implementation of best practice in the prevention of … article implementation of best practice in...
TRANSCRIPT
ORIGINAL ARTICLE
Implementation of bestpractice in the preventionof heel pressure ulcersin the acute orthopedicpopulationKaren E Campbell, M Gail Woodbury, Pamela E Houghton
Campbell KE, Woodbury MG, Houghton PE. Implementation of best practice in the prevention of heel pressureulcers in the acute orthopedic population. Int Wound J 2010; 7:28–40
ABSTRACTTo implement and evaluate a heel pressure ulcer prevention program (HPUPP) for orthopaedic patients. Programdevelopment of HPUPP involved input from administrators, staff and adult patients on an orthopaedic service in anacademic tertiary care facility, located in a small urban centre in Canada. Prospective evaluation was conducted.Consensus exercises with clinical staff and administrators (Delphi and Nominal group) were used to, evaluatecurrent practices, select a heel protective device, and develop key aspects of the HPUPP. HPUPP involved anindividualised, bedside, staff education program, a team approach to improve patient mobility and use of a heelprotective device. A 2-inch foam wedge covered in washable vinyl was placed at the foot of all beds on theorthopedic service. After the program was implemented, the incidence of heel pressure ulcers was 0%, whichwas a significant reduction compared with pre-implementation levels [13·8% (95% confidence interval 8–18%)].Key components of the program success were initial and ongoing support from administration and surgeons,incorporation of feedback from clinical staff and patients, and keeping the program simple. Heel PU can beprevented in most orthopaedic patients using a universal heel PU prevention program.
Key words: heel pressure ulcers • prevention program • heel device • RNAO best practice guidelines • RNAO toolkit
Pressure ulcers are an ongoing and serious
Key Points
• pressure ulcers can significantlyincrease a patient’s length ofstay in the hospital, mortal-ity and costs, reduce qualityof life, increase the risk of abelow-the-knee amputation indiabetics and limit rehabilita-tion
• heel pressure ulcers are dif-ferent than pressure ulcers onother parts of the body
• the shape of the heel makesit more difficult to downloadpressure unless the heel is lifteddirectly off the bed
• prevention strategies for theheel are different than preven-tion strategies for other partsof the body and need to includea method to completely offloadpressure by lifting the heel offthe bed
health concern. Pressure ulcers can signifi-cantly increase a patient’s length of stay inthe hospital (1,2), mortality (3), and costs (2,4),reduce quality of life (5), increase the risk ofa below-the-knee amputation in diabetics (6)and limit rehabilitation. Heel pressure ulcers(HPUs) are different than pressure ulcers onother parts of the body. The shape of the heel
Authors: KE Campbell, RN, MScN, PHD, London HealthSciences Center, London, Ontario, Canada; MG Woodbury,BSc, BScPT, MSc, PhD, University of Western Ontario, London,Ontario, Canada; PE Houghton, BScPT, PhD, University ofWestern Ontario, London, Ontario, Canada.Address for correspondence: Karen E Campbell, Faculty ofHealth Sciences, Elborn College, University of Western Ontario,London, Ontario, Canada, N6G 1H1E-mail: [email protected]
makes it more difficult to download pressureunless the heel is lifted directly off the bed.The calcaneus bone has a pointed shape withlittle subcutaneous fat and this as well makesit vulnerable to pressure (7). It has been foundpreviously that heel perfusion is highest withcomplete pressure relief (7), and this find-ing is supported by a recent research study(8). Therefore, prevention strategies for theheel are different than prevention strategiesfor other parts of the body and need to includea method to completely offload pressure bylifting the heel off the bed. Heels have beenidentified as a common site for pressure ulcers,and generally either the most common orthe second most common site in studies inEurope, the USA and Canada (9–15). Some
28 © 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc • International Wound Journal • Vol 7 No 1

Prevention of heel pressure ulcers
studies have found that the prevalence ofHPU is increasing over the past, whereas thenumber occurring in other body locations is thesame or decreasing (13,16). Individuals under-going lower extremity orthopedic surgery areat particularly high risk of developing HPU(10,17–19) as are the elderly (20–23).
Much work on developing pressure ulcerprevention programs has been carried out,with the development of best practice guide-lines (BPGs) or clinical practice guidelines(CPGs) by organisations, such as the Regis-tered Nurse Association of Ontario (RNAO)(24), the US Agency for Health Care Policy
& Research (AHCPR) (25) and the CanadianAssociation of Wound Care (26).
RNAO developed a toolkit for implementingBPG because of its concern that BPG would notbe fully used by health care clinicians if theywere not effectively introduced, supported andimplemented (27). In the toolkit, which canbe used to implement any BPG, six essentialcomponents of successful BPG implementationare proposed: BPG identification, stakeholderinvolvement, environmental readiness, use ofeffective implementation strategies, evaluationof BPG implementation and identification ofrequired resources.
Research studies and quality improvementprojects on the prevention of pressure ulcershave focused on implementation of partor all of the BPG, such as the AHCPRguidelines and the Guidelines for Preventionand Management of Pressure Ulcers fromthe Wound Ostomy and Continence NursesSociety (28–32). Some of these preventionprograms have been successful (12,17,33–35),whereas others have not been successful(11,36). Barriers to implementation included
a lack of visible senior nursing leadershipand time required to learn new skills andimplement the guideline, as well as difficultieswith the computer (37).
Although the ability of BPG implementationto reduce the prevalence or incidence ofpressure ulcers has been documented inseveral studies, the effectiveness of preventionprograms designed specifically for heel ulcershas been examined in only a few studies (38).
In a recent meta-analysis, the authors con-cluded that there was limited research that hasevaluated whether heel boots or similar devicesreduce the risk of HPU development (39). Twoclinical trials were located in this systematic
literature search and review and both found no Key Points
• RNAO developed a toolkit forimplementing BPG because ofits concern that BPG wouldnot be fully used by healthcare clinicians if they werenot effectively introduced, sup-ported and implemented
• in the toolkit, which can beused to implement any BPG, sixessential components of suc-cessful BPG implementationare proposed: BPG identifica-tion, stakeholder involvement,environmental readiness, useof effective implementationstrategies, evaluation of BPGimplementation and identifica-tion of required resources
• although the ability of BPGimplementation to reduce theprevalence or incidence of pres-sure ulcers has been docu-mented in several studies, theeffectiveness of prevention pro-grams designed specifically forheel ulcers has been examinedin only a few studies
• the purpose of this projectwas to develop, implementand evaluate a HPU preventionprogram
significant difference in HPU incidence (40,41).In a recent product evaluation report, greaterpatient satisfaction was found with a fibrefilled boot than with an air-filled foot waffle(42). After the meta-analysis was completed,a randomised controlled trial (RCT) involvingintensive care unit (ICU) patients showed a sta-tistically significant reduction in the number ofHPU for patients using a heel device comparedwith control subjects who did not use heel pro-tection. The device tested in this RCT was afoam body support covered in fabric that sus-pended the heel off the bed, with a second pieceof foam that was used to prevent foot drop (43).
In our previous research, performed in thesame acute care facility, the incidence of HPUoccurring on patients undergoing an acuteorthopedic procedure was 13·3%, 95% confi-dence interval (CI) 8–18% (44). In a furtherstudy, we followed acute orthopedic subjectspost-operatively as they were admitted anddischarged across health care settings (45).From this research we determined that 17%of subjects developed a HPU and that all newHPU occurred while they were in acute care(45). Therefore, intervention that prevents theoccurrence of HPU in the orthopedic popula-tion should be focused in the acute care setting.There is no current research that describes theimplementation of BPG to prevent HPU inacute orthopedic patients.
