immunodiagnostic assayfor helicobacterpyloni ...jcm.asm.org/content/32/1/46.full.pdf ·...
TRANSCRIPT

JOURNAL OF CLINICAL MICROBIOLOGY, Jan. 1994, p. 46-50 Vol. 32, No. 10095-1137/94/$04.00+0Copyright © 1994, American Society for Microbiology
Evaluation of a New Immunodiagnostic Assay forHelicobacter pyloni Antibody Detection: Correlation with
Histopathological and Microbiological ResultsALLAN D. PRONOVOST,l* STEVEN L. ROSE,1 JAN W. PAWLAK,1 HOWARD ROBIN,2
AND R. SCHNEIDER3Quidel Corporation, San Diego, California 921211; Department ofMedicine, Sharp Cabrilo Hospital,
San Diego, California 921232; and Byk-Gulden Phannazeutika, Konstanz, Gernnany3
Received 18 June 1993/Returned for modification 27 July 1993/Accepted 11 October 1993
Infection with Helicobacter pylori has been associated with the pathogenesis of chronic active gastritis andgastric and duodenal ulcer disease. Detection of immunoglobulin G antibodies to H. pylon offers a simplealternative to direct detection of the organism in biopsied tissue by culture or histopathological methods. Arapid flow-through membrane-based enzyme immunoassay for the detection of human immunoglobulin Gantibodies to H. pyloni has been developed and evaluated. Clinical evaluations were performed with 256 patientserum samples obtained from four clinical sites. Biopsy samples were obtained by endoscopic procedures at thesame time as the serum samples, and were histopathologically and microbiologically categorized for thepresence or absence of H. pyloni. Sensitivity and specificity for this rapid enzyme immunoassay were 92 and88%, respectively, compared directly with endoscopy results. After discordant results were resolved by aquantitative microwell enzyme-linked immunosorbent assay, the resulting sensitivity and specificity were 94and >99%, respectively. These results indicate that this rapid enzyme immunoassay is a useful technique todetermine H. pylori infection status and is a viable alternative to invasive endoscopic procedures.
Helicobacter pylon is a spiral-shaped microaerophilicgram-negative bacterium that is often observed in the mu-cous layer that coats the gastric mucosa (17). In recentyears, many reports have identified an association betweenthe presence of H. pylon and gastrointestinal symptoms andpathology, including gastritis and gastric and duodenal ul-cers (2, 3). Type B gastritis, particularly in the antrum of thestomach, is quite often associated with H. pylon coloniza-tion (24).The designation of pathologic status and the possibility of
H. pylon etiology are routinely established by invasiveendoscopic procedures. Biopsy specimens may be cultured,examined histopathologically, or tested for the presence ofin vitro urease activity (3, 21). Alternatively, 13C or 14Cbreath tests employing ingestion of [13CJurea or [14C]urea bythe patient followed by breath sample analysis for in situurease activity have also been described (14). Once H. pyloninfection is identified, treatment with specific antibiotics andbismuth compounds has been demonstrated to provide reliefand permit regeneration of the gastric tissues, presumablybecause H. pylon organisms were eliminated or populationswere greatly reduced in the intestinal tract (8, 13, 15).
Recently, an increasing number of studies have demon-strated that the presence of H. pylon-specific serum immu-noglobulin G (IgG) antibodies is strongly associated withgastrointestinal infection by these organisms (9, 12). Severalstudies have focused on the development of microtiterenzyme-linked immunosorbent assays (ELISAs) and corre-lation with endoscopic findings (10, 18, 25). In the presentstudy, patients with gastrointestinal complaints and healthyvolunteers underwent endoscopic examinations. Biopsysamples were taken during the procedure. The tissues were
* Corresponding author. Mailing address: Quidel Corporation,10165 McKellar Court, San Diego, CA 92121. Phone: (619) 552-1100.Fax: (619) 455-4840.
cultured and examined histologically for pathologic statusand for the presence of H. pylori organisms. Serum sampleswere taken at the same time as the endoscopy examinationsand were assayed for H. pylon-specific IgG antibodies by arapid membrane-based enzyme immunoassay (EIA) method.Results with the assay system demonstrated excellent cor-relation with standard histological and culture results.
