immunogenicity and safety of a pertussis vaccine composed of pertussis toxin inactivated by hydrogen...
TRANSCRIPT

Immunogenicity and safety of a pertussis vaccine composed of pertussis toxin inactivated by hydrogen peroxide, in J18- to 23-month-old children
Ingela Krantz, MD, Ronald Sekura, PhD, Birger Trollfors, MD, John Taranger, MD, Gunil la Zackrisson, MD, Teresa LagergOrd, PhD, Rachel Schneerson, MD, and John Robbins, MD
From the Departments of Infectious Diseases, Pediatrics, Clinical Bacteriology, and Medical Microbiology, University of GOteborg, GOteborg, Sweden; the Pediatric Outpatient Clinic, Vastra FrOlunda, Sweden; Amvax Inc., Laurel, Maryland; and the Laboratory of Developmen- tal and Molecular Immunity and Biometry Branch, National Institute of Child Health and Human Development, National Institutes of Health, Bethesda, Maryland
A new pertussis vaccine, composed of purif ied pertussis toxin inact ivated by hydrogen peroxide and adsorbed onto aluminum hydroxide (NICHD-Ptxd), was injected into 60 children aged 18 to 23 months without a history of pertussis or pertussis vaccinat ion. Two doses of toxoid, 10 and 50 ~g, were used. Two injec- tions, given 8 to 12 weeks apart, el ic i ted increases in serum levels of antitoxin and IgG antibodies in 56 children who had no detectab le antitoxin (<5 units) before vaccinat ion. Four children with detectab le anti toxin (~5 units) before the first vaccinat ion had pronounced ant ibody increases after the first dose. After the second dose, the geometr ic mean antitoxin concentrat ion was 29 units with the 50 ~g dosage and 10 units with the 10/~g dosage (p <0.001). Serum ant ibody levels el ic i ted by two injections of 50 ~g were similar to those in patients con- valescing from pertussis. A third injection given to seven children 9 to 10 months after the second injection gave a booster response, with high levels of antitoxin (160 to 1280 units) and of IgG antibodies. With few exceptions the ant ibody re- sponse was restricted to the IgG class. Transient local reactions >__2 cm in diam- eter occurred in 14% of the children after the first dose and in 44% after the sec- ond and third doses. Moderate fever was recorded after 6% of al l injections. There were no changes in peripheral b lood leukocyte counts or fasting b lood glucose levels measured before and 24 hours after the first injection. We con- c lude that NICHD-Ptxd is immunogenic in children. No serious adverse effects were noted. (J PEDIATR 1990,116:539-43)
Supported in part by the National Institute of Child Health and Human Development and by the Petter Silfverski61d Memorial Foundation. Submitted for publication July 18, 1989; accepted Oct. 11, 1989. Reprint requests: lngela Krantz, Mlb, Department of International Health Care Research, Karolinska Institutet, Box 60400,. 104 01 Stockholm, Sweden. 9/20/17335
Pertussis toxin, a protein produced by Bordetella pertussis, has an essential role in the pathogenesis and development of immunity to pertussis. 1 Previous names describe some of its biologic activities: lymphocytosis-promoting factor, his- tamine-sensitizing factor, and islet-activating protein. 1 In mice, actively induced or passively transferred serum toxin antibodies protect against infection with B. pertussis and
539

5 4 0 Krantz et al. The Journal of Pediatrics April 1990
ELISA FHA NICHD-Ptxd
Enzyme-linked immunosorbent assay Filamentous hemagglutinin Vaccine developed at National Institute of Child Health and Human Development, composed of pertussis toxin inactivated with hydrogen peroxide and adsorbed onto aluminum hydroxide
death.2, 3 In a double-blind, placebo-controlled clinical trial, two injections of a monocomponent vaccine, composed of formalin-treated pertussis toxin, induced protection, al- though not complete, against pertussis. 4-6 The toxoid used in that study showed some reversion to toxin during the course of the study. 6 Thus it seemed important to evaluate the protective role of irreversibly inactivated toxin with re- maining immunogenicity.
