immunisation update september 2014 dr karen lake screening and immunisation team phe
TRANSCRIPT

Immunisation UpdateSeptember 2014
Dr Karen LakeScreening and Immunisation TeamPHE
Contents• Aim and Learning objectives
• Aim of immunisation programmes
• Objectives of surveillance
• COVER and Immform data
• National schedule and updates
• Influenza and child flu pilot
• Cold Chain
• Contacts/resources
2 Immunisations
Aim
• To increase knowledge and awareness of immunisation programmes and recent changes in schedule
• To increase knowledge and awareness of vaccine surveillance and data
• Support health care practitioners involved in discussing immunisation by providing evidence base information
• Promote high uptake of immunisation by increasing knowledge and awareness
3 Immunisations

Learning Objectives• Describe how immunisation programmes are monitored
through the use of surveillance, the COVER programme and Immform
• Describe the current UK vaccine schedule including selective vaccination and new programmes and deal with variations to the schedule
• Describe the Influenza vaccine campaign for 2014/5
• Define how to maintain the Vaccine Cold Chain
• Identify sources of information
4 Immunisations
Aim of Immunisation programmes
5 Immunisations

Public health• The two public health interventions with
the greatest impact are clean water and vaccination
• Vaccination is the most effective medical intervention in the world
6 Immunisations
Aim of Immunisation Programmes
Need to decide overall aim:
• To protect those at highest risk
(selective immunisation strategy)
or
• To eradicate, eliminate or contain disease
(mass immunisation strategy)
7 Immunisations

Selective vaccinationSometimes vaccines do not need to be given to all, only to those at increased
risk of disease:
• Travel
e.g. Japanese B encephalitis
• Outbreak control
e.g. Hepatitis A
• High risk groups
e.g. Hepatitis B for neonates
• Occupational risk Outbreak control
e.g. Anthrax
8 Immunisations
Mass vaccination
Either:
• EradicationDisease and its causal agent have been removed worldwide e.g. smallpox
• Elimination
Disease has disappeared from one WHO Region but remains elsewhere e.g. polio
• Containment
The point at which the disease no longer constitutes a ‘significant public health problem’ e.g. Hib
9 Immunisations

Health Professionals role…..
10 Immunisations
• You are a vital part of the world wide delivery of one of the most important public health interventions
• You are the front line• You ensure protection for children, some of
which will last them throughout their lives• You continue to protect young people as they
travel and take up an occupation• You protect those who are vulnerable as they
are unable to have, or respond to immunisations
Objective of Surveillance
11 Immunisations

Objectives of Surveillance• Surveillance needs to be carried out both before and
after a vaccine programme is introduced:
• Pre-implementation of vaccine
To estimate burden of disease
To decide vaccination strategy
• Post implementation of vaccine
To monitor effectiveness of vaccine strategy
12 Immunisations
Surveillance for Vaccine Programmes Disease incidence
•Reports of disease from a variety of sources are collated by the Centre for Infections (CfI)
Susceptibility
•Residual blood samples used for serological surveillance
Vaccine Coverage
•Vaccine uptake monitored across the country, collated by CfI from local Child Health Computers
Monitoring adverse events and vaccine safety
•Collated by Medicines and Healthcare products Regulatory Agency (MHRA) Yellow Card scheme
•Investigated by CfI and immunisation experts worldwide
13 Immunisations
Disease incidence
14 Immunisations
Main sources of data:- Statutory notification-Laboratory reporting-Death notification
Other sources- Hospital episodes- Sentinel physician reporting- Paediatric surveillance
COVER and Immform
15 Immunisations

Vaccination CoverageCOVER (Cover of Vaccination Evaluated Rapidly)• It is important to know what proportion of any targeted population
has received each vaccine
• Since 1988 computerised child health systems across the country have held vaccination details for all children resident in the area
• Every 3 months, information collected by CfI from each child health computer as to number of children who have completed scheduled vaccine courses at 1, 2 & 5y of age
• This information used to evaluate and improve immunisation coverage by regular feedback to local areas
16 Immunisations

