implementation of a cancer prevention program for working class, multiethnic populations
TRANSCRIPT
www.elsevier.com/locate/ypmed
Preventive Medicine 38 (2004) 766–776
Implementation of a cancer prevention program for working class,
multiethnic populations
Rebecca Lobb, M.P.H.,a,* Elizabeth Gonzalez Suarez, M.A.,b Martha E. Fay, M.P.H.,c
Caitlin M. Gutheil, M.S.,b Mary K. Hunt, M.P.H.,b
Robert H. Fletcher, M.D.,a,d and Karen M. Emmons, Ph.D.b,c
aDepartment of Ambulatory Care and Prevention, Harvard Pilgrim Health Care, Boston, MA 02215, USAbDana-Farber Cancer Institute, USA
cHarvard School of Public Health, Boston, MA 02115, USAdHarvard Medical School, Boston, MA 02115, USA
Available online 19 March 2004
Abstract
Background. This paper describes the implementation of the Healthy Directions-Health Centers intervention and examines the
characteristics of participants associated with completion of intervention activities. Healthy Directions-Health Centers was designed to
address social contextual factors relevant to cancer prevention interventions for working class, multi-ethnic populations.
Methods. Ten community health centers were paired and randomly assigned to intervention or control. Patients who resided in low
income, multi-ethnic neighborhoods were approached for participation. This study targeted fruit and vegetable consumption, red meat
consumption, multi-vitamin intake, and physical activity. The intervention components consisted of: (1) a brief study endorsement from a
clinician; (2) an in-person counseling session with a health advisor; (3) four follow-up telephone counseling sessions; and (4) multiple
distributions of tailored materials.
Results. Among the 1,088 intervention group participants, 978 participants (90%) completed at least five out of six intervention activities.
Participants who missed clinical appointments were less likely to complete all components of the intervention. Participant characteristics that
predicted receipt of clinician endorsement differed from characteristics that predicted completion of health advisor activities. Low
acculturation did not present a barrier to delivery of the intervention once the participant was enrolled.
Conclusions. Collection and reporting on process evaluation results can help explain variations in program implementation.
D 2004 The Institute For Cancer Prevention and Elsevier Inc. All rights reserved.
Keywords: Multiethnic populations; Cancer; Prevention
Introduction Patterns of behavioral risk factors differ by socioeconomic
Over two thirds of cancer deaths could be prevented by
changes in nutrition, physical activity, and other health
behaviors [1,2]. These same behavioral risk factors are
associated with cardiovascular disease, diabetes, and osteo-
porosis [3–7]. Yet, the prevalence of poor diet and inactivity
in the United States is widespread [3]. As a result, national
health agencies have called for population-based approaches
to prevention with emphasis on reducing socioeconomic and
racial/ethnic disparities in health [8–12].
0091-7435/$ - see front matter D 2004 The Institute For Cancer Prevention and
doi:10.1016/j.ypmed.2003.12.025
* Corresponding author. Department of Ambulatory Care and Preven-
tion, 133 Brookline Avenue, 6th floor, Harvard Pilgrim Health Care,
Boston, MA 02215. Fax: +1-617-859-8112.
E-mail address: [email protected] (R. Lobb).
position and ethnicity [13–19]. Both risk factor prevalence
and cancer morbidity and mortality are higher among low-
income populations, and among some racial and ethnic
minority groups [8–11]. A nationally representative study
of adults found that lower levels of income are significantly
associated with higher prevalence of unhealthy dietary
behaviors and inactivity [14]. During 1990–1998, trends in
death rates from lung/bronchus, colon/rectum, prostate, and
female breast cancer-related deaths generally declined but the
rates remained high and increased in certain instances for
high-risk and underserved populations [11,20]. Health
behaviors do not appear in isolation, but reflect the complex
dynamic between an individual’s characteristics and societal
forces. The context in which behavior occurs includes mul-
Elsevier Inc. All rights reserved.

R. Lobb et al. / Preventive Medicine 38 (2004) 766–776 767
tiple levels of influence including individual factors (e.g.,
material circumstances, psychosocial factors), interpersonal
factors, (e.g., social ties, roles/responsibilities, social norms),
organizational factors (e.g., work organization, access to
healthcare), and neighborhood/community factors (e.g., safe-
ty, access to grocery stores) [21]. Addressing contextual
factors that influence behavior may make interventions more
meaningful to at-risk populations, thereby enhancing the
effectiveness of interventions aimed at reducing social
inequalities in risk behaviors [14,22–35].
The health care system plays an important role in preven-
tion because patients often consider clinicians to be credible
sources for health information [36–39]. In addition, brief
clinician endorsement partnered with counseling from allied
health professionals can be both efficacious and cost-effec-
tive [40–48]. Community health centers that serve diverse
populations can provide access to those who have the highest
prevalence of preventable cancer-risk factors [1–3,49,50].
In this paper, we describe the implementation of the
Healthy Directions-Health Centers (HC) intervention that
occurred June 2000 through February 2002 and examine the
characteristics of intervention participants associated with
completion of intervention activities. Healthy Directions-
HC is part of the Harvard Cancer Prevention Program
Project, the theme of which is to create cancer prevention
interventions that are effective with working class, multi-
ethnic populations. The Healthy Directions-HC intervention
is designed to take into account elements of social context
that are critical components of an ecological approach to
health behavior change [27,35]. A full description of the
baseline characteristics of the intervention and control
participants is provided by Emmons et al. [22].
Methods
Study design
Healthy Directions-HC was a randomized controlled trial
in which the health center was the unit of randomization and
intervention. We paired 10 health centers based on mem-
bership size, and within each pair, randomly assigned one
site to the intervention condition.
Setting
This study was conducted in collaboration with Harvard
Vanguard Medical Associates, a multi-specialty group prac-
tice composed of 14 health centers serving over 270,000
patients.
Internal Medicine departments at 10 health centers were
invited to participate in this study and all agreed to partic-
ipate. Clinician participation was high across the health
centers, averaging 83%, (range 50–100%); totaling 97
physicians, nurse practitioners, and physician assistants
(intervention n = 49; usual care n = 48). Physicians
represented the majority of participating clinicians, averag-
ing 71% (range 33–86%) across health centers. Each
internal medicine department received a financial incentive
(intervention $2,500; usual care $1,000) for participation.
Sample
Potential study participants were 18–75 years of age, had
a scheduled appointment with an enrolled clinician, and
were identified through Harvard Vanguard’s automated
central appointment system. We used geocoding to identify
patients who lived in neighborhoods that were predominate-
ly working class, impoverished, or with low levels of
education [51–54]. At the time of enrollment, we excluded
patients who did not speak English or Spanish as a primary
language, currently had cancer, were employed by one of
the participating health centers, or were participating in a
companion study focused on work sites [55]. Participants
received a 45-min telephone card for completing the base-
line survey. Details of the recruitment process and response
rates are provided elsewhere [22].