In a previous study, it was shown that pertussis toxin in- activated by hydrogen peroxide (NICHD-Ptxd) retained --<0.1% hemagglutination and adenosine diphosphate-ribo- syltransferase activity, <0.001% histamine-sensitizing and lymphocytosis-promoting activities, and <0.01% of the toxic activity on CHO (chinese hamster ovary) cells. 7 NICHD-Ptxd was highly immunogenic in adult volunteers, all of whom had been vaccinated in childhood with cellular vaccines and had low prevaccination levels of antibodies. 7
We now report a trial of primary vaccination with NICHD-Ptxd of children 18 to 23 months of age who had neither been vaccinated with whole cell vaccines nor expe- rienced clinical disease. (General vaccination against per- tussis was discontinued in Sweden in 1979. 8) The study was approved by the University of G6teborg Ethical Committee, the Drug Department of the Swedish Board of Health and Welfare, the National Institutes of Health (clinical proto- col 86-CH-92), and the U.S. Food and Drug Administra- tion (BB-IND-2329). Written informed consent was ob- tained from the parents of all participants.
M E T H O D S
Study design. Sixty-three healthy children, 18 to 23 months of age, with no known history of pertussis or previ- ous vaccination against pertussis, were recruited during visits to child health care centers in G6teborg, Sweden. All participants had received three injections of aluminum ad- sorbed diphtheria and tetanus toxoids and of inactivated polio vaccine during their first year of life. Almost all had received a combination measles-mumps-rubella vaccine at 18 months of age, at least 3 weeks before entering this trial. The children were given two injections of either 10 or 50 #g of NICHD-Ptxd (lot PTH-06) at intervals of 8 to 12 weeks. The first 30 children enrolled received the 10 #g dosage and the remaining 33 received the 50 #g dosage. All injections were given subcutaneously in the anterolateral part of the
thigh. Three children were excluded after symptoms of pertussis developed within 10 days after the first vaccina- tion; the children had been exposed to pertussis during the week before vaccination, but this was not known by the parents when the vaccine was given. Of the remaining 60 children (31 boys), 29 received 10 #g and 31 received 50 fzg of NICHD-Ptxd. Their mean age at the time of the first in- jection was 20.4 months (range 18 to 23 months). All chil- dren had been afebrile and without signs of infection for at least 1 week before the vaccinations were given. Three chil- dren from India or Sri Lanka had been adopted and had ar- rived in Sweden at the age of 6 to 9 months. It is possible that they had been vaccinated with whole cell pertussis vaccines in their countries of origin.
Venous (or in a few cases capillary) blood samples for se- rologic studies were obtained immediately before the first and second vaccinations and 6 to 8 weeks after the second. The serum sample before the second vaccination was omit- ted for nine children.
Four children who had received the 10 Izg dose and four who had received the 50 ~g dose were given a third injec- tion at the same dose 9.to 10 months after the second injec- tion. Venous blood samples were obtained immediately be- fore the injection and 4 to 6 weeks later. The parents of one child, who had received the 10 #g dosage, withdrew the child after the third injection, before the last blood sample had been collected, because of the child's fear of venous punc- ture.
Recording of side effects. All children returned in 24 hours after the first injection for inspection of the injection site. The parents were instructed to measure the child's temperature 6, 24, 48, and 72 hours after each injection and to inspect the injection site daily for 1 week. The results were recorded on a form, which the parents returned at the next visit, when they were also interviewed for any reactions that might have been related to the vaccination. All parents an- swered a mailed questionnaire concerning side effects, per- tussis-like symptoms, and exposure topertussis 8 to 12 months after the second vaccination. Blood glucose and pe- ripheral leukocyte count were measured immediately before and 24 hours after the first vaccination. The children fasted before these visits.