The purpose of this project was to develop,implement and evaluate a HPU preventionprogram. There were three steps involved inthis study:
1. Development of the HPU preventionprogram
i. To identify key stakeholders in thehospital and obtain their supportfor the implementation of a HPUprevention program.
ii. To involve clinical staff in thereview current knowledge andpractices and propose a simpleuniversal HPU prevention pro-gram.
iii. To select a HPU prevention deviceby identifying important selectioncriteria, using these criteria toselect three devices for trial, andselecting the device for universal
© 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc 29

Prevention of heel pressure ulcers
use based on patient and patientfeedback.
2. Implementation of the HPU prevention
Key Points
• this project was undertakenin six phases or parts: stake-holder involvement, develop-ment of HPU prevention pro-gram, identification of the bestHPU prevention device, prod-uct evaluation, HPU preventionprogram implementation andpost-incidence study
• the RNAO Toolkit on imple-mentation of Best PracticeGuidelines was used as aframework for this implemen-tation process
• as recommended in the toolkit,key stakeholders were identi-fied, analysed and engaged
programOver a 1-month period, a HPU cham-pion provided education about HPUand supported clinical staff to improvepatient mobility and use a heel protec-tion device.
3. Evaluation of the HPU prevention pro-gramThe incidence of new heel ulcers thatdevelop in this patient population whileon the orthopaedic service was deter-mined
METHODSPrior to beginning the study, approval for theproject was obtained from the research ethicsboard at the local university and the hospitalreview board.
SettingThe research took place in an academic tertiarycare facility, London Health Sciences Centre,University Hospital (UH). It is located in asmall urban centre in southwestern Ontario,Canada. The health centre has approximately850 beds. At UH, there are 36 inpatientacute orthopaedic surgery beds, and 15 otherorthopaedic surgery patients are often off ser-vice on other units. The hospital performs 1300elective hip and knee replacements and caresfor 200 patients with fractured hips per year.The prevention program was conducted in theemergency department (ED), the orthopaedicunit and the post-anaesthetic care unit (PACU)because the majority of the orthopaedic pati-ents were cared for in those places.
Study designThis project was undertaken in six phases orparts – stakeholder involvement, developmentof HPU prevention program, identification ofthe best HPU prevention device, product eval-uation, HPU prevention program implemen-tation and post-incidence study. This studywas performed in partial fulfilment of a PhDthesis, therefore a single and consistent person(termed HPU champion) lead the developmentand implementation of the project. Therefore,time spent by this advanced practice nursespent on the project was resourced through anursing doctoral research fellowship.
PREPARATION ANDDEVELOPMENT OF THE HPUPREVENTION PROGRAMThe RNAO Toolkit on implementation ofBPGs was used as a framework for thisimplementation process. As recommended inthe toolkit, key stakeholders were identified,analysed and engaged (27).
Part 1: Stakeholder involvementStakeholders included three key groups:(i) hospital administrators in surgery, medicine,the ED and the professional practice lead-ers (PPLs) for nursing, physical therapy andoccupational therapy; (ii) orthopaedic sur-geons and surgical residents and (iii) clini-cal staff providing direct care to orthopaedicpatients including nurse practitioners, occu-pational therapists (OTs), physical therapists(PTs), registered nurses (RNs) and registeredpractical nurses (RPN). Twelve administrators,all the orthopaedic surgeons and their resi-dents (n = 15), and forty orthopaedic clinicalstaff participated in the information sessions.It took a total of 18 months to complete thisvery important consultative process with keystakeholders prior to implementing the HPUprevention program.
Several consistent points were stressed inmeetings with the key stakeholders:
• A review of previous research conductedin other countries showed that a rel-atively high incidence of HPU in thispatient population is common and notjust a problem in our region.
• Our previous research showed a rela-tively high incidence of HPU (13%) inthis patient population and all of newHPU developed while patients were inacute care.
• The prevention of HPU would startwhen the patients entered the acutecare hospital and stop when they weredischarged from acute care.
• The solutions would be positive changesin practice; minimal focus would be onnegative practices and no blaming orfinger pointing would be tolerated.
• Interventions would be based on theRNAO BPGs.
• The HPU champion was willing to workcollaboratively on this project as part offulfilling requirements for a PhD.
30 © 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc

Prevention of heel pressure ulcers
Although background information andrationale for doing the project was consistent,the communication strategies and informationwere tailored for each of these groups. A for-mal presentation was delivered by the HPUchampion to the orthopaedic surgeons, fel-lows and residents. In this presentation, theextent of HPU in the acute orthopaedic pop-ulation was provided, the RNAO BPG’s andthe research support was reviewed, and theproposed intervention was outlined. The pre-sentation was followed by an opportunity foropen discussion, and their feedback was incor-porated into the project. From this meeting, allorthopaedic surgeons recognised the negativeimpact that pressure ulcer had on their patientoutcomes and they offered their support for theproject. Individual meetings were booked withdirectors, managers and PPLs. Because theseadministrative personnel were not involved indirect patient care, they received more infor-mation regarding resource use, patient safetyand patient outcomes. Concerns expressed byadministrators related to the cost to implementthe intervention program and the potentialcost of the device. One director had had apersonal experience with a family memberbreaking a hip and developing two HPU in hos-pital. This individual understood the impact ofthe HPU on the patient. Both the presenta-tion to orthopaedic surgeons and the meetingswith hospital administrators were conductedprior to approaching clinical staff. In this way,support from necessary key stakeholders wasobtained very early on in the project imple-mentation.
At staff meetings and lunch in-services, theHPU prevention project was outlined and theclinical staff members were provided withspecific details regarding how this initiativewould change their clinical practice. It wasemphasised that interventions needed to besimple and easily integrated with all patients.The clinical staff was very supportive of asimple intervention approach and easy-to-use device. They were also pleased that thedevice did not compromise or negativelyaffect the orthopedic condition/surgery. It wasimportant to the front line clinical staff thatthis initiative was supported fully by hospitaladministrators involved in their supervisionand by the orthopedic surgeons.
A key aspect to this consultative processwas that at all levels of discussion; feedback
on the proposed intervention was requested Key Points
• although background informa-tion and rationale for doingthe project was consistent, thecommunication strategies andinformation were tailored foreach of these groups
• a formal presentation wasdelivered by the HPU championto the orthopaedic surgeons,fellows and residents
• at staff meetings and lunch in-services, the HPU preventionproject was outlined and theclinical staff members wereprovided with specific detailsregarding how this initiativewould change their clinicalpractice
• the clinical staff was very sup-portive of a simple interven-tion approach and easy-to usedevice
• the study was to include anHPU prevention program thatwould be provided to allpatients on the orthopaedicservice who underwent lowerextremity orthopaedic surgery
and used to shape how the process proceeded.For example, initially the project was to focusonly on patients with fractured hips, butthe clinical staff indicated that heel ulcerswere a problem with all patients undergoinglower extremity surgery. The study was thenchanged to include a HPU prevention programthat would be provided to all patients onthe orthopaedic service who underwent lowerextremity orthopaedic surgery. This includednot only those individuals who requiredsurgical repair of a recent hip fracture but alsothose undergoing elective hip and knee jointreplacement surgery.
