impact of birth hiv pcr testing on uptake of follow-up eid...
TRANSCRIPT
Impact of birth HIV PCR testing on uptake of follow-up EID services for HIV-exposed infants in Cape Town
Lorna Dunning1, Max Kroon2, Lezanne Fourie2, Andrea Ciaranello3, Landon Myer1
1Division of Epidemiology & Biostatistics, School of Public Health and Family Medicine, University of Cape Town, South Africa2Department of Neonatal Medicine, University of Cape Town, South Africa3 Division of Infectious Disease, Medical Practice Evaluation Center, Massachusetts General Hospital, Boston, MA, USA
Pediatric HIV Workshop 2016
Background – Early Infant Diagnosis
• WHO recommends all HIV-exposed infants should be tested by six weeks of age – Virological tests
– Detect in utero, intra-partum and very early post-partum infections*
• 94% of HIV-exposed infants have access to a virologic test in South Africa1
* Debate around effect of infant prophylaxis on the sensitivity of the assay at 6 weeks1 World Health Organization. Progress report on the global plan towards the elimination of new HIV infections among children and keeping their mothers alive. Geneva, Switzerland2015

Background – 6 week EID Cascade
Infant born HIV-
exposed
6 weeks-Offer HIV
testing
Specimen Processing
Result Return
HIV-infected InfantLink to care - ART
HIV-uninfected Exposed Infant
Repeat testing after weening
Peak age of mortality 11
weeks for HIV-infected
infants
Background – Birth Testing
• Improved PMTCT coverage
– Increased proportion of in utero infections relative to intrapartum and early post partum
– More infected infants detectable at birth
• Benefits earlier treatment
– Limit disease progression
– Lower viral reservoirs
– Increase survival1
1 Francke et al. Clinical impact and cost effectiveness of early infant HIV diagnosis in South Africa: Test timing and frequency. Pre-publication JID

Background – Birth Testing Cascade
Birth-HIV PCR testing
Specimen Processing
Result Return
Birth Testing
HIV-exposed
Infant
Infant born HIV-exposed
6 week-HIV PCR testing
Specimen Processing
Result Return
HIV-infected InfantLink to care - ART
HIV-uninfected Exposed Infant
Repeat testing after weening
HIV-infected –Linked to Care
LTFU?
Returning a negative result to women immediately after delivery could cause confusion around the need for testing at 6 weeks• Recent observational study – only 49% of infants returned for follow up testing after
an initial test at birth1
1 J Matritz et al. Low Uptake of Routine Infant Diagnostic Testing Following HIV PCR Testing at Birth. Poster Presentation. CROI 2016

Objectives
1. To compare the attendance at follow-up EID testing by receipt of an HIV PCR test at birth- Does receipt of a negative birth test impact uptake of 6 weeks testing?
2. Examine yield of targeted birth testing in this setting
Site Characteristics• Secondary level
- Obstetric Hospital• Women referred from
primary care • 13% of newborn HIV-exposed
Cohort Characteristics• July 2013 – August 2015• All mothers eligible for Option B+ • HIV PCR test at birth – Infants high risk for perinatal transmission• Birth tests occurred within 48hrs of delivery: result return prior to discharge• All HIV exposed infants tested at 6 weeks, or screened if presenting to hospital
with OI
Methods – Site and Cohort Characteristics
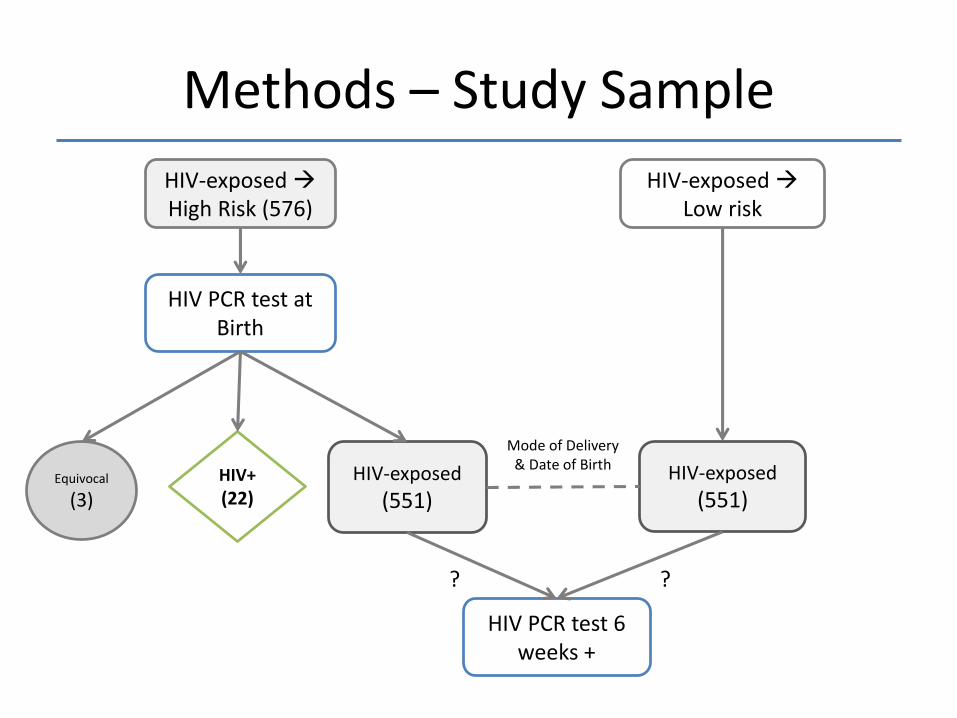
Methods – Study Sample
HIV-exposed High Risk (576)
HIV PCR test at Birth
Equivocal
(3)HIV+
(22)HIV-exposed
(551)HIV-exposed
(551)
HIV-exposed Low risk
Mode of Delivery & Date of Birth
HIV PCR test 6 weeks +
??