Vaccine. The standardization and clinical and immuno- logic properties of NICHD-Ptxd (lot PTH-06) in healthy adult volunteers has been described. 7
Antibody assays. Antibodies against pertussis toxin of the IgG, IgM, and IgA classes were measured by ELISA with pertussis toxin attached to fetuin-treated plates. 9 Sera were tested in duplicate in five fivefold dilutions. The antibody titer is expressed as the inverted highest serum dilution showing an extinction of 0.2 greater than the background value. Titers <20 for IgG and <100 for IgM and IgA were
Volume 116 Pertussis toxo id vaccine 5 4 1 Number 4
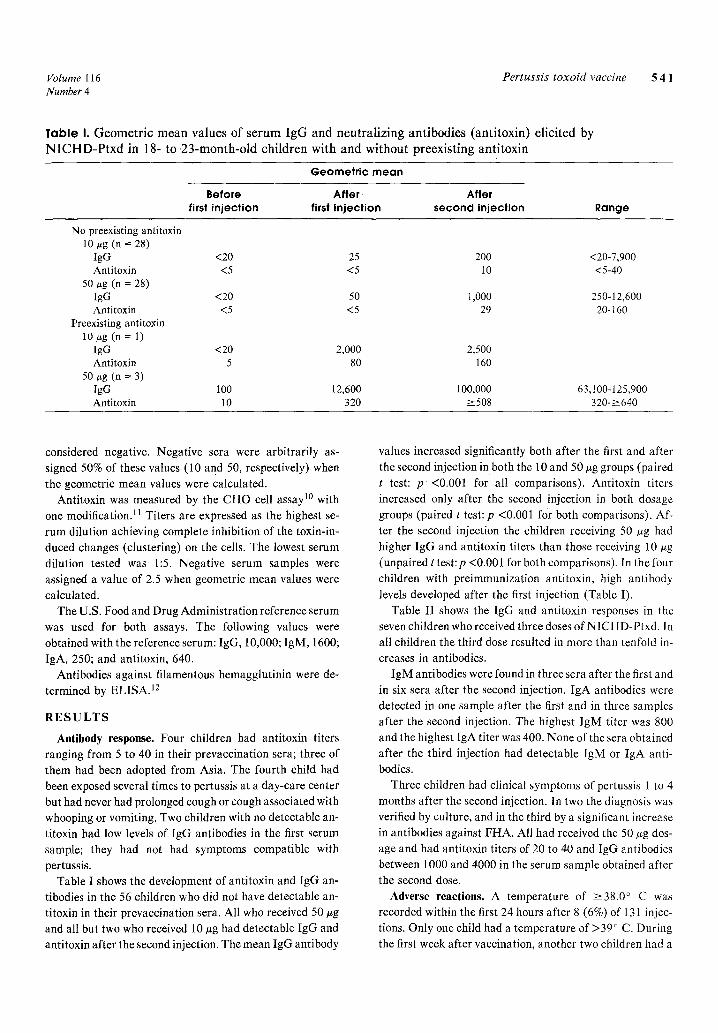
Table I. Geometr ic mean values of serum IgG and neutral iz ing antibodies (anti toxin) elicited by N I C H D - P t x d in 18- to .23-month-old children with and without preexisting anti toxin
Geometr ic m e a n
Before After After first injection first injection second injection Range
No preexisting antitoxin 10 #g (n = 28)
IgG <20 Antitoxin <5
50 ttg (n = 28) IgG <20 Antitoxin <5
Preexisting antitoxin 10 #g (n = 1)
IgG <20 Antitoxin 5
50 **g (n = 3) IgG 100 Antitoxin 10
25 200 <20-7,900 <5 10 <5-40
50 1,000 250-12,600 <5 29 20-160
2,000 2,500 80 160
12,600 100,000 63,100-125,900 320 >_508 320-~>640
considered negative. Negative sera were arbitrarily as- signed 50% of these values (10 and 50, respectively) when the geometric mean values were calculated.