Intervention components
The Healthy Directions-HC study recommendations for
cancer prevention were: (1) eat z5 servings of fruits and
vegetables a day; (2) eat <3 servings of red meat a week; (3)
take a multi-vitamin daily; and (4) get at least 2.5 h of
moderate physical activity per week. The intervention was
delivered over 5 months and consisted of: (1) a brief in-
person clinician endorsement of the study recommendations;
(2) an initial in-person counseling session (ICS) with a health
advisor; (3) four follow-up telephone counseling sessions
with a health advisor; and (4) multiple tailored materials. The
health advisor-counseling sessions and materials were pro-
vided to participants either in Spanish or English.
Clinician endorsement
Research staff trained physicians, nurse practitioners,
and physician’s assistants to deliver the endorsement at a
1-h group orientation delivered at each of the intervention
health centers 2 weeks before the start of the study. The
goal of the orientation was to review the scientific evidence
that supports the relationship between the study outcomes
and cancer prevention, discuss the clinician endorsement
protocol, and identify factors that would assure clinicians’
comfort with following the protocol. All participating clini-
cians received the orientation. Two of the 49 clinicians who
participated in the intervention delivery could not attend the
group orientation but did receive 15-min individual orienta-
tions with the project director.
The clinician endorsement, which occurred at a routine
care visit scheduled by the participant, consisted of the
clinician giving the participant a form called ‘Prescription
for Cancer Prevention’ (see Fig. 1) and making a supportive
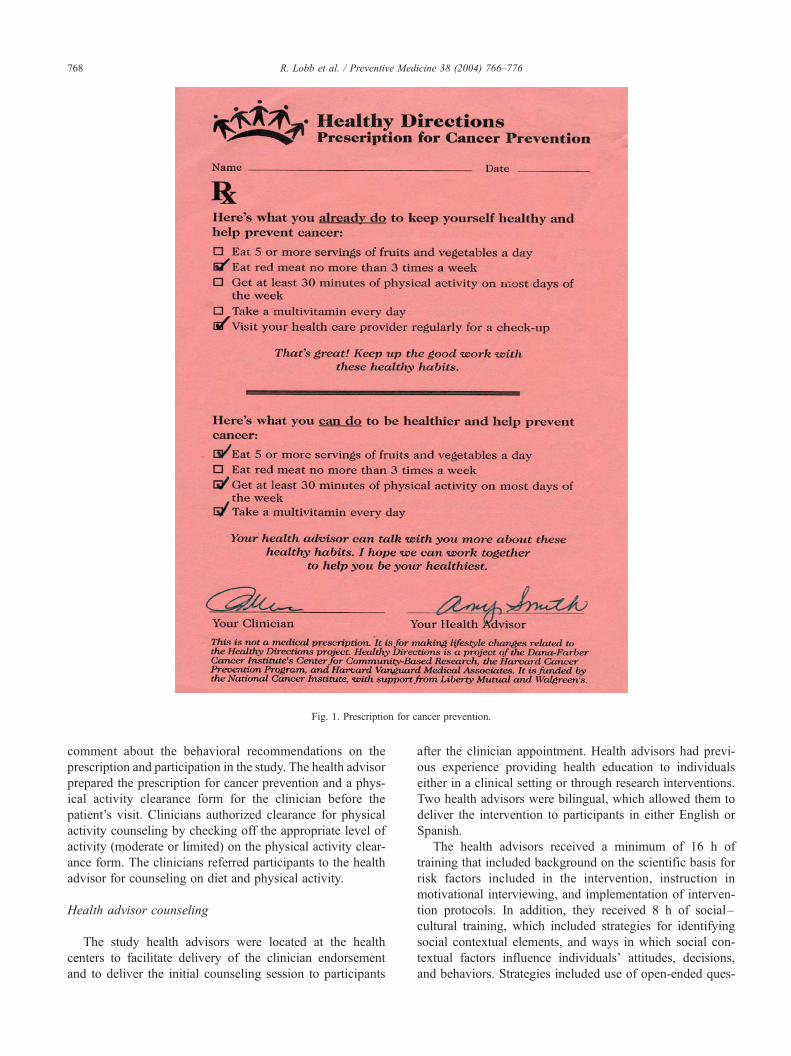
Fig. 1. Prescription for cancer prevention.
R. Lobb et al. / Preventive Medicine 38 (2004) 766–776768
comment about the behavioral recommendations on the
prescription and participation in the study. The health advisor
prepared the prescription for cancer prevention and a phys-
ical activity clearance form for the clinician before the
patient’s visit. Clinicians authorized clearance for physical
activity counseling by checking off the appropriate level of
activity (moderate or limited) on the physical activity clear-
ance form. The clinicians referred participants to the health
advisor for counseling on diet and physical activity.
Health advisor counseling
The study health advisors were located at the health
centers to facilitate delivery of the clinician endorsement
and to deliver the initial counseling session to participants
after the clinician appointment. Health advisors had previ-
ous experience providing health education to individuals
either in a clinical setting or through research interventions.
Two health advisors were bilingual, which allowed them to
deliver the intervention to participants in either English or
Spanish.
The health advisors received a minimum of 16 h of
training that included background on the scientific basis for
risk factors included in the intervention, instruction in
motivational interviewing, and implementation of interven-
tion protocols. In addition, they received 8 h of social–
cultural training, which included strategies for identifying
social contextual elements, and ways in which social con-
textual factors influence individuals’ attitudes, decisions,
and behaviors. Strategies included use of open-ended ques-

R. Lobb et al. / Preventive Med
tions, self-assessments with feedback, and asking partici-
pants to reflect on what a typical day was like for them.
The project director provided on-going training, supervi-
sion, and quality assurance for the health advisor activities
through weekly staff meetings and review of monitoring
reports from the computerized process tracking system. In
addition, health advisors tape-recorded 10% of the coun-
seling sessions and completed a self-assessment of key
components of the patient/health advisor interactions. The
self-assessment had a 5-point scale ranging from ‘‘needs
improvement’’ to ‘‘completely achieved’’ to rate the health
advisor’s performance with: building rapport; identifying
participant’s living arrangement/context; assessing partici-
pant’s view of health; defining potential barriers, facilitators,
and supports to assist with health behavior change; assessing
readiness to change; discussing health habits; praising
accomplishments; reviewing materials; encouraging use of
materials; summarizing session; closing call; asking open
ended questions; and, use of reflective listening. A certified
motivational counseling trainer reviewed the tape-recorded
sessions and self-assessments with the health advisors to
assure compliance with motivational interviewing style and
adherence to the counseling protocols. Self-assessment forms
are available from the corresponding author on request.
Health advisors used motivational interviewing to elicit
motivation to change and to enhance understanding of the
factors that influence a patient’s ability to change. The
motivational interviewing techniques are well suited to
explore social context of participants’ lives because the
non-confrontational and supportive dialogue can facilitate
an open discussion of the participant’s views of health,
needs, experiences, barriers, supports, and readiness to
change. Motivational interviewing techniques include the
use of reflective listening, rolling with resistance, agenda
setting, eliciting self-motivational statements, and change
talk [56–58].
Tailored materials
The Healthy Directions-HC materials were tailored to the
participant’s risk factor-related behavioral status, gender, and
self-efficacy, as well as social contextual factors such as
social supports, barriers to change, family constellation,
health center, and clinician affiliation. Participants received
tailored materials in either English or Spanish. Each partic-
ipant received one baseline tailored feedback report at the
ICS and five mailed tailored ‘‘Step-by-Step’’ guides, a guide
was mailed after each contact with the participant. Each
tailored report addressed multiple levels of influence based
on the social ecological model. For example, we addressed
intrapersonal influences through providing feedback on
participants’ personal risk factor profiles, interpersonal influ-
ences by incorporating information on social supports such
as ways to involve family and friends, and we addressed
environmental influences through promotion of community
resources related to nutrition and physical activity.