1. Results of HIV PCR tests were determined from NHLS database– Non-attendance at follow up testing:
no subsequent HIV PCR test recorded since birth test or no recorded HIV PCR test
– Linkage to care: Infect infant specimen sent to laboratory for processing
2. Participant demographic characteristics – Mean/median, frequency
3. Logistic regression models – OR with 95% confidence intervals
Analysis

6%
38%
15%
15%
14%
6%
5%
4%4%
3%
1% 1% 2%
Results – HIV-exposed infants receiving an HIV PCR test at Birth
6%
38%
15%15%
14%
6%
5%
4%
4% 3%
1% 1% 2%
6%
38%
15%15%
14%
6%
5%
4%4%
3%
1% 1% 2%
6%
38%
15%15%
14%
6%
5%
4%4%
3%
1%1%
2%
6%
38%
15%15%
14%
6%
5%
4%4%
3% 1% 1%2%
No Reason
ART <12 weeks
Low Birthweight / Preterm
High Viral Load
Default from Treatment
Unbooked
No ART during Pregnancy
Seroconverted during Pregnancy
Maternal Infection
2nd Line Treatment
Substance Abuse
Other
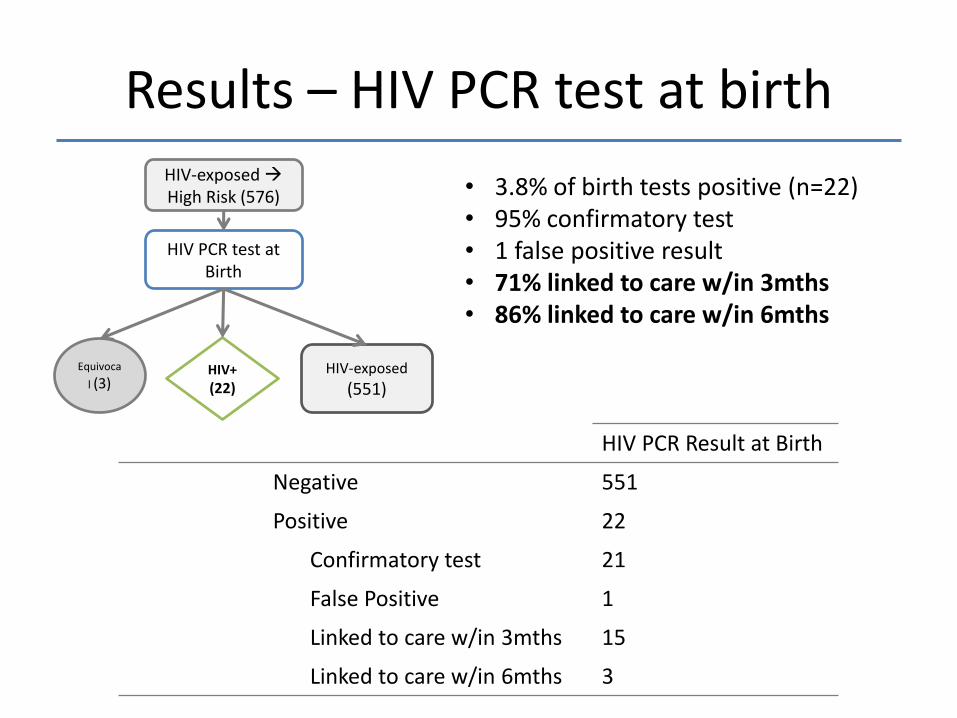
Results – HIV PCR test at birthHIV-exposed High Risk (576)
HIV PCR test at Birth
Equivoca
l (3)HIV+
(22)HIV-exposed
(551)
• 3.8% of birth tests positive (n=22)• 95% confirmatory test• 1 false positive result • 71% linked to care w/in 3mths• 86% linked to care w/in 6mths
