implant prototypes and_designs
TRANSCRIPT

IMPLANT PROTOTYPES DESIGNS AND SYSTEMS
(How to select an implant system)
� Objectives
� Participants will understand the rationale behind the design of the root form implant. They will be given an over view of the other types of Implant systems. Nobel Replace® and Nobel Active ® designs will be discussed in some detail. At the end of the course they will be in a position to select an implant and a system on a scientific basis.
� DEFINITION :
� A Dental Implant is defined as “ A substance that is placed into the jaw to support a crown or fixed or removable denture.”
� History
� ANCIENT IMPLANTS :-
� Ú 16 th Dark stone
� ( Egyptian-South American)
� Ú 17 th Carved ivory teeth
� EARLY IMPLANTS :-
� Ú 1809 Gold implant
� Ú e.20th Lead, iridium, tantalum,
� stainless steel, & cobalt alloy
� Ú 1913 hollow basket, iridium + gold wires
� EARLY IMPLANTS
� Ú 1937 Adams’s submergible threaded
� cylindrical implant with round bottom
� Ú 1938 Strock’s (long term) threaded vitallium
� implant (cobalt+chrome+molybdenum)
� Ú The modern implants appear to be variants or composites of some of the designs of early implants

DENTAL IMPLANT DESIGNS
� Endosteal Implants Root/Blade
� Subperiosteal Implants
� Transosteal Implants
� Intramucosal implants
� Dental Implant Designs
� Endosteal Implants Root /Blade
� Subperiosteal Implants
� Transosteal Implants
� Intramucosal implants
AN ENDOSTEAL IMPLANT
IS PLACED DIRECTLY INTO THE BONE, LIKE NATURAL TOOTH ROOTS AND CAN BE USED FOR MANY PURPOSES. A SINGLE PIN CAN BE INSERTED THROUGH AN EXISTING TOOTH TO STRENGTHEN AND STABILIZE IT. OTHER STYLES CAN PROVIDE AN ANCHOR FOR ONE OR MORE ARTIFICIAL TEETH.
� Root Form Dental Implants
� Solid Tapering types
� Solid cylinder
� Pin types
� Screw shaped implant type
� Hollow cylinder design
� Basket design
� Solid Tapering types
� Solid cylinder
� Pin types
� Screw shaped implant type
� Basket design/BOI
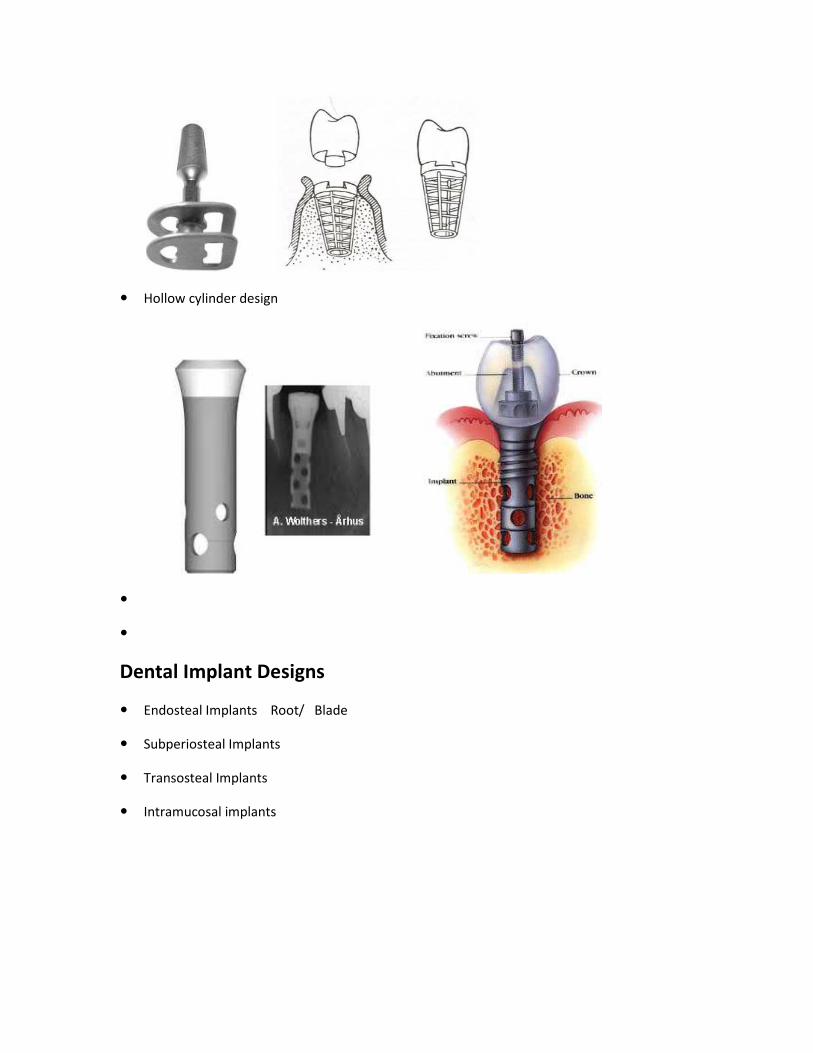
� Hollow cylinder design
�
�
Dental Implant Designs
� Endosteal Implants Root/ Blade
� Subperiosteal Implants
� Transosteal Implants
� Intramucosal implants

