impact - aims center | advancing integrated mental...
TRANSCRIPT

IMPACTImproving Mood –
Promoting Access to Collaborative Treatment for Late-Life Depression
Funded by
John A. Hartford Foundation, California HealthCare Foundation, Robert Wood Johnson Foundation,
Hogg Foundation
What is Depression?
Depression is NOT…Having -a ‘bad day’, -a ‘bad attitude’, -or ‘normal sadness’-Part of ‘normal aging’

Major Depression
Common: 5-10 % in primary care
Pervasive depressed mood / sadness and loss of interest/ pleasure …Plus: lack of energy, Fatigue, poor sleep and appetite, physical slowing or agitation, poor concentration, physical symptoms (aches and pains), thoughts of guilt, irritability and thoughts of suicide
If untreated, depression can last for years.
Often complicated by: chronic medical disorders, chronic pain, anxiety, cognitive impairment, grief/ bereavement, substance abuse

In late-life, depression israrely the only health problem
Depression
NeurologicalDisordersGeriatric
Syndromes
Diabetes
20-40%
10-20%
10-20%
Heart Disease20-40%
Chronic Pain
40-60%10-20%Cancer

Depression is expensive:Annual Health Costs in 1995 $
0
10002000
30004000
50006000
7000
0 (n=859)
1-2(n=616)
3-5 (n=659)
6-16(n=423)
Nodepression
Milddepression
Moderate toseveredepression
Unützer et al, JAMA, 1997
Chronic disease score
$

Depression is deadlyOlder adults have the highest rate of suicide.

Few Older Adults receive Effective Treatment
Depression CAN be treated, BUT…
-Only half of depressed older adults are ‘recognized’
-Older men, African Americans and Latinos have particularly low rates of depression treatment
-Fewer than 10% seek care from a mental health specialist. Most prefer treatment by their primary care physician
-Only one in five older adults treated for depression in primary care improve

One-Year Service Use by Depressed Adults
3%4%Inpatient Mental Health (MH)
1%4%ER visit for MH
8%25%Outpatient Mental Health
65 + (N = 113)
18-64(N = 1,382)
AGE GROUP
Primary care visit addressing
Mental Health Needs49%45%
9,585 adults from 60 US communities. Klap, Tschantz, Unützer. AJGP, 2003

Barriers to Effective Depression Care
“I didn’t know what hit me …”
Stigma of mental illness: “I am not crazy”
“Isn’t depression just a part of ‘normal aging’?”
“Of course I am depressed. Wouldn’t you be?”The ‘fallacy of good reasons’
Knowledge and Attitudes
Limited time and competing priorities: Limited follow-up -> early treatment dropoutStaying on ineffective treatments for too long
“I thought this was as good as I was going to get”Limited access to mental health experts
Challenges in Primary Care
IMPACT Study
1998 – 2003
1,801 depressed older adults in primary care
18 primary care clinics - 8 health care organizations in 5 states
Diverse health care systems (FFS, HMO, VA)450 primary care providers Urban and semi-rural settings Capitated and fee-for-service
Funded byJohn A. Hartford Foundation; California HealthCare Foundation; Robert Wood Johnson Foundation; Hogg Foundation
IMPACT Study TeamNone of us is as smart as all of us.
Study coordinating center
Study sitesUniversity of Washington / Group Health CooperativeWayne Katon (PI), Elizabeth Lin (Co-PI), Paul CiechanowskiDuke University Linda Harpole (PI), Eugene Oddone (Co-PI), David SteffensKaiser Permanente, Southern CA (La Mesa, CA)Richard Della Penna (Co-PI), Lydia Grypma (Co-PI), Mark Zweifach, MD, Rita Haverkamp, RN, MSN, CNSIndiana UniversityChristopher Callahan (PI), Kurt. Kroenke, Hugh. Hendrie (Co-PI)UT Health Sciences Center at San AntonioJohn Williams (PI), Polly Hitchcock-Noel (Co-PI), Jason WorchelKaiser Permanente, Northern CAEnid Hunkeler (PI), Patricia Arean (Co-PI)Desert Medical GroupMarc Hoffing (PI); Stuart Levine (Co-PI)
Study Advisory BoardLisa Goodale (NDMDA), Rick Birkel (NAMI), Thomas Oxman, Kenneth Wells, Cathy Sherbourne, Lisa Rubenstein, Howard Goldman
Jürgen Unützer (PI), Sabine Oishi, Diane Powers, Michael Schoenbaum, Tom Belin, Linqui Tang, Ian Cook. PST-PC experts: Patricia Arean, Mark Hegel

