transrectal ultrasonographic examinations were performed immediately before, immediately after, and at 24, 72 and 168 h after intraglandular antibiotic treatment to monitor changes in glandular echotexture and changes in volume. A crude estimate of volume was determined by length x width x depth measurements through the central region of the glands. A real-time, B-mode scanner (Model SSD-900; Aloka, Tokyo, Japan) equipped with a 7.5 MHz linear-array transducer was used. The ultrasound scanner had a built-in program that allowed for the construction of a histogram that indicated the intensity distribution of image pixels within a randomly selected area (1 cm2). The data provided by the built-in program included:T - the total number of pixels in the specified areaL - the intensity level that occurred most frequently in the specified areaM - the number of pixels corresponding to the intensity level that most frequently occurred in the specified area.MN - the mean intensity level in the specified area.SD - the standard deviation of the intensity distribution in the specified area.
A mean high intensity pixel value was also calculated based on L multiplied by its frequency M. Percentage of MN and SD were also analyzed using the ultrasound scan at Time 0 (before treatment) as the reference control equal to 100
4.2. Statistical analysis
Pearson’s correlation coefficients were calculated for semen characteristics (density, gross motility, individual motility, percentage of normal spermatozoa, presence of blood, pus, or leukocytes). Scores of consistency of the vesicular glands and the presence of blood, pus or leukocytes among semen samples were compared by the Kruskal-Wallis non-parametric test. Mean ranks between groups were further compared by the Mann-Whitney test. The MN and SD of pixel distribution were analyzed by analysis of variance in a 2x 2 factorial design (Status: affected or healthy gland; Time: before and 7 d after treatment). Data and graph processing were performed with Microsoft Office Excel and statistical analyses were conducted with SPSS for Windows (SPSS v. 11.5, SPSS Inc. 2002, USA).
4.3. Results
A. pyogenes was the most common bacterium isolated from the infected bulls. In addition, there were isolates of Acinetobacter sp., Streptococcus sp., Pasteurella sp. and Corynebacterium sp. All bacteria isolated from the different bulls were sensitive to ceftiofur, penicillin, and tilmicosin. Seven of 13 bulls recovered after one intraglandular injection of ceftiofur, and 1 of 1 bull recovered after one intraglandular injection of penicillin. Three of six bulls that did not recover after one injection of ceftiofur recovered after a second intraglandular injection with penicillin. Three bulls that did not recover after a ceftiofur and a penicillin intraglandular treatment, recovered after receiving three treatments of tilmicosin by subcutaneous injection.

There was a difference (P-0.05) among successive ejaculates in pus, leukocytes, and blood (Fig. 1). Ejaculates 8 to 11 had less pus than the first two ejaculates (P-0.05), and less leukocytes than the first five ejaculates (P-0.05). Ejaculates 6 to 11 had less blood than Ejaculates 2 and 3 (P-0.05).
The mean change in consistency score of the glands (transrectal palpation) remained unremarkable from the first to the last examination in most bulls (P = 0.63); however, in three bulls, the consistency score decreased from 4 to 1 by the time of the last examination. When inflamed and healthy vesicular glands were compared by ultrasonography before and 1 wk after treatment, there was no effect of gland health status, time, or health status by time interaction on the MN (P = 0.3, P = 0.46, and P = 0.64, respectively) or SD (P = 0.16, P = 0.77, and P = 0.20, respectively) of pixel distribution.
4.4. Discussion
In this experiment, intraglandular injection of ceftiofur or penicillin in beef bulls via the ischiorectal fossa appeared to be safe and effective in the treatment of vesicular adenitis. A major fault of this experiment was a lack of a contemporary control group, in which bulls with vesiculitis were not treated to ensure that any recoveries due to intraglandular antibiotic treatment was not due to spontaneous recovery. To compensate for a contemporary control group, a control period of at least 3 wk was allowed before bulls were treated; none of the bulls recovered during this time period.
Ultrasonography can be used to evaluate the characteristics of the glands prior to and after intraglandular antibiotic treatment. Evaluation of vesicular glands by transrectal palpation was also useful in monitoring the effect of treatments, but semen collection is likely the most useful method to evaluate the progress of recovery from vesiculitis.