BLADE IMPLANT
IT IS A BLADE PLACED DIRECTLY INTO BONE AND MAY BE SOLID OR VENTED. IT MAY BE USED TO SUPPORT SINGLE OR MULTIPLE TEETH. IT USES THE CONCE
SUBPERIOSTEAL IMPLANT:
IS USED WHEN THE BONE HAS ATROPHIED AND JAW STRUCTURE IS LIMITED. THE LIGHTWEIGHT, INDIVIDUALLYBONE, PROVIDING THE EQUIVALENT OF MULTIPLE TOOTH ROOTS. IT MAY BE USED IAREA OR, IF ALL THE TEETH ARE MISSING IN THE ENTIRE MOUTH
� Subperiosteal Implants
IT IS A BLADE PLACED DIRECTLY INTO BONE AND MAY BE SOLID OR VENTED. IT MAY BE USED TO MULTIPLE TEETH. IT USES THE CONCEPT OF ‘FIBROOSSEOUS’ INTEGRATION
SUBPERIOSTEAL IMPLANT:
IS USED WHEN THE BONE HAS ATROPHIED AND JAW STRUCTURE IS LIMITED. THE LIGHTWEIGHT, INDIVIDUALLY-DESIGNED, METAL FRAMEWORK FITS OVER THE REMAINING BONE, PROVIDING THE EQUIVALENT OF MULTIPLE TOOTH ROOTS. IT MAY BE USED IAREA OR, IF ALL THE TEETH ARE MISSING IN THE ENTIRE MOUTH.
IT IS A BLADE PLACED DIRECTLY INTO BONE AND MAY BE SOLID OR VENTED. IT MAY BE USED TO PT OF ‘FIBROOSSEOUS’ INTEGRATION
IS USED WHEN THE BONE HAS ATROPHIED AND JAW STRUCTURE IS LIMITED. THE DESIGNED, METAL FRAMEWORK FITS OVER THE REMAINING
BONE, PROVIDING THE EQUIVALENT OF MULTIPLE TOOTH ROOTS. IT MAY BE USED IN A LIMITED
A Letter to the editor BDJ
Sir,
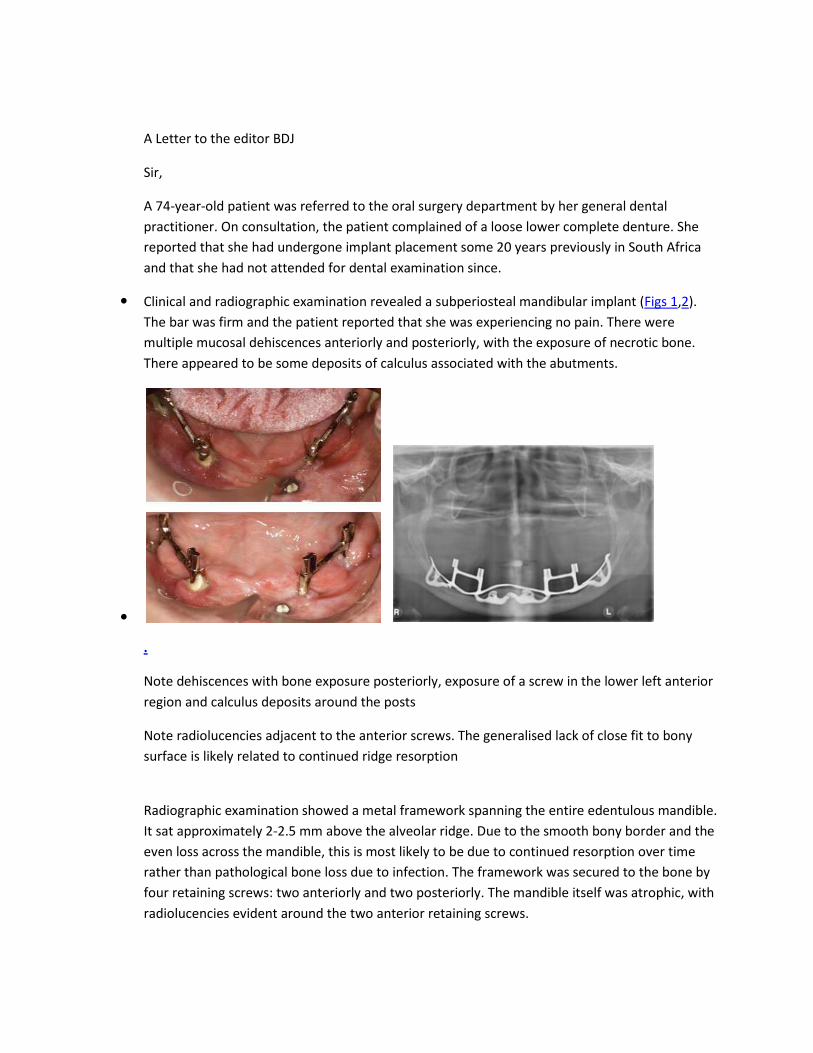
A 74-year-old patient was referred to the oral surgery department by her general dental practitioner. On consultation, the patient complained of a loose lower complete denture. She reported that she had undergone implant placement some 20 years previously in South Africa and that she had not attended for dental examination since.
� Clinical and radiographic examination revealed a subperiosteal mandibular implant (Figs 1,2). The bar was firm and the patient reported that she was experiencing no pain. There were multiple mucosal dehiscences anteriorly and posteriorly, with the exposure of necrotic bone. There appeared to be some deposits of calculus associated with the abutments.
�
.
Note dehiscences with bone exposure posteriorly, exposure of a screw in the lower left anterior region and calculus deposits around the posts
Note radiolucencies adjacent to the anterior screws. The generalised lack of close fit to bony surface is likely related to continued ridge resorption
Radiographic examination showed a metal framework spanning the entire edentulous mandible. It sat approximately 2-2.5 mm above the alveolar ridge. Due to the smooth bony border and the even loss across the mandible, this is most likely to be due to continued resorption over time rather than pathological bone loss due to infection. The framework was secured to the bone by four retaining screws: two anteriorly and two posteriorly. The mandible itself was atrophic, with radiolucencies evident around the two anterior retaining screws.