Part 2: Design of a specific HPUprevention programAll clinical staff members were invited toparticipate in a focus group or writtensurvey that reviewed current knowledge andpractices regarding HPU prevention. A letterof information was provided and consent wasassumed if the staff participated in the process.Twenty-seven staff members including asurgeon (n = 1), RNs (n = 15), RPNs (n = 4),PTs (n = 4) and OTs (n = 3) volunteered toparticipate in this process. The HPU championmet with the clinical staff that volunteered andasked for their responses to the following fourquestions:
1. What factors contribute to HPU devel-opment in the orthopaedic population?
2. What current practices are used for HPUprevention in the area in which youwork?
3. What are possible interventions that thehealth care team could implement thatwould help prevent HPU?
4. What are the current barriers andchallenges to the implementation of aHPU prevention program?
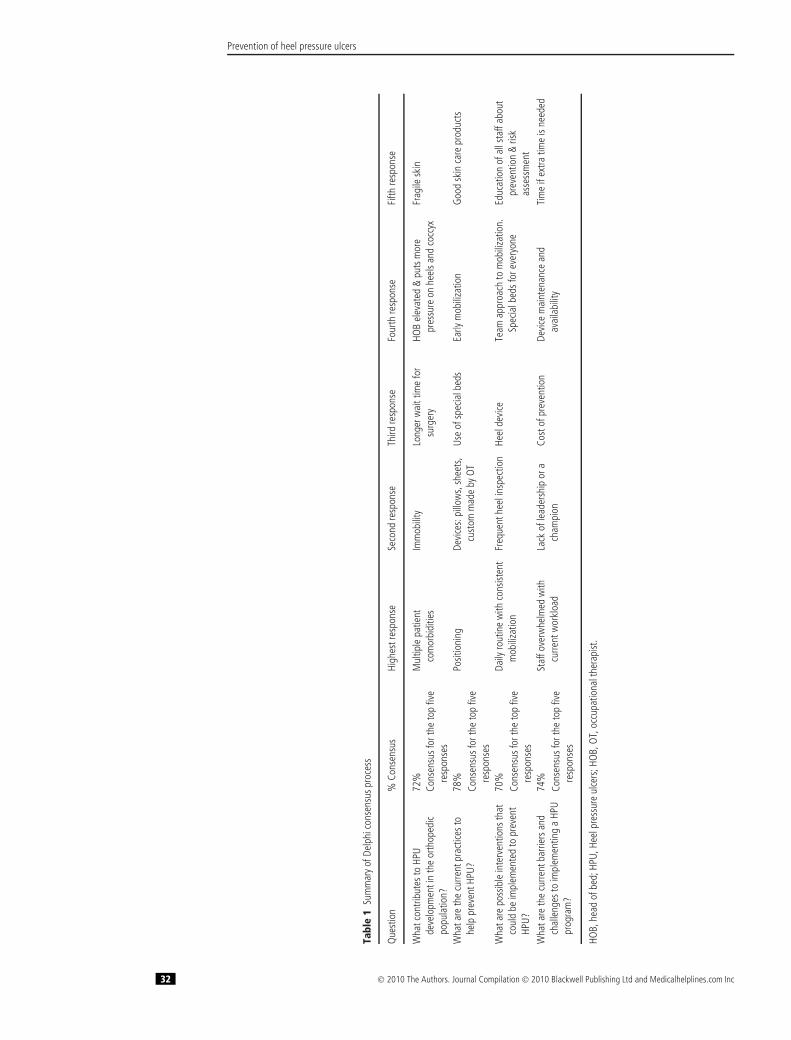
From these meetings, a list of responses wasgenerated from each participant and then aDephi process was used to build consensusand help prioritise responses (46). A collatedlist of responses from all 27 participantswas generated and circulated by e-mail, andparticipants were asked to rank the responsesto each of the questions. From this consensusprocess, the top five responses to each of thefour questions were identified (see Table 1). Ittook one iteration performed by e-mail to reach
© 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc 31
Prevention of heel pressure ulcers
Tabl
e1
Sum
mar
yof
Delp
hico
nsen
susp
roce
ss
Que
stio
n%
Cons
ensu
sHi
ghes
tres
pons
eSe
cond
resp
onse
Third
resp
onse
Four
thre
spon
seFi
fthre
spon
se
Wha
tcon
tribu
test
oHP
Ude
velo
pmen
tin
the
orth
oped
icpo
pula
tion?
72%
Mul
tiple
patie
ntco
mor
bidi
ties
Imm
obili
tyLo
nger
wai
ttim
efo
rsu
rger
yHO
Bel
evat
ed&
puts
mor
epr
essu
reon
heel
sand
cocc
yxFr
agile
skin
Cons
ensu
sfor
the
top
five
resp
onse
sW
hata
reth
ecu
rrent
prac
tices
tohe
lppr
even
tHPU
?78
%Po
sitio
ning
Devi
ces:
pillo
ws,
shee
ts,
cust
omm
ade
byO
TUs
eof
spec
ialb
eds
Early
mob
iliza
tion
Goo
dsk
inca
repr
oduc
tsCo
nsen
susf
orth
eto
pfiv
ere
spon
ses
Wha
tare
poss
ible
inte
rven
tions
that
coul
dbe
impl
emen
ted
topr
even
tHP
U?
70%
Daily
rout
ine
with
cons
isten
tm
obili
zatio
nFr
eque
nthe
elin
spec
tion
Heel
devi
ceTe
amap
proa
chto
mob
iliza
tion.
Spec
ialb
edsf
orev
eryo
neEd
ucat
ion
ofal
lsta
ffab
out
prev
entio
n&
risk
asse
ssm
ent
Cons
ensu
sfor
the
top
five
resp
onse
sW
hata
reth
ecu
rrent
barri
ers
and
chal
leng
esto
impl
emen
ting
aHP
Upr
ogra
m?
74%
Staf
fove
rwhe
lmed
with
curre
ntw
orkl
oad
Lack
ofle
ader
ship
ora
cham
pion
Cost
ofpr
even
tion
Devi
cem
aint
enan
cean
dav
aila
bilit
yTi
me
ifex
tratim
eis
need
edCo
nsen
susf
orth
eto
pfiv
ere
spon
ses
HOB,
head
ofbe
d;HP
U,He
elpr
essu
reul
cers
;HO
B,O
T,oc
cupa
tiona
lthe
rapi
st.
32 © 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc

Prevention of heel pressure ulcers
our goal of at least 67% consensus amongstresponders. Despite several reminders, wehad only a 52% response rate from the 27participants to these e-mail based iterations.
1. Factors contributing to HPU developmentin the orthopedic population. The followingfive themes arose:
• Patient factors including advanced age,fragile skin, comorbidities [periph-eral vascular disease (PVD), diabetes,hypoxia, dementia, delirium] and painmanagement (either not well managedor overly sedated).
• Positioning and mobilisation, for exampleimmobility post-operatively; head of bedelevated so there is pressure on the heels;operative leg not easily moved post-operatively; exercise for knee replace-ment patents requires them to drag theirheel up and down the bed; and patientslying on fracture board until cervicalspine is cleared.