Antitoxin was measured by the CHO cell assay l~ with
one modification, u Titers are expressed as the highest se- rum dilution achieving complete inhibition of the toxin-in- duced changes (clustering) on the cells. The lowest serum dilution tested was 1:5. Negative serum samples were assigned a value of 2.5 when geometric mean values were calculated.
The U.S. Food and Drug Administration reference serum was used for both assays. The following values were obtained with the reference serum: IgG, 10,000; IgM, 1600; IgA, 250; and antitoxin, 640.
Antibodies against filamentous hemagglutinin were de- termined by ELISA. 12
R E S U L T S
Antibody response. Four children had antitoxin titers ranging from 5 to 40 in their prevaceination sera; three of them had been adopted from Asia. The fourth child had been exposed several times to pertussis at a day-care center but had never had prolonged cough or cough associated with whooping or vomiting. Two children with no detectable an- titoxin had low levels of IgG antibodies in the first serum sample; they had not had symptoms compatible with
pertussis. Table I shows the development of antitoxin and IgG an-
tibodies in the 56 children who did not have detectable an- titoxin in their prevaccination sera. All who received 50 ug and all but two who received 10 #g had detectable IgG and antitoxin after the second injection. The mean IgG antibody
values increased significantly both after the first and after the second injection in both the 10 and 50 ~g groups (paired
t test: p <0.001 for all comparisons). Antitoxin titers increased only after the second injection in both dosage groups (paired t test: p <0.001 for both comparisons). Af- ter the second injection the children receiving 50 #g had higher IgG and antitoxin titers than those receiving 10 ug (unpaired t test:p <0.001 for both comparisons). In the four children with preimmunization antitoxin, high antibody
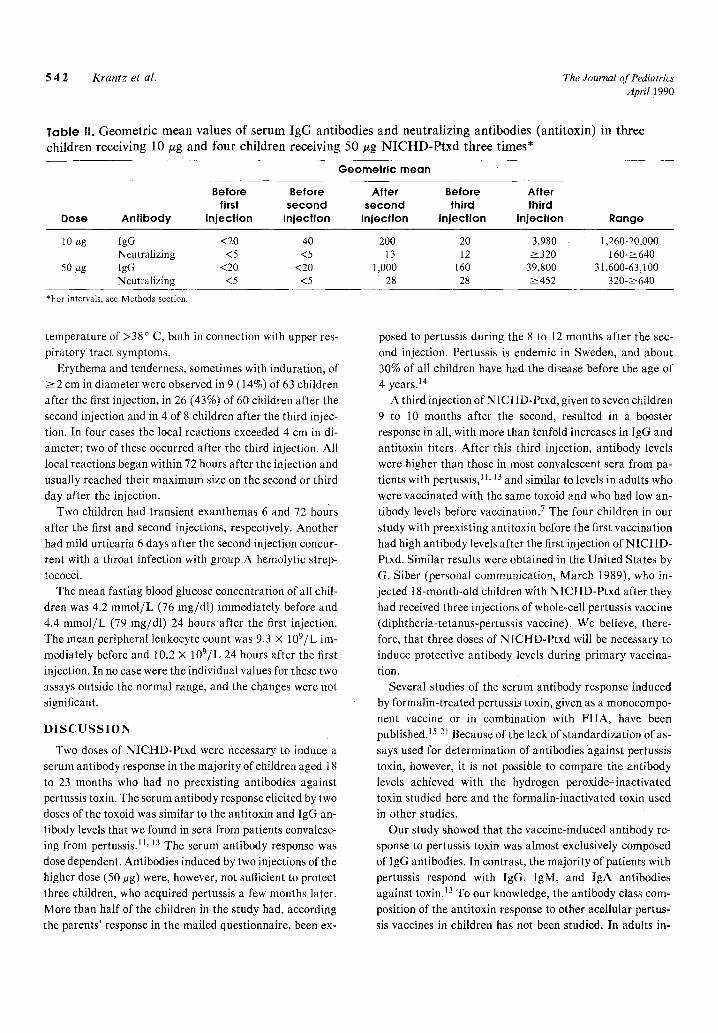
levels developed after the first injection (Table I). Table II shows the IgG and antitoxin responses in the
seven children who received three doses of NICHD-Ptxd. In all children the third dose resulted in more than tenfold in- creases in antibodies.