� Complete subperiosteal implant placement was first described as a treatment for the atrophic mandible in the 1940s. A mucoperiosteal flap would be raised to allow an impression to be made of the surface of the mandible. CT scans were also used to allow CAD/CAM fabrication of the framework, negating the need for impressions. The framework usually rests on the mandible, with no penetration into the bone.
� Due to the high success rates in atrophic mandibles of osseointegrated implants facilitated by the placement of autogenous grafts, subperiosteal implants are no longer used. However, as this case highlights, there may still be some in situwhich could present to the general dental practitioner.
� Manchester
TRANSOSSTEAL IMPLANTS
Transosteal or transosseous dental implants are implants composed of a metal plate and transosteal pins or posts. The metal plate is held with retentive pins or screws fixed to the inferior border of the mandible. This metal plate supports the transosteal pins/posts that penetrate the full thickness of the mandible and project into the mouth in the inter-foraminal area.
� The transosseous dental implants used in humans are the ‘staple bone implant’ system and the ‘transmandibular implant’ system (TMI).
� Transosteal Implants

INTRAMUCOSAL INSERTS
� REPRESENT A FOURTH TYPE OF IMPLANT USED WITH REMOVABLE DENTURES. THE MUSHROOM-SHAPED INSERTS ATTACH TO THE GUM-SIDE OF THE DENTURE AND FIT INTO SPECIALLY PREPARED INDENTIONS IN THE ROOF OF THE MOUTH. THEY PROVIDE GREATLY INCREASED STABILITY AND HOLDING POWER.
� Intramucosal implants

Implant BioMaterials
A. Metals and Alloys
B. Inert ceramics
C. Ca phosphate ceramics
D. Bioactive and biodegradable ceramics
E. Polymers
� Metals and alloys
� Titanium (Pure) 100% Cp Titanium
� Titanium alloy Titanium 90%
Chromium 2%
Molybedenium 7%
Zirconium
� Chromium cobalt Cobalt 66%
alloy Chromium 37%
Molybedenium 7%
� Stainless Steel Iron 70%
Chromium 18%
Nickel12%
� Tantalum / Gold/ Platinium
� Inert Ceramics
� Aluminium oxide Al2O3
i. Polycrystalline
ii. Single crystal
� Zirconium oxide ZrO2
� Zircona

� Titanium Oxide TiO2
ENGINEERING PROPERTIES OF METALS AND ALLOYS USED FOR SURGICAL IMPLANTS
Material Nominal Modulus of Ultimate Elongation Surface
Analysis(w/o) Elasticity Tensile to Fracture(%)
GN/m(psi x 10) MN/m(ksi)
Titanium 99+Ti 97(14) 240-550(25-70) >15 Ti oxide
Ti Al 90Ti-6Al-4V 117(17) 869-896(125-130) >12 Ti oxide
vanadium
Co CrMo- 66Co-27Cr-7Mo 235(34) 655(95) >8 Cr oxide
(casting)
Stainless steel 70Fe-18Cr-12Ni 193(28) 480-1000 >30 Cr oxide
(316L) (70-145)
Zirconium 99+Zr 97(14) 552(80) 20 Zr oxide
Tantalum 99+Ta - 690(100) 11 Ta oxide
Gold 99+Au 97(14) 207-310(30-45) >30 Au
Platinum 99+Pt 166(24) 131(19) 40 Pt
IMPLANT DESIGN