COVER (cont)Additionally, COVER data can be used to:
• detect change rapidly and monitor trends in uptake
• provide information on impact of media stories
• look for pockets of poor coverage
• estimate vaccine efficacy
• measure impact and success of a vaccination campaign
• It is thus vital than anyone who gives an immunisation, records and reports that immunisation to the child’s local Child Health System [CHIS]
17 Immunisations
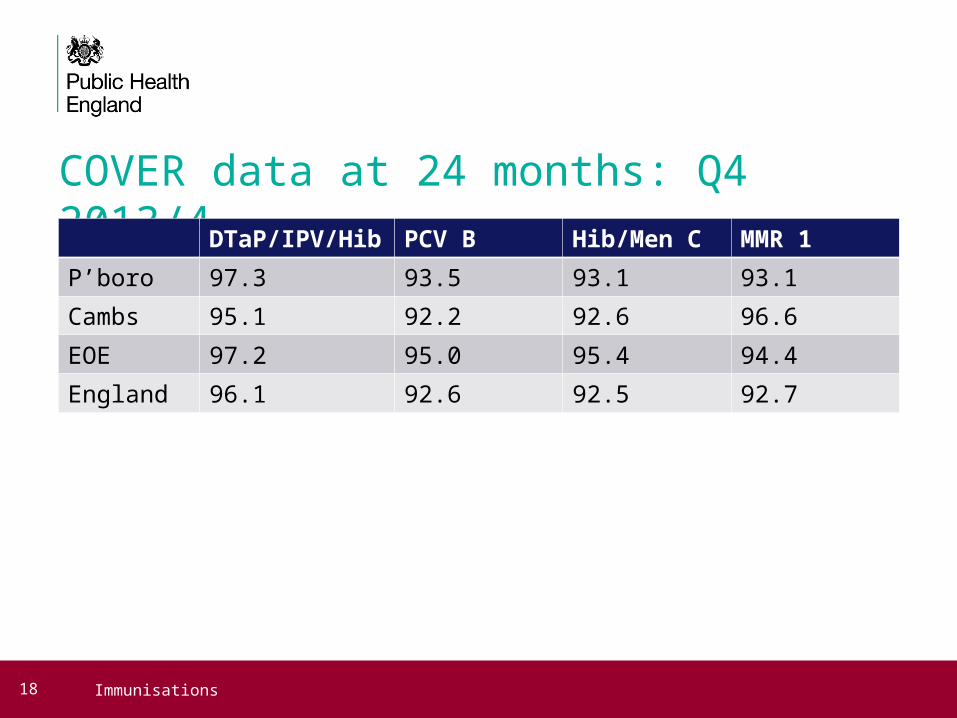
COVER data at 24 months: Q4 2013/4
18 Immunisations
DTaP/IPV/Hib PCV B Hib/Men C MMR 1
P’boro 97.3 93.5 93.1 93.1
Cambs 95.1 92.2 92.6 96.6
EOE 97.2 95.0 95.4 94.4
England 96.1 92.6 92.5 92.7
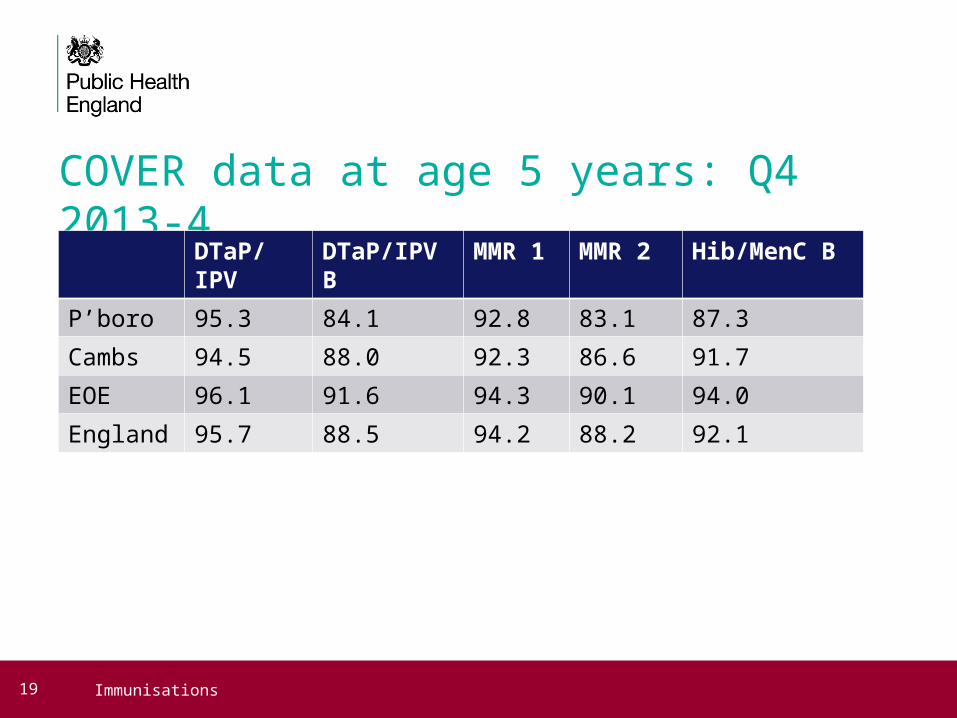
COVER data at age 5 years: Q4 2013-4
DTaP/IPV DTaP/IPV B MMR 1 MMR 2 Hib/MenC B
P’boro 95.3 84.1 92.8 83.1 87.3
Cambs 94.5 88.0 92.3 86.6 91.7
EOE 96.1 91.6 94.3 90.1 94.0
England 95.7 88.5 94.2 88.2 92.1
19 Immunisations