IMPACT Study Methods
Randomized control trial. 1,801 depressed older adults with major depression and / or dysthymia randomly assigned to IMPACT or Care as Usual
Primary care or referral to specialty mental health as available
Collaborative / stepped care disease management program for depression in primary care offered for up to 12 months
Independent assessments of health outcomes and costs for 24 months. Intent to treat analyses.
Unützer et al, Med Care 2001; 39(8):785-99
Design
Usual Care
IMPACT Care
Analyses

IMPACT Study Participants
42 %Antidepressant use in 3 months prior to study
12 %African American
35 %Cognitive impairment at screening
3.2Mean chronic medical diseases (out of 10)
53 %Major depression + dysthymia3 %All others8 %Latino
23 %Non-white71.2 (7.5)Mean age (SD)
65 %Female
N = 1,801*
* No significant baseline differences between intervention and usual care.

EffectiveCollaboration
Prepared, Pro-activePractice Team
Informed, ActivatedPatient
IMPACT Team Care Model
Practice Support
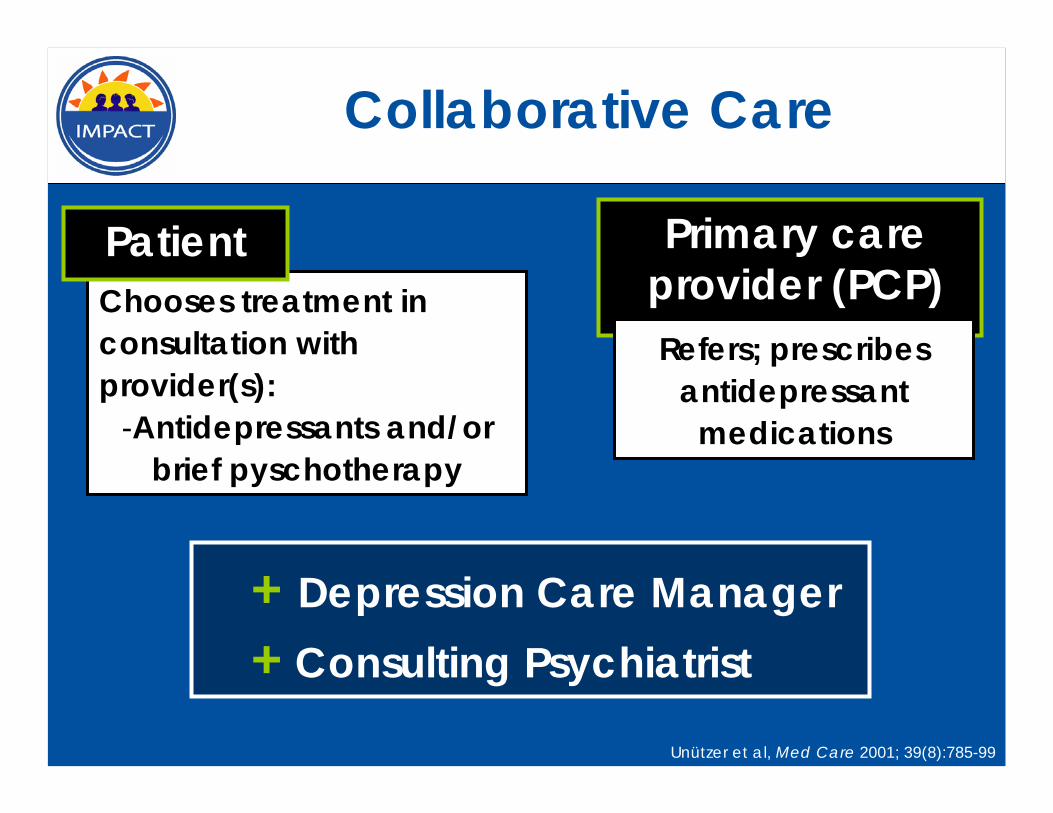
Collaborative Care
Primary care provider (PCP)Refers; prescribes
antidepressant medications
+ Depression Care Manager+ Consulting Psychiatrist
Unützer et al, Med Care 2001; 39(8):785-99
Chooses treatment in consultation with provider(s):
-Antidepressants and/or brief pyschotherapy
Patient