� Crestal Module design
� Internal vs External Hex

� Smooth vs Rough/Threaded
� Cylinder vs Flare
� Platform switch vs Platform shift
Smooth vs Rough/Threaded
Platform switch vs Platform shift

� Crestal Module design
q INTERNAL vs EXTERNAL HEX vs TRI LOBE
q
� Precision fit
� Crestal Module design
q Smooth vs. Rough/Threaded
INTERNAL vs EXTERNAL HEX vs TRI LOBE
Smooth vs. Rough/Threaded

q
� Crestal Module design
q Cylinder vs. Flare
� Crestal Module design
q Platform switch vs shift
q When platform switching, a narrower abutment diameter for a given implant platform diameter is used; for example, placing a 3.8
q However when the implant system provides for a NEP abutment then a Astra, Ankylos, or Bicon.
� 1) Esthetics. .
� 2) Implant Placement Flexibility
� Platform switch/shift
, a narrower abutment diameter for a given implant platform diameter is used; for example, placing a 3.8 mm-wide abutment on a 4.8 mm-wide implant. Osstem
plant system provides for a NEP abutment then a platform shift
2) Implant Placement Flexibility.
, a narrower abutment diameter for a given implant platform diameter wide implant. Osstem
platform shift is done.
� Implant Body Design
� Cylinder vs tapered threaded
� Thread shapes-V thread/buttress/r
� Thread geometry shape/pitch/depth
� Surface preparation-Ti plasma spray coating, sand blasting surface etching, acid etching, laser induced etching, HA coating , Ti Unite™, SLA® surface
� Flat /grooved areas
� Implant Body Design
� Implant Body design
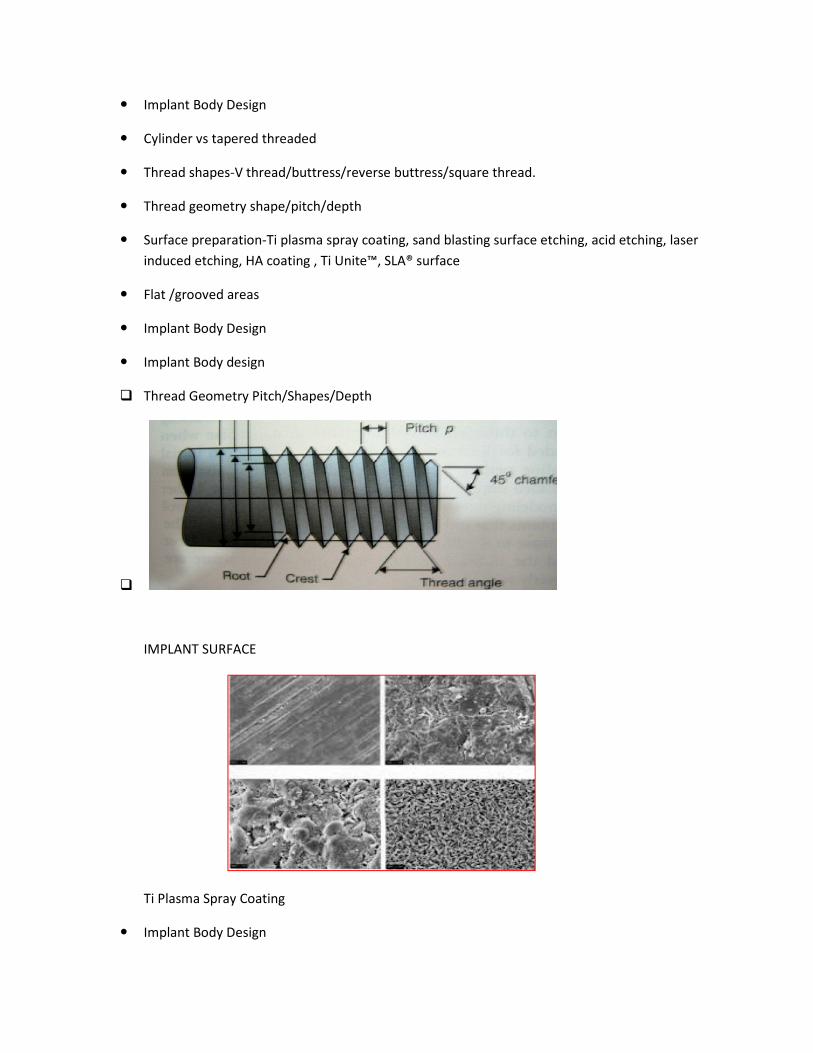
q Thread Geometry Pitch/Shapes/Depth
q
IMPLANT SURFACE
Ti Plasma Spray Coating
� Implant Body Design
Cylinder vs tapered threaded
V thread/buttress/reverse buttress/square thread.
Thread geometry shape/pitch/depth
Ti plasma spray coating, sand blasting surface etching, acid etching, laser induced etching, HA coating , Ti Unite™, SLA® surface
Thread Geometry Pitch/Shapes/Depth
Ti plasma spray coating, sand blasting surface etching, acid etching, laser