Process tracking
We captured data on dose of the intervention delivered by
the study team, as well as dose received by the participants.
For dose of the intervention delivered, the health advisor
recorded the length and completion of the intervention
activity in a portable laptop computer at the conclusion of
each activity. Health advisors followed protocols to deter-
mine when an intervention activity was completed. The
clinician endorsement was complete when a participant
displayed the Prescription for Cancer Prevention to the health
advisor after the clinician appointment. Physical activity
clearance was complete when the health advisor received
the physical activity clearance form from the clinician, either
via the patient during the ICS or via the clinician. The ICS
was complete if the health advisor: (1) established rapport by
exploring the participant’s living arrangements (e.g., family
constellation, sources of support, social norms) and view of
health (attitudes and cultural and religious health beliefs); (2)
reviewed the tailored feedback report recommendations for
cancer prevention (i.e., multivitamin use, physical activity,
and diet) in relation to the participant’s health behaviors; and
(3) asked the participant to comment on the discrepancies
between personal health behaviors and the study recommen-
dations. Calls 1–4 were complete if the health advisor: (1)
assessed the participant’s readiness to change; (2) discussed
goal setting; (3) explored existing social supports; and (4)
reviewed barriers and facilitators to change. In Call 4, the
health advisor also needed to discuss ways to draw on
existing social supports and community resources beyond
the end of the intervention. The baseline-tailored feedback
report was documented as complete if the participant re-
ceived the report by the time of the ICS. Mailed Step-by-Step
guides were considered delivered if the guides were prepared
and sent to the mailroom by a study research assistant.
For data on dose received by participants, we used the 8-
month follow-up survey to measure patients’ receipt of
tailored materials. We asked participants, ‘Did you receive
any materials from Healthy Directions, such as the personal
health profile and step by Step-by-Step guides?’. Response
options were No, Yes, or Don’t Recall. Participants who
responded ‘‘no’’ to this question were instructed to ‘Skip to
question 2 on the next page’. Those who responded ‘‘yes’’
were asked to respond to two additional questions, ‘How
much of these materials would you say that you read?’
(Most or all, A little or some, None) and ‘How helpful were
the materials in helping you to set personal goals for
changing your health habits?’ (Very helpful, Neither helpful
nor unhelpful, Very unhelpful).
Measures of baseline characteristics
This paper describes the baseline health behaviors and a
subset of sociodemographic characteristics for participants
in the intervention group. A full description of the study and
baseline survey including social contextual variables is
icine 38 (2004) 766–776 769

R. Lobb et al. / Preventive Medicine 38 (2004) 766–776770
found elsewhere [22]. The survey instrument is available
from the corresponding author on request.
Sociodemographic characteristics
We asked respondents to report their date of birth,
gender, racial and ethnic groups, first or native language,
level of education completed, immigration status, proportion
of life lived in the US, and household income. We calculated
income relative to the federal poverty guidelines [59] (below
the poverty guideline, between the poverty guideline and
185% of the guideline, or above 185% poverty guideline).
As an additional measure of financial status, we asked
participants to indicate whether they had run out of money
to buy food at any time in the last 12 months [60].
Health behaviors
We assessed servings of fruit and vegetables consumed
per day using a screener developed for the National Cancer
Institute’s 5-a Day for Better Health research projects [61].
We computed a dichotomous measure: five or more servings
per day; or less than five servings per day.
We assessed servings of red meat using an abbreviated
form of the semi-quantitative food frequency questionnaire
[61]. We coded responses to equivalent servings per week
and summed, excluding poultry and fish, to obtain the total
servings of red meat per week. We dichotomized the totals
to three or fewer servings; or more than three servings per
week.
We based our physical activity assessment on the ques-
tionnaire used in the Nurses Health Study [62] by adapting
the items to include specific activities that are more common
in our target population. For physical activity, we asked how
often in the last 4 weeks respondents engaged in each of
eight moderate or vigorous activities, on average (e.g.,
walking for exercise jogging; running; bicycling; aerobics
or aerobic dancing; playing soccer, rugby, basketball, or
lacrosse; playing baseball, football, or lifting weights). We
coded responses to equivalent minutes per week and
summed for total minutes of physical activity per week.
We dichotomized the totals 150 min (2.5 h) or greater per
week; or fewer than 150 min per week.
We asked respondents on average how many days per
week they took a multi-vitamin. Responses were coded as
daily if participants reported taking one multi-vitamin at least
6 days per week. We asked respondents whether they had
ever smoked at least 100 cigarettes and whether they had
smoked even a puff in the last 7 days. Based on responses,
participants were categorized as not current smokers or
current smokers (smoked a puff in the last 7 days).
Measures of implementation
We assessed three measures of implementation: (1)
reach; (2) extent of implementation; and (3) fidelity to
intervention protocol. To determine the reach of interven-
tion, we computed the number of participants who received
the clinician endorsement, completed the initial counseling
session (ICS), completed counseling calls, were mailed
tailored materials, and received tailored materials. We mea-
sured extent of implementation by calculating the average
number of intervention activities per participant, average
number of telephone calls completed, and average number
of tailored materials mailed. Fidelity to intervention protocol
was measured by the proportion of participants who re-
ceived key intervention components as planned, the ICS on
the same day as the clinician visit, physical activity clear-
ance on the same day as the ICS, and ICS at the health
center. We also examined the mean length of the initial
counseling session, telephone sessions, and the proportion
of call attempts that resulted in completed calls.
In addition, we created a multi-item index of protocol
completion to summarize the overall reach of intervention.
For each person-to-person intervention activity, we scored a
‘1’ if completed or a ‘0’ if not completed. The scores for
each participant were added to determine the index of
protocol completion for person-to-person activities. An
index of six indicates that all person-to-person intervention
activities (one clinician endorsement, one ICS, and four
follow-up telephone calls) were completed by the partici-
pant; an index of five indicates that one activity was missed.
Data analyses
Using SAS (SAS Institute, Cary, NC, v.8), we exam-
ined the distribution of participants according to measures
of sociodemographic characteristics, social context, and
levels of target health behaviors. We then examined the
measures of intervention activity and the bivariate associ-
ations between baseline participant characteristics and
intervention activities. To control for the clustering of
participants within health centers, we calculated a chi-
square statistic for each bivariate association using the
SAS GLIMMIX macro with health center as a random
effect. Because having the ICS and clinician visit on the
same day strongly predicted a successful outcome on all
three measures, the bivariate analyses were repeated after
exclusion of participants who did not see the clinician on the
same day as the health advisor. All reported P values were
two-tailed and P values of 0.05 or less were considered
statistically significant.
We performed multivariate analysis for the index of
protocol completion, receipt of clinician endorsement, and
completion of health advisor calls using linear logistic
regression controlling for health center as a random effect.
