imbalanced anti-h1n1 immunoglobulin subclasses and dysregulated cytokines in hospitalized pregnant...
TRANSCRIPT

Human Immunology 73 (2012) 906–911
Contents lists available at SciVerse ScienceDirect
www.ashi-hla.org
journal homepage: www.elsevier .com/ locate/humimm
Imbalanced anti-H1N1 immunoglobulin subclasses and dysregulated cytokinesin hospitalized pregnant women with 2009 H1N1 influenza and pneumoniain Shenyang, China
Rui Zheng a, Xiaosong Qin b,⇑, Yang Li b, Xiaojun Yu b, Jun Wang c, Mingqi Tan a, Zehui Yang a, Wenjie Li a
a Department of Respiratory Medicine, Shengjing Hospital of China Medical University, Shenyang 110004, Chinab Department of Laboratory Medicine, Shengjing Hospital of China Medical University, Shenyang 110004, Chinac Department of Obstetrics, Shengjing Hospital of China Medical University, Shenyang 110004, China
a r t i c l e i n f o a b s t r a c t
Article history:Received 17 November 2011Accepted 13 June 2012Available online 28 June 2012
0198-8859/$36.00 - see front matter � 2012 Americahttp://dx.doi.org/10.1016/j.humimm.2012.06.005
Abbreviations: CDC, center for disease control; Clactic dehydrogenase; CK, creatine kinase; AST, aspaglutamic alanine aminotransferase; Alb, albumin; IFNIL-4, interleukin-4; IL-10, interleukin-10; IgG, immrespiratory distress syndrome.⇑ Corresponding author. Address: Department of La
Hospital of China Medical University, 36 Sanhao Stre110004, China. Fax: +86 24 96615 72116.
E-mail address: [email protected] (X. Qin).
Influenza virus can cause an acute respiratory illness of variable intensity. In our study, we describe theclinical and immunological characteristics of pregnant and nonpregnant women who were hospitalizedwith 2009 H1N1 influenza and pneumonia in Shenyang, China, from November 2009 to January 2010.Forty-two female patient infected with H1N1 were divided into groups according to pregnancy. Clinicaldata were collected. Cytokines and anti-H1N1 IgG subclasses were detected. We observed significantlymphopenia, hypoproteinemia, reduced CD4+T cell counts and CD4+/CD8+ ratios, reduced anti-H1N1IgG subclasses IgG2 and IgG3 constituent ratios, elevated C reactive protein and interleukin-10 levelswith regard to nonpregnant H1N1 group. Compared with the healthy pregnant group, the pregnantH1N1 group showed elevated aspartate aminotransferase and glutamic alanine aminotransferase levels,an increased interferon-gamma and interleukin-10 levels and reduced anti-H1N1 IgG subclasses IgG2,IgG3 and IgG4 combination ratios. There was a statistically significant association between imbalancedanti-H1N1 immunoglobulin subclasses and dysregulated cytokines in pregnant women with H1N1infection.� 2012 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights
reserved.
1. Introduction
Influenza virus can cause an acute respiratory illness with vary-ing degrees of severity. This orthomyxovirus has the ability tocause pandemics occasionally as a result of antigenic shifts. Thefirst pandemics occurred in 1918 (Spanish flu), and three morepandemics have occurred since then. Although the 2009 pandemicH1N1 influenza had largely run its course by August 2010, as an-nounced by the World Health Organization [1], the H1N1 virus la-ter took on the behavior of a seasonal influenza virus andcontinued to circulate in the winter of 2010, just as expected. Inthe spring of 2011, there were increasing reports of a new roundof H1N1-subtype influenza infection in Europe, and reports of
n Society for Histocompatibility an
RP, C reactive protein; LDH,rtate aminotransferase; ALT,-gamma, interferon-gamma;
unoglobulin G; ARDS, acute
boratory Medicine, Shengjinget, Heping District, Shenyang
death have been made in England, Germany, Switzerland andChina. Most infections with the 2009 pandemic H1N1 virus havebeen self-limited, but a high risk of influenza complications wasobserved in some subpopulations [2]. Pregnant women had anincreased risk of influenza complications in the past two pandem-ics (1918–1919 and 1957–1958) [3]. The first case of an infectionwith 2009 pandemic influenza A (H1N1) virus in China was docu-mented on May 10, 2009, and by December 2009, the number ofreported cases in China was 110,590 [China Centre for DiseaseControl, CDC]. Although the severity of disease ranged from mildto severe, little information has been reported about how thisoutbreak affected pregnant women in China. During pregnancy,physiologic alterations in the respiratory, cardiovascular and im-mune systems may increase the susceptibility to respiratory infec-tions or adversely alter their clinical course [4,5]. During bothseasonal influenza epidemics [6,7] and previous pandemics [8,9],pregnant women have had increased morbidity and mortality frominfluenza infection compared with women who were not pregnant.