q Sand blasting surface etching
� Implant Body Surface Modification
q ACID ETCHING
The acid etched dental implants were immersed in a mixture of HNOsurface treatment, the samples were rinsed with distilled water, dried in an air furnace at 70 ºC for 2 h, packed and sterilized with gamma radiation (25 kgray).
IMPLANT SURFACE MODIFICATIONS
q Laser induced etching/sintering
q SEM image of ablated holes formed on a titanium surface with 0.5 ps pulses of a KrF excimer laser. The laser fluence was 2.4 J/cm2 and 1000 shots were applied (Bereznai et al., 2003).
� Implant Body Surface
H A COATING
Sand blasting surface etching
Implant Body Surface Modification
The acid etched dental implants were immersed in a mixture of HNO3, HCl and Hsurface treatment, the samples were rinsed with distilled water, dried in an air furnace at 70 ºC for 2 h, packed and sterilized with gamma radiation (25 kgray).
LANT SURFACE MODIFICATIONS
Laser induced etching/sintering
SEM image of ablated holes formed on a titanium surface with 0.5 ps pulses of a KrF excimer laser. The laser fluence was 2.4 J/cm2 and 1000 shots were applied (Bereznai et al., 2003).
, HCl and H2SO4 After surface treatment, the samples were rinsed with distilled water, dried in an air furnace at 70 ºC
SEM image of ablated holes formed on a titanium surface with 0.5 ps pulses of a KrF excimer laser. The laser fluence was 2.4 J/cm2 and 1000 shots were applied (Bereznai et al., 2003).

� HA coatings on dental implants have been shown to accelerate surface bone apposition, shortening the waiting period for dental implant restoration.
� HA surface known to degrade and in some instances separates
� Implant Body Surface
q Ti Unite™
q TiUnite is titanium oxide rendered into an osseoconductive ceramic biomaterial through spark anodization. Unlike implants with machined surfaces, TiUnite has clinically demonstrated the ability to increase the predictability and speed at which dental implants osseointegrate through osseoconductivity.
� Implant Body Surface
q SLA® surface
� Surface roughening is achieved through large grit sand-blasting with corundum particles followed by acid etching, commonly referred to as SLA® surface.
� The SLActive® surface has less surface tension and increases hydrophilic properties (wetability) intended to attract blood cells. SLActive® treated implants are stored and shipped in a vial filled with an isotonic liquid (salt water) to preserve the reduced surface tension qualities of the implant.
� Implant Body Design
� Cylinder vs tapered threaded

� Apex design
Tapered
� Antirotational Feature
Hole/Vent
Grooves/Flat sides
� Flat /Rounded End
NobelReplace™ Tapered
� History of NobelReplace™
� Evolution of NobelReplace™
Easy to use

Prosthetic connection design for ease of use and to stabilise prosthetic
Standardized tapered drilling protocol
Groovy to enable faster bone formation
Coronal design to improve soft tissue support
Tapered body design for optimal initial stability
Triunite oxidised surface to enhance osseointegration
� NobelReplace™ – Strong user benefits
� Tri-channel internal connection
� Color-coding
The implant of choice for Advanced Users
Prosthetic connection design for ease of use and to stabilise prosthetic restorations
Standardized tapered drilling protocol
Groovy to enable faster bone formation
Coronal design to improve soft tissue support
Tapered body design for optimal initial stability
Triunite oxidised surface to enhance osseointegration
Strong user benefits
channel internal connection
The implant of choice for Advanced Users: Treatment predictability/Safety
restorations