MMR 2 at 5 yrs
20 Immunisations
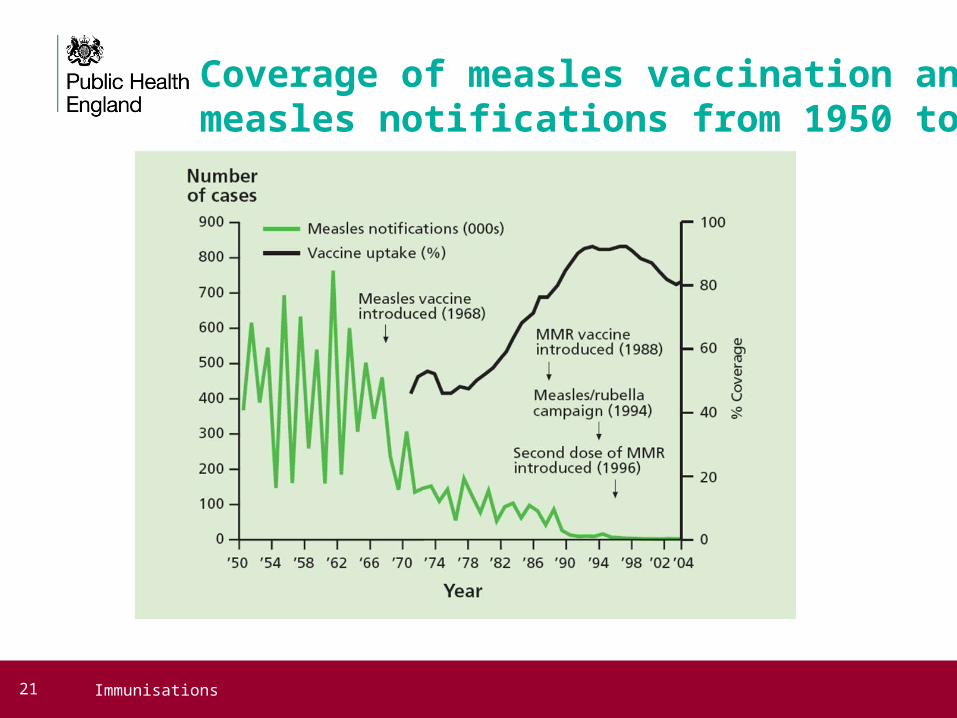
Coverage of measles vaccination and measles notifications from 1950 to 2004
21 Immunisations