HIV PCR Result at Birth
Negative 551
Positive 22
Confirmatory test 21
False Positive 1
Linked to care w/in 3mths 15
Linked to care w/in 6mths 3
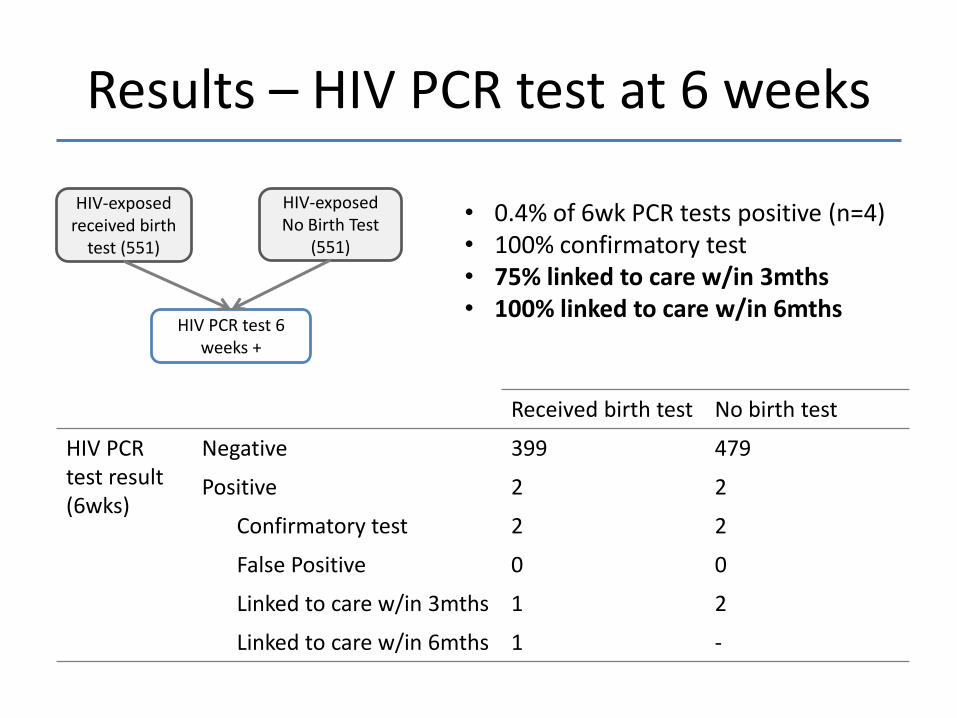
HIV-exposed received birth
test (551)
HIV-exposed No Birth Test
(551)
HIV PCR test 6 weeks +
Results – HIV PCR test at 6 weeks
Received birth test No birth test
HIV PCR test result(6wks)
Negative 399 479
Positive 2 2
Confirmatory test 2 2
False Positive 0 0
Linked to care w/in 3mths 1 2
Linked to care w/in 6mths 1 -
• 0.4% of 6wk PCR tests positive (n=4)• 100% confirmatory test• 75% linked to care w/in 3mths• 100% linked to care w/in 6mths
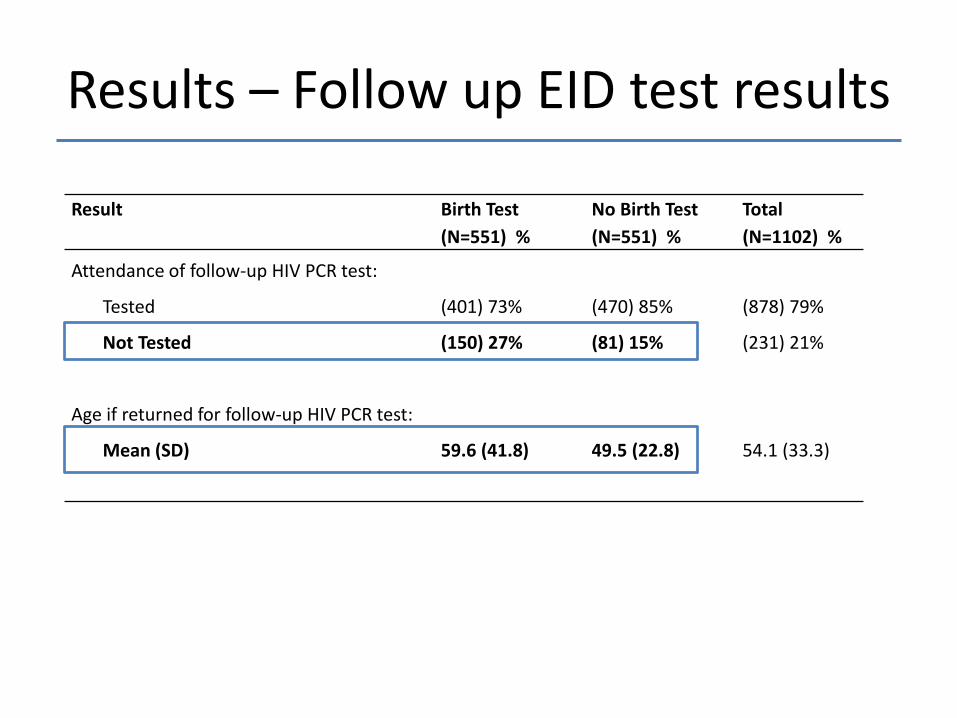
Results – Follow up EID test results
Result Birth Test
(N=551) %
No Birth Test
(N=551) %
Total
(N=1102) %
Attendance of follow-up HIV PCR test:
Tested
Not Tested
(401) 73%
(150) 27%
(470) 85%
(81) 15%
(878) 79%
(231) 21%
Age if returned for follow-up HIV PCR test:
Mean (SD) 59.6 (41.8) 49.5 (22.8) 54.1 (33.3)
Age if returned for 6wk HIV PRC
Less than 28 days
4 – 10 weeks
10 weeks – 6 months
6 – 9 months
9 – 12 months
(4) 1%
(337) 84%
(50) 13%
(5) 1%
(5) 1%
(10) 2%
(436) 91%
(32) 7%
(2) 0.4%
(1) 0.2%
(14) 1%
(773) 70%
(82) 7%
(7) 0.6%
(6) 0.5%