5. Experiment 4: Treatment of field cases of vesicular adenitis with tilmicosin and tulathromycin
Two antibiotics, tilmicosin and tulathromycin, were chosen for use in a field test for efficacy in the treatment of clinical vesiculitis. Tilmicosin and tulathromycin were chosen over other antibiotics, based on previous experimental results of vesicular gland tissue fluid inhibition of in vitro bacterial growth. In addition, there was evidence that tilmicosin and tulathromycin accumulated in macrophages and neutrophils and were subsequently released slowly from such cell types [11]. Thus, immune defense cells would carry these antibiotics into sites of infection [12]. Antibiotic coverage was for 6 d, i.e., a single tulathromycin treatment, or two tilmicosin treatments 72 h apart, at a dose indicated by the label information.
A mail-out of an experimental protocol was done to veterinarians in large animal practices in Alberta, Manitoba, and Saskatchewan, Canada. A total of 180 veterinary practices were contacted and offered financial incentive to participate.
Eligible cases of vesiculitis were considered to be those in which clots or flakes of pus were visible in semen samples, white blood cells were found at ≥1 per five microscope fields at 1000X magnification, the vesicular glands were enlarged and hardened, and there was no record of previous antibiotic treatment.
Response to treatment was determined 21 to 28 d after the beginning of treatments. A positive response was considered to be: no clots of pus in the semen, no flakes of pus in the bottom of the tube after 5 min of settling time, and ≤ 1 white blood cells per microscope field at 1000X magnification.
Gland size and hardness were often reduced in bulls with a positive response, but this was not required to qualify as a positive response. Participating veterinarians were required to obtain a sample of semen by sterile means, submit it to a provincial laboratory, and report the results. Semen collection for bacterial culture was done after penile protrusion by electroejaculation. The glans penis

was grasped with a sterile surgical sponge and the tip of the penis was swabbed with betadine and dried with a sterile sponge. A spurt of semen was directed into a sterile vial held horizontally near the penis. In the control group, the possibility of spontaneous remission was investigated at 3 wk from the discovery of the case.
5.1. Results
Seventeen veterinarians participated in the study, involving 65 bulls. The recovery rate was higher for bulls treated with Tulathromycin (22/25= 88 than for Tilmicosin (11/23 = 48 and both antibiotics resulted in a higher recovery rates than occurred the untreated control group (0/17; P-0.01). In the tulathromycin group, six bulls were mature (four 2-y-olds and two 3-y-olds), but the three bulls that did not recover were yearlings. In the tilmicosin group, five bulls were mature (three 2-y-olds, one 4-y-old, and one 6-y-old). Two of the 2-y-old bulls treated with tilmicosin recovered, but the other mature bulls did not. In the control group, all bulls were yearlings and none recovered.
5.2. Discussion
Based on the outcome, both Tilmicosin and Tulathromycin should be useful in the treatment of vesiculitis. Studies of vesicular gland tissue concentrations of antibiotics indicated that tilmicosin concentrations achieved may be inadequate in some bulls and therefore, an increased dosage, or a more frequent treatment regime than that recommended on the label, might give better results. Anecdotal reports of treatment of clinical cases in the field appeared to confirm this finding.
Many of the semen culture sensitivity tests indicated that the organisms isolated were resistant to tulathromycin and tilmicosin. This included organisms considered likely to be pathogens; however, a large proportion of isolated organisms were considered contaminants. The organisms considered pathogens were H. somni and A. pyogenes, and the main contaminants were Pseudomonas spp., Proteus spp, E. coli, Staphlococcus spp and Streptococcus spp. Nevertheless, recovery occurred after treatment in a large proportion of the cases.
Both antibiotics resulted in cures of vesiculitis (as defined for this study), including some bulls that were ≥2-y-old. Although the time of onset of vesiculitis in these bulls could not be determined, it is likely that the infections were of a chronic nature. If this is so, then a 6-d course of antibiotics was apparently able to overcome chronic infections in some bulls. Further studies are needed to determine the relapse rate in bulls that appear to recover after antibiotic treatment.