Immform data: Rotavirus vaccine uptake: East Anglia April-August 2014 [dose 2]
22 Immunisations

Immform: Prenatal Pertussis East Anglia 2014 April-July
23 Immunisations
UK Vaccine Policy published in:
• Immunisation against Infectious Disease (the ‘Green Book’)
• Currently available on Department Health website
• Chapters can be individually downloaded from the website and printed off - updated chapters will replace previous versions as they become available
• Chief Medical Officer Updates, Letters, Publications and Urgent Communications
• These detail any changes to vaccine policy and recommendations
24 Immunisations
National Immunisation Schedule
25 Immunisations
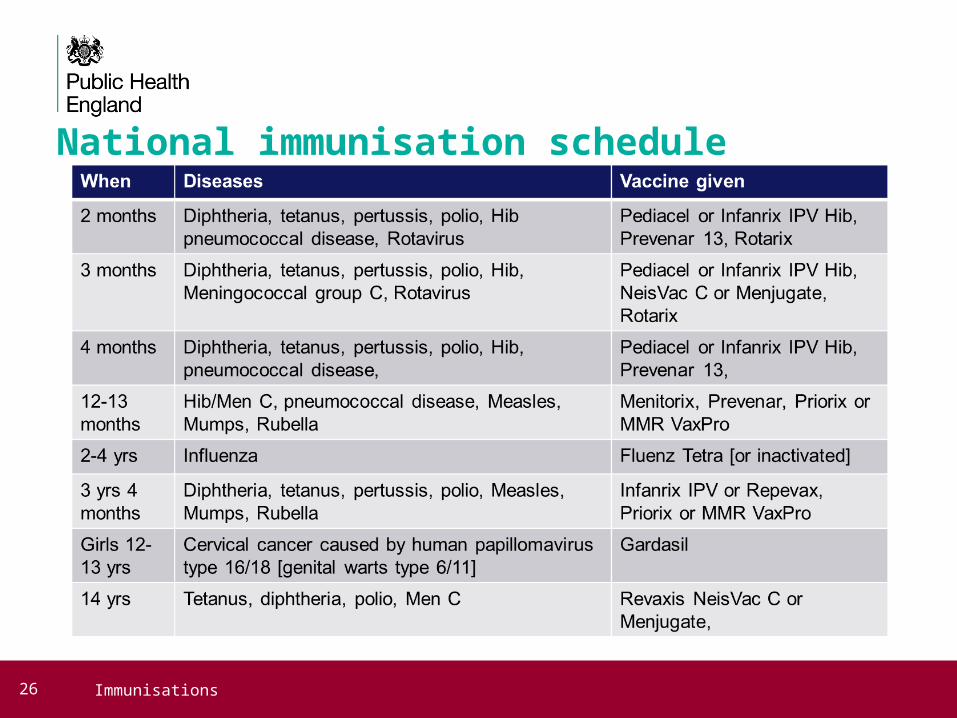
National immunisation schedule
26 Immunisations
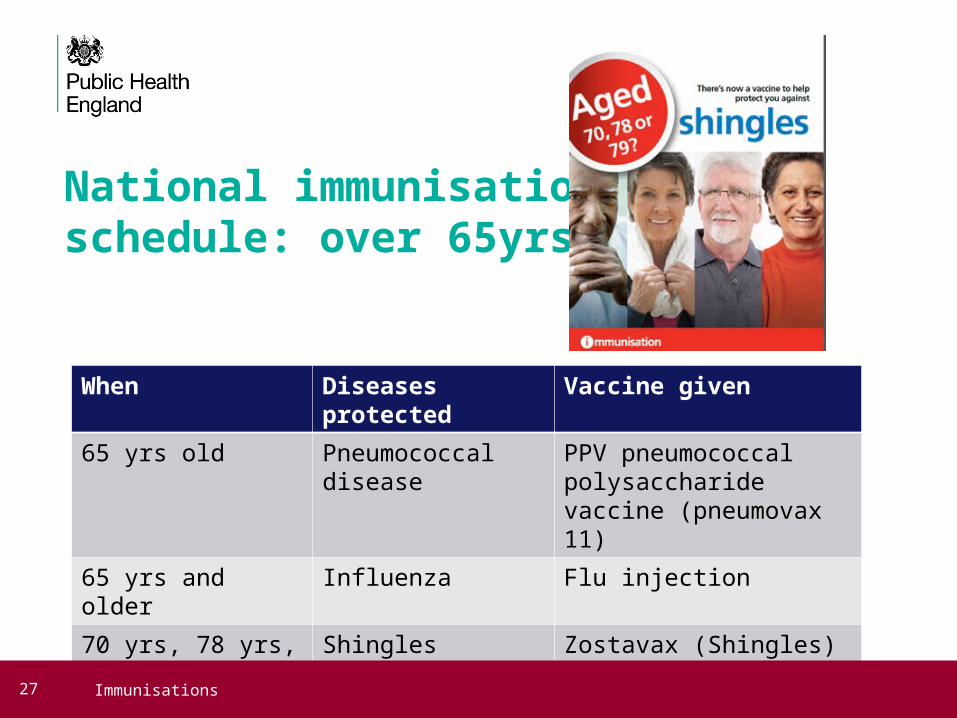
National immunisation schedule: over 65yrs
When Diseases protected Vaccine given
65 yrs old Pneumococcal disease
PPV pneumococcal polysaccharide vaccine (pneumovax 11)
65 yrs and older Influenza Flu injection
70 yrs, 78 yrs, 79 yrs
Shingles Zostavax (Shingles)
27 Immunisations