• Hospital materials and resources, forexample current hospital mattresses aretoo soft; reduced access to pressure reliefmattresses; ED stretchers do not havepressure reduction foam on them; andlack of access to pressure relief surfaces.
• Staff factors such as over use of Foleycatheters and not getting patients outof bed to toilet; differing expectations ofstaff regarding mobilisation, for examplesome staff thought that this was theresponsibility of the PT; risk assessmentnot being performed; and lack of knowl-edge on how to prevent HPU.
• System factors such as wait time in ERand reluctance of administrative staff tolisten to complaints about heel ulcers.
2. Current practices that reduce the risk ofheel ulcersInterventions that they are currently doingto prevent HPU included the use of pillowsand folded flannels, use of special surfaces,early mobilisation, good skin care products,automatic referrals to PT and OT for certainpatients, frequent skin assessment, positioning,following the pathway for hip and kneereplacements, educating patients on how tolift their heels and using a multidisciplinaryapproach.
The hospital had already implementedcertain aspects of best practice, such as pressure
Key Points
• staff identified 29 potentialinterventions that they couldadd to current practices thatcould help prevent HPU
• examples included a dailyroutine of mobilisation, use of aheel protective device, involvethe ED and PACU, managepain, use simple approachesthat achieve multiple goals,provide pressure relief for everypatient, consult the dieticianfor all patients with fracturedhips, check albumin levelson every patient, have bettermattresses for stretchers, usevisual cues like pictures tohelp staff, teach patients andfamilies how to prevent HPU,and have all patients wearsocks to help with friction
• examples of the 14 barriersthat were identified were lackof knowledge of options avail-able for prevention, gettingthe ED to see HPU preventionas a priority, availability andmaintenance of devices, hav-ing extra time if it is needed,process of implementation isoverwhelming, gaining supportfrom administration, improvinglimited dietary support, blam-ing approach and the cost ofprevention if extra resourceswere needed
reduction foam replacement mattresses on allbeds, the Braden Scale risk assessment, skincare protocols and access to interdisciplinaryteam members by referral. Each surgeon alsohad a preventative program for deep veinthrombosis, which is a common complicationthat can develop in this patient population. Allof these current practices were not changed.The HPU prevention program dealt only withspecific interventions based on the RNAO BPGon prevention of pressure ulcers.
A final examination of current practicesinvolved a visit by the HPU champion to theoperating room (OR) to observe positioning ofpatients undergoing hip and knee surgeries.From this observation, she determined that theposition in which patients were placed duringsurgery did not result in sustained pressures onthe heel and therefore no changes in practicewere recommended in the OR. Rather, thisHPU prevention program would focus onstrategies for patients in the ED and once theywere in the post-operative recovering period.
3. Additional practices that could helpprevent HPUsStaff identified 29 potential interventions thatthey could add to current practices that couldhelp prevent HPU. Examples included a dailyroutine of mobilisation, use of a heel protectivedevice, involve the ED and PACU, managepain, use simple approaches that achievemultiple goals, provide pressure relief forevery patient, consult the dietician for allpatients with fractured hips, check albuminlevels on every patient, have better mattressesfor stretchers, use visual cues like pictures tohelp staff, teach patients and families how toprevent HPU, and have all patients wear socksto help with friction.
4. Barriers and challenges to implementationof a HPU prevention programExamples of the 14 barriers that were identifiedwere lack of knowledge of options available forprevention, getting the ED to see HPU preven-tion as a priority, availability and maintenanceof devices, having extra time if it is needed,process of implementation is overwhelming,gaining support from administration, improv-ing limited dietary support, blaming approach
© 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc 33

Prevention of heel pressure ulcers
and the cost of prevention if extra resourceswere needed.
A working group of made up of sevenkey opinion leaders: the coordinator, clinicaleducator, two RNs, one RPN, one OT andone PT (total n = 7) from ED, PACU andthe orthopaedic unit was formed. They weretasked with taking the consensus documentand developing clinically based interventionsthat would prevent HPU. Recommendedchanges combined responses from the Delphiprocess with RNAO BPGs on risk assessmentand prevention of pressure ulcer (24).
An overarching principle that arose from the
Key Points
• offloading the heel was basedon previous research thatsuggested that this was theonly way to prevent pressureinduced skin damage in theheel region
• they selected three heel pro-tective devices that best metthe criteria above: a hospitalpillow, the Repose™boot anda wedge
Delphi process was that the program shouldbe implemented on all patients on all threeunits (ED, PACU and Orthopaedic) and runfrom admission until patients were mobile.Moreover, everyone thought the programshould be simple.
The following interventions were selectedfor implementation:
1. Use a heel device to be chosen duringa product evaluation process, on everypatient. The device will be cleaned bypatient care assistants and be stored ineach patient’s room where pillows arestored.
2. Mobilise all orthopaedic patients. Thegoal is to mobilise all patients unlesscontraindicated (e.g. non weight bearingstatus). Mobilisation involves all mem-bers of every heath care discipline (notjust the PTs). Getting patients out of bedand on their feet is helpful for manythings including preventing HPU.
Part 3: Identification of the best HPUprevention deviceA three-step process was undertaken in orderto select an appropriate HPU preventiondevice. The first step involved orthopaedicclinicians who identified key criteria to beconsidered when selecting a heel protectiondevice. Then a small group of wound carespecialists applied these criteria to select threedevices from a long list of commerciallyavailable products. These devices were theytrialed on the orthopaedic service and a finalsingle device was selected based on feedbackgathered from both patients and cliniciansusing the device.
To determine key criteria for selection ofa heel device, a group of 12 experienced
clinicians (RN, OT, PT and coordinator)from various areas of the orthopaedic service(orthopaedic unit, ED and PACU) were invitedto a 1·5-hour meeting. A nominal groupprocess (47) was used to come to 100%agreement that the top criteria for heel bootselection in order of priority are:
1. cleanable, reusable and approved byinfection control,
2. ease of use,3. price,4. effectiveness without side effects,5. comfortable to patient,6. BPG supports the device,7. Available to purchase or make.
A group of five wound care experts reviewedall devices available on the market. They wereasked to use a 3-point Likert scale to rank theHPU devices based on how well they met thekey criteria. The higher the score, the morelikely it was that the device met the criteria.It was determined that if the device did notmeet infection control criteria completely ordid not float the heel off the bed, it would notbe considered. The infection control concernwas prompted by the increasing concernabout hospital-acquired infections and multi-resistant organisms. Offloading the heel wasbased on previous research that suggested thatthis was the only way to prevent pressure-induced skin damage in the heel region. Theyselected three heel protective devices that bestmet the criteria above: a hospital pillow, theRepose™ boot and a wedge. The wedge we hadselected was no longer available so the HPUchampion and two orthopaedic OT’s customdesigned a wedge.
Part 4: Product evaluationPrior to initiation of the product evaluation, allclinical staff and orthopaedic surgeons weresent electronic messages about the productevaluation. Orthopaedic surgeons were givenan opportunity to raise any concerns aboutorthopaedic patients being randomly selectedto use a heel protection device during the trial.Three of nine orthopaedic surgeons respondedto e-mails stating that they had no concernsabout testing the devices on any of theirpatients and that they were supportive of thisproject. An additional step taken just prior tothe trial of these three products was that theHPU champion met with staff daily on the
34 © 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc

Prevention of heel pressure ulcers
orthopaedic unit for 1 week to remind themabout the upcoming trial. She also met withthe patient care assistants to review all theprocesses for cleaning and storing the devicesunder trial.