This report describes the clinical course of the disease andimmunological characteristics of pregnant and nonpregnant wo-men hospitalized with 2009 H1N1 influenza in Shenyang, China,from November 14, 2009, to January 10, 2010.
d Immunogenetics. Published by Elsevier Inc. All rights reserved.

R. Zheng et al. / Human Immunology 73 (2012) 906–911 907
2. Materials and methods
2.1. Patients
A total of 42 women with both pneumonia and 2009 H1N1 influ-enza infection were hospitalized in the Shengjing Hospital of ChinaMedical University from November 14, 2009, to January 10, 2010.We conducted a retrospective review of the charts from all 42 caseswithout any selection. Of these patients, 22 were pregnant andserved as the pregnant H1N1 group, and the other 20 were nonpreg-nant and served as a nonpregnant H1N1 group. An additional 19 nor-mal pregnant women with positive anti-H1N1 IgG, as screened byELISA, served as the pregnant control group. During the 2009H1N1 influenza epidemic, patients in clinics or emergency depart-ments who presented with an influenza-like illness were testedfor the 2009 H1N1 influenza virus, and only those patients whose ill-ness was accompanied by pneumonia were admitted to our hospital.Patients with mild symptoms were isolated for treatment at home.The Shengjing Hospital of China Medical University is a tertiary carecenter that includes obstetric services and pediatric wards; it is alsoa tertiary referral center for patients infected with 2009 H1N1 influ-enza, especially for children and pregnant women, as appointed bythe national government. All patients were identified as positivefor 2009 H1N1 influenza A by using a real-time reverse-transcrip-tase-polymerase-chain-reaction (RT-PCR) assay of nasopharyngealand throat swabs at the CDC. All tests used standard CDC-basedprimers. Pneumonia was diagnosed by chest radiography and clini-cal symptoms and physical signs on admission. The study was ap-proved by the Ethics Committee of China Medical University.
2.2. Study design
Four clinicians reviewed and abstracted data from all available hos-pital records for each hospitalized woman with confirmed 2009 H1N1influenza by using a standardized abstraction form. To ensure that thedata collected by all investigators were consistent, a standardizeddata-collection method was defined. For both pregnant and nonpreg-nant women, we abstracted data elements to assess time of symptomonset, underlying conditions, intervals between symptom onset andinitiation of oseltamivir therapy, treatment course and length of stay,and selected laboratory results, including white blood cell classifica-tion and count, levels of C reactive protein (CRP), lactic dehydrogenase(LDH), creatine kinase (CK), aspartate aminotransferase (AST),glutamic alanine aminotransferase (ALT), albumin (Alb), interferon-gamma (IFN-gamma), interleukin-4 (IL-4), interleukin-10 (IL-10), per-centage of CD4+ and CD8+ T cells, subclasses of anti-H1N1 specificimmunoglobulin G (total, IgG1, IgG2, IgG3 and IgG4), blood gas analy-ses and radiographic findings. All of the laboratory test data wereacquired within 24 h of admission to the hospital. For pregnant wo-men, we abstracted additional details of gestational age and, whenapplicable, labor and delivery. Gestational age at the onset of illnesswas computed as 40 weeks – (estimated delivery date – illness onsetdate)/7. For those women who had delivered, gestational age at deliv-ery was computed as 40 weeks – (estimated delivery date – actualdelivery date)/7. Delivery at a gestational age of less than 37 com-pleted weeks was categorized as a preterm delivery. Underlying con-ditions were entered as open text and were classified into thefollowing categories: cardiovascular, hepatic, thyroid, diabetes, ane-mia and other. Hospital length of stay was computed as (dischargedate) – (admission date). Maternal outcome was recorded as survivalor death.
2.3. Laboratory assays
Tests to confirm infection with 2009 H1N1 influenza A wereperformed by using standard CDC-based primers and real-time
reverse-transcriptase-polymerase-chain-reaction (RT-PCR) assaysof nasopharyngeal and throat swab specimens.