Other selective vaccination (1) (not for travel)Hepatitis A
•Used to protect contacts of cases
•Used occupationally e.g. sewage workers, lab staff
Hepatitis B
•Given to specific risk groups either because of their lifestyle or health
•Used to protect babies born to Hep B positive mothers
•Used to protect contacts of cases
•Used occupationally e.g. healthcare workers
Influenza (seasonal)
•Over 65s and at risk groups
Pneumococcal
•Over 65s and at risk groups
28 Immunisations

Other selective vaccination (2) (not for travel)Prenatal Pertussis
•Temporary programme to provide Pertussis vaccine to women who are between 28-38 weeks pregnant [from 1st July Boostrix IPV vaccine]
Rabies
•Used for post-exposure prophylaxis
•Used occupationally e.g. bat handlers, animal quarantine centres
TB (BCG)
•< 16yr olds depending on incidence of TB where they live and/or where they originate from
•Occupational risk if < 35 yrs
Varicella
•Contacts of immunocompromised patients
•Used occupationally e.g. health care workers, lab staff
29 Immunisations
Planning schedules for individuals of uncertain or incomplete immunisation status
• Transfer individual onto UK schedule if come from abroad
• No need to restart schedule if evidence of previous immunisation or longer than recommended intervals between vaccine doses – restart schedule where left off [if MMR given before 12months disregard dose]
• Plan catch-up immunisation schedule with minimum number of visits and minimum possible timescale
• Aim to protect individual in shortest time possible
• Consider vaccines that may not have been given to children coming from abroad e.g. MenC, Hib, PCV
• Use PHE algorithm to help plan schedule according to age of individual
30 Immunisations

