impact of computerized physician order entry (cpoe) on picu prescribing errors
TRANSCRIPT
Barbara MaatCasper W. BollenAdrianus J. van VughtToine C. G. EgbertsCarin M. A. Rademaker
Impact of computerizedphysician order entry (CPOE)on PICU prescribing errors
Accepted: 7 December 2013Published online: 19 December 2013� Springer-Verlag Berlin Heidelberg andESICM 2013
Dear Editor,Prescribing errors frequently occur inpediatric intensive care units (PICUs),for which both low- and high-tech-nology solutions have been evaluated[1, 2]. Computerized physician orderentry (CPOE) systems, includingclinical decision support (CDS), offerthe potential to reduce prescribingerror rates in PICUs, but only if welldesigned and implemented [2–4]. Weexamined frequency, types, and riskfactors of PICU prescribing errors inrelation to use of CPOE.
This prospective study was per-formed in a 14-bed PICU of a tertiary
children’s hospital using a home-grown CPOE system since 2001.Contemporaneously, orders could behandwritten, allowing comparison.Medication orders of all patientsadmitted between February 2008 andDecember 2010 were reviewed forprescribing errors. The study wasperformed in accordance with theinstitutional review board guidelines.
A total of 718 patients wereincluded with 22,280 medicationorders, of which 15,136 (68 %) werehandwritten and 7,144 (32 %) CPOE.Omission rates were 66 % in hand-written versus 24 % in CPOE orders.Writing by hand was a strong riskfactor for omissions, but CPOE didnot reduce the error rate to zero. Thiswas mainly due to the possibility toenter free text into the CPOE system.Because an order has to be completefor the purpose of dose checking, westate that free text entry should beminimized.
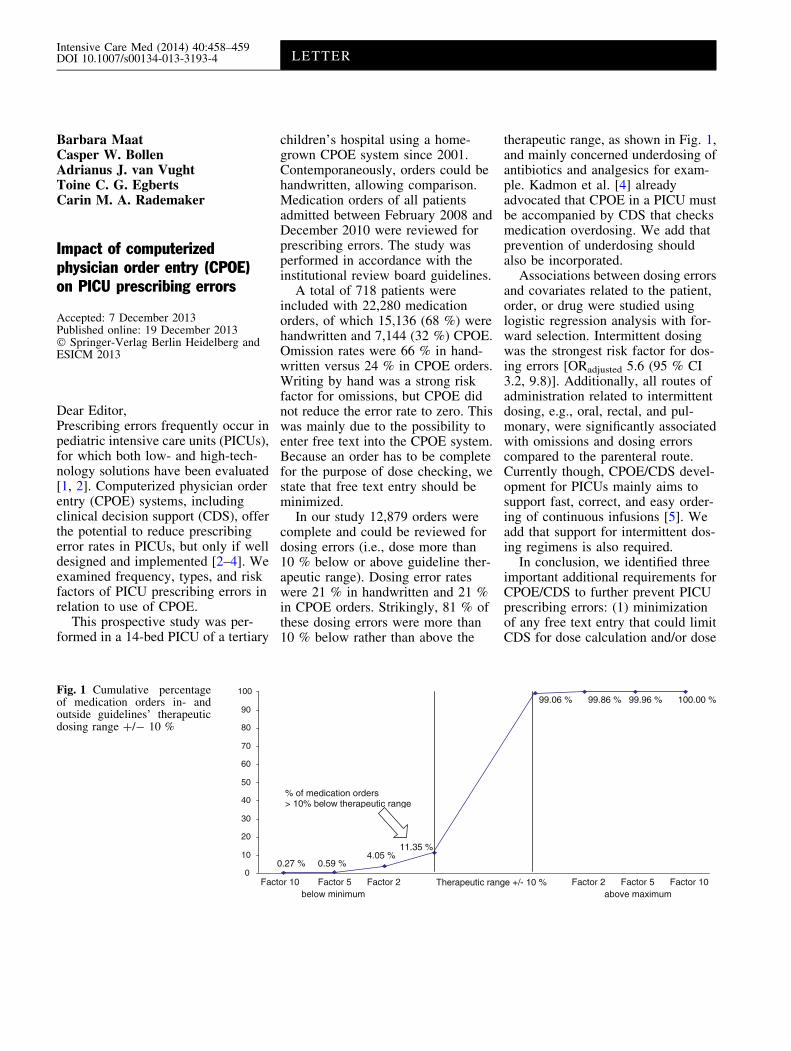
In our study 12,879 orders werecomplete and could be reviewed fordosing errors (i.e., dose more than10 % below or above guideline ther-apeutic range). Dosing error rateswere 21 % in handwritten and 21 %in CPOE orders. Strikingly, 81 % ofthese dosing errors were more than10 % below rather than above the
therapeutic range, as shown in Fig. 1,and mainly concerned underdosing ofantibiotics and analgesics for exam-ple. Kadmon et al. [4] alreadyadvocated that CPOE in a PICU mustbe accompanied by CDS that checksmedication overdosing. We add thatprevention of underdosing shouldalso be incorporated.
