implications of lung cancer screening in the new millenia andrew r. haas, md, phd assistant...
TRANSCRIPT

Implications of lung cancer screening in the new millenia
Andrew R. Haas, MD, PhD
Assistant Professor of Medicine
Section of Interventional Pulmonary and Thoracic Oncology
Perelman School of Medicine of the University of Pennsylvania

Disclosures
• None

Rationale for lung CA screening
• Lung CA– 2nd most common cancer in the US– Most common cause of cancer death in the US
and world– Prognosis depends primarily upon stage at
diagnosis– Early detection with screening may lead to
improved outcomes???
Siegel et al, CA Cancer J Clin 2011

Rationale for lung CA screening
• Smoking– ~1 in 5 adults (~46 million people) in US smoke– #1 risk factor for lung CA
• ~85% of lung CA deaths are due to smoking
– > 94 million current and former smokers in US are at increased risk for lung CA
http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htmhttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5935a3.htmhttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5844a2.htm
Prior Lung Ca Screening Trials
• CXR vs. usual care• CXR vs. CXR with sputum cytology• CT scan vs. usual care
No benefit until – National Lung Screening trial
Fontana et al Cancer 67:1155; Tockman et al Chest 89:324SKubik et al Int J Ca 45:26; Melamed et al Chest 86:44Oken et al JAMA 306:1865; Hocking et al J NCI 102:722Infante et al AJRCCM 180:445;
National Lung Screening Trial (NLST)
A collaboration between ACRIN and NCI The largest and most expensive randomized
clinical trial of a single screening test in US medical history
$250,000,000

NLST – Eligibility criteria
• Age 55-74 years• Current or former > 30 pack-year smoking
history– Former smokers quit within last 15 years
• No history of lung CA• No treatment for or evidence of any other
cancer within the last 5 years

NLST – Study design
Enrollment: 8/2002-4/2004Annual Interim Analyses: 4/2006 - 4/2010
Final: 10/2010
Prospective randomized controlled trialScreening for 3 consecutive years with either CXR or low-dose chest CT

NLST – Primary endpoint
• Lung cancer specific mortality– 20% difference between CT vs. CXR
• Type 1 error rate (a) = 5%• Power (1 - b) = 90%• Compliance 85% CT | 80% CXR• Contamination 5% CT | 10% CXR• Size = 25,000 subjects/arm

NLST – Secondary endpoints
• Comparison of CT and CXR regarding– All-cause mortality– Incidence of lung CA– Lung CA stage distribution– Medical resource utilization– Quality of life and psychological impact– Cost-effectiveness
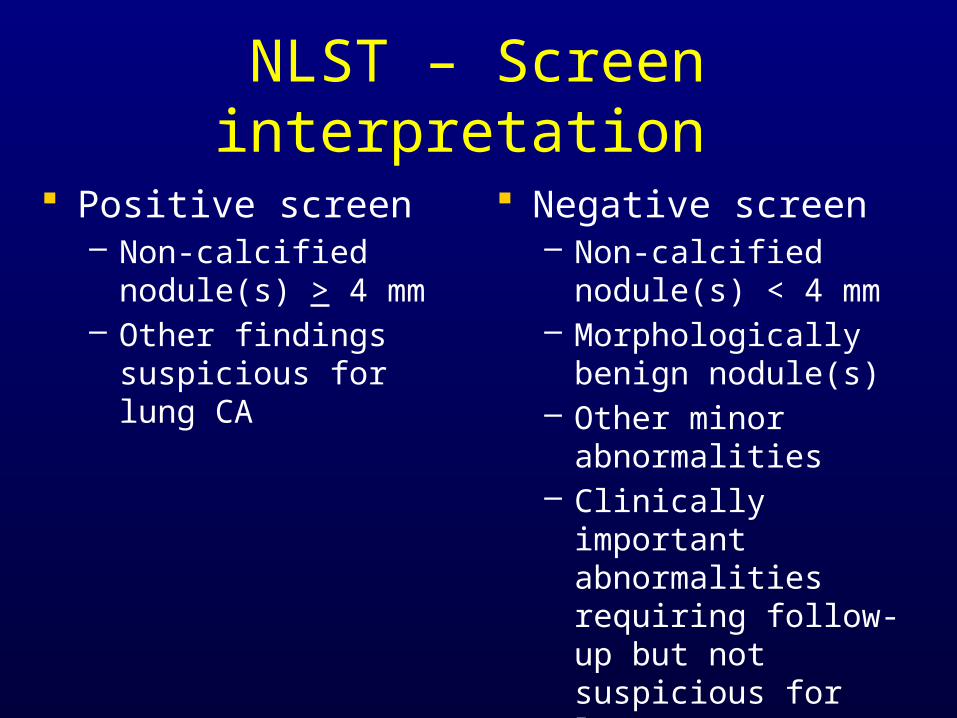
NLST – Screen interpretation
Positive screen– Non-calcified nodule(s)
> 4 mm– Other findings
suspicious for lung CA
Negative screen– Non-calcified nodule(s)
< 4 mm– Morphologically benign
nodule(s)– Other minor
abnormalities– Clinically important
abnormalities requiring follow-up but not suspicious for lung CA