Ease-of-use, simplified drilling protocols, consistent restorative oustability allows the use of NobelReplace also in more demanding indications.
Clinical flexibility
Satisfies broad range of indication: from single tooth to fully edentulous restorations as well as temporary solutions. Due to itsplacement in extraction sites.
Suitable for NobelGuide
Prosthetic versatility
Tri-channel connection supports all types of restorative solutions including individualized NobelProcera prosthetic sollong term esthetics and functionality.
NobelReplace™ Tapered Groovy
TiUnite “all the way up”
• Strong and faster osseointegration than machined surface implants
Grooves on Threads
• Bone is formed more rapidly inside the groove
High stability
Grooves on Collar
• Intended for hard and soft tissue stabilization and improved long term esthetics
use, simplified drilling protocols, consistent restorative outcomes and optimal initial stability allows the use of NobelReplace also in more demanding indications.
Satisfies broad range of indication: from single tooth to fully edentulous restorations as well as temporary solutions. Due to its tapered design NobelReplace is also ideal for immediate placement in extraction sites.
channel connection supports all types of restorative solutions including individualized NobelProcera prosthetic solutions. It also secures accurate prosthetic positioning and provides long term esthetics and functionality.
NobelReplace™ Tapered Groovy
osseointegration than machined surface implants
Bone is formed more rapidly inside the groove
for hard and soft tissue stabilization and improved long term esthetics
tcomes and optimal initial
Satisfies broad range of indication: from single tooth to fully edentulous restorations as well as tapered design NobelReplace is also ideal for immediate
channel connection supports all types of restorative solutions including individualized utions. It also secures accurate prosthetic positioning and provides
for hard and soft tissue stabilization and improved long term esthetics

� Differences between Replace™ Select Tapered and NobelReplace™ Tapered
� Implant surface and grooves
� Bone forms faster within the grooves, compared to implant surfaces without grooves
� Resulting in higher implant stability2
� Grooves on collar:designed esthetics
1.Zechner et al. Clin Oral Implants Res 2003
SINGLE TOOTH RESTORATION
Young female, non-smoker, no parafunctional habit, persistent deciduous lateral incisor
Diagnosis Extraction of persistent deciduous lateral incisor. Orthodontic treatment finalized. Missing lateral central incisor, limited space to adjacent teeth.
Treatment Insertion of a NobelReplace Tapered Groovy NP/13 mm implant, intraoperative X-rays shows narrow space conditions, immediate loading with a temporary resin crown.
Replace™ Select Tapered and NobelReplace™ Tapered
surface and grooves – Osseointegration1
Bone forms faster within the grooves, compared to implant surfaces without grooves
Resulting in higher implant stability2
for hard and soft tissue stabilization and improved long term
Zechner et al. Clin Oral Implants Res 2003
SINGLE TOOTH RESTORATION
smoker, no parafunctional habit, persistent deciduous lateral incisor
Extraction of persistent deciduous lateral incisor. Orthodontic treatment finalized. Missing lateral central incisor, limited space to adjacent teeth.
Insertion of a NobelReplace Tapered Groovy NP/13 mm implant, shows narrow space conditions, immediate loading with a temporary resin crown.
Bone forms faster within the grooves, compared to implant surfaces without grooves
for hard and soft tissue stabilization and improved long term
smoker, no parafunctional habit, persistent deciduous lateral incisor
Extraction of persistent deciduous lateral incisor. Orthodontic treatment finalized. Missing lateral central
shows narrow space conditions, immediate loading with a temporary resin crown.

Treatment Insertion of a NobelReplace Tapered Groovy NP/13 mm implant, intraoperative X-rays shows narrow space conditions, immediate loading with a temporary resin crown.
Results
Excellent esthetics and soft tissue response shortly after final esthetic installed and after three years
� Multiple teeth restoration
Young female, came to clinic because of trauma against central incisors
Treatment Atraumatic extraction of central incisors. Flapless immediate implant placement 2 NobelReplace Tapered Groovy, WP Platform Shifting.
Products used
2 NobelReplace Tapered WP
2 NobelProcera Zirconia Abutments
2 NobelProcera Alumina Crowns
Results
2 NobelProcera Alumina Crowns (Graft for soft tissue thickness).
� NobelActive™ design
Insertion of a NobelReplace Tapered Groovy NP/13 mm implant, rays shows narrow space conditions, immediate loading with a temporary resin crown.
Excellent esthetics and soft tissue response shortly after final esthetic installed and after three years
Young female, came to clinic because of trauma against central incisors
extraction of central incisors. Flapless immediate implant placement 2 NobelReplace Tapered Groovy, WP Platform Shifting.
2 NobelReplace Tapered WP
2 NobelProcera Zirconia Abutments
2 NobelProcera Alumina Crowns
a Crowns (Graft for soft tissue thickness).
rays shows narrow space conditions, immediate loading with a temporary resin crown.
Excellent esthetics and soft tissue response shortly after final esthetic installed and after three years
extraction of central incisors. Flapless immediate implant placement 2 NobelReplace

• Expanding tapered body with double variable thread design and apical drilling blades.
• Manual insertion protocol
Benefits
• Gradual bone condensing and high initial
• Enables ”active” directional changes for optimal restorative position
� NobelActive™ design
Features:
Triunite
groovy
Features
Expanding tapered body with double variable thread design and apical drilling blades.
Gradual bone condensing and high initial stability
Enables ”active” directional changes for optimal restorative position
Expanding tapered body with double variable thread design and apical drilling blades.