Evaluation of the selected heel protectiondevices occurred over a 14-day period inJanuary 2008. All consecutive patients withorthopaedic condition or surgery below thewaist (lower extremity) that were admitted tothe orthopaedic service over a 2-week periodwere recruited to participate in the trial. A letterof information about the study was providedto clinical staff and patients on the orthopaedicservice. Written consent was obtained fromthose who completed an evaluation form aboutthe device they used. Patients could refuseto use a device. Because the use of a heeloffloading device is considered best practice,all patients on the orthopaedic service wereoffered a heel protection device. Howeverwhich one of the three devices being testedthe patient received was determined randomlyusing a table of random numbers. A total of 72subjects participated with each person testingonly one device. Of these 72 subjects, 27 testedthe Repose boot, 23 the wedge and 22 thepillow.
A photo of the device used on a particularpatient was placed above his or her bedto ensure that patients received the correctdevices that they had been assigned. Thesephotos also showed the correct use of thedevice. Daily visits by the HPU champion werecarried out to reinforce the correct use of eachdevice, solve problems and obtain feedback.
Separate evaluation forms were developedfor patients and clinical staff and the HPUchampion recorded any oral feedback that wasvolunteered by either patients or clinicians.Both written and verbal feedback that wasgathered was based on the key criteriaidentified during the consensus process. Anyside effects related to the device were recorded;this included the development of a HPU orany other complication. At the end of theevaluation, the device with the most favuorablefeedback and the fewest complaints wereselected for use as the HPU prevention deviceto be used in the prevention program.
Device failures, where the device wasremoved from the patients because of clinicalconcerns, occurred with four subjects whena pillow was used to protect the heel. All
four of these subjects had undergone knee Key Points
• evaluation of the selected heelprotection devices occurredover a 14-day period in January2008
• a total of 72 subjects partici-pated with each person testingonly one device. Of these 72subjects, 27 tested the Reposeboot, 23 the wedge and 22 thepillow
• none of the 72 patients devel-oped a HPU during the 14-dayproduct trial
replacement surgery. They had relatively shortlegs and the pillow bunched up behindthe knee, thereby interfering with the newlyreplaced joint. The wedge had a device failureon a subject with a fractured hip because itwas not high enough to keep the subject’ship aligned in traction. No device failureswere reported by subjects using the Reposeboot™. All patients who reported a devicefailure were provided with an alternate heelprotection device, and no further evaluationwas recorded. All three devices were liked anddisliked by some subjects and staff.
In general, all the devices were easy to clean.Six RNs stated that all three devices werehelpful in preventing HPU and that they wouldbe happy using any one of them. Two patientswere admitted with existing bilateral heelulcers; one patient was randomly selected touse the pillow and the other to use the wedge.Both patients had an improvement in the heelulcers and neither patient had deterioration.None of the 72 patients developed a HPUduring the 14-day product trial. A commoncomplaint about all three devices was that itdid not stay in place. Staff reported that aspatients recovered and were more mobile, thedevice was less likely to stay in place.
Eighteen patients and staff gave specificpositive feedback regarding the pillow. Someof the comments included: ’My heels feel betteralready’; ’My heels feel better with the pillow’;’I had the pillow when I first came back fromsurgery and it was excellent. Now I am movingabout and don’t need it’. Negative commentswere received from 15 staff and patientsregarding the pillow. Four main themes arose:the pillow was not seen as a device, it was notalways put in place; it did not stay in place andhad to be repositioned; there was no standardsize so some pillows were too thin and sometoo thick; and it caused pain in the Achillestendon.
The Repose boot™ had 19 positive com-ments. Some of the comments included: ’Com-fortable and kept leg in proper alignment’; ’Theboots keep my hips in alignment’; ’My heelswere sore, and now that I have the boots, theyare not’; and ’My heels feel better’. The Repose™ boot received 19 complaints. Ten peopleindicated that it hurt the calf. The second mostcommon complaint was that it did not stay inplace.
© 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc 35

Prevention of heel pressure ulcers
The wedge had 28 positive comments.Key Points
• the wedge had 28 posi-tive comments and was theselected heel device
• during the 1-month implemen-tation of the heel ulcer preven-tion program, no heel ulcersdeveloped on any patient onthe orthopedic service
Several patients captured their approval in thefollowing comments: ’Wish I had this 2 yearsago when my heel burned and hurt’; ’I thinkthis wedge helps; can we keep it?’; ’The wedgewas comfortable, and I did not develop ulcers’.Staff and patients liked the wedge as it was easyto use and comfortable. The wedge received 13negative comments. The most common themewas that it did not stay in place, and there weretwo comments that it was not high enough forheavy legs.
HPU PREVENTION PROGRAMIMPLEMENTATIONThe HPU prevention program that wasshaped by an extensive pre-implementationconsultation process was then implementedover a 1-month period. In addition to using theselected heel device (the wedge), a mobilisationprogram was instituted that promoted earlyand frequent mobilisation of all patients by allteam members. The wedge and mobilisationinterventions were implemented universallywith all patients on the orthopaedic servicewho underwent lower extremity surgery(below the waist).
Prior to the implementation phase of thisHPU prevention program, the HPU championsent out e-mails to remind all staff ofthe commencement of the HPU preventionprogram. In addition, she visited all three unitsdaily for 2 weeks prior to the actual startdate and conducted direct education aboutthe program. The percentage of staff receivingdirect education prior to the implementationwas 60% for the orthopaedic unit, 67% for thePACU and 50% for the ED. This education waseither one-on-one or with a few staff at thebedside.
During the implementation period, theHPU champion visited all three units andsaw patients daily for 1 month, at whichtime further education took place, thereforeincreasing the proportion of staff who receivededucation. Initially, the HPU champion spent4 hours a day on the units, but as theproject progressed, this time was reducedto 1·5 hours. Finally, the HPU championmade a point of praising the staff for anyeffort to implement the prevention strategiesand everyone involved was motivated withimproved outcomes. During the 1-monthimplementation of the heel ulcer prevention
program, no heel ulcers developed on anypatient on the orthopedic service.
EVALUATION OF PROGRAMOne month after the implementation began; theincidence of HPU was re-evaluated. Patientswho were admitted to LHSC UH for fracturesor surgery below the waist were approachedconsecutively from May 2008 to June 2008.The methods used were identical to a priorstudy by the research team when the pre-implementation was completed (44). Briefly,this involved direct examination of the heels ofpatients on admission and prior to dischargefrom the orthopaedic service.
When using an alpha level of 0·05 and betaof 0·20, the sample size to detect a changein incidence rate from 13·3% to 2% afterimplementation of our program would requireus to follow 38 patients (48).
The incidence estimates were expressed aspercentages with 95% confidence intervals(CI) (49).
RESULTSAn important lesson learned during prepa-ration and development of the heel ulcerprevention program was the need to obtainsupport from hospital administration andorthopaedic surgeons prior early in the pro-cess. This support was facilitated by having aprior incidence study of the target populationthat provided an accurate assessment of thenumber of patients who develop HPU whileon their service. Support from supervisors andsurgeons were key to involvement by clinicalstaff.