Predictor variables that were significantly associated (P V0.05) with the outcomes in bivariate analysis or sub-group
analysis were included in the logistic regression multivariate
model. Variables related to the outcome, but presented in the
bivariate analyses, were excluded (clinician same day visit
as ICS and clinician endorsement).
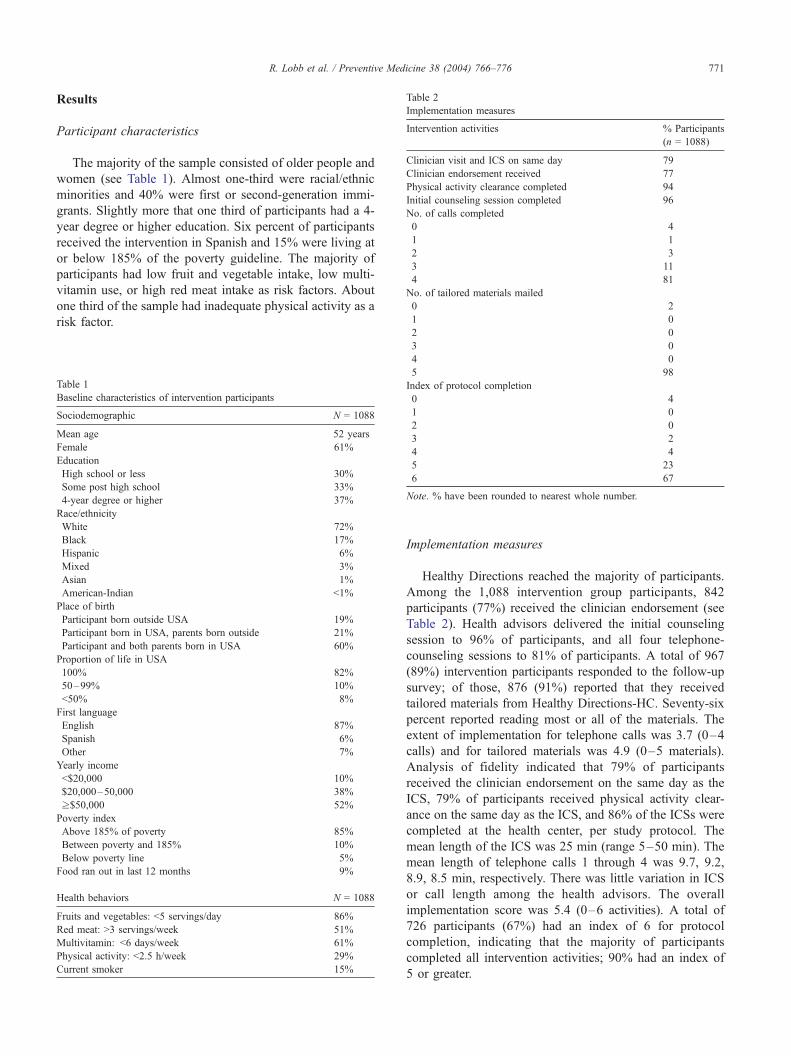
Table 2
Implementation measures
Intervention activities % Participants
(n = 1088)
Clinician visit and ICS on same day 79
Clinician endorsement received 77
Physical activity clearance completed 94
Initial counseling session completed 96
No. of calls completed
0 4
1 1
2 3
3 11
4 81
No. of tailored materials mailed
0 2
1 0
R. Lobb et al. / Preventive Medicine 38 (2004) 766–776 771
Results
Participant characteristics
The majority of the sample consisted of older people and
women (see Table 1). Almost one-third were racial/ethnic
minorities and 40% were first or second-generation immi-
grants. Slightly more that one third of participants had a 4-
year degree or higher education. Six percent of participants
received the intervention in Spanish and 15% were living at
or below 185% of the poverty guideline. The majority of
participants had low fruit and vegetable intake, low multi-
vitamin use, or high red meat intake as risk factors. About
one third of the sample had inadequate physical activity as a
risk factor.
Table 1
Baseline characteristics of intervention participants
Sociodemographic N = 1088
Mean age 52 years
Female 61%
Education
High school or less 30%
Some post high school 33%
4-year degree or higher 37%
Race/ethnicity
White 72%
Black 17%
Hispanic 6%
Mixed 3%
Asian 1%
American-Indian <1%
Place of birth
Participant born outside USA 19%
Participant born in USA, parents born outside 21%
Participant and both parents born in USA 60%
Proportion of life in USA
100% 82%
50–99% 10%
<50% 8%
First language
English 87%
Spanish 6%
Other 7%
Yearly income
<$20,000 10%
$20,000–50,000 38%
z$50,000 52%
Poverty index
Above 185% of poverty 85%
Between poverty and 185% 10%
Below poverty line 5%
Food ran out in last 12 months 9%
Health behaviors N = 1088
Fruits and vegetables: <5 servings/day 86%
Red meat: >3 servings/week 51%
Multivitamin: <6 days/week 61%
Physical activity: <2.5 h/week 29%
Current smoker 15%
2 0
3 0
4 0
5 98
Index of protocol completion
0 4
1 0
2 0
3 2
4 4
5 23
6 67
Note. % have been rounded to nearest whole number.
Implementation measures
Healthy Directions reached the majority of participants.
Among the 1,088 intervention group participants, 842
participants (77%) received the clinician endorsement (see
Table 2). Health advisors delivered the initial counseling
session to 96% of participants, and all four telephone-
counseling sessions to 81% of participants. A total of 967
(89%) intervention participants responded to the follow-up
survey; of those, 876 (91%) reported that they received
tailored materials from Healthy Directions-HC. Seventy-six
percent reported reading most or all of the materials. The
extent of implementation for telephone calls was 3.7 (0–4
calls) and for tailored materials was 4.9 (0–5 materials).
Analysis of fidelity indicated that 79% of participants
received the clinician endorsement on the same day as the
ICS, 79% of participants received physical activity clear-
ance on the same day as the ICS, and 86% of the ICSs were
completed at the health center, per study protocol. The
mean length of the ICS was 25 min (range 5–50 min). The
mean length of telephone calls 1 through 4 was 9.7, 9.2,
8.9, 8.5 min, respectively. There was little variation in ICS
or call length among the health advisors. The overall
implementation score was 5.4 (0–6 activities). A total of
726 participants (67%) had an index of 6 for protocol
completion, indicating that the majority of participants
completed all intervention activities; 90% had an index of
5 or greater.