Associations between dosing errorsand covariates related to the patient,order, or drug were studied usinglogistic regression analysis with for-ward selection. Intermittent dosingwas the strongest risk factor for dos-ing errors [ORadjusted 5.6 (95 % CI3.2, 9.8)]. Additionally, all routes ofadministration related to intermittentdosing, e.g., oral, rectal, and pul-monary, were significantly associatedwith omissions and dosing errorscompared to the parenteral route.Currently though, CPOE/CDS devel-opment for PICUs mainly aims tosupport fast, correct, and easy order-ing of continuous infusions [5]. Weadd that support for intermittent dos-ing regimens is also required.
In conclusion, we identified threeimportant additional requirements forCPOE/CDS to further prevent PICUprescribing errors: (1) minimizationof any free text entry that could limitCDS for dose calculation and/or dose
0
10
20
30
40
50
60
70
80
90
100
0.27 % 0.59 %4.05 %
11.35 %
99.06 % 99.86 % 99.96 % 100.00 %
Factor 10 Factor 5 Factor 2 Factor 2 Factor 5 Factor 10above maximumbelow minimum
Therapeutic range +/- 10 %
% of medication orders> 10% below therapeutic range
Fig. 1 Cumulative percentageof medication orders in- andoutside guidelines’ therapeuticdosing range ?/- 10 %
Intensive Care Med (2014) 40:458–459DOI 10.1007/s00134-013-3193-4 LETTER

checking, (2) dose checking supportincluding lower and upper limits, and(3) simultaneous support for bothordering continuous infusions andintermittent dosing schemes.
Acknowledgments We thank Koos J.G. Jansen and the PICE (Pediatric IntensiveCare Evaluation) database for providingpatient admission data. We thank HannekeJ. H. den Breeijen and the Utrecht PatientOriented Database (UPOD) for extensivehelp with data management. We thankNicole J. M. Willard, Chantal Ricken,Bianca W. J. Bakkum, Ruud van der Noll,Eva V. A. Mulder, Tessa van der Maaden,Esther Kuipers, Stefan W. C. van Roosma-len, Cynthia Lagrand, and Annemieke D.M. van der Kaaij, at the time master’sdegree students of the Utrecht UniversityFaculty of Pharmaceutical Sciences, forcollecting much of the data.
Ethical standards This study was per-formed in accordance with the ethicalstandards laid down in the 1964 Declarationof Helsinki and its later amendments. Thestudy was approved by the InstitutionalReview Board of the University MedicalCenter Utrecht.
Conflicts of interest The authors declare
that they have no conflict of interest.
References
1. Booth R, Sturgess E, Taberner-Stokes A,Peters M (2012) Zero toleranceprescribing: a strategy to reduceprescribing errors on the paediatricintensive care unit. Intensive Care Med38:1858–1867
2. van Rosse F, Maat B, Rademaker CM,van Vught AJ, Egberts AC, Bollen CW(2009) The effect of computerizedphysician order entry on medicationprescription errors and clinical outcomein pediatric and intensive care: asystematic review. Pediatrics123:1184–1190
3. Warrick C, Naik H, Avis S, Fletcher P,Franklin BD, Inwald D (2011) A clinicalinformation system reduces medicationerrors in paediatric intensive care.Intensive Care Med 37:691–694
4. Kadmon G, Bron-Harlev E, Nahum E,Schiller O, Haski G, Shonfeld T (2009)Computerized order entry with limiteddecision support to prevent prescriptionerrors in a PICU. Pediatrics 124:935–940
5. Lehmann CU, Kim GR, Gujral R, VeltriMA, Clark JS, Miller MR (2006)Decreasing errors in pediatric continuousintravenous infusions. Pediatr Crit CareMed 7:225–230
B. Maat ()) � T. C. G. Egberts �C. M. A. RademakerDepartment of Clinical Pharmacy,D.00.2.04, University Medical CenterUtrecht, P. O. Box 85500, 3508 GA Utrecht,The Netherlandse-mail: [email protected].: ?31-88-7557218Fax: ?31-88-7555316
C. W. Bollen � A. J. van VughtDepartment of Pediatric Intensive Care,KG.02.301.0, Wilhelmina Children’sHospital, University Medical CenterUtrecht, P. O. Box 85090, 3508 AB Utrecht,The Netherlands
T. C. G. EgbertsDepartment of Pharmacoepidemiology andClinical Pharmacology, Utrecht Institute forPharmaceutical Sciences, UtrechtUniversity, P. O. Box 80082, 3508 TBUtrecht, The Netherlands
459