Serum CRP was assessed using a Beckman IMMAGE 800 ana-lyzer (Beckman Coulter). Alb and serum enzymes (LDH: lacticdehydrogenase; CK: creatine kinase; AST: glutamic-oxaloacetictransaminase; ALT: glutamic alanine aminotransferase) were as-sessed using an Abbott Architect ci8200 analyzer (Abbott Laborato-ries, Abbott Park) in accordance with the manufacturer’sinstructions. White blood cell classification and count were ana-lyzed by a Beckman LH750 analyzer (Beckman Coulter). CD4+
and CD8+ T cell percentages were analyzed by FACSCalibur flowcytometry (BD).
Enzyme-Linked Immunosorbent Assays (ELISAs) were performedby using ELISA Kits (eBioscience) to examine serum interferon-gam-ma (IFN-gamma), interleukin-4 (IL-4) and interleukin-10 (IL-10)levels. Anti-H1N1 IgG levels were measured using a Human H1N1IgG antibody ELISA Kit (Wuhan Huamei Bioscience) in accordancewith the manufacturer’s instructions.
Similarly, specific anti-H1N1 IgG1, IgG2, IgG3 and IgG4 levelswere measured by using Human H1N1 IgG antibody ELISA Kits(Wuhan Huamei Bioscience) with HRP-conjugated mouse anti-hu-man IgG1, IgG2, IgG3 and IgG4 (eBioscience) as the detection anti-bodies. To determine the constituent ratio of anti-H1N1 IgGsubclasses in each specimen, the sum total of the optical density(OD) values from the assays of anti-human H1N1 IgG1, IgG2,IgG3 and IgG4 was defined as 100%, and then, the OD percentageof each anti-human H1N1 IgG1, IgG2, IgG3 and IgG4 was calcu-lated. To determine the combination ratio of each anti-H1N1 IgGsubclass, the average OD values from the blank wells and the posi-tive control wells for that subclass were defined as 0% and 100%,respectively, a regression equation was established, and the combi-nation percentage of the IgG subclass was calculated.
2.4. Statistical analysis
All statistical analyses were performed using SPSS Version 11.5(SPSS, Inc., Chicago, IL). A two-sided P-value of less than 0.05 wasconsidered statistically significant. Continuous variables were re-ported as the median (range: min–max), and a nonparametric testwas used when appropriate. For categorical variables, the percent-age of patients in each category was calculated, and a Chi-squaretest or Fisher’s exact test was used as appropriate.
3. Results
3.1. Clinical characteristics
The median ages were 28 years (range: 20–39 years), 41 years(range: 14–68 years) and 29 years (range: 23–38 years) for thepregnant H1N1 group, nonpregnant H1N1 group and pregnantcontrol group, respectively. The pregnant H1N1 and pregnant con-trol groups were, on average, younger than the nonpregnant H1N1group (Table 1).
Medical histories of pregnant and nonpregnant cases werenotably different. Among the 22 pregnant H1N1 patients, 4 hadat least two conditions other than pregnancy that put them at highrisk for influenza complications; these chronic co-existing illnessesincluded cardiovascular, hepatic, thyroid and pulmonary diseasesas well as diabetes and anemia (Table 1). While 16 (72.7%) of thepregnant H1N1 patients had such high-risk conditions, only 4(20.0%) of the nonpregnant women and 5 (26.3%) of the normalpregnant women had one or more of these underlying conditions(P < 0.01).