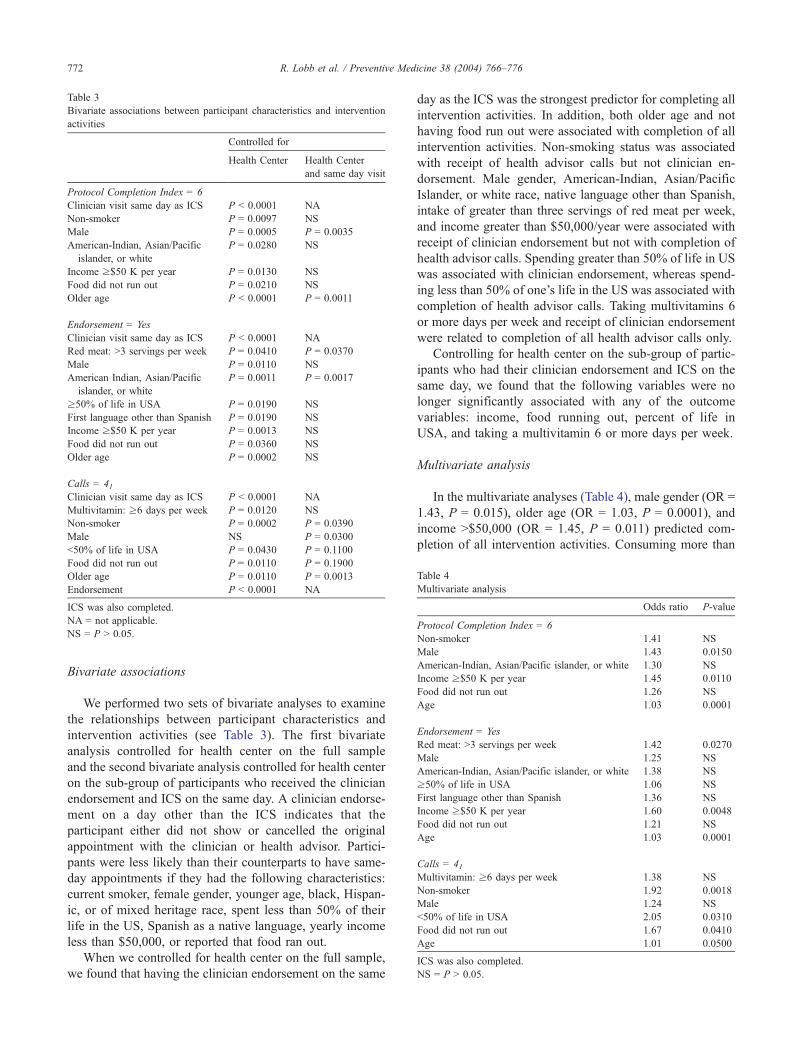
Table 3
Bivariate associations between participant characteristics and intervention
activities
Controlled for
Health Center Health Center
and same day visit
Protocol Completion Index = 6
Clinician visit same day as ICS P < 0.0001 NA
Non-smoker P = 0.0097 NS
Male P = 0.0005 P = 0.0035
American-Indian, Asian/Pacific
islander, or white
P = 0.0280 NS
Income z$50 K per year P = 0.0130 NS
Food did not run out P = 0.0210 NS
Older age P < 0.0001 P = 0.0011
Endorsement = Yes
Clinician visit same day as ICS P < 0.0001 NA
Red meat: >3 servings per week P = 0.0410 P = 0.0370
Male P = 0.0110 NS
American Indian, Asian/Pacific
islander, or white
P = 0.0011 P = 0.0017
z50% of life in USA P = 0.0190 NS
First language other than Spanish P = 0.0190 NS
Income z$50 K per year P = 0.0013 NS
Food did not run out P = 0.0360 NS
Older age P = 0.0002 NS
Calls = 41Clinician visit same day as ICS P < 0.0001 NA
Multivitamin: z6 days per week P = 0.0120 NS
Non-smoker P = 0.0002 P = 0.0390
Male NS P = 0.0300
<50% of life in USA P = 0.0430 P = 0.1100
Food did not run out P = 0.0110 P = 0.1900
Older age P = 0.0110 P = 0.0013
Endorsement P < 0.0001 NA
ICS was also completed.
NA = not applicable.
NS = P > 0.05.
Table 4
Multivariate analysis
Odds ratio P-value
Protocol Completion Index = 6
Non-smoker 1.41 NS
Male 1.43 0.0150
American-Indian, Asian/Pacific islander, or white 1.30 NS
Income z$50 K per year 1.45 0.0110
Food did not run out 1.26 NS
Age 1.03 0.0001
Endorsement = Yes
Red meat: >3 servings per week 1.42 0.0270
Male 1.25 NS
American-Indian, Asian/Pacific islander, or white 1.38 NS
z50% of life in USA 1.06 NS
First language other than Spanish 1.36 NS
Income z$50 K per year 1.60 0.0048
Food did not run out 1.21 NS
Age 1.03 0.0001
Calls = 41Multivitamin: z6 days per week 1.38 NS
Non-smoker 1.92 0.0018
Male 1.24 NS
<50% of life in USA 2.05 0.0310
Food did not run out 1.67 0.0410
Age 1.01 0.0500
ICS was also completed.
NS = P > 0.05.
R. Lobb et al. / Preventive Medicine 38 (2004) 766–776772
Bivariate associations
We performed two sets of bivariate analyses to examine
the relationships between participant characteristics and
intervention activities (see Table 3). The first bivariate
analysis controlled for health center on the full sample
and the second bivariate analysis controlled for health center
on the sub-group of participants who received the clinician
endorsement and ICS on the same day. A clinician endorse-
ment on a day other than the ICS indicates that the
participant either did not show or cancelled the original
appointment with the clinician or health advisor. Partici-
pants were less likely than their counterparts to have same-
day appointments if they had the following characteristics:
current smoker, female gender, younger age, black, Hispan-
ic, or of mixed heritage race, spent less than 50% of their
life in the US, Spanish as a native language, yearly income
less than $50,000, or reported that food ran out.
When we controlled for health center on the full sample,
we found that having the clinician endorsement on the same
day as the ICS was the strongest predictor for completing all
intervention activities. In addition, both older age and not
having food run out were associated with completion of all
intervention activities. Non-smoking status was associated
with receipt of health advisor calls but not clinician en-
dorsement. Male gender, American-Indian, Asian/Pacific
Islander, or white race, native language other than Spanish,
intake of greater than three servings of red meat per week,
and income greater than $50,000/year were associated with
receipt of clinician endorsement but not with completion of
health advisor calls. Spending greater than 50% of life in US
was associated with clinician endorsement, whereas spend-
ing less than 50% of one’s life in the US was associated with
completion of health advisor calls. Taking multivitamins 6
or more days per week and receipt of clinician endorsement
were related to completion of all health advisor calls only.
Controlling for health center on the sub-group of partic-
ipants who had their clinician endorsement and ICS on the
same day, we found that the following variables were no
longer significantly associated with any of the outcome
variables: income, food running out, percent of life in
USA, and taking a multivitamin 6 or more days per week.
Multivariate analysis
In the multivariate analyses (Table 4), male gender (OR =
1.43, P = 0.015), older age (OR = 1.03, P = 0.0001), and
income >$50,000 (OR = 1.45, P = 0.011) predicted com-
pletion of all intervention activities. Consuming more than

R. Lobb et al. / Preventive Medicine 38 (2004) 766–776 773
three servings of red meat per week (OR = 1.42, P = 0.027),
and income >$50,000 (OR = 1.60, P = 0.0048) were
significantly associated with receipt of endorsement. The
characteristics that predicted completion of all health advi-
sor calls were non-smoker (OR = 1.92, P = 0.0018), food
not running out (OR = 1.67, P = 0.041), and percent of life
in USA less than 50% (OR = 2.05, P = 0.031).