Evidence-based ‘team care’ for depression
- Consultation focused on patients not improving as expected
- Recommendations for additional treatment / referral according to evidence-based guidelines
- Support anti-depressant Rx by PCP
- Brief counseling (behavioral activation, PST-PC, CBT, IPT)
- Facilitate treatment change / referral to mental health
- Relapse prevention
2. Stepped Care
a) Change treatment according to evidence-based algorithm if patient is not improving
b) Relapse prevention once patient is improved
- Caseload consultation for care manager and PCP (population-based)
- Diagnostic consultation on difficult cases
-Patient education / self management support
-Close follow-up to make sure pts don’t ‘fall through the cracks’
1. Systematic diagnosis and outcomes tracking
e.g., PHQ-9 to facilitate diagnosis and track depression outcomes
Consulting Psychiatrist
Care Manager
TWO NEW ‘TEAM MEMBERS’Supporting the Primary Care Provider (PCP)TWO PROCESSES

Stepped Care
Insufficient responseChange treatment
• According to evidence-based algorithm• In consultation with team psychiatrist
Adjust treatment based on clinical outcomes
Systematic outcomes tracking
•Patient Health Questionnaire (PHQ-9)

Evidence-Based Depression Care Management
a.Case finding (screening, referral) -> confirm diagnosisb.Proactive follow-up & tracking (PHQ-9)
•Change treatment if patient not improving•Relapse prevention plan for patients in remission
a. Educationb. Brief Therapy: Behavioral Activation / Problem Solving
a. Primary Care (Antidepressant Medications)b. Specialty Mental Health Care / Psychotherapy
a. Caseload supervision / consultation for care managersb. Psychiatry consultation for treatment nonresponders
Identify and track depressed patients
Enhance patient self-management
Support additional treatment
Mental health consultation for difficult cases

Improved Satisfaction with Depression Care
020406080
100
0 3 12month
perc
ent
Usual Care Intervention
P<.0001 P<.0001
P=.2375
Unützer et al, JAMA 2002; 288:2836-2845
(% Excellent, Very Good)

Mean HSCL-20 Depression Severity Score
0.0
0.5
1.0
1.5
2.0
Baseline 3 6 12
Follow-up (Months)
P=.553
P<.0001P<.0001
Usual Care
Intervention
P<.0001
Unutzer, et al. JAMA 2002; 288:2836-2845
IMPACT: Doubles the Effectiveness of Usual Care for Depression

Findings Robust Across Diverse Health Care Organizations
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8
Usual Care IMPACT
%
Participating Organizations
TREATMENT RESPONSE50 % or greater improvement in depression at 12 months
Unutzer, et al. JAGS 2003; 51:505-514

Better Physical Function
38
38.5
39
39.5
40
40.5
41
41.5
Baseline 3 mos 6 mos 12 mos
Usual Care IMPACT
PCS-12
P<0.01
P<0.01P<0.01
P=0.35
Callahan et al, JAGS 2005; 53:367-373.