References
[1] Cavalieri J, Van Camp SD. Bovine seminal vesiculitis. A review and update. Vet Clin North Am Food Anim Pract 1997;13:233-241. [2] Ball L, Young S, Carroll EJ. Seminal vesiculitis syndrome, lesions in genital organs of young
bulls. Am J Vet Res 1968;29:1173-1184.[3] Dargatz DA, Mortimer RG, Ball L. Vesicular adenitis of bulls: a review. Theriogenology 1987;28:513-521.[4] Phillips PE. Seminal vesiculitis: New strategies for an old problem. Proc Soc for
Theriogenology, Jacksonville, 1993, pp. 59-66[5] Blom E. Malformation of the pelvic genital organs as a possible predisposing factor in the
pathogenesis of vesiculitis in the bull. 9th Internat Congr Anim Reprod and AI, 1980, III: pp 217.
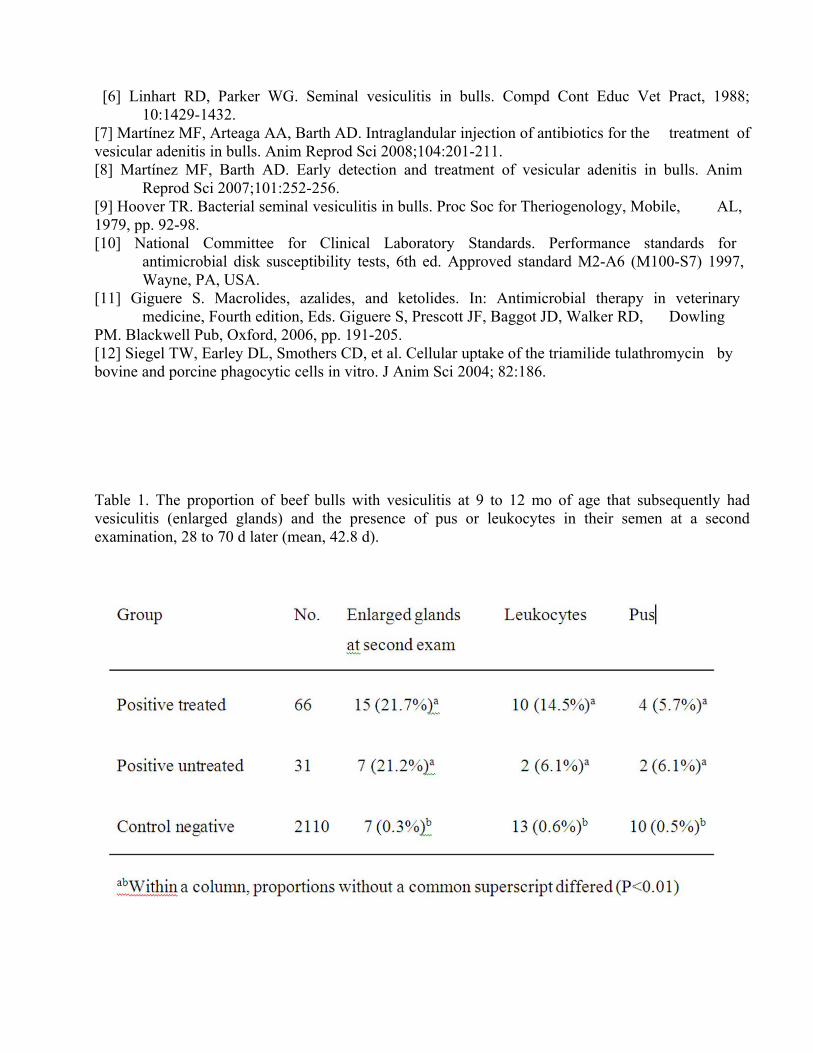
[6] Linhart RD, Parker WG. Seminal vesiculitis in bulls. Compd Cont Educ Vet Pract, 1988;10:1429-1432.
[7] Martínez MF, Arteaga AA, Barth AD. Intraglandular injection of antibiotics for the treatment of vesicular adenitis in bulls. Anim Reprod Sci 2008;104:201-211. [8] Martínez MF, Barth AD. Early detection and treatment of vesicular adenitis in bulls. Anim
Reprod Sci 2007;101:252-256.[9] Hoover TR. Bacterial seminal vesiculitis in bulls. Proc Soc for Theriogenology, Mobile, AL, 1979, pp. 92-98.[10] National Committee for Clinical Laboratory Standards. Performance standards for
antimicrobial disk susceptibility tests, 6th ed. Approved standard M2-A6 (M100-S7) 1997, Wayne, PA, USA.