The clinical staff was involved in shapingthe nature of the HPU program. Through thisconsensus process, it was decided that theprevention program should be applied univer-sally to all patients undergoing lower extremitysurgery. Based on the current practices alreadyin place, this program focused in three areas:(i) education of staff, (ii) a team approach toearly and frequent patient mobilisation and(iii) use of a heel protection device.
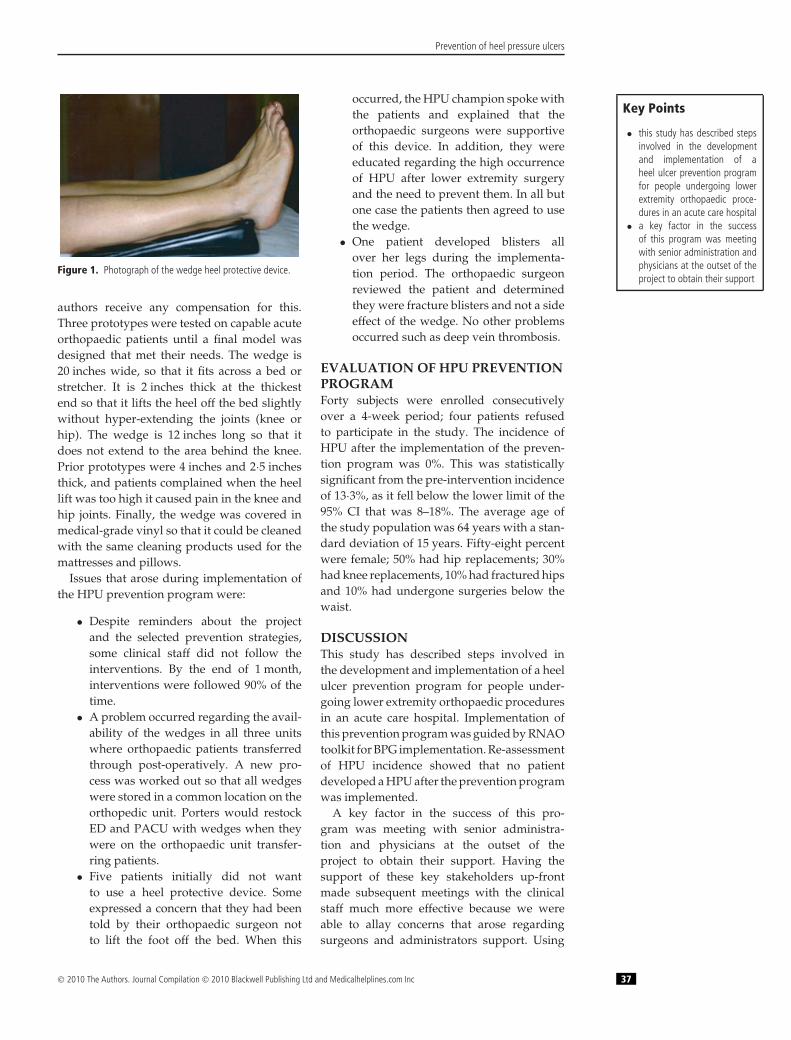
The heel protection device that was selectedwas the wedge. The wedge was designedby the primary author and two OTs (seeFigure 1 for a photograph). A third partycompany (Remington Medical) then made theprototypes for the study and now sells thisproduct in Canada. Neither the OTs nor the
36 © 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc
Prevention of heel pressure ulcers
Figure 1. Photograph of the wedge heel protective device.
authors receive any compensation for this.Three prototypes were tested on capable acuteorthopaedic patients until a final model wasdesigned that met their needs. The wedge is20 inches wide, so that it fits across a bed orstretcher. It is 2 inches thick at the thickestend so that it lifts the heel off the bed slightlywithout hyper-extending the joints (knee orhip). The wedge is 12 inches long so that itdoes not extend to the area behind the knee.Prior prototypes were 4 inches and 2·5 inchesthick, and patients complained when the heellift was too high it caused pain in the knee andhip joints. Finally, the wedge was covered inmedical-grade vinyl so that it could be cleanedwith the same cleaning products used for themattresses and pillows.
Issues that arose during implementation ofthe HPU prevention program were:
• Despite reminders about the projectand the selected prevention strategies,some clinical staff did not follow theinterventions. By the end of 1 month,interventions were followed 90% of thetime.
• A problem occurred regarding the avail-ability of the wedges in all three unitswhere orthopaedic patients transferredthrough post-operatively. A new pro-cess was worked out so that all wedgeswere stored in a common location on theorthopedic unit. Porters would restockED and PACU with wedges when theywere on the orthopaedic unit transfer-ring patients.
• Five patients initially did not wantto use a heel protective device. Someexpressed a concern that they had beentold by their orthopaedic surgeon notto lift the foot off the bed. When this
occurred, the HPU champion spoke withthe patients and explained that theorthopaedic surgeons were supportiveof this device. In addition, they wereeducated regarding the high occurrenceof HPU after lower extremity surgeryand the need to prevent them. In all butone case the patients then agreed to usethe wedge.
• One patient developed blisters allover her legs during the implementa-tion period. The orthopaedic surgeonreviewed the patient and determinedthey were fracture blisters and not a sideeffect of the wedge. No other problemsoccurred such as deep vein thrombosis.
EVALUATION OF HPU PREVENTIONPROGRAMForty subjects were enrolled consecutively
Key Points
• this study has described stepsinvolved in the developmentand implementation of aheel ulcer prevention programfor people undergoing lowerextremity orthopaedic proce-dures in an acute care hospital
• a key factor in the successof this program was meetingwith senior administration andphysicians at the outset of theproject to obtain their support
over a 4-week period; four patients refusedto participate in the study. The incidence ofHPU after the implementation of the preven-tion program was 0%. This was statisticallysignificant from the pre-intervention incidenceof 13·3%, as it fell below the lower limit of the95% CI that was 8–18%. The average age ofthe study population was 64 years with a stan-dard deviation of 15 years. Fifty-eight percentwere female; 50% had hip replacements; 30%had knee replacements, 10% had fractured hipsand 10% had undergone surgeries below thewaist.
DISCUSSIONThis study has described steps involved inthe development and implementation of a heelulcer prevention program for people under-going lower extremity orthopaedic proceduresin an acute care hospital. Implementation ofthis prevention program was guided by RNAOtoolkit for BPG implementation. Re-assessmentof HPU incidence showed that no patientdeveloped a HPU after the prevention programwas implemented.
A key factor in the success of this pro-gram was meeting with senior administra-tion and physicians at the outset of theproject to obtain their support. Having thesupport of these key stakeholders up-frontmade subsequent meetings with the clinicalstaff much more effective because we wereable to allay concerns that arose regardingsurgeons and administrators support. Using
© 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc 37

Prevention of heel pressure ulcers
e-mail and personal reminders was helpful toKey Points
• our results strongly suggestthe program was successfulbecause no HPUs were iden-tified during or within 1 monthof implementing the preven-tion program
• it is possible that the reduc-tion in the number of peoplewho acquired heel ulcers afterthe prevention program wasimplemented was influencedby the younger, healthier sam-ple population included post-intervention
keep administrators and clinical staff engagedand supportive throughout the project. In aCanadian study on pressure ulcers and imple-mentation of evidenced-based nursing prac-tice, a lack of visible senior nursing leadershipwas found to be a barrier to the implemen-tation of BPG on PU (37). In a US studyof a program to prevent HPU, incidence ofHPU stayed essentially the same after the pro-gram implementation. The authors attributedtheir lack of success to a lack of organisa-tional approval and the fact that managementfailed to convey messages to staff about theimportance of the project and their supportfor it (50).