Variable Birth Test
% (N=551)
No Birth Test
% N=551)
Total
% (N=1102)
Sex:
Female (279) 51% (276) 50% (555) 50%
Birthweight (g):
Low (<2500) (184) 34% (45) 7% (229) 21%
Mode of Delivery
C/S (291) 53% (291) 53% (582) 53%
Gestation (wks)
Preterm (34-37) (148) 27% (50) 9% (198) 17%
Infant Feeding
Breastfeeding (438) 80% (460) 83% (898) 82%
Maternal Age (years)
Adolescent Mothers (<24) (157) 29% (102) 19% (259) 24%
Maternal Population Group
Black African (433) 79% (454) 82% (887) 81%
Results – Demographics
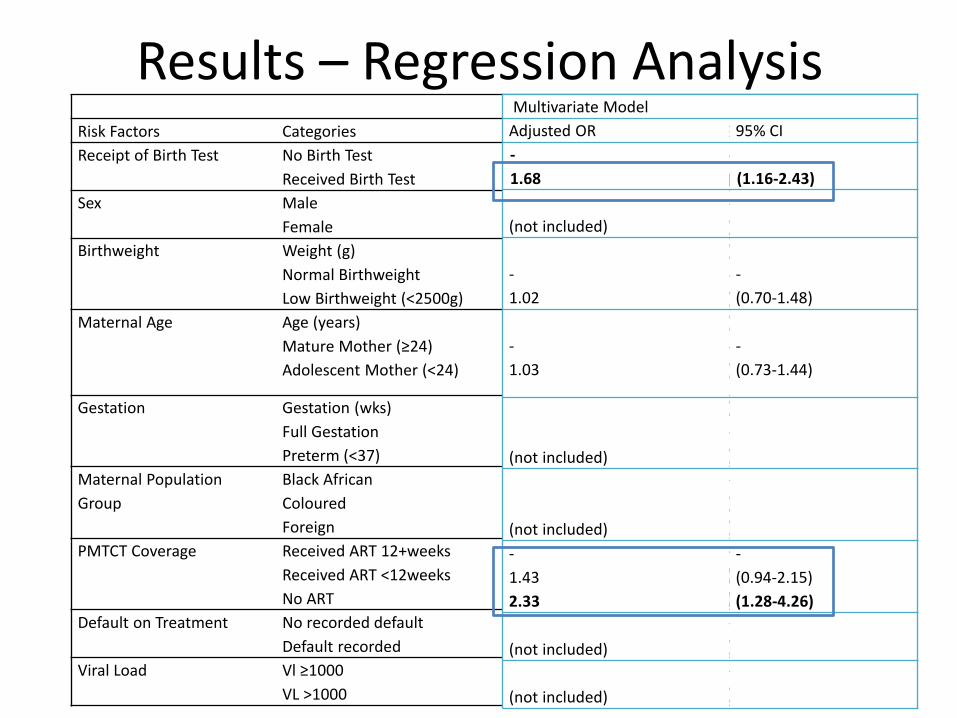
Results – Regression AnalysisUnivariate Model
Risk Factors Categories Crude OR 95% CI
Receipt of Birth Test No Birth Test
Received Birth Test
-
2.17
-
(1.61-2.93)
Sex Male
Female
-
0.92
-
(0.69-1.23)
Birthweight Weight (g)
Normal Birthweight
Low Birthweight (<2500g)
1.00
-
0.79
(0.99-1.00)
-
(0.56-1.12)
Maternal Age Age (years)
Mature Mother (≥24)
Adolescent Mother (<24)
1.01
-
0.86
(0.98-1.03)
-
(0.62-1.21)
Gestation Gestation (wks)
Full Gestation
Preterm (<37)
1.00
-
0.93
(0.95-1.07)
-
(0.64-1.35)
Maternal Population
Group
Black African
Coloured
Foreign
-
0.69
0.37
-
(0.43-1.09)
(0.06-2.25)
PMTCT Coverage Received ART 12+weeks
Received ART <12weeks
No ART
-
2.03
3.24
-
(1.44-2.86)
(1.85-5.66)
Default on Treatment No recorded default
Default recorded
-
0.94
-
(0.52-1.69)
Viral Load Vl ≥1000
VL >1000
-
1.42
-
(0.85-2.37)
Multivariate Model
Adjusted OR 95% CI
-
1.68 (1.16-2.43)
(not included)
-
(0.69-1.23)
-
1.02
-
(0.70-1.48)
-
1.03
-
(0.73-1.44)
(not included)
0.95-1.07)
-
(0.64-1.35)
(not included)
-
(0.43-1.09)
(0.06-2.25)
-
1.43
2.33
-
(0.94-2.15)
(1.28-4.26)
(not included)
-
(0.52-1.69)
(not included)
-
(0.85-2.37)