Discussion
We examined the implementation of the overall inter-
vention and identified associations between participant
characteristics and individual components of the interven-
tion. Implementation measures of reach, extent of imple-
mentation, and fidelity to protocol indicated high levels of
participation in Healthy Directions-HC compared to similar
studies [42,46,56,63–66]. The combination of clinician
endorsement, use of motivational interviewing techniques,
and strategies to incorporate social context in the interven-
tion through counseling and tailored materials may account
for the higher rates of completed counseling calls in the
Healthy Directions-HC study. Several studies have evaluat-
ed the effect of these individual techniques or combinations
of these techniques with success but we are not aware of any
studies that have used all of these techniques simultaneously
in an intervention. Reasons why participants did not com-
plete all study activities included missed appointments with
the clinician, missed appointments with the health advisor,
and lack of time to complete the activity during an interac-
tion with the participant.
Three findings from our analyses are especially relevant
to cancer prevention programs delivered in health centers.
First, patient characteristics associated with a missed ap-
pointment, either with the clinician or health advisor for the
ICS, were consistently associated with low levels of inter-
vention completion. Missed appointment rates in general
medical settings range from 5% to 30%, so it is not surprising
that our implementation was affected by ‘no-shows’ [67].
However, relatively little consideration has been given to the
impact of missed appointments within health-care-based
prevention research. Characteristics of participants who
missed appointments in our study are consistent with previ-
ous reports or positive correlations between missed appoint-
ments and characteristics of younger age, non-white race,
current smoker, lower income status, and lower acculturation
[67–69]. Missed appointments within these groups may be
due to fewer resources or more complex lives. Researchers
who design interventions for health care settings should
anticipate this barrier to intervention delivery and partner
with the health care system to provide facilitators to encour-
age patients with these characteristics to keep appointments.
Reminder phone calls, flexible scheduling, assistance with
transportation, or incentives for keeping an appointment may
serve as a means for assuring higher show rates in groups
that have difficulty keeping appointments.
Second, participants who spent less than 50% of their life
in the US were more than twice as likely to receive all four
calls from health advisors compared to those who spent 50%
or more of their life in the US. This finding indicates that
although participants with lower acculturation may be asso-
ciated with high rates of missed appointments, they can also
be highly compliant with intervention protocols. Our inter-
vention materials and health advisor counseling addressed
social contextual factors that may have made our interven-
tion more salient to participants with lower acculturation
than traditional interventions based solely on health behav-
iors [23,36,70,71]. In particular, the emphasis placed on the
individual’s view of health and social supports during the
health advisor counseling sessions may have helped partic-
ipants with lower acculturation overcome barriers to com-
pleting intervention activities [34,72–75]. It is noteworthy
that we found higher levels of intervention participation
among more recent immigrants, as utilization of preventive
services are generally lower for minority patients.
Third, participant characteristics associated with receipt
of the clinician endorsement differed from characteristics
that predicted completion of the health advisor activities.
Previous studies on utilization of health care services indi-
cate that clinicians sometimes differentially manage patients
based on gender, race, acculturation, or socioeconomic
position [48,68,76–80]. In addition, there is evidence that
rates of clinician advice delivered during usual care to reduce
chronic disease-risk factors is low; 20–57% for dietary
advice, 15–69% for physical activity [50,81]. When clini-
cians do provide advice it tends to be directive and less open
to the patient’s agenda due to time constraints and counseling
style [80]. In our pairing of the clinician and health advisor to
deliver the Healthy Directions-HC activities, we may have
created a safety net for those patients who would have
received lower doses of the intervention had only the
clinician or the health advisor been used in the study. The
patient-centered, contextually based counseling used by the
health advisors in our study contrasts with the behavior-
based recommendations provided by clinicians, yet may
create a synergy that appeals to a broader audience of
patients. Interventions delivered in health centers that rely
on clinician as well as auxiliary supports should examine the
relationships between the care provider’s characteristics and
participant’s characteristics so we may gain further insight
into the dynamics of patient and provider interactions.
Our analysis of predictors of intervention activities was
limited to participant characteristics reported on the baseline
survey and the data collected in the automated process
tracking system. It is possible that other factors, such as
clinician characteristics or co-morbid conditions may have
influenced the implementation of the Healthy Directions-
HC intervention. In addition, we did not control for health
advisor in our analysis because the health advisors rarely
worked with participants outside of their primary health
center. It could be that the data are confounded by a health
advisor effect independent of the health center effect, but

R. Lobb et al. / Preventive Medicine 38 (2004) 766–776774
our small numbers of health advisors and health centers
prevent us from analyzing this possibility. Finally, sub-
analysis like the type we describe can be difficult to interpret
when nearly all participants complete most of the desired
number of intervention activities. There may be some
associations between participant characteristics and inter-
vention activities where the strength of clinical significance
is not supported by statistical significance or statistical
significance is achieved but clinical significance is not
relevant. This manuscript reports baseline data and explores
predictors of participation. In a future paper, we will explore
possible relationships between process data and outcomes.
The data reported here provide health care professionals
and researchers with a description of the implementation of
a cancer prevention intervention for working class, multi-
ethnic populations. Participation in Healthy Directions-HC
was highly successful, particularly with participants of
lower acculturation, a group that has traditionally been
difficult to reach because of missed appointments or low
compliance with treatment regimens. Consideration of so-
cial contextual factors in addition to health behaviors in the
counseling and tailored materials may have resulted in our
success with reaching our target population. This paper
demonstrates the contributions that process evaluation can
make to understanding the implementation of intervention
studies.
Acknowledgments
This research was supported by grant # 5 PO1 CA 75308
from the National Institutes of Health and support to Dana-
Farber Cancer Institute by Liberty Mutual and National Grid.
The authors would like to thank the numerous staff
members contributing to this study, including Elizabeth
Alvarez, Jamie Baron, Simone Pinheiro, Kathleen Scafidi,
Tracy Liwen, and Tatyana Pinchuk. In addition, this work
could not have been done without the participation of the
internal medicine departments of Harvard Vanguard Medical
Associates.
References
[1] Harvard report on cancer prevention: causes of human cancer. Cancer
Causes Control 1996;1(7 Suppl.):S3–58.
[2] American Cancer Society. Cancer Facts and Figures, 2002. Atlanta,
GA: American Cancer Society; 2002.
[3] Dubbert PM, Carithers T, Sumner AE, et al. Obesity, physical inac-
tivity, and risk for cardiovascular disease. Am J Med Sci 2002;
324(3):116–26.
[4] Centers for Disease Control and Prevention. Coronary heart disease
attributable to sedentary lifestyle-selected states, 1988. JAMA 1990;
264:1390–2.
[5] Powell KE, Thompson PD, Caspersen CJ, Kendrick JS. Physical
activity and the incidence of coronary heart disease. Annu Rev Public
Health 1987;8:253–87.
[6] Willett WC, Stampfer MJ, Colditz GA, Rosner BA, Speizer FE. Rela-
tion of meat, fat, and fiber intake to the risk of colon cancer in a
prospective study among women. N Engl J Med 1990;323(24):
1664–72.
[7] McTiernan A, Ulrich C, Slate S, Potter J. Physical activity and cancer
etiology: associations and mechanisms. Cancer Causes Control
1998;9:487–509.