In this study, the Delphi process (46) wasused so that all staff would have input, andno one person could influence the groupto make decisions because the voting wascarried out privately. The nominal groupprocess (47) was used to determine keycriteria for choosing a heel protection device.This consensus method was very efficient andprevented any one person from overpoweringthe group process. The selection process usedin this study for determining which devicesshould be tested was transparent and objective.This systematic process also served to addressany issues related to commercial interests andlimited biases and conflicts of interest. Theinvolvement of clinical staff and patients in thedecisions about which heel protective deviceto adopt for use in the heel ulcer preventionprogram also served to promote adoption ofthe program and compliance with the use ofthe heel device. All of these methodologies areunique to this project and have not been usedpreviously in other pressure ulcer preventionprograms.
We elected to apply this prevention programuniversally to all orthopaedic patients who hadundergone surgery to the lower extremity. Thisis in contrast to prevention programs that havea risk assessment tool like the Braden scaleto identify high-risk individuals for whomthe prevention program is applied. We didnot elect to use a risk assessment tool in thisprevention program because all orthopaedicpatients are likely to be high risk, and adoptionand use of risk assessment tools by staff at thisfacility has been historically been low. Thisuniversal approach allowed the program tobe simple and efforts of clinical staff could
be focused on implementing the preventionstrategies rather than performing assessments.
A simple foam wedge with vinyl coatingwas selected and used as the heel protectiondevice in this study. The effectiveness of thisdevice as a heel protection device has not beentested previously. We organised for the specificdimensions of the wedge to be made by a localcompany for a cost of $48·35 cdn per wedge.However, given the simple design it could beeasily produced by other sources. We electedto use only one size of the wedge. The ease ofadoption of a program that has a one size fitsall approach to the heel protection device wereobvious. We recognize that other sizes mayhave better suited certain leg and body shapes.For example, people with larger and heavierlegs may have benefited from a thicker wedge.We decided to lay a folded sheet underneaththe wedge in these cases to lift the heels off thebed. This simple approach was appropriate forall but 1 of 23 patients who tested the wedgeand was in traction.
Previous work in this health care settingshowed a heel ulcer incidence of 13·3% (95%CI8–18%) (44). To obtain this estimate of the pro-portion of patients undergoing leg surgerywho develop HPU while on this orthopedicservice, we directly examined both heels of150 consecutive patients. In this study, werepeated the same methodology using 40 con-secutive patients to evaluate the effectivenessof the HPU prevention program. Our resultsstrongly suggest the program was successfulbecause no HPUs were identified during orwithin 1 month of implementing the preven-tion program. This reduction in HPU incidencepost-implementation is significant because it iswell below the lower 95% confidence limitaround the estimate of HPU incidence pre-intervention. However, the sample populationin the present report was younger (63 versus77 years), included more people with hip frac-tures (33% versus 10%), and contained a lowerproportion of females (58% versus 69%) com-pared with the population used to estimateHPU incidence prior to intervention. There-fore, it is possible that the reduction in the num-ber of people who acquired heel ulcers afterthe prevention program was implemented wasinfluenced by the younger, healthier samplepopulation included post-intervention. How-ever, the higher proportion of female hipfracture patients in the post-implementation
38 © 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc

Prevention of heel pressure ulcers
sample would offset this. Collectively, webelieve these slight differences in pre- and post-implementation samples would even out andit is likely that these populations had a similarrisk of heel ulcer development.
The sample population used to estimate theHPU incidence post-implementation was fairlysmall (n = 40) compared with other studiespublished in this field. However, we used asample size calculation by Baumgarten (48) todetermine that a sample size of 38 or greaterwould give us 80% power to detect a significantdifference in incidence between the pretestvalue of 13·3 and a post-implementation valueof 2%.
The implementation and evaluation periodswere fairly short in duration (each lasting1 month). However, given that HPU weretotally eliminated after a 1-month interventionsuggested the intervention period was longenough to produce the desired response. Ourevaluation period performed within 1 monthof program implementation allows us tocomment on the short-term effect of thisprogram. It would be of interest to repeat theincidence of HPU in a few months time to seewhether the heel ulcer prevention program hashad lasting effects.
CONCLUSIONHPUs are a common and serious healthconcern, but they can be prevented in mostpatients with a universal HPU preventionprogram that incorporated patient and staffinput.
This research project was funded by theRegistered Nurses Association of Ontario,Canadian Nurses Foundation, and LondonHealth Sciences Center.
REFERENCES1 Graves N, Birrell FA, Whitby M. Modeling the
economic losses from pressure ulcers amonghospitalized patients in Australia. Wound RepairRegen 2005;13:462–67.
2 Allman RM, Goode PS, Burst N, Bartolucci AA,Thomas DR. Pressure ulcers, hospital complica-tions, and disease severity: impact on hospitalcosts and length of stay. Adv Wound Care1999;12:22–30.
3 Brandeis GH, Morris JN, Nash DJ, Lipsitz LA. Theepidemiology and natural history of pressureulcers in elderly nursing home residents. JAMA1990;264:2905–09.
4 Allman RM, Laprade CA, Noel LB. Pressure soresamong hospitalized patients. Ann Intern Med1986;105:337–42.
5 Langemo DK, Melland H, Hanson D, Olson B,Key Points
• it would be of interest to repeatthe incidence of HPU in a fewmonths time to see whether theheel ulcer prevention programhas had lasting effects
Hunter S. The lived experience of having apressure ulcer: a qualitative analysis. Adv SkinWound Care 2000;13:225–35.
6 Jacobs TS, Kerstein MD. Is there a difference inoutcome of heel ulcers in diabetic and non-diabetic patients? Wounds 2000;12:96–101.
7 Mayrovitz HN, Sims N. Effects of different cyclicpressurization and relief patterns on heelskin blood perfusion. Adv Skin Wound Care2002;15:158–64.
8 Huber J, Reddy R, Pitham T, Huber D. Increasingheel skin perfusion by elevation. Adv SkinWound Care 2008;21:37–41.
9 Schoonhoven L, Defloor T, Grypdonck MHF. Inci-dence of pressure ulcers due to surgery. J ClinNurs 2002;11:479–87.
10 Versluysen M. Pressure sores in elderly patients.J Bone Joint Surg 1985;67:10–13.
11 Vangilder C, MacFarlane GD, Meyer S. Feature:results of nine international pressure ulcerprevalence surveys: 1989 to 2005. Ostomy WoundManage 2008;54:40–54.
12 Bours GJ, Halfens RJ, Lubbers M, Haalboom JR. Thedevelopment of a national registration formto measure the prevalence of pressure ulcersin The Netherlands. Ostomy Wound Manage1999;45:28–33, 36.
13 Barczak CA, Barnett RI, Childs EJ, Bosley LM.Fourth national pressure ulcer prevalence sur-vey. Advances in wound care : the journal forprevention and healing 1997;10:18–26.
14 Goodridge DM, Sloan JA, LeDoyen YM, McKen-zie J, Knight WE, Gayari M. Risk-assessmentscores, prevention strategies, and the incidenceof pressure ulcers among the elderly in fourCanadian health-care facilities. Can J Nurs Res1998;30:23–44.