None of the patients had been vaccinated for seasonal or 2009H1N1 influenza during 2008 or 2009, because only a selected
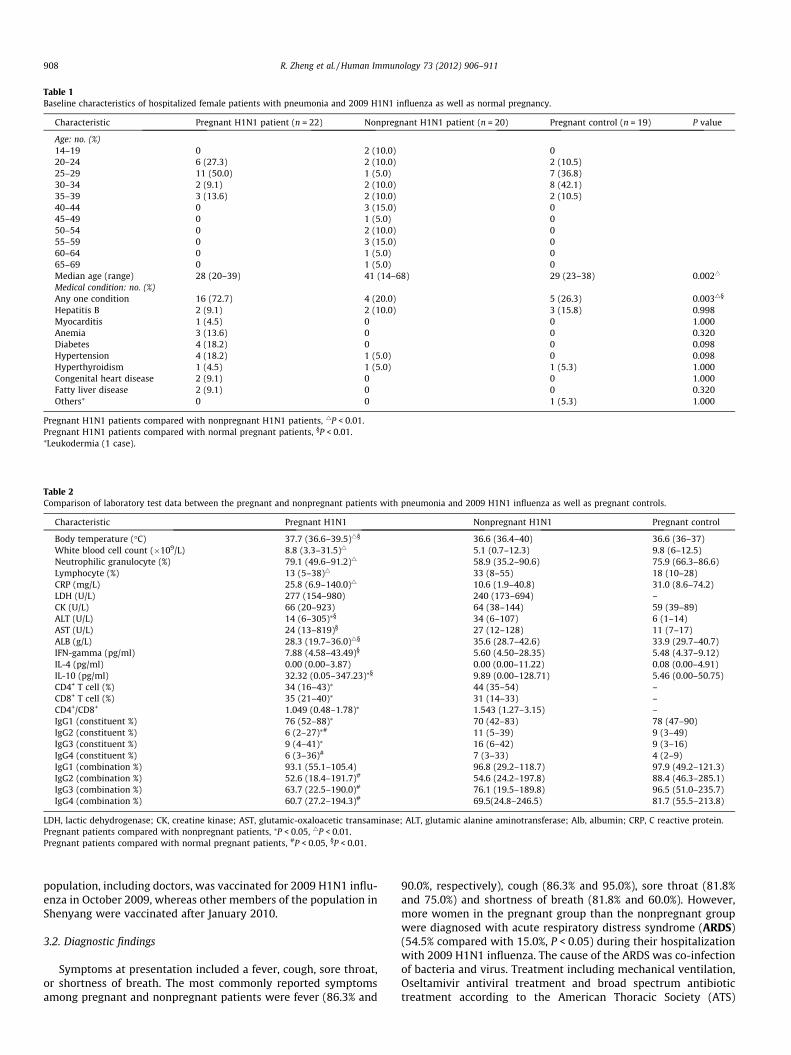
Table 1Baseline characteristics of hospitalized female patients with pneumonia and 2009 H1N1 influenza as well as normal pregnancy.
Characteristic Pregnant H1N1 patient (n = 22) Nonpregnant H1N1 patient (n = 20) Pregnant control (n = 19) P value
Age: no. (%)14–19 0 2 (10.0) 020–24 6 (27.3) 2 (10.0) 2 (10.5)25–29 11 (50.0) 1 (5.0) 7 (36.8)30–34 2 (9.1) 2 (10.0) 8 (42.1)35–39 3 (13.6) 2 (10.0) 2 (10.5)40–44 0 3 (15.0) 045–49 0 1 (5.0) 050–54 0 2 (10.0) 055–59 0 3 (15.0) 060–64 0 1 (5.0) 065–69 0 1 (5.0) 0Median age (range) 28 (20–39) 41 (14–68) 29 (23–38) 0.0024
Medical condition: no. (%)Any one condition 16 (72.7) 4 (20.0) 5 (26.3) 0.0034§
Hepatitis B 2 (9.1) 2 (10.0) 3 (15.8) 0.998Myocarditis 1 (4.5) 0 0 1.000Anemia 3 (13.6) 0 0 0.320Diabetes 4 (18.2) 0 0 0.098Hypertension 4 (18.2) 1 (5.0) 0 0.098Hyperthyroidism 1 (4.5) 1 (5.0) 1 (5.3) 1.000Congenital heart disease 2 (9.1) 0 0 1.000Fatty liver disease 2 (9.1) 0 0 0.320Others⁄ 0 0 1 (5.3) 1.000
Pregnant H1N1 patients compared with nonpregnant H1N1 patients, 4P < 0.01.Pregnant H1N1 patients compared with normal pregnant patients, §P < 0.01.⁄Leukodermia (1 case).
Table 2Comparison of laboratory test data between the pregnant and nonpregnant patients with pneumonia and 2009 H1N1 influenza as well as pregnant controls.