IgM antibodies were found in three sera after the first and in six sera after the second injection. IgA antibodies were detected in one sample after the first and in three samples after the second injection. The highest lgM titer was 800 and the highest IgA titer was 400. None of the sera obtained after the third injection had detectable IgM or IgA anti- bodies.
Three children had clinical symptoms of pertussis 1 to 4 months after the second injection. In two the diagnosis was verified by culture, and in the third by a significant increase in antibodies against FHA. All had received the 50 ug dos- age and had antitoxin titers of 20 to 40 and IgG antibodies between 1000 and 4000 in the serum sample obtained after the second dose.
Adverse reactions. A temperature of >--38.0 ~ C was recorded within the first 24 hours after 8 (6%) of 131 injec- tions. Only one child had a temperature of >39 ~ C. During the first week after vaccination, another two children had a
5 4 2 Krantz et al. The Journal of Pediatrics April 1990
Table li. Geometric mean values of serum IgG antibodies and neutral iz ing antibodies (anti toxin) in three children receiving 10 Izg and four children receiving 50 Izg N I C H D - P t x d three times*
Geometr ic mean
Before Before first second
injection injection Dose Ant ibody Range
After Before After second third third
injection injection injection
10 ~g lgG <20 40 200 20 3 , 9 8 0 1,260-20,000 Neutralizing <5 <5 13 12 >_320 160->~640
50 ~zg IgG <20 <20 1,000 160 39,800 31,600-63,100 Neutralizing <5 <5 28 28 >-452 320->--640
*For intervals, see Methods section.
temperature of >38 ~ C, both in connection with upper res- piratory tract symptoms.
Erythema and tenderness, sometimes with induration, of ~>2 cm in diameter were observed in 9 (14%) of 63 children after the first injection, in 26 (43%) of 60 children after the second injection and in 4 of 8 children after the third injec- tion. In four cases the local reactions exceeded 4 cm in di- ameter; two of these occurred after the third injection. All local reactions began within 72 hours after the injection and usually reached their maximum size on the second or third day after the injection.
Two children had transient exanthemas 6 and 72 hours after the first and second injections, respectively. Another had mild urticaria 6 days after the second injection concur- rent with a throat infection with group A hemolytic strep- tococci.
The mean fasting blood glucose concentration of all chil- dren was 4.2 mmol/L (76 mg/dl) immediately before and 4.4 mmol/L (79 mg/dl) 24 hours after the first injection. The mean peripheral leukocyte count was 9.3 x 109/L im- mediately before and 10.2 • 109/L 24 hours after the first
injection. In no case were the individual values for these two assays outside the normal range, and the changes were not significant.
D I S C U S S I O N
Two doses of NICHD-Ptxd were necessary to induce a serum antibody response in the majority of children aged 18 to 23 months who had no preexisting antibodies against pertussis toxin. The serum antibody response elicited by two doses of the toxoid was similar to the antitoxin and IgG an- tibody levels that we found in sera from patients convalesc- ing from pertussis. TM 13 The serum antibody response was
dose dependent. Antibodies induced by two injections of the higher dose (50 tsg) were, however, not sufficient to protect three children, who acquired pertussis a few months later. More than half of the children in the study had, according the parents' response in the mailed questionnaire, been ex-
posed to pertussis during the 8 to 12 months after the sec- ond injection. Pertussis is endemic in Sweden, and about 30% of all children have had the disease before the age of 4 years. )4
A third injection of N ICHD-Ptxd, given to seven children 9 to 10 months after the second, resulted in a booster response in all, with more than tenfold increases in IgG and antitoxin titers. After this third injection, antibody levels were higher than those in most convalescent sera from pa- tients with pertussis, TM 13 and similar to levels in adults who were vaccinated with the same toxoid and who had low an- tibody levels before vaccination] The four children in our study with preexisting antitoxin before the first vaccination had high antibody levels after the first injection of NICHD- Ptxd. Similar results were obtained in the United States by G. Siber (personal communication, March t989), who in- jected 18-month-old children with NICHD-Ptxd after they had received three injections of whole-cell pertussis vaccine (diphtheria-tetanus-pertussis vaccine). We believe, there- fore, that three doses of NICHD-Ptxd will be necessary to induce protective antibody levels during primary vaccina- tion.