31 Immunisations

Flu programme
32 Immunisations

Influenza campaign 2013-14
33 Immunisations
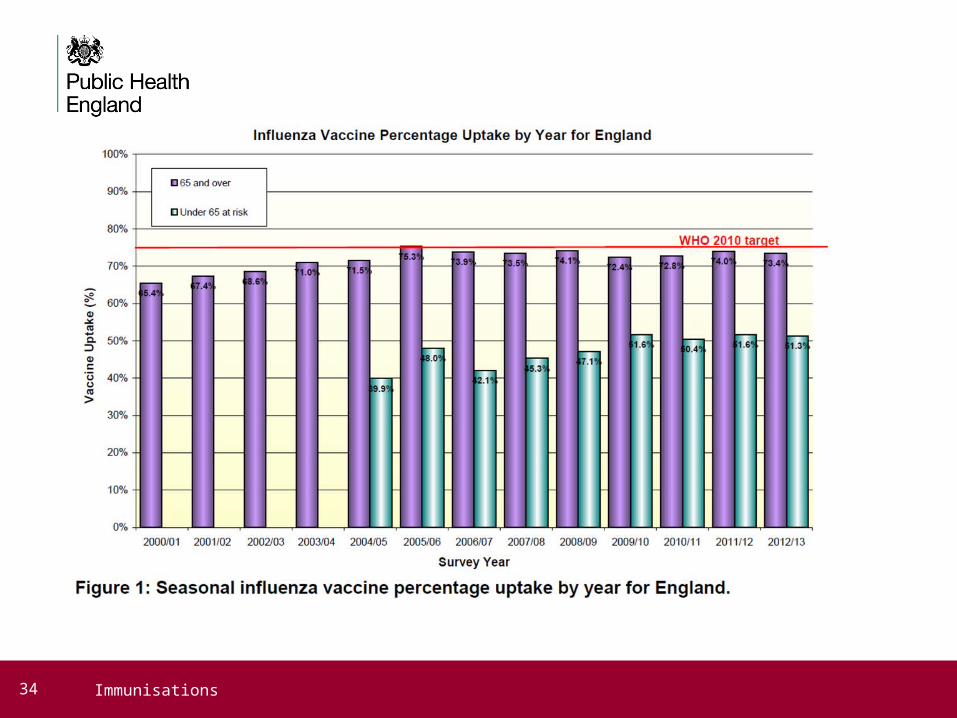
34 Immunisations

2013/4 Influenza uptakes by clinical risk group
35 Immunisations

Influenza
36 Immunisations

Influenza vaccine 2014-15• Trivalent vaccines will contain the following three viruses:
A/California/7/2009 (H1N1)pdm09-like virus
A/Texas/50/2012 (H3N2)-like virus
B/Massachusetts/2/2012-like virus
• In addition to the above, the quadrivalent vaccine will also contain:
B/Brisbane/60/2008-like virus
• None of the influenza vaccines for the 2014/15 season contain thiomersal as an added preservative
• More detailed information on the characteristics of the available vaccines, including age indications and ovalbumin (egg) content can be found in the Influenza chapter of the Green Book
37 Immunisations

Influenza vaccine campaign 2014-15• Over 65 yrs
• Pregnant
• those aged from six months in clinical risk groups
• all children aged two, three and four years on or before 1 Sept 2014 (DOB on or after 2/9/09 and on or before 1/9/12)
• school-aged children [yr 7 & 8] in pilot areas
• carers
• Health and social care workers who are in direct contact with patients or service users should be offered flu vaccination by their employer
38 Immunisations

Child influenza• Average influenza season: estimated 0.3% to 9.8% of 0-14 year old
children present to a GP with influenza
• Incidence rates can be markedly higher in the younger age groups
• Influenza associated hospitalisation rates:
• - 83-1,038/ 100,000 children 0-59 months old (highest in <6m) - 16-210/100,000 children 5-17 years
• Children more vulnerable to infection than adults when exposed
• Children with influenza contribute to the burden of influenza in all age groups because they are more likely to pass on the infection than adults
39 Immunisations
Extended flu programme for children
40 Immunisations

Child Influenza vaccine Pilot• East Anglia participating in child flu pilot programme
• School nursing/imms teams commissioned to deliver programme
• School yr 7 & 8
• Cambs provider: Cambridge Community Services [CCS]
• P’boro provider: Cambridge and Peterborough Foundation Trust [CPFT]
• Starting in Autumn Term 2014
41 Immunisations

Influenza vaccine Two main types of vaccine available:
• Inactivated - by intramuscular injection
• Live - by nasal application
• None of the influenza vaccines can cause clinical influenza in those that can be vaccinated
• Most inactivated flu vaccines are trivalent, containing two subtypes of Influenza A and one type B virus
• A quadrivalent live intranasal vaccine will be offered to children aged 2yrs and over in the 2014/15 flu season Fluenz Tetra® is the recommended vaccine for the childhood flu programme
• *Quadrivalent inactivated influenza vaccine is only authorised for children aged three years and older
42 Immunisations
Fluenz vaccine
43 Immunisations
Contraindications
44 Immunisations