Characteristic Pregnant H1N1 Nonpregnant H1N1 Pregnant control
Body temperature (�C) 37.7 (36.6–39.5)4§ 36.6 (36.4–40) 36.6 (36–37)White blood cell count (�109/L) 8.8 (3.3–31.5)4 5.1 (0.7–12.3) 9.8 (6–12.5)Neutrophilic granulocyte (%) 79.1 (49.6–91.2)4 58.9 (35.2–90.6) 75.9 (66.3–86.6)Lymphocyte (%) 13 (5–38)4 33 (8–55) 18 (10–28)CRP (mg/L) 25.8 (6.9–140.0)4 10.6 (1.9–40.8) 31.0 (8.6–74.2)LDH (U/L) 277 (154–980) 240 (173–694) –CK (U/L) 66 (20–923) 64 (38–144) 59 (39–89)ALT (U/L) 14 (6–305)⁄§ 34 (6–107) 6 (1–14)AST (U/L) 24 (13–819)§ 27 (12–128) 11 (7–17)ALB (g/L) 28.3 (19.7–36.0)4§ 35.6 (28.7–42.6) 33.9 (29.7–40.7)IFN-gamma (pg/ml) 7.88 (4.58–43.49)§ 5.60 (4.50–28.35) 5.48 (4.37–9.12)IL-4 (pg/ml) 0.00 (0.00–3.87) 0.00 (0.00–11.22) 0.08 (0.00–4.91)IL-10 (pg/ml) 32.32 (0.05–347.23)⁄§ 9.89 (0.00–128.71) 5.46 (0.00–50.75)CD4+ T cell (%) 34 (16–43)⁄ 44 (35–54) –CD8+ T cell (%) 35 (21–40)⁄ 31 (14–33) –CD4+/CD8+ 1.049 (0.48–1.78)⁄ 1.543 (1.27–3.15) –IgG1 (constituent %) 76 (52–88)⁄ 70 (42–83) 78 (47–90)IgG2 (constituent %) 6 (2–27)⁄# 11 (5–39) 9 (3–49)IgG3 (constituent %) 9 (4–41)⁄ 16 (6–42) 9 (3–16)IgG4 (constituent %) 6 (3–36)# 7 (3–33) 4 (2–9)IgG1 (combination %) 93.1 (55.1–105.4) 96.8 (29.2–118.7) 97.9 (49.2–121.3)IgG2 (combination %) 52.6 (18.4–191.7)# 54.6 (24.2–197.8) 88.4 (46.3–285.1)IgG3 (combination %) 63.7 (22.5–190.0)# 76.1 (19.5–189.8) 96.5 (51.0–235.7)IgG4 (combination %) 60.7 (27.2–194.3)# 69.5(24.8–246.5) 81.7 (55.5–213.8)
LDH, lactic dehydrogenase; CK, creatine kinase; AST, glutamic-oxaloacetic transaminase; ALT, glutamic alanine aminotransferase; Alb, albumin; CRP, C reactive protein.Pregnant patients compared with nonpregnant patients, ⁄P < 0.05, 4P < 0.01.Pregnant patients compared with normal pregnant patients, #P < 0.05, §P < 0.01.
908 R. Zheng et al. / Human Immunology 73 (2012) 906–911
population, including doctors, was vaccinated for 2009 H1N1 influ-enza in October 2009, whereas other members of the population inShenyang were vaccinated after January 2010.
3.2. Diagnostic findings
Symptoms at presentation included a fever, cough, sore throat,or shortness of breath. The most commonly reported symptomsamong pregnant and nonpregnant patients were fever (86.3% and
90.0%, respectively), cough (86.3% and 95.0%), sore throat (81.8%and 75.0%) and shortness of breath (81.8% and 60.0%). However,more women in the pregnant group than the nonpregnant groupwere diagnosed with acute respiratory distress syndrome (ARDS)(54.5% compared with 15.0%, P < 0.05) during their hospitalizationwith 2009 H1N1 influenza. The cause of the ARDS was co-infectionof bacteria and virus. Treatment including mechanical ventilation,Oseltamivir antiviral treatment and broad spectrum antibiotictreatment according to the American Thoracic Society (ATS)

R. Zheng et al. / Human Immunology 73 (2012) 906–911 909
guidelines of 2007 [10] in ICU hospitalized patients with commu-nity acquired pneumonia (CAP). During hospitalization, all patientswere treated with antiviral drugs and antibiotics. In pregnant andnon-pregnant patients, the start time of Oseltamivir antiviral treat-ment from admission were 2 (1–4) and 1 (1–3) days, respectively;the start time of antibiotics therapy from admission were 2 (1–10)and 1(1–3) days, respectively; the length of hospital day were 12(6–55) and 11(6–22) days, respectively. 100% of the ARDS patientsreceived more than one antibiotic. Commonly used antibiotics in-cluded ceftriaxone, cefoperazone/sulbactam, meropenem, azithro-mycin, moxifloxacin, levofloxacin and vancomycin. Meanantibiotics administration time were 13 (7–21) days in ARDSpatients.
Among the 22 pregnant H1N1 patients, 13.6% (3 of 22) were inthe first trimester, 27.3% (6 of 22) were in the second trimester and59.1% (13 of 22) were in the third trimester. Among the pregnantcontrol group, 15.8% (3 of 19) were in the first trimester, 26.3%(5 of 19) were in the second trimester and 57.9% (11 of 19) werein the third trimester.