Results – Subgroup analyses
Adjusted OddsRatio
Restricted analyses showing effect size in multiple subpopulations: Association between non-attendance at follow-up EID testing for infants who received a birth test compared to those that did not
All
HIV
exp
osed In
fants
Pre
term
Full Ges
tatio
n
Low B
irth
wei
ght
Norm
al B
irthw
eight
Adole
scen
t Moth
er
Mat
ure M
other
Popula
tion G
roup-B
lack
Afric
an
Popula
tion G
roup-O
ther
0.1
1
10
AdOR for non-reportingat follow up EID testing forno HIV PCR test receivedat birth
All LBW Norm BW
Pre-term
Full term
Mother <24yrs
Mother >24yrs
Black African
Other
All
HIV
exp
osed In
fants
Pre
term
Full Ges
tatio
n
Low B
irth
wei
ght
Norm
al B
irthw
eight
Adole
scen
t Moth
er
Mat
ure M
other
Popula
tion G
roup-B
lack
Afric
an
Popula
tion G
roup-O
ther
0.1
1
10
AdOR for non-reportingat follow up EID testing forno HIV PCR test receivedat birth
Limitations
• Results reflect a single urban setting within South Africa. All participants delivered at an obstetric hospital
– Generalizations should be made with caution
• Social and demographic variables would provide greater insight into predictors for non-attendance
– Risk factors used to identify infants as high risk at delivery could also be predictors for non-attendance

Conclusions
1. Targeted birth testing successfully identified mothers at high risk for transmission to their infants
2. Neonates undergoing HIV testing at birth appear less likely to receive subsequent EID testing compared to infants who did not receive a birth test. – More emphasis on negative results
– How does universal birth testing affect these results?

Acknowledgements
Research supported by the Elizabeth Glaser Pediatric AIDS Foundation
Leigh Anne van Balla & Alex Paone for their contribution during data collection, along with all the
staff at MMH.