15 Horn SD, Bender SA, Bergstrom N, Cook AS, Fer-guson ML, Rimmasch HL, Sharkey SS, Voss AC.Description of the national pressure ulcerlong-term care study. J Am Geriatr Soc2002;50:1816–25.
16 Meehan M. National pressure ulcer prevalencesurvey. Adv Wound Care 1994;7:27–30, 34, 36.
17 Baumgarten M, Margolis D, Berlin JA, Strom BL,Garino J, Kagan SH, Kavesh W, Carson JL. Riskfactors for pressure ulcers among elderlyhip fracture patients. Wound Repair Regen2003;11:96–103.
18 Cuddigan J, Berlowitz DR, Ayello EA. Prevalence,incidence, and implications for the future: anexecutive summary of the national pressureulcer advisory panel. Adv Skin Wound Care2001;14:208–15.
19 Gunningberg L. Implementation of risk assessmentand classification of pressure ulcers as qualityindicators for patients with hip fractures. J ClinNurs 1999;8:396–406.
20 Bours GJJW, Halfens RJG, Berger MPF, Abu-Saad HH, Grol RTPM. Development of a modelfor case-mix adjustment of pressure ulcer preva-lence rates. Med Care 2003;41:45–55.
© 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc 39

Prevention of heel pressure ulcers
21 Fisher AR, Wells G, Harrison MB. Factors associatedwith pressure ulcers in adults in acute carehospitals. Adv Skin Wound Care 2004;17:80–90.
22 Lindgren M, Unosson M, Fredrikson M, Ek A.Immobility – A major risk factor for develop-ment of pressure ulcers among adult hospitalizedpatients: a prospective study. Scand J of CaringSci 2004;18:57–64.
23 Young J, Nikoletti S, McCaul K, Twigg D, Morey P.Risk factors associated with pressure ulcerdevelopment at a major western Australianteaching hospital from 1998 to 2000: secondarydata analysis. J Wound Ostomy Continence Nurs2002;29:234–41.
24 MacLeod FE, Harrison MB, Graham ID. The processof developing best practice guidelines for nursesin Ontario: risk assessment and preventionof pressure ulcers. Ostomy Wound Manage2002;48:30–32, 34.
25 Panel for the prediction and prevention of pressureulcers in adults. Pressure ulcers in adults:prediction and prevention. Clinical Guideline,Number 3, AHCPR publication no. 92-0097.Rockville, MD, USA: Agency for Health CarePolicy and Research, Public Health Service, USDepartment of Health and Human Services.
26 Dolynchuk K, Keast D, Campbell K, Houghton P,Orsted H, Sibbald G, et al. Best practices for theprevention and treatment of pressure ulcers.Ostomy Wound Manage 2000;46:38–52; quiz 53.
27 Registered Nurses Association of Ontario. Toolkit:Implementation of clinical practice guidelines,2002.
28 Ratliff CR, Bryant DE, Dutcher JA. Guideline forprevention and management of pressure ulcers.Glenview, Ill: Wound Ostomy Continence NursesSociety, 2003.
29 Baldelli P, Paciella M. Creation and implementationof a pressure ulcer prevention bundle improvespatient outcomes. Am J Med Qual 2008;23:136–42.
30 Sacharok C, Drew J. Use of a total quality manage-ment model to reduce pressure ulcer prevalencein the acute care setting. J Wound Ostomy Conti-nence Nurs 1998;25:88–92.
31 Robinson C, Gloekner M, Bush S, Copas J, Kearns C,Kipp K, Labath B, Wentz D. Determining theefficacy of a pressure ulcer prevention programby collecting prevalence and incidence data:a unit-based effort. Ostomy Wound Manage2003;49:44–6, 48.
32 McInerney JA. Reducing hospital-acquired pressureulcer prevalence through a focused preventionprogram. Adv Skin Wound Care 2008;21:75–8.
33 Hunter SM, Cathcart-Silberberg T, Langemo DK,Olson B, Hanson D, Burd C, Sauvage TR. Pressureulcer prevalence and incidence in a rehabilitationhospital. Rehabil Nurs 1992;17:239–42.
34 Langemo DK, Olson B, Hunter S, Hanson D,Burd C, Cathcart-Silberberg T. Incidence and pre-diction of pressure ulcers in five patient caresettings. Decubitus 1991;4:25–26, 28, 30 passim.
35 Bergquist S, Frantz R. Pressure ulcers in community-based older adults receiving home health care.Prevalence, incidence, and associated risk factors.Adv Wound Care 1999;12:339–51.
36 Langemo D, Thompson P, Hunter S, Hanson D,Anderson J. Heel pressure ulcers: stand guard.Adv Skin Wound Care 2008;21:282–292; quiz293–4.
37 Clarke HF, Bradley C, Whytock S, Handfield S, VanDer Wal R, Gundry S. Pressure ulcers: implemen-tation of evidence-based nursing practice. J AdvNurs 2005;49:578–90.
38 Frain R. Decreasing the incidence of heel pressureulcers in long-term care by increasing awareness:results of a 1-year program. Ostomy WoundManage 2008;54:62–7.
39 Nicosia G, Gliatta AE, Woodbury MG,Houghton PE. The effect of pressure-relievingsurfaces on the prevention of heel ulcers in avariety of settings: A meta-analysis. Int Wound J2007;4:197–207 232–233.
40 Gilcreast DM, Warren JB, Yoder LH, Clark JJ, Wil-son JA, Mays MZ. Research comparing three heelulcer-prevention devices. J Wound Ostomy Con-tinence Nurs 2005;32:112–20.
41 Tymec AC, Pieper B, Vollman K. A comparison oftwo pressure-relieving devices on the preventionof heel pressure ulcers. Adv Wound Care1997;10:39–44.
42 Walsh JS, Plonczynski DJ. Evaluation of a protocolfor prevention of facility-acquired heel pressureulcers. J Wound Ostomy Continence Nurs2007;34:178–83.
43 Cadue J, Karolewicz S, Tardy C, Barrault C,Robert R, Pourrat O. Prevention of heel pressuresores with a foam body-support device. A ran-domized controlled trial in a medical intensivecare unit. Presse Med 2008;37:30–6.
44 Campbell KE, Woodbury MG, Houghton PE.Incidence and risk factors of heel pressureulcers in an acute orthopedic population. OstomyWound Manage In press.
45 Campbell KE, Woodbury MG, Labte T, LesMesurierA, Houghton PE. Heel ulcers develop in anorthopedic population while in an acute carehospital. Ostomy Wound Manage Submitted Nov2009.
46 Powell C. The Delphi technique: myths and realities.J Adv Nurs 2003;41:376–82.
47 McMurray AR. Three decision-making aids: brain-storming, nominal group, and Delphi technique.J Nurses Staff Dev 1994;10:62–5.
48 Baumgarten M. Designing prevalence and incidencestudies. Adv Wound Care 1998;11:287–93.
49 Colton T. Statistics in medicine. 1st edn. Boston:Little Brown and Company, 1974.
50 McElhinny ML, Hooper C. Reducing hospital-acquired heel ulcer rates in an acute care facility:an evaluation of a nurse-driven performanceimprovement project. J Wound Ostomy Conti-nence Nurs 2008;35:79–83.
40 © 2010 The Authors. Journal Compilation © 2010 Blackwell Publishing Ltd and Medicalhelplines.com Inc