NLST – Subject accrual and biospecimen collection
• Recruitment from 33 screening centers
• Blood, urine, and sputum biospecimens collected at
– 15 NLST-ACRIN sites– 10208 subjects total
• Paraffin blocks of resected tumors collected
– Across all NLST sites

NLST – Subject accrual
NLST Research Team slide set
50,000
40,000
30,000
20,000
10,000
Aug 02 Nov 02 Feb 03 May 03 Aug 03 Nov 03 Feb 04
Total 53,454- CT 26,722- CXR 26,732
LSS 34,614(65%)
Month Enrolled
Subj
ects
ACRIN 18,840(35%)
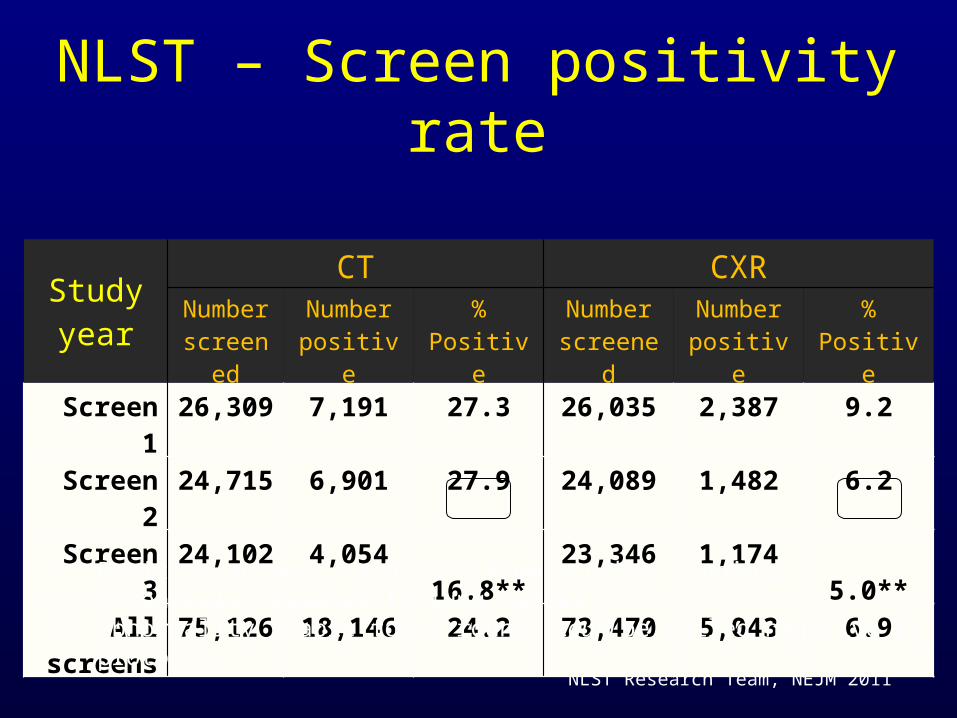
NLST – Screen positivity rate
NLST Research Team, NEJM 2011
Study year
CT CXRNumber
screenedNumber positive % Positive
Number screened
Number positive % Positive
Screen 1 26,309 7,191 27.3 26,035 2,387 9.2
Screen 2 24,715 6,901 27.9 24,089 1,482 6.2
Screen 3 24,102 4,054 16.8** 23,346 1,174 5.0**
All screens 75,126 18,146 24.2 73,470 5,043 6.9
* Positive screen: nodule ≥ 4 mm or other findings potentially related to lung cancer.** Abnormality stable for 3 rounds could be called negative by protocol.