Benefits
• Documented to enhance osseointegration and increase of the predictability of implant treatment1
• Bone forms faster within the grooves, compared to implant without grooves2
� NobelActive™ design
Benefits
• Allows for maximum alveolar bone volume around implant for improved soft tissue support
Animation: Bone condensing
� NobelActive™ design
Features:
APICAL:Drilling blades on apex.
BENEFITS:
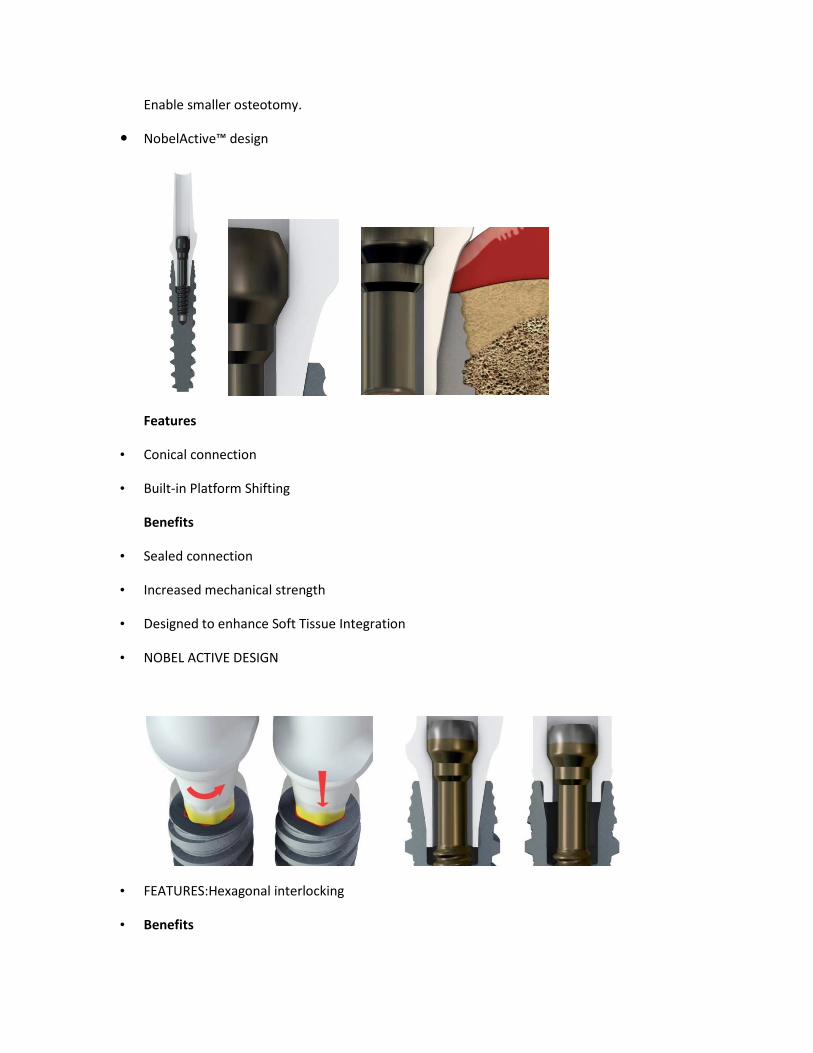
Enable smaller osteotomy.
� NobelActive™ design
Features
• Conical connection
• Built-in Platform Shifting
Benefits
• Sealed connection
• Increased mechanical strength
• Designed to enhance Soft Tissue Integration
• NOBEL ACTIVE DESIGN
• FEATURES:Hexagonal interlocking
• Benefits

• Secure reposition of prosthetic components
• Allows for prosthetic flexibility and implant level bridges
Dual-function prosthetic connection
� NobelActive™ Macro Design Features
1. Coronal portion back taper (except 3,5)
• Maximizes the volume of alveolar bone around the implant
2. Constantly expanding central core
• Acts like a threaded osteotome
• Compacts the bone outward
• Provides excellent primary stability
3. Sharp blades, deep widely spaced 35º double lead threads
• Allows implant to condense through bone
• Actively changes direction
� Titanium Abutment Fit Into Implant

�
� Insertion Torque Discussion
Insertion torque requirements for different implant designs are not comparable.
The NobelActive implant requires higher insertion torque due to the large helix angle of the thread
For each rotation, the implant advances 2.4 mm
� Occlusal Forces and Implant Design
� Stress and strain cause crestal bone loss and decrease long term survival of implant.
Force applied to dental implants may be characterised as
q Force Magnitude
q Force duration
q Force Type
q Force Direction
OCCLUSAL FORCES AND IMPLANT DESIGNS
Insertion Torque Discussion
e requirements for different implant designs are not comparable.
The NobelActive implant requires higher insertion torque due to the large helix angle of the
For each rotation, the implant advances 2.4 mm
Occlusal Forces and Implant Design
and strain cause crestal bone loss and decrease long term survival of implant.
Force applied to dental implants may be characterised as
OCCLUSAL FORCES AND IMPLANT DESIGNS
e requirements for different implant designs are not comparable.
The NobelActive implant requires higher insertion torque due to the large helix angle of the
and strain cause crestal bone loss and decrease long term survival of implant.