[8] U.S. Department of Agriculture, U.S. Department of Health and
Human Services. Nutrition and your Health: Dietary Guidelines
for Americans. Fifth ed. Washington, DC: US Government Printing
Office; 2000.
[9] USDHHS. Healthy People 2010: Understanding and Improving
Health and Objectives for Improving Health. Washington, DC: Gov-
ernment Printing Office; 2000.
[10] USDHHS. Physical Activity and Health: A Report of the Surgeon
General. Atlanta, GA: Center for Disease Control and Prevention,
National Center for Chronic Disease Prevention and Health Promo-
tion; 1996.
[11] MMWR. Recent trends in mortality rates for four major cancers, by
sex and race/ethnicity—United States, 1990–1998. Morb Mortal
Wkly Rep 2002;51(3):49–53.
[12] Briss PA, Zaza S, Pappaioanou M, et al. Developing an evidence-
based guide to community preventive services: methods. Am J Prev
Med 2000;18(1 Suppl.):35–43.
[13] World Health Organization. Diet, Nutrition, and Prevention of Chron-
ic Diseases: Report of the Joint WHO/FAO Expert Consultation.
Geneva, Switzerland: World Health Organization; 2002.
[14] Lantz PM, House JS, Lepkowski JM, Williams DR, Mero RP, Chen J.
Socioeconomic factors, health behaviors, and mortality: results from a
nationally representative prospective study of US adults. JAMA
1998;279(21):1703–8.
[15] Institute of Medicine. Unequal Treatment: Confronting Racial and
Ethnic Disparities in Health Care. Washington, DC: National Aca-
demic Press; 2002.
[16] Shea S, Melnik TA, Stein AD, Zansky SM, Maylahn C, Basch CE.
Age, sex, educational attainment, and race/ethnicity in relation to
consumption of specific foods contributing to the atherogenic poten-
tial of diet. Prev Med 1993;22(2):203–18.
[17] MMWR CE. Prevalence of leisure-time and occupational physical
activity among employed adults—United States, 1990. Morb Mortal
Wkly Rep 2000;49(19):420–4.
[18] Sundquist J, Winkleby MA, Pudaric S. Cardiovascular disease risk
factors among older Black, Mexican-American, and White women
and men: an analysis of NHANES III, 1988–1994. J Am Geriatr
Soc 2001;49(2):109–16.
[19] Smit E, Nieto FJ, Crespo CJ, Mitchell P. Estimates of animal and
plant protein intake in US adults: results from the third national health
and nutrition examination survey, 1988–1991. J Am Diet Assoc 1999;
99(7):813–20.
[20] Krieger N. Is breast cancer a disease of affluence, poverty, or both?
The case of African American women. Am J Public Health 2002;
92(4):611–3.
[21] Stokols D. Translating social ecological theory into guidelines for
community health promotion. Am J Health Promot 1996;10(4):
282–98.
[22] Emmons KM, Stoddard AM, Gutheil C, Suarez ER, Lobb R, Fletcher
R. Cancer prevention for working class, multi-ethnic populations
through health centers: the healthy directions study. Cancer Causes
Control 2003;14(8):727–37.
[23] Kidd KE, Altman DG. Adherence in social context. Control Clin
Trials 2000;21(5 Suppl.):184S–7S.
[24] Emmons KM. Health behaviors in a social context. In: Berkman LF,
Kawachi I, editors. Social Epidemiology. Oxford: Oxford Univ. Press;
2000. p. 242–66.
[25] Institute of Medicine. Promoting Health: Intervention Strategies from
Social and Behavioral Research. Washington DC: National Academy
Press; 2000.
[26] Sorensen G, Emmons K, Hunt M, Johnston D. Implications of the
R. Lobb et al. / Preventive Medicine 38 (2004) 766–776 775
results of community intervention trials. Annu Rev Public Health
1998;19:379–416.
[27] Goldman R, Hunt MK, Allen JD, et al. The life history interview
method: applications to intervention development. Health Educ
Behav 2003;30(5):564–81.
[28] Becker MH. Understanding Patient Compliance: The Contribution of
Attitudes and Other Psychosocial Factors. Lexington, MS: Health;
1979.
[29] Slovic P. Perception of risk. Science 1987;236:280–5.
[30] Gore S. Stress-buffering functions of social supports: an appraisal and
clarification of research models. In: Dohrenwend BS, Dohrenwend
BP, editors. Stressful Life Events and Their Context. New York: Neale
Watson Academic Press; 1984. p. 202–22.
[31] Graham H. Poverty and national health strategies. In: Doyal L, editor.
Women and Health Services: An Agenda for Change. Philadelphia:
Open Univ. Press; 1998. p. 22–38.
[32] Kaplan GA. Where do shared pathways lead? Some reflections on a
research agenda. Psychosom Med 1995;57:208–12.
[33] Freudenberg N. Time for a national agenda to improve the health of
urban populations. Am J Public Health 2000;90(6):837–40.
[34] MMWR. Increasing physical activity: a report on recommendations of
the task force on community preventive services. Morb Mortal Wkly
Rep 2001;50(RR18):1–14.
[35] Sorensen G, Emmons KM, Hunt MK, et al. Model for incorporating
the social context in health behavior interventions: applications for
cancer prevention for working-class, multiethnic populations. Prev
Med 2003;37:188–97.
[36] Kreuter MW, Oswald DL, Bull FC, Clark EM. Are tailored health
education materials always more effective than non-tailored materi-
als? Health Educ Res 2000;15(3):305–15.
[37] Harris SS, Caspersen CJ, DeFriese GH, Estes EH. Physical activity
counseling for healthy adults as a primary preventive intervention in
the clinical setting: report for the US Preventive Services Task Force.
JAMA 1989;261(24):3590–8.
[38] Hunt JR, Kristal AR, White E, Lynch JC, Fries E. Physician recom-
mendations for dietary change: their prevalence and impact in a pop-
ulation-based sample. Am J Public Health 1995;85(5):722–6.
[39] Ockene JK, Kristeller J, Goldberg R, et al. Increasing the efficacy of
physician-delivered smoking interventions: a randomized clinical
trial. J Gen Intern Med 1991;6(1):1–8.
[40] Albright CL, Cohen S, Gibbons L, et al. Incorporating physical ac-
tivity advice into primary care physician-delivered advice within the
activity counseling trial. Am J Prev Med 2000;18(3):225–34.
[41] Norris SL, Grothaus LC, Buchner DM, Pratt M. Effectiveness of
physician-based assessment and counseling for exercise in a staff
model HMO. Prev Med 2000;30:513–23.
[42] Marcus BH, Goldstein MG, Jette A, et al. Training physicians to
conduct physical activity counseling. Prev Med 1997;26:382–8.
[43] Baron JA, Gleason R, Crowe B, Mann JI. Preliminary trial of the
effect of general practice based nutritional advice. Br J Gen Pract
1990;40:137–41.
[44] Beresford SAA, Curry SJ, Kristal AR, Lazovich D, Feng Z, Wagner
EH. A dietary intervention in primary care practice: the eating pat-
terns study. Am J Public Health 1997;87(4):610–6.
[45] Delichatsios HK, Hunt MK, Lobb R, Emmons K, Gillman MW.
EatSmart: efficacy of a multifaceted preventive nutrition intervention
in clinical practice. Prev Med 2001;33(2 Pt 1):91–8.