Laboratory results of pregnant H1N1 and nonpregnant H1N1cases were notably different, except for the levels of serum CKand serum LDH. Pregnant patients were more likely than nonpreg-nant patients to have elevated levels of WBC, CRP and percentageof neutrophilic granulocyte as well as reduced levels of ALT andAlb (P < 0.01) (Table 2). In addition, we observed that pregnant pa-tients infected with H1N1 virus had a lower percentage of lympho-cytes than that of nonpregnant patients (P < 0.01). All patientswere negative for HIV. To evaluate the immunological responseof these cases, we further determined the levels of IL-4, IL-10,IFN-gamma and anti-H1N1 IgG subclasses (IgG1–4). Among thethree groups, the level of IFN-gamma was higher in pregnantH1N1 patients than in normal pregnant patients: 7.88 (range:4.58–43.49) pg/ml versus 5.48 (range: 4.37–9.12) pg/ml, respec-tively, P < 0.05. IL-10 levels were notably different among the threegroups. In pregnant H1N1 patients, the IL-10 level was 32.32(range: 0.05–347.23) pg/ml, which was higher than that in non-pregnant patients and normal pregnant women, P < 0.01. Both areduction in CD4+ and CD8+ T cell percentages and a low CD4+/CD8+ ratio were found in the pregnant H1N1 group compared withthe nonpregnant group, P < 0.05. For anti-H1N1 IgG subclasses,there were lower combination ratios of IgG subclasses IgG2, IgG3and IgG4 in the pregnant H1N1 group than in the pregnant con-trols, P < 0.05 (Table 2). Furthermore, an imbalanced constituentproportion among anti-H1N1 IgG subclasses was found, and theconstituent proportions of IgG1, IgG2, IgG3 and IgG4 among thethree groups were different. An increased anti-H1N1 IgG1 constit-uent proportion was found in the pregnant H1N1 group comparedwith the nonpregnant patients, while at the same time, IgG2 andIgG3 constituent proportions were decreased in the pregnantH1N1 group, P < 0.05. Compared with the pregnant controls, theanti-H1N1 IgG2 constituent proportion was decreased, and IgG4was increased in the pregnant H1N1 group, P < 0.05 (Table 2).
3.3. Outcomes
Among the 42 hospitalized H1N1 patients, 20 (90.1%) of 22pregnant women and all 20 nonpregnant patients were discharged.There were two deaths (9.9%) among the pregnant patients, both ofwhose symptoms became critical after delivery. The antiviral ther-apy time of two death were started at 7 and 8 days after onset (1and 2 days after their hospital admission), the antiviral treatmentwere lasted for 15 and 7 days, respectively, until their death. Ofthe two deaths, one patient delivered a live birth at gestationalweek 34 by an emergency Cesarean after hospitalization and died9 days after delivery. In the other patient, the fetus was found deadin the uterus on the day of hospitalization and was delivered by an
emergency cesarean section; maternal death occurred 16 daysafter delivery. There were nine live births in 12 deliveries amongpregnant H1N1-infected patients. In addition to the intrauterinefetal death mentioned above, another two fetal losses occurred:one more intrauterine loss and one loss during urgent cesareandelivery to save the mother’s life. The time from hospital admissionto the two maternal deaths was 16 and 9 days, respectively. Themedian length of stay in the hospital for survivors was 12 days(range: 6–55) and 11 days (range: 6–22) for pregnant and non-pregnant H1N1-infected patients, respectively.
4. Discussion
In current study, we report on a series of hospitalized pregnantpatients infected with H1N1 influenza. We found that imbalancedanti-H1N1 immunoglobulin subclasses and dysregulated cytokineswere notable characteristics of pregnant women infected withH1N1 influenza.
In this study, most of these patients had no certain history ofcontact with other H1N1-infected patients, and there were nocases of similar severity in their families. The median age of thepregnant patients affected with H1N1 virus was 28 years, and themedian gestational week was 32 weeks, which is consistent withother reports [11–13]. These findings indicate that pregnant wo-men are more easily infected with H1N1 during the third trimesterof gestational age. At a late gestational age, the high oxygen con-sumption of the mother can easily lead to an anoxic or hypoxiccondition that makes the mother prone to infection with patho-gens. Our study found that pregnant women hospitalized with2009 H1N1 influenza were more likely to have underlying medicalconditions than nonpregnant hospitalized women. These findingssuggest that pregnancy increases the incidence of medical compli-cations and that pregnant women infected with the H1N1 viruswill easily develop a severe case. However, the detailed mechanismof is not clear. This result may be because pregnant women had achanged immunological condition during the gestational period.Their other underlying medical conditions may have made preg-nant women sensitive to viruses and other pathogenic pathogens.Heart disease is considered a predisposing factor for 2009 H1N1influenza infection [14]. In our study, about 27% of the pregnantpatients with pre-existing medical conditions suffered from heartdisease (hypertension or congenital heart disease). Thus, it isappropriate that physicians should pay close attention to patients,especially pregnant patients, with chronic heart disease during theinfluenza epidemic.