Several studies of the serum antibody response induced by formalin-treated pertussis toxin, given as a monocompo- nent vaccine or in combination with FHA, have been published.15-2) Because of the lack of standardization of as- says used for determination of antibodies "against pertussis toxin, however, it is not possible to compare the antibody levels achieved with the hydrogen peroxide-inactivated toxin studied here and the formalin-inactivated toxin used in other studies.
Our study showed that the vaccine-induced antibody re- sponse to pertussis toxin was almost exclusively composed of lgG antibodies. In contrast, the majority of patients with pertussis respond with IgG, IgM, and IgA antibodies against toxin. ]3 To our knowledge, the antibody class com- position of the antitoxin response to other acellular pertus- sis vaccines in children has not been studied. In adults in-

Volume 116 Pertussis toxo id vaccine 5 4 3 Number 4
jected with formal in- t rea ted toxin, 68% responded with IgG
antibodies and 23% with IgG antibodies; no IgM response
was seen. 17
The incidence of fever and local reactions in adults
receiving the same vaccine was considerably lower than in
our children. 7 All children in our study had received three
doses of a luminum-adsorbed d iphther ia- te tanus toxoids
during the first year of life. Thus the N I C H D - P t x d injec-
tions were their fourth, fifth, and sixth doses of a luminum
adsorbed vaccines given within less than 3 years. A luminum
salt alone induces local reactions, and the reactivity in-
creases with the number of doses. 19 No late-occurring local
reactions, which have been described in adults receiving a
formalin- inact ivated acellular pertussis vaccine,17 were ob-
served in our children or in the adults receiving the same
vaccine. 7
We conclude tha t a monocomponent pertussis toxoid
vaccine, composed of hydrogen peroxide- inact ivated per-
tussis toxin, was immunogenic in children aged 18 to 23
months. T h r e e injections were necessary to achieve high
levels of ant i toxin and IgG antibodies. The ant ibody
response was almost exclusively restricted to the IgG class.
No serious side effects were observed.
We are grateful to Gunvor Lindel6f and Maja Berg for skilled technical assistance and to all the physicians and nurses who helped recruit study participants.
R E F E R E N C E S
1. Pittman M. The concept of pertussis as a toxin-mediated dis- ease. Pediatr Infect Dis 1984;3:467-86.
2. Sato Y, Izumiya K, Sato H, Cowell L, Manclark CR. Role of antibody to lcukocytosis-promoting factor hemagglutinin and to hemagglutinin in immunity to pertussis. Infect Immun 1981;31:1223-31.
3. Sato H, Sato Y. Bordetella pertussis infection in mice: Cor- relation of specific antibodies against two antigens, pertussis toxin, and hemagglutinin with mouse protectivity in an intra- cerebral or aerosol challenge system. Infect Immun 1984;46: 415-21.
4. Ad hoc Group for the Study of Pertussis Vaccines. Placebo- controlled trial of two aceltular pertussis vaccines in Sweden: protective efficacy and adverse events. Lancet 1988;1:955-60.