MATERIALS AND METHODS
Patients. The present study was undertaken at gastroen-terology clinics at four sites: Los Angeles County/Universityof Southern California Hospital (Los Angeles, Calif.), SharpMemorial Hospital (San Diego, Calif.), the University ofVirginia Health Sciences Center (Charlottesville, Va.), andByk-Gulden Pharmazeutika (Konstanz, Germany). In-formed consent, in compliance with Institutional ReviewBoard requirements, was obtained from patients. Subjectsenrolled in the study were either patients with primarygastrointestinal complaints or asymptomatic individuals.Asymptomatic controls were healthy volunteers from SharpMemorial Hospital or the University of Southern CaliforniaHospital, who were recruited to participate for monetarycompensation. The Charlottesville, Va., and Konstanz, Ger-many, sites contributed only patients positive for H. pyloniby culture and histopathology. Approximately equal num-bers of patients were obtained from all sites with theexception of Charlottesville, which contributed less than10% of the positive samples. Potential subjects for eithergroup were excluded if they had received antibiotics orbismuth compounds within the previous 14 days. Initialdiagnoses were recorded, and serum samples were obtainedfrom all subjects at the time of endoscopy.
Endoscopy, histopathology, and culture. During the endos-copy procedures, all facilities obtained biopsy specimensfrom the antrum of the stomach. Portions of the biopsy were
46
on July 10, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NEW IMMUNODIAGNOSTIC ASSAY FOR HELICOBACTER PYLORI 47
fixed in formalin or placed in transport medium. Formalin-fixed specimens were stained with hematoxylin and eosin or
by other standard methods and examined for histopathologyand for the presence of curved bacilli characteristic of H.pylon. Histopathology results were run blindly by a pathol-ogist. For microbiological purposes, tissues were removedfrom the transport medium and plated onto chocolate agarplates. After 2 to 3 days, colonies were stained with Giemsaor Gram's stain and examined for the presence of typicalcurved bacilli (16).Two clinics, Virginia Health Sciences Center and Byk-
Gulden Pharmazeutika, also cultured biopsy specimens inthe CLOtest (Tri-Med Specialties; Overland Park, Kans.). Inthis test, urease produced by H. pylon acts upon the ureasubstrate in the culture chamber and the production ofNH4(is indicated by a color change. The Charlottesville siteincluded some patient samples positive for H. pylon by theI14C]urea breath test.
Assays. (i) Preparation of the antigen. H. pylon (ATCC43504) was grown in brucella broth supplemented with 10%(vol/vol) fetal calf serum. The cultures were grown at 35°Cunder controlled atmosphere on a rotary shaker, after whichcells were harvested and washed twice by centrifugation(19). The final cell pellet was resuspended in phosphate-buffered saline (PBS) containing 1% N-octyl-3-glucopyrano-side for 30 min at 25°C to release membrane proteins. Theextract was dialyzed overnight at 4°C against PBS and thenapplied to a 6FF-Sepharose resin (Pharmacia) equilibratedwith 50 mM Tris-HCl buffer (pH 8.0). After size exclusionchromatography, urease enzyme activity-free fractions witha molecular mass <200,000 kDa were pooled and frozen.This yielded antigen preparations enriched for H. pylonspecies-specific antigens. The process for purifying antigenswas optimized against a bank of known positive and negativeH. pylon sera to obtain the best performance in the rapidEIA before the clinical studies described herein were per-formed. This semipurified antigen material was subsequentlyutilized as the specific capture antigen (U.S. patent pending)in the membrane-based EIA. Other antigen preparationscited in the literature were evaluated by using a bank ofculture- and histopathology-confirmed positive and negativesera prior to developing the antigen preparation describedabove. These included acid glycine extracts (7), crude celllysates (26), high-molecular-weight urease preparations (6),and flagellar extracts (22), all of which were found uponinitial evaluation to exhibit poor sensitivity and specificityversus culture and histopathological results in the antibodyassay system under development.
(ii) Rapid membrane-based EIA. The QUIDEL QuickVueH. Pylori Test utilizes a flow-through membrane-based EIAprocedure to detect IgG antibody to H. pylon in humanserum and plasma. Thirty microliters of sample is mixedwith 150 pl of sample diluent containing PBS and proteinstabilizers and preservative (1:6 dilution). Diluted sample isadded to a flow-through test cartridge which contains a nylonmembrane coated with purified H. pylon antigen. The mem-branes are blocked with bovine serum albumin-PBS toprevent nonspecific human antibody absorption and thendried. As the patient's sample passes through the testcartridge membrane, H. pylon-specific antibody present inthe sample binds to the antigen on the membrane's surface.
Rabbit anti-human IgG conjugated to alkaline phosphataseis then added to the test cartridge membrane and allowed toflow through. IfH. pylon-specific IgG antibody is present onthe membrane, a complex forms with the enzyme-labeledrabbit anti-human IgG. The test cartridge membrane is then
rinsed with bufered wash solution in order to remove anyfree antibody-enzyme conjugate. Enzyme substrate is thenapplied to the test cartridge membrane and allowed todevelop for 5 mim at room temperature. At the end of the 5min, the test cartridge membrane is again rinsed with washsolution to stop the substrate reaction and the results of thetest are then determined visually. The enzyme substrate isspecific for the enzyme and will form a solid blue circle onthe membrane, indicating a positive result, when H. pylon-specific IgG antibody is present. If H. pylon-specific IgGantibody is not present in the patient's sample, a negativeresult will be indicated by a blue-negative bar. The blue-negative bar contains nonimmune human IgG deposited as abar pattern priar to antigen spotting (antigen is spotted in acircular pattern). This negative bar sign is also an indicatorthat the test reagents are working properly. If the test is notperformed correctly, no test result (no solid blue circle) andno negative bar will appear and the test must be repeated.
(iii) Confirmatory microtiter ELISA In the case of discrep-ant findings between the QUIDEL immunoassay and clinicalresults, a confirmatoxy microtiter ELISA was run to confirmthe presence or absence of H. pylon IgG antibody in thespecimen. T.he Biometra ELISA (Biometra, Gottingen, Ger-many) waS run in accordance with the manufacturer's rec-ommendations. Briefly, the serum sample was diluted 1:100with 100 ,ul of the diluted sample, added to antigen-coatedwells, and, incubated for 1 h. The plates were washed, and 2drops of enzyme conjugate were added to the appropriatewells and incubated for 1 h. The plates were again washed,and 2 drops of substrate reagent were added and incubatedfor 45 miii. The reaction was stopped, and the color was readat 492 nm. Standards were also included in this test. Allincubations were at room temperature.An H. pylon microwell ELISA developed at QUIDEL
was also used as a confirmatory tool to detect H. pylon-specific IgG. For this assay, the same semipurified H. pylonantigens as used in the rapid membrane-based EIA wereadsorbed to microwell strips and then blocked. Test sampleswere diluted 1:101 and added to the wells along with predi-luted serum standards and controls. During the first 30-minroom temperature incubation period, antibodies specific forH. pylon in the specimens and/or serum standards bound tothe immobilized H. pylon antigens. After washing of thewells to remove unbound antibodies, enzyme-conjugatedantibodies specific for human IgG [F(ab')2 fragment rabbitanti-human IgG and Fc fragment specific] were added toeach test well and allowed to react with the antigen-antibodycomplexes for 30 min at room temperature. Unbound en-zyme antibodies were washed out of the wells, and achromogenic substrate was incubated for 15 min at roomtemperature. An acidic stop solution was added, and theA405 was read. The intensity of the green color formed wasproportional to the number ofH. pylon-specific antibodies ineach well. A standard curve of A405 values versus antibodyunits per milliliter of standard was established. Specimenswhich gave antibody unit-per-milliliter values greater than orequal to 35 were considered positive. Any specimen result of25 to 34 antibody U/ml, inclusive, was considered equivocal.Any specimen result of less than or equal to 24 antibodyU/ml was considered negative.
RESULTS
Study population. Serum and/or plasma samples from atotal of 256 patients presenting with symptoms or healthyvolunteers without symptoms were examined by endo-
VOL. 32, 1994
on July 10, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
48 PRONOVOST ET AL.
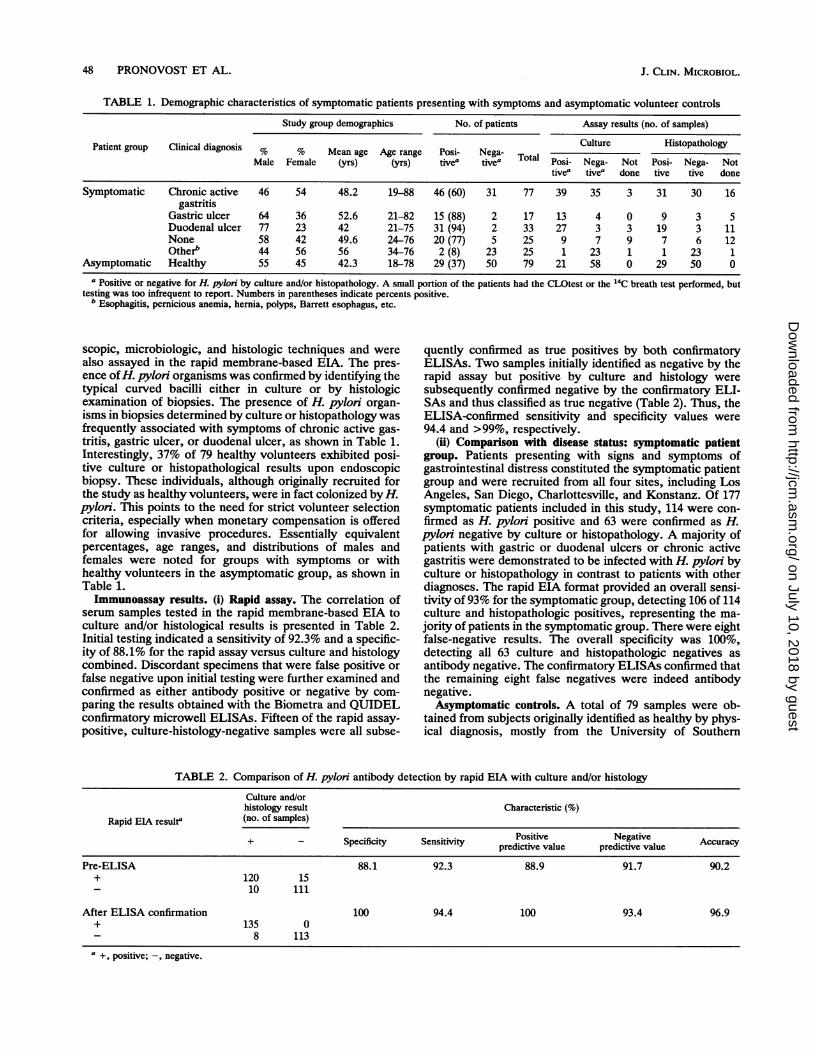
TABLE 1. Demographic characteristics of symptomatic patients presenting with symptoms and asymptomatic volunteer controls
Study group demographics No. of patients Assay results (no. of samples)
Patient group Clinical diagnosis % 9 Mean a Age rane Posi- N Culture Histopathologyo ea g Age age Poi ega-Toa PsiNMale Female (yrs) yrs) tivea tivea ° Posi- Nega- Not Posi- Nega- Not
tivea tivea done tive tive done
Symptomatic Chronic active 46 54 48.2 19-88 46 (60) 31 77 39 35 3 31 30 16gastritis
Gastric ulcer 64 36 52.6 21-82 15 (88) 2 17 13 4 0 9 3 5Duodenal ulcer 77 23 42 21-75 31 (94) 2 33 27 3 3 19 3 11None 58 42 49.6 24-76 20 (77) 5 25 9 7 9 7 6 12Otherb 44 56 56 34-76 2 (8) 23 25 1 23 1 1 23 1
Asymptomatic Healthy 55 45 42.3 18-78 29 (37) 50 79 21 58 0 29 50 0a Positive or negative for H. pylon by culture and/or histopathology. A small portion of the patients had the CLOtest or the 14C breath test performed, but
testing was too infrequent to report. Numbers in parentheses indicate percents positive.b Esophagitis, pernicious anemia, hernia, polyps, Barrett esophagus, etc.
scopic, microbiologic, and histologic techniques and werealso assayed in the rapid membrane-based EIA. The pres-ence ofH. pylori organisms was confirmed by identifying thetypical curved bacilli either in culture or by histologicexamination of biopsies. The presence of H. pylon organ-isms in biopsies determined by culture or histopathology wasfrequently associated with symptoms of chronic active gas-tritis, gastric ulcer, or duodenal ulcer, as shown in Table 1.Interestingly, 37% of 79 healthy volunteers exhibited posi-tive culture or histopathological results upon endoscopicbiopsy. These individuals, although originally recruited forthe study as healthy volunteers, were in fact colonized by H.pylon. This points to the need for strict volunteer selectioncriteria, especially when monetary compensation is offeredfor allowing invasive procedures. Essentially equivalentpercentages, age ranges, and distributions of males andfemales were noted for groups with symptoms or withhealthy volunteers in the asymptomatic group, as shown inTable 1.Immunoassay results. (i) Rapid assay. The correlation of
serum samples tested in the rapid membrane-based EIA toculture and/or histological results is presented in Table 2.Initial testing indicated a sensitivity of 92.3% and a specific-ity of 88.1% for the rapid assay versus culture and histologycombined. Discordant specimens that were false positive orfalse negative upon initial testing were further examined andconfirmed as either antibody positive or negative by com-paring the results obtained with the Biometra and QUIDELconfirmatory microwell ELISAs. Fifteen of the rapid assay-positive, culture-histology-negative samples were all subse-
quently confirmed as true positives by both confirmatoryELISAs. Two samples initially identified as negative by therapid assay but positive by culture and histology weresubsequently confirmed negative by the confirmatory ELI-SAs and thus classified as true negative (Table 2). Thus, theELISA-confirmed sensitivity and specificity values were94.4 and >99%, respectively.
(ii) Comparison with disease status: symptomatic patientgroup. Patients presenting with signs and symptoms ofgastrointestinal distress constituted the symptomatic patientgroup and were recruited from all four sites, including LosAngeles, San Diego, Charlottesville, and Konstanz. Of 177symptomatic patients included in this study, 114 were con-firmed as H. pylon positive and 63 were confirmed as H.pylori negative by culture or histopathology. A majority ofpatients with gastric or duodenal ulcers or chronic activegastritis were demonstrated to be infected with H. pyloni byculture or histopathology in contrast to patients with otherdiagnoses. The rapid EIA format provided an overall sensi-tivity of 93% for the symptomatic group, detecting 106 of 114culture and histopathologic positives, representing the ma-jority of patients in the symptomatic group. There were eightfalse-negative results. The overall specificity was 100%,
detecting all 63 culture and histopathologic negatives asantibody negative. The confirmatory ELISAs confirmed thatthe remaining eight false negatives were indeed antibodynegative.Asymptomatic controls. A total of 79 samples were ob-
tained from subjects originally identified as healthy by phys-ical diagnosis, mostly from the University of Southern
TABLE 2. Comparison of H. pylori antibody detection by rapid EIA with culture and/or histologyCulture and/orhistology result Characteristic (%)
Rapid EIA resulta (no. of samples)
+ - Specificity Sensitivity Positive Negative Accuracypredictive value predictive value
Pre-ELISA 88.1 92.3 88.9 91.7 90.2+ 120 15
10 111
After ELISA confirmation 100 94.4 100 93.4 96.9+ 135 0
8 113a +, positive; -, negative.
J. CLIN. MICROBIOL.
on July 10, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NEW IMMUNODIAGNOSTIC ASSAY FOR HELICOBACTER PYLORI 49
California Hospital. Subsequent histopathology confirmedthat 29 of these subjects (36.7%) actually had gastric pathol-ogy. Twenty-one of the 29 histopathologically positiveasymptomatic individuals were also microbiologically posi-tive for H. pylon. By the rapid EIA and the confirmatoryELISA, all 29 individuals were defined as antibody positivefor H. pylon. For this asymptomatic population, both thesensitivity and specificity for the rapid EIA were >99%.
DISCUSSION
The association between the presence of H. pylon andgastrointestinal signs, symptoms, and pathology and theiralleviation by specific antimicrobial and/or bismuth saltstherapy has been increasingly reported (2). The chief imped-iment to the diagnosis of infection has been the necessity forinvasive protocols and the lack of availability of rapid andaccurate diagnostic tools. Traditionally, the diagnosis of H.pylon infection has been accomplished by culture and/orhistology of gastrointestinal specimens obtained by invasiveendoscopic biopsy procedures. Tissue sections may be in-adequate for diagnosis because of the possible focal natureof the infection and the problem of inadequate specimencollection (20). Additionally, growth of the organisms isdifficult, and recent evidence indicates that at best only 71%of H. pylon strains will grow in a specific medium (1). Forbest results, several selective media with various antibioticsupplements in addition to at least one nonselective mediumwould be required to provide the highest culture recoveryrates.The presence of specific H. pylon-directed IgG antibodies
has shown excellent correlation with the presence of H.pylon enteric infection (7). In our studies, we have shownthat the sensitivity and specificity of a rapid membrane-based EIA correlate well with the presence of H. pyloninfection. The rapid assay detects antibody-positive patientswho may not be culture or histopathology positive uponbiopsy. This may indicate prior infection or a falsely positiveresult for the antibody assay. The incidence of H. pylonantibody seroconversion increases with age in the popula-tion as exposure increases, but this does not necessarilyalways relate to peptic ulcer disease (11). The rapid EIAcould provide the opportunity for testing patients during anoffice visit, or the test could be used to confirm endoscopicfindings, especially if a biopsy was not taken for culture orhistopathology. The advent of more specific tests correlatingwith active infection, either through the use of better purifiedspecies-specific antigens or recombinant antigens or throughthe detection of specific immunoglobulin responses (e.g., forIgA or IgM), may show promise and allow them to be useddirectly for screening or diagnostic purposes and not just asconfirmatory tools.
In our assays, a high correlation of infection was noted inconjunction with the specific diagnostic disorders of gastricand duodenal ulcers. This observation has been publishedpreviously (23). In patients with diagnosable chronic activegastritis, 60% were subsequently found to be infected withH. pylon. This may be the target group for whom rapiddiagnostic assays would prove most beneficial. For a patientpresenting with gastric symptoms, including nonulcerativedyspepsia, a positive H. pylon serology would suggest theneed for further testing with appropriate therapy. Thissuggestion would be warranted on the basis of the demon-strated high specificity of the assays.
In this study, 37% of the asymptomatic control group werefound to have demonstrable subclinical gastritis. Con-
versely, in the histopathologically normal population, only14% of the individuals were confirmed as H. pylon positive.Again, these rates are similar to those reported previously(4).The epidemiology of this infection remains unclear. Early
studies indicated that intrafamilial transmission was poten-tially operative (5). Thus, if one symptomatic family memberis diagnosed as H. pylon positive, testing of other familymembers may be indicated. If they test positive, treatment toeradicate family reservoirs may be indicated. Again, becauseof the high specificity of these assays, treatment of unin-fected individuals would be very limited.
In summary, the high positive correlation of the ETAresults with determination of H. pylon infection by endo-scopic procedures demonstrates the utility of this test as analternative to invasive procedures.
ACKNOWLEDGMENTS
We are grateful for the excellent technical contributions of E.Fox, R. Eisenger, P. Morrow, P. W. Wang, C. P. Dooley, K.Condon, L. Cragle, and J. Shinkai-Langit. We thank Barry Marshalland Irving Nachamkin for materials generously provided for thesestudies.
REFERENCES1. Ansorg, R. G., G. Von Recklinghausen, R. Pomarius, and E. N.
Schmid. 1991. Evaluation of techniques for isolation, subculti-vation, and preservation of Helicobacterpylori. J. Clin. Micro-biol. 29:51-53.
2. Beftits, R., M. Granstrom, M. Rylander, and C. Rubio. 1993.Helicobacter pylon in 205 consecutive endoscopy patients.Scand. J. Infect. Dis. 25:185-191.
3. Brown, K. E., and D. A. Peura. 1993. Diagnosis of Helicobacterpylon infection. Gastroenterol. Clin. N. Am. 22:105-115.
4. Dooley, C. P., P. L. Fitzgibbons, H. Cohen, M. Appleman, M.Bauer, G. I. Perez-Perez, and M. J. Blaser. 1989. Prevalence ofHelicobacterpyloni infection and histologic gastritis in asymp-tomatic persons. N. Engl. J. Med. 321:1562-1566.
5. Drumm, B., G. I. Perez-Perez, M. J. Blaser, and P. Sherman.1990. Intrafamilial clustering of Helicobacter pylon infection.N. Engl. J. Med. 322:359-363.
6. Evans, D. G., D. J. Evans, and D. Y. Graham. November 1989.U.S. patent 4,882,271.
7. Goodwin, C. S., E. Blincow, G. Peterson, C. Sanderson, W.Cheng, B. Marshall, J. R. Warren, and R. McCulloch. 1987.Enzyme-linked immunosorbent assay for Campylobacter py-loridis: correlation with presence of C. pyloridis in the gastricmucosa. J. Infect. Dis. 155:488-494.
8. Graham, D. Y., G. M. Lew, H. M. Malaty, D. G. Evans, D. J.Evans, Jr., P. D. Klein, L. C. Alper, and R. M. Genta. 1992.Factors influencing the eradication of Helicobacter pylori withtriple therapy. Gastroenterology 102:493-496.
9. Hirschl, A. M., G. Brandstatter, B. Dragosics, E. Hentschel, M.Kundi, M. L. Rotter, K. Schutze, and M. Taufer. 1993. Kineticsof specific IgG antibodies for monitoring the effect of anti-Helicobacterpylori chemotherapy. J. Infect. Dis. 168:763-766.
10. Hoek, F. J., A. Noach, E. A. J. Rauws, and G. N. J. Tytgat. 1992.Evaluation of the performance of commercial test kits fordetection of Helicobacter pylon antibodies in serum. J. Clin.Microbiol. 30:1525-1528.
11. Jones, D. M., J. Eldridge, A. J. Fox, P. Sethe, and P. J.Whorwell. 1986. Antibody to the gastric campylobacter-likeorganism (Campylobacter pylonidis): clinical correlations anddistribution in the normal population. J. Med. Microbiol. 22:57-62.
12. Kosunen, T. U., K. Seppala, S. Sarna, and P. Sipponen. 1992.Diagnostic value of decreasing IgG, IgA and IgM antibody titresafter eradication of Helicobacter pylori. Lancet 339:893-895.
13. Labenz, J., E. Gyenes, G. H. Ruhl, and G. Borsch. 1993.Omeprazole plus amoxicillin: efficacy of various treatment
VOL. 32, 1994
on July 10, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

50 PRONOVOST ET AL.
regimens to eradicate Helicobacter pylori. Am. J. Gastroen-terol. 88:491-495.
14. Lin, S. K., J. R. Lambert, M. Schembri, L. Nicholson, M.Finlay, C. Wong, and A. Coulepis. 1992. A comparison ofdiagnostic tests to determine Helicobacter pylori infection. J.Gastroenterol. Hepatol. 7:203-209.
15. Logan, R. P., P. A. Gummett, J. J. Misiewicz, Q. N. Karim,M. M. Walker, and J. H. Baron. 1993. Two week eradicationregimen for metronidazole-resistant Helicobacter pylori. Ali-ment. Pharmacol. Ther. 7:149-153.
16. Marshall, B. J., D. B. McGechie, P. A. Rogers, and R. G.Glancy. 1985. Pyloric Campylobacter infection and gastroduo-denal disease. Med. J. Aust. 142:439--444.
17. McGuigan, J. E. 1978. Peptic ulcer and gastritis, p. 1229-1248.In J. D. Wilson, et al. (ed.), Harrison's principles of internalmedicine, 12th ed. McGraw-Hill, New York.
18. Megraud, F., M.-P. Brassens-Rabbe, F. Denis, A. Belbouri, andD. Q. Hoa. 1989. Seroepidemiology of Campylobacter pyloriinfection in various populations. J. Clin. Microbiol. 27:1870-1873.
19. Morgan, D. R., R. Freedman, C. E. Depew, and W. G. Kraft.1987. Growth of Campylobacter pylori in liquid media. J. Clin.Microbiol. 25:2123-2125.
20. Morris, A., G. Nicholson, G. Lloyd, D. Haines, A. Rogers, and D.Taylor. 1986. Seroepidemiology of Campylobacter pyloridis.N. Z. Med. J. 99:657-659.
21. Ng, T. M., K. M. Fock, J. Ho, A. L. Tan, S. C. Chia, C. K. Yap,C. N. Chew, and E. N. Chee. 1992. Clotest (rapid urease test) inthe diagnosis of Helicobacterpyloni infection. Singapore Med.J. 33:568-569.
22. Perez-Perez, G. I., B. M. Dworldn, J. E. Chodos, and M. J.Blaser. 1988. Campylobacterpylori antibodies in humans. Ann.Intern. Med. 109:11-17.
23. Rathbone, B. J., J. I. Wyatt, and R. V. Heatley. 1988. Incidenceof Campylobacter pylori in patients with gastritis and pepticulcer disease in various countries, p. 95-102. In H. Menge, M.Gregor, G. N. J. Tytgat, and B. J. Marshall (ed.), Campylobac-terpylori. Springer-Verlag, New York.
24. Rugge, M., F. Di Mario, M. Cassaro, R. Baffa, F. Farinati, J.Rubio, Jr., and V. Ninfo. 1993. Pathology of the gastric antrumand body associated with Helicobacter pylori infection in non-ulcerous patients: is the bacterium a promoter of intestinalmetaplasia? Histopathology (Oxford) 22:9-15.
25. Talley, N. J., L. Kost, A. Haddad, and A. R. Zinsmeister. 1992.Comparison of commercial serological tests for detection ofHelicobacter pylori antibodies. J. Clin. Microbiol. 30:3146-3150.
26. Von Wullfen, H. 1988. Systemic immune responses to Campy-lobacter pylori colonization, p. 157-163. In H. Menge, M.Gregor, G. N. J. Tytgat, and B. J. Marshall (ed.), Campylobac-terpylon. Springer-Verlag, New York.
J. CLIN. MICROBIOL.
on July 10, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from