q Force magnitude
� Average forces of mastication vary from 10lb to 350lb
� Molars 200lb Canine100lb Incisors 25-35lb
� Parafunction as high as 1000lb
� Occlusal Forces and Implant Design
q Force Duration
� Normally teeth are loaded during swallowing and eating which is less than 30 min /day
� Bruxism increases duration to several hrs a day
� Occlusal Forces and Implant Design
q Force Type
� Compression, tension and shear
� Bone is strongest under compression ,35% weaker under tension and 65% weaker when loaded in shear
� Occlusal Forces and Implant Design
q Force Direction
� Implant that is angled receives increased amount of shear loads especially in the crestal region.
� Angled implant will also receives more stress on the overall implant system with increased risk of abutment screw loosening and and fatigue fractures of the implant or its components.
� Occlusal Forces and Implant Design
q Force Magnification
� Occurs when the stress is increased beyond the usual conditions of load.
Ø Cantilevered prosthesis
Ø Crown height ratio greater than normal
Ø Parafunction
� IMPLANT SIZE AND DIAMETER
� Short vs long implants: To obtain predictable success in situations with most patient force factors or bone densities, there is minimum implant length, depending on the implant body

width and the implant design. After the ideal treatment plan determines the key implant positions and implant number, the implant length selected for most treatment plan options is at least 12 mm long.
� Wide vs narrow implants :The logical method to increase functional surface area is to increase the implant diameter , because the opposing landmarks limit the implant length. Wider root form designs exhibit a greater area of bone contact than narrow implants of similar design, in part from an increase in circumferential bone contact.
SHORT VS LONG IMPLANTS
DISADVANTAGES
� Studies show success with implant lengths of at least 10-15mm in lengths
� Implants 10mm and smaller had increased failure rates.( 10% vs 3%)
� Failures of short implants occurred after prosthetic loading and especially in the posterior region
q ADVANTAGES
� Bone grafting not required to restore alveolar ht
� Less risk of damage to adjacent structures and thermal insult during osteotomy
� Surgical ease
� IMPLANT SIZE:SHORT VS LONG
GUIDELINES
� Increase diameter
� Splint together
� Decrease crown ht
� Decrease cantilever
� Increase surface area design
� OD vs FPD
� Minimise lateral forces
� Improve bone density

� WIDE VS NARROW IMPLANTS
q ADVANTAGES
� Surgical Rescue implant
� Failed implant/immediate implant
� Tooth extraction/immediate
� Increased surface area
� Compensate unfavourable patient force factors
� Enhance surface for short implants
� Compensate for poor bone density
� Minimise loads for angled implants/cantilevers
q DISADVANTAGES
� Bone trauma because of extended drill sequence
� Decreased facial thickness may lead to recession
� Stress shielding
� Increased surgical failure rate
� Too close to adjacent tooth ,PDL encroachment
� Selecting an Implant System
� Training
� Budget
� Established company
� Versatility of System
� Mentorship
� Warranty

THANK YOU
Suggested references:
Branemark PI,Hansson BO,Adell R, Briene U,Lindstorm J,Hallen O,et al.(1997).Osseoitegrated implants in the treatment of the edentulous jaw,experience from a 10yr period.Scand J Plast.Reconstr Surg 16:1-132
Goldberg NI,Gershkoff A (1949),The implant lower denture.Dental digest 55 :490-494
Subperiosteal implants,H Beddis,S Lello,J Cunliffe &P Coulthard BDJ 212,4(2012)Published online:13jan 2012,doi;10.1038/sj;bdj:2012:6
Small IA, Misiek D(1986),Asixteen year evaluation of the mandibular staple bone plate.J. Oral Maxillofac. Surg. 44:60-66
Dahl G,History of intramuscular inserts.J Oral Implantol 1991;17(4):440
Becker J, Ferrari D, Herten M, Kirsch A, Schaer A, Schwartz F, Influence of platform switching on crestal bone changes at non submerged titanium implants :A histomorphometrical study in dogs.J Clin Periodontal 2007;34:1089-1096.
Vigolo P, Givani A, Platform switched restorations on wide diameter implants;a 5yr clinical prospective study.Int J Oral Maxillof Implants 2009;24:103-109.
Fickl S, Zuhr O, Stein JM, Hurzeler MB.Periimplant bone level around implants with platform switched abutments .Int J Oral Maxillofac.implants 2010;25:577-581
Berenznai et al,2003, Glauser R , Zembic A, Rahstaller P,Windisch S.Five year results of implants with an oxidized surface placed predominantly in soft quality bone and subjected to immediate occlusal loading.J Prosthet.Dent.2007;97(suppl):559-568.