5. Olin P, Storsaeter J, Romanus V. The efficacy of acellular pertussis vaccine [Letter]. JAMA 1989;26:560.
6. Tiru M. Characterization of the acellular pertussis vaccines used in the Swedish clinical trial. In: A clinical trial of acellu- lar pertussis vaccines in Sweden. [technical report]. Stock- holm, Sweden: National Bacteriological Laboratory, 1988.
7. Sekura RD, Zhang Y, Roberson R, et al. Clinical, metabolic,
and antibody responses of adult volunteers to an investigational vaccine composed of pertussis toxin inactivated by hydrogen peroxide. J PEDIATR 1988;113:807-13.
8. Romanus V, Jonsell R, Bergquist S-O. Pertussis in Sweden af- ter the cessation of general immunization in 1979. Pediatr In- fect Dis J 1987;6:364-71.
9. Zackrisson G, Lagergftrd T, L6nnroth I. An enzyme-linked immunosorbent assay method for detection of immunoglobu- lins to pertussis toxin. Acta Pathol Microbiol Scand Sect C 1986;94:227-31.
10. Gillenius P, J~i/itmaa E, Askel6f P, Granstr6m M, Tiru M. The standardization of an assay for pertussis toxin and antitoxin in microplate culture of Chinese hamster ovary ceils. J Biol Standard 1985;13:61-6.
11. Trollfors B, Krantz l, Sigurs N, Taranger J, Zackrisson G, Roberson R. Toxin-neutralizing antibodies in patients with pertussis compared with antibodies determined by enzyme- linked immunosorbent assay. J Infect Dis 1988;158:991-5.
12. Zackrisson G, Arminjon F, Krantz I, et al. Serum antibody response to filamentous hemaggtutinin in patients with clinical pertussis measured by an enzyme-linked immunosorbent as- say. Eur J Clin Microbiol Infect Dis 1988;7:764-70.
13. Zackrisson G, Krantz I, Lagerg~ird T, et al. Antibody response to pertussis toxin in patients with clinical pertussis measured by enzyme-linked immunosorbent assay. Eur J Clin Microbiol Infect Dis 1988;7:149-54.
14. Krantz I, Taranger J, Trollfors B. Estimating incidence of whooping cough over time: a cross-sectional recall study of four Swedish birth cohorts. Int J Epidemiol 1989;18:901-5.
15. Pichichero RD, Badgett JT, Rodgers GC; et al. Acellular per- tussis vaccine: immunogenicity and safety of an aceltular per- tussis vs. a whole cell pertussis vaccine combined with diph- theria and tetanus toxoids as a booster in 18- to 24-month old children. Pediatr Infect Dis J 1987;6:352-63.
16. Lewis K, Cherry JD, Holroyd J, Baker LR, Dudenhoeffer FE, Robinson RG. A double-blind study comparing an acellular pertussis-component DTP vaccine with a whole-cell pertussis- component DTP vaccine in 18-month-old children. Am J Dis Child 1986;140:872-6.
17. Granstr6m M, Thor6n M, Blennow M, Tiru M, Sato Y. Acel- lular pertussis vaccine in adults: adverse reactions and immune response. Eur J Clin Microbiol 1987;6:18-21.
18. Anderson EL, Belshe RB, Bartram J, et al. Clinical and sero- logical responses to acellular pertussis vaccine in infants and young children. Am J Dis Child 1987;141:949-53.
19. Blennow M, Granstrfm M, J~i~itmaa E, Olin P. Primary im- munization of infants with an acellular pertussis vaccine in a double-blind randomized clinical trial. Pediatrics 1988;82: 293-9.
20. Hedenskog S, Granstr6m M, Olin P, Tiru M. A clinical trial of monocomponent pertussis toxoid vaccine. Am J Dis Child 1987;141:844-7.
21. Aoyama T, Hagiwara S, Murase Y, Kato T, Iwata T. Adverse reactions and antibody response to aceltular pertussis vaccine. J PEDIATR 1986;109:925-30,