Several studies have found that patients infected with H1N1virus will experience hypoproteinemia and lymphopenia. In thisstudy, we found that the WBC counts, neutrophil percentagesand CRP levels in pregnant patients were higher than those of non-pregnant patients, while lymphocytes were decreased in pregnantH1N1 patients. These findings indicate that pregnant women weresusceptible to combined bacterial infection.
The observed CD4+ and CD8+ T cell percentages indicated that areduction in CD4+ T cell percentage and a low CD4+/CD8+ ratiocould be found in most pregnant patients during the early stagesof 2009 H1N1 virus infection. This result is similar to that of previ-ous reports in China [13–15]. Compared with pregnant controls, anelevated level of IFN-gamma was found in pregnant women in-fected with the H1N1 virus. Considering the finding of CD4+ T cellreduction in the pregnant infected group, the increased IFN-gam-ma might originate mainly from CD8+ T cell. Consistent with this,a lower level of IL-4 was observed in pregnant women infectedwith H1N1 virus, indicating that the CD4+ Th2 cell populationwas also diminished in pregnant infected patients. Taken together,lymphopenia may be caused by T cell reduction, especially a

910 R. Zheng et al. / Human Immunology 73 (2012) 906–911
reduction of CD4+ Th2 cells. The direction of helper T cell differen-tiation is decided by cytokines and hormones. In pregnant women,an overwhelming Th2 expression allows the mother to inhibit anexclusion response to agnate MHC (human histocompatibility anti-gen) in the fetus and to maintain the balance of a suppressed cell-mediated immune response and an enhanced humoral immune re-sponse. IL-10 is a characteristic cytokine that is secreted by acti-vated Th2 cells and IL-10 increase in normal pregnancy is mainlythe representation of immune response inhibition during preg-nancy. A recent review [16] further demonstrated that the majorTh1/Th2 changes are at the local (intervillous), rather than at themother’s systemic circulation. Another study [17] also describedthat after H1N1 vaccination, pregnant women showed increasesof regulatory CD4+FoxP3+% and CD4+IL-10+% and decreased anti-body responses to the H1N1 vaccine. In current study, the CD4+
Th2 cell population was diminished in pregnant H1N1-infected pa-tients, here, we speculate that, when pregnant women are suffer-ing H1N1 attack, rather than secreted by Th2 cells, the observedincrease in IL-10 production may be a consequence of other origi-nation of IL-10 such as regulatory CD4+T cells and enhanced hu-moral immunity and a protectively negative feedback in responseto increased levels of pro-inflammatory cytokines such as IFN-gamma during H1N1 infection. However, the elevated IL-10 couldalso inhibit the host immune response to pathogens and lead to afailure to clear the virus so that the infection deteriorated. Thus,the effect of dysregulated cytokines on maternal immunity is apredisposition to more severe manifestations of H1N1 influenza.