[46] Calfas KJ, Sallis JF, Zabinski MF, et al. Preliminary evaluation of a
multicomponent program for nutrition and physical activity change in
primary care: PACE + for adults. Prev Med 2002;34:153–61.
[47] Dietrich AJ, O’Connor GT, Keller A, Carney PA, Levy D, Whaley
FS. Cancer: improving early detection and prevention. A community
practice randomised trial. Br Med J 1992;304:687–91.
[48] Friedman C, Brownson RC, Peterson DE, Wilkerson JC. Physician
advice to reduce chronic disease risk factors. Am J Prev Med 1994;
10(6):367–71.
[49] Kerr DL, Davis RM. The guide to community preventive services:
managed care/clinical practice commentary. Am J Prev Med 2000;
18(1S):5–6.
[50] Wechsler H, Levine S, Idelson RK, Rohman M, Taylor JO. The
physician’s role in health promotion—A survey of primary care prac-
titioners. N Engl J Med 1983;308(2):97–100.
[51] Krieger N, Williams DR, Moss NE. Measuring social class in US
public health research: concepts, methodologies, and guidelines.
Annu Rev Public Health 1997;18:341–78.
[52] U.S. Bureau of Census. Census Use Study: Health Information Sys-
tem-II. Washington, DC: US Government Printing Office; 1971. Re-
port No.: 12.
[53] Krieger N. Overcoming absence of socioeconomic data in medical
records: validation and application of the census-based methodology.
Am J Public Health 1992;92:703–10.
[54] Krieger N. Women and social class: a methodological study compar-
ing individual, household, and census measures as predictors of black/
white differences in reproductive history. J Epidemiol Community
Health 1991;45:35–42.
[55] Hunt MK, Stoddard AM, Barbeau E, et al. Cancer prevention for
working class, multiethnic populations through small businesses:
the healthy directions study. Cancer Causes Control 2003;14(8):
749–60.
[56] Resnicow KS, Jackson A, Wang T, De AK, McCarty F, Dudley WN.
A motivational interviewing intervention to increase fruit and vege-
table intake through Black churches: results of the eat for life trial.
Am J Public Health 2001;91(10):1686–93.
[57] Resnicow K, DiIorio C, Soet JE, Ernst D, Borrelli B, Hecht J. Mo-
tivational interviewing in health promotion: it sounds like something
is changing. Health Psychol 2002;21(5):444–51.
[58] Emmons KM, Rollnick S. Motivational interviewing in health care
settings: opportunities and limitations. Am J Prev Med 2001;20(1):
68–74.
[59] USDHHS. The 2001 HHS Poverty Guidelines. U.S. Department of
Health and Human Services; 2001. Available at: http://aspe.hhs.gov/
poverty/01poverty.htm.
[60] Blumberg S, Bialostosky K, Hamilton W, Briefel R. The effectiveness
of a short form of the household food security scale. Am J Public
Health 1999;89:1231–4.
[61] Subar AS, Heimdinger J, Krebs-Smith SM, Patterson BH, Kessler R,
Pivonka E. Fruit and vegetable intake in the United States: the base-
line survey of the Five a Day for Better Health Program. Am J Health
Promot 1995;9(5):352–60.
[62] Wolf AM, Hunter DJ, Colditz GA, et al. Reproducibility and validity
of a self-administered physical activity questionnaire. Int Epidemiol
1994;23:991–9.
[63] Stevens VJ, Glasgow RE, Toobert DJ, Karanja N, Smith KS. Ran-
domized trial of a brief dietary intervention to decrease consumption
of fat and increase consumption of fruits and vegetables. Am J Health
Promot 2002;16(3):129–34.
[64] Lazovich D, Curry SJ, Beresford SA, Kristal AR, Wagner EH. Imple-
menting a dietary intervention in primary care practice: a process
evaluation. Am J Health Promot 2000;15(2):118–25.
[65] Hunt MK, Lobb R, Delichatsios HK, Stone C, Emmons KM, Gillman
MW. Process evaluation of a clinical preventive nutrition intervention.
Prev Med 2001;33(2):82–90.
[66] Green BB, McAfee T, Hindmarsh M, Madsen L, Caplow M, Buist D.
Effectiveness of telephone support in increasing physical activity lev-
els in primary care patients. Am J Prev Med 2002;22(3):177–83.
[67] Smith CM, Yawn BP. Factors associated with appointment keeping in
a family practice residency clinic. J Fam Pract 1994;38(1):25–9.
[68] Strzelczyk J, Dignan MB. Disparities in adherence to recommended
follow up on screening mammography: interaction of sociodemo-
graphic factors. Ethn Dis 2002;12:77–86.
[69] Gruzd DC, Shear CL, Rodney MW. Determinants of no-show appoint-
ment behavior: the utility of multivariate analysis. Fam Med 1986;
18(4):217–20.
[70] Campbell M, DeVellis B, Strecher V, Ammerman A, DeVellis RR,

R. Lobb et al. / Preventive Medicine 38 (2004) 766–776776
Osborn EH. Improving dietary behavior: the effectiveness of tailored
messages in primary care settings. Am J Public Health 1994;84:
783–7.
[71] Skinner CS, Campbell MK, Rimer BK, Curry S, Prochaska JO. How
effective is tailored print communication? Ann Behav Med 1999;
21(4):290–8.
[72] Katapodi MC, Facione NC, Miaskowski C, Dodd MJ, Waters C. The
influence of social support on breast cancer screening in a multicul-
tural community sample. Oncol Nurs Forum 2002;29(5):845–52.
[73] Pasick RJ, Stewart SL, Bird JA, D’Onofrio CN. Quality of data in
multiethnic health surveys. Public Health Rep 2001;116(1 Suppl.):
223–43.
[74] Ma G, Fleisher L. Awareness of cancer information among Asian
Americans. J Community Health 2003;28(2):115–30.
[75] McGarvey EL, Clavet GJ, Johnson II JB, Butler A, Cook KO, Pen-
nino B. Cancer screening practices and attitudes: comparison of low-
income women in three ethnic groups. Ethn Health 2003;8(1):
71–82.
[76] Sheifer SE, Escarce JJ, Schulman KA. Race and sex differences in the
management of coronary artery disease. Am Heart J 2000;139(5):
848–57.
[77] Schulman KA, Berlin JA, Harless W, et al. The effect of race and sex
on physicians’ recommendations for cardiac catheterization. N Engl J
Med 1999;340(8):618–26.
[78] Solberg LI, Brekke ML, Kottke TE. Are physicians less likely to
recommend preventive services to low-SES patients? Prev Med
1997;26:350–7.
[79] Franks P, Clancy CM. Physician gender bias in clinical decision-
making: screening for cancer in primary care. Med Care 1993;31(3):
213–8.
[80] Fiscella K, Goodwin MA, Stange KC. Does patient educational level
affect office visits to family physicians? J Natl Med Assoc 2002;
94(3):157–65.
[81] McPhee SJ, Bird JA, Fordham D, Rodnick JE, Osborn EH. Promoting
cancer prevention activities by primary care physicians. Results of a
randomized, controlled trial. JAMA 1991;266(4):538–44.