NLST – Significance ofpositive screens
NLST Research Team, NEJM 2011
Screening result
CT CXRScreen 1
N (%)Screen 2
N (%)Screen 3
N (%)TotalN (%)
Screen 1N (%)
Screen 2N (%)
Screen 3N (%)
TotalN (%)
Total Positives
7,191 (100)
6,901 (100)
4,054 (100)
18,146 (100)
2,387 (100)
1,482 (100)
1,174 (100)
5043 (100)
Lung CA confirmed 270 (3.8) 168 (2.4) 211 (5.2) 649 (3.6) 136 (5.7) 65 (4.4) 78 (6.6) 279 (5.5)
Lung CA not confirmed
6,921 (96.2)
6,733 (97.6)
3,843 (94.8)
17,497 (96.4)
2,251 (94.3)
1,417 (95.6)
1,096 (93.4)
4,764 (94.5)

NLST – Results• Lung CA specific mortality
– Relative reduction by 20% (95% CI 6.8-26.7, p=0.004) (87 fewer deaths in CT vs. CXR arm)
– The number needed to screen with CT to prevent 1 death from lung CA is 320
• All cause mortality– Rate of death reduction decreased by 6.7% (95% CI
1.2-13.6, p=0.02)– Rate of death reduction decreased by 3.2% (p=0.28)
when lung CA deaths excluded• Stage distribution more favorable for CT than CXR
• 70.2% vs. 56.7% were stage I-II

NLST – Biospecimen bank
• Intended for validation of promising biomarkers in preliminary testing– Biomarkers for high risk of lung CA– Biomarkers for benign vs. malignant nodules– Biomarkers predictive or prognostic of lung CA
behavior

NLST – Pending analyses
• Costs– Direct medical (screening, Dx tests, Rx’s)– Non-medical (travel, lodging)– Opportunity (lost wages)
• Cost-effectiveness (ICER)• Quality of life effects• Smoking behavior effects• Health care utilization

NLST – Pending questions
• Policy recommendations to implement CT screening in standardized fashion– Starting age? Frequency? # of scans?– How do we integrate prevention, Dx, and Rx
algorithms in standardized fashion?– How extrapolate/model to other populations?
• Younger or older people• People with lower smoking history• People with family history• Non-urban non-3o community practice settings

NLST – Pending questions
• Who will cover costs of CT screening?– Out-of-pocket? Insurance? Tobacco industry?
• How can the number of false positive CT screens be decreased?
• What other factors define very high risk?– Biospecimen analysis

“Formal” guidelines
• American College Chest Physicians• American Society of Clinical Oncology• National Comprehensive Cancer Netwrok
– 55-74 yo – > 30 pk-yrs tobacco use
• US Preventive Services Task Force– No guideline comments
Implications of lung cancer screening
• 10 – 15 million smokers fulfill screening criteria• 2.5 – 4.5 million new pulmonary nodules• Cost – $5 – $7.5 billion USD• Screen positives that went on to biopsy –
estimated deaths

Conclusions
• The NLST has shown that CT screening– Decreases lung CA specific mortality– Has a high false positive rate
• Further analyses ongoing• Additional questions about CT screening need to
be answered prior to implementation• Smoking prevention and cessation are still critical
to reduce lung CA incidence and mortality rates

The National Lung Screening Trial has demonstrated which of the following :
• A) A reduction in all cause mortality of 15.3%• B) A modest false positive rate of 9%• C) A relative reduction in lung cancer specific
mortality of 20%• D) Follow up of false positive scans had no
patient impact• E) A very cost effective approach to reduction
in lung cancer mortality
Thank you!