To further study how humoral immunity was changed in H1N1-infected pregnant patients, we measured the levels of anti-H1N1IgG and its subclasses. To our knowledge, this is the first reportto identify the immune response of pregnant women infected withH1N1 influenza. We specifically measured the subclasses of anti-H1N1 influenza IgG antibodies in pregnant patients. IgG is com-posed of 4 subclasses: IgG1, IgG2, IgG3 and IgG4. On average, thedistrubution of IgG subclasses is IgG1 > IgG2 > IgG3 = IgG4. Abnor-mality in the distribution of IgG subclasses is usually asymptom-atic, and low levels of one or more IgG subclasses can be foundin �2–20% of healthy individuals [18,19]. In mouse models, anti-influenza antibodies (specifically IgG) play a vital role in virus con-trol in the lower respiratory tract as compared with the upperrespiratory tract [20,21]. In humans, some studies have found thatpatients with severe H1N1 infection are likely to be deficient inIgG2 [22–24]. However, to our knowledge, the specific anti-H1N1IgG and subclasses have not been studied in detail in humans withinfluenza infection. In our current study, the anti-H1N1 specific IgGsubclass combination ratio is representative of the production ofeach IgG subclass. The finding that the combination ratio of anti-H1N1 IgG2, IgG3 and IgG4 were decreased in the pregnantH1N1-infected group suggests that production of these subclasseswas reduced in pregnant H1N1-infected women compared withnonpregnant infected women. Pregnancy may be one factor thataccounts for the decreased production of anti-H1N1 specificIgG2, IgG3, IgG4 subclasses. Anti-H1N1 specific IgG2 deficiencymay partially contribute to the IgG2 deficiency observed inH1N1-infected patients. We further studied the constituent pro-portion of anti-H1N1 IgG subclasses. Our data indicated thatIgG1 was a dominant subclass of anti-H1N1 IgG in all groups, whileIgG2, IgG3 and IgG4 had varying distributions in different groups.We found that the proportion of IgG2 among total anti-H1N1 IgGdiffered notably between pregnant H1N1-infected patients andnonpregnant H1N1-infected patients. This difference may be dueto the decrease in immunoglobulin levels, especially IgG2, whichalways occurs during normal pregnancy. However, compared withpregnant controls, pregnant H1N1 patients had a lower IgG2 pro-portion of total anti-H1N1 IgG. From this result, combined withthe decreased IgG2 combination ratio in pregnant H1N1-infected
women, we speculated that in pregnant H1N1-infected patients,there was a reduction of total IgG and IgG2. The simultaneously re-duced production of IgG2 and imbalanced IgG subclasses resultedin a decreased proportion of IgG2 among total IgG. Even consider-ing the reduced immunoglobulin normally occurs in during preg-nancy, these results show that an imbalanced distribution ofIgG2 was correlated with H1N1 infection. The finding that the pro-portion of IgG3 was lower in the pregnant H1N1 group than in thenonpregnant group, but similar to that in the pregnant controlgroup, implies that the decrease in IgG3 proportion is probablydue to pregnancy whereas the decrease in IgG2 proportion is morelikely to be correlated with H1N1 infection.
The absolute reduction of H1N1-specific IgG2 in pregnancy withH1N1 infection was accompanied by a relative decline of the IgG2constituent ratio and an imbalance of various IgG subclasses. Thesedata showed that in H1N1-infected pregnant women, there wasnot only a reduction of total anti-H1N1 IgG but also an imbalanceof IgG subclasses characterized by decreased a proportion of IgG2.Furthermore, the deficiency of IgG3 found in pregnant H1N1-in-fected women compared with nonpregnant H1N1-infected womensuggests that IgG3 seems to be more important for pregnant wo-men during the emergence of the H1N1 pandemic. Therefore, weshould pay more attention to the imbalance of immunoglobulinsubclasses when we treat the special subpopulations, such as preg-nant women. Although IgG2 and IgG3 deficiency appears to beassociated with the severity of H1N1 infection, especially in preg-nant women, it remains uncertain whether administration ofimmunoglobulin to patients who have imbalance of immunoglob-ulin subclasses is likely to be therapeutically beneficial. Recently,samples of plasma obtained from a convalescent-phase patientwho recovered from H5N1 influenza infection were used success-fully [25]. Our findings suggest that even if the serum immuno-globulin subclasses in pregnant H1N1-infected women were inthe normal range, the possibility of specific anti-H1N1 IgG subclassdeficiency should not be neglected.
Here, we found that IgG2 deficiency occurs in severe cases ofH1N1 in pregnant women. We strongly remind the clinician thatfor special subpopulations such as pregnant women, they shouldpay great attention to imbalances of immunoglobulin subclassesand dysregulation of cytokine when H1N1 is pandemic. For preg-nant H1N1 patients, changes in the immune response may includethe suppression of cell-mediated immunity and an unbalanced hu-moral immunity, which are prone to alter a pregnant woman’s sus-ceptibility to and the severity of certain infectious diseases.Infectious pathogens may also cause placental inflammatory andpossible neuro-mental disorders in the human offspring [26].Pregnancy must be considered a potential risk factor for diseasesusceptibility as well as for illness and death.
Our study has several limitations, including its relatively lim-ited size. We specifically evaluated only patients with severe con-firmed 2009 H1N1 infection, so the group may not berepresentative of all hospitalized patients because some infectionsmay not have been detected. Even though this H1N1 influenzapandemic has almost finished, the characteristics of the immuneresponse