[11] Giguere S. Macrolides, azalides, and ketolides. In: Antimicrobial therapy in veterinary medicine, Fourth edition, Eds. Giguere S, Prescott JF, Baggot JD, Walker RD, Dowling
PM. Blackwell Pub, Oxford, 2006, pp. 191-205.[12] Siegel TW, Earley DL, Smothers CD, et al. Cellular uptake of the triamilide tulathromycin by bovine and porcine phagocytic cells in vitro. J Anim Sci 2004; 82:186.
Table 1. The proportion of beef bulls with vesiculitis at 9 to 12 mo of age that subsequently had vesiculitis (enlarged glands) and the presence of pus or leukocytes in their semen at a second examination, 28 to 70 d later (mean, 42.8 d).

Table 2. Inhibition of in-vitro growth of H. somni or A. pyogenes by serum or vesicular gland tissue fluid when samples were collected from beef bulls 6 to 12 h after treatment with saline (control), or the recommended dose of penicillin, ceftiofur, tilmicosin, or florfenicol (n=5 bulls/group).
a>
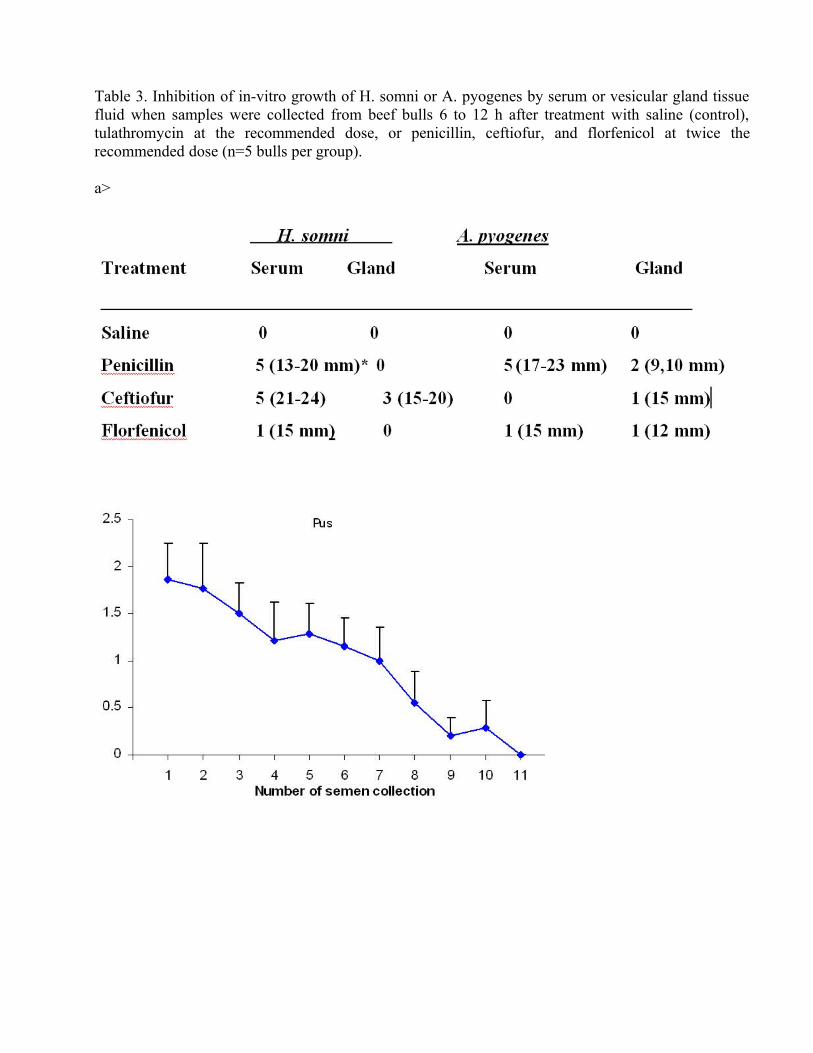
Table 3. Inhibition of in-vitro growth of H. somni or A. pyogenes by serum or vesicular gland tissue fluid when samples were collected from beef bulls 6 to 12 h after treatment with saline (control), tulathromycin at the recommended dose, or penicillin, ceftiofur, and florfenicol at twice the recommended dose (n=5 bulls per group).
a>

Fig. 1. Mean ( SD) scores representing the presence of pus, leukocytes and blood in the semen samples obtained from all bulls affected with vesicular adenitis.