00.20.40.60.8
11.21.41.61.8
2
Baseline 3 6 12 18 * 24 *
months
Mea
n HS
CL-
20 D
epre
ssio
n Se
verit
y Sc
ore
IMPACT Usual Care
Effects persist even 1 year after the program ends
AFTER IMPACTIMPACT INTERVENTION
P=0.55
P<0.01P<0.01
P<0.01
Hunkeler et al, BMJ, 2006.
P<0.01 P<0.01

IMPACT
Usual Care
Additional Depression-Free Days
0
100
200
300
400
IMPACT in Diabetes116 more Depression-Free Days over 2 Years
381
265
116
Days
Katon et al, Diabetes Care; 2006
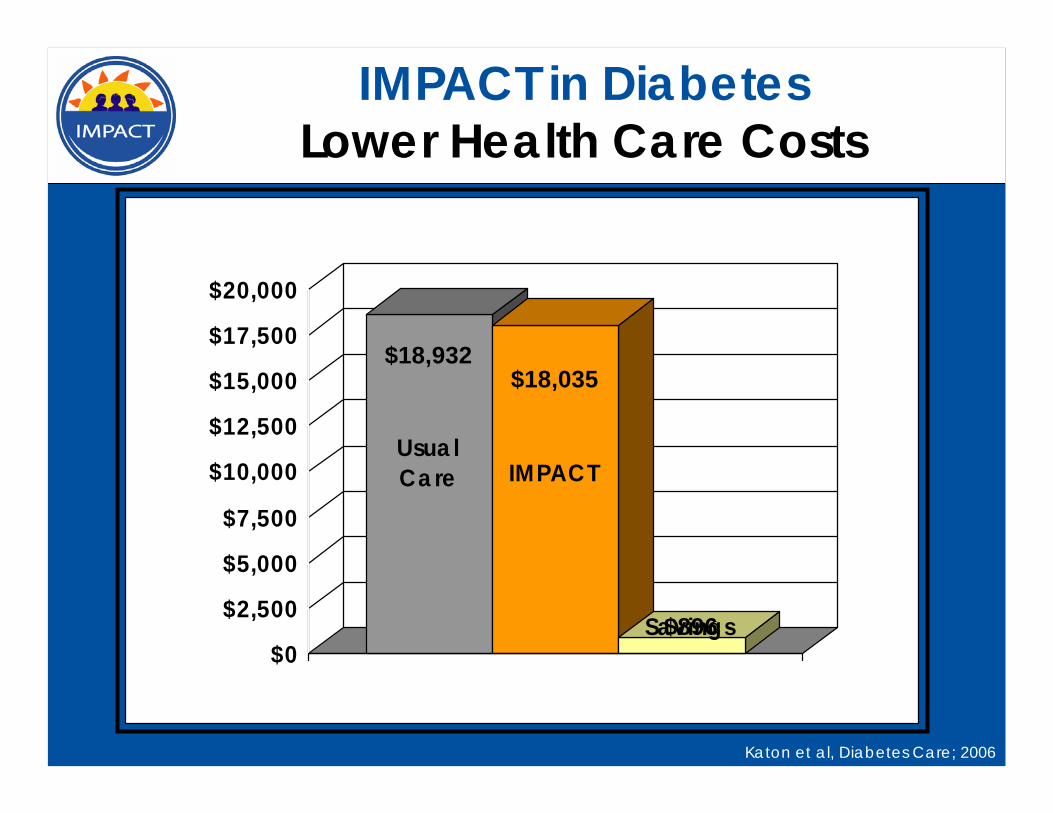
IMPACT in DiabetesLower Health Care Costs
Usual Care IMPACT
Savings$0
$2,500
$5,000
$7,500
$10,000
$12,500
$15,000
$17,500
$20,000
$896
Katon et al, Diabetes Care; 2006
$18,035$18,932
IMPACT Summary
Photo credit: J. Lott, Seattle Times
- Less depression(IMPACT doubles effectiveness of usual care)
- Less physical pain- Better functioning- Higher quality of life- Greater patient and
provider satisfaction- More cost-effective
“I got my life back”

Moving IMPACT from Research to PracticeJohn A. Hartford Foundation

Supported by a grant from the John A. Hartford Foundation.
IMPACT Disseminationhttp://impact-uw.org

IMPACT TrainingIn Person and on the Web
Trained over 1600 providers

The IMPACT Communityhttp://impact-uw.org