Cold Chain
45 Immunisations

Cold Chain• The ‘cold chain’ is a term used to describe the cold
temperature conditions in which certain products need to be kept during storage and distribution.
• Maintaining the cold chain ensures that vaccines are transported and stored according to the manufacturer’s recommended temperature range of +2˚C to +8˚C until the point of administration.
[see Green Book Chapter 3, for more details]
46 Immunisations

Cold Chain
47 Immunisations

Cold Chain• On receipt of vaccines, staff should check them against the order for
discrepancies and leakage or damage before accepting and signing for them.
• Pharmaceutical distributors and manufacturers will not accept any vaccine for return once it has left their control.
• Vaccines must be refrigerated immediately and must not be left at room temperature.
• The receipt of vaccines should be recorded on a stock inventory It is the responsibility of the named individuals to ensure there is adequate recording of stock ordering and receipt of vaccines.
48 Immunisations
Refrigerators• Specialised refrigerators are available for the
storage of pharmaceutical products and must be used for vaccines and diluents.
• Ordinary domestic refrigerators must not be used. Food, drink and clinical specimens must never be stored in the same refrigerator as vaccines. Opening of the refrigerator door should be kept to a minimum in order to maintain a constant temperature. The fridge temperature gauge should be clearly visible to read without needing to open the fridge door.
49 Immunisations

Read, Record, Reset, ReactRead: daily reading of the thermometer’s maximum, minimum and
current temperatures at the same time every day during the working week
Record: recording temperatures in a standard fashion and on a standard form, including signing each entry on the recording sheet
Reset: resetting the thermometer after each reading. The thermometers should also be reset when temperatures have stabilized after periods of high activity
React: the person making the recording should take action if the temperature falls outside +2˚C to +8˚C and document this action.
50 Immunisations

To improve uptake YOU need to….
• Keep up to date with changes to policy
• Ensure you have access to current vaccine policy and PGD’s
• Ensure you know who to contact when you need further advice or information
• Attend regular training updates
• Make time to discuss parental concerns about immunisation
• Make EVERY effort to vaccinate individuals, as necessary
• No opportunity to vaccinate should be missed
• BE KNOWLEDGABLE AND CONFIDENT
• PROMOTE VACCINATION
51 Immunisations
Health Protection Team Contacts Anglia Health Protection Team
Tel 0344 225 3546 option 1
Fax 01842 765260
Generic email [email protected]
Secure email [email protected]
52 Immunisations
East Anglia SIT ContactsDr. Shylaja Thomas Screening and Immunisation Lead:
For Cambridge and Peterborough:
Dr. Colin Uju Screening and Immunisation Manager: [email protected]
Dr. Karen Lake Screening and Immunisation Co ordinator: [email protected]
For Suffolk
Hossein Khaled Screening and Immunisation Manager: [email protected]
For Norfolk
Sarah Mossop Screening and Immunisation Manager: [email protected]
Dr. Jamie Scott Screening and Immunisation Co ordinator: [email protected]
53 Immunisations

Thank you for listening
Any Questions?
54 Immunisations

Resources
55 Immunisations

56 Immunisations
ResourcesThe Green Book https://www.gov.uk/government/collections/immunisation-
against-infectious-disease-the-green-book
Letter detailing childhood programme: Department of Health, Public Health England, NHS England. The national flu immunisation programme 2014/15. 28 April 2014. Available at: https://www.gov.uk/government/publications/flu-immunisation-programme-2014-to-2015
A leaflet and a poster have been prepared specifically for the childhood influenza programme. Available at: https://www.gov.uk/government/organisations/public-health-england/series/annual-flu-programme
57 Immunisations
Resourceshttps://www.gov.uk/government/news/successful-start-to-rotavirus-vaccination-
programme
PHE website with links to all national training slides:
https://www.gov.uk/government/collections/immunisation
PHE Vaccine updates:
https://www.gov.uk/government/collections/vaccine-update
Immform:
https://www.gov.uk/government/collections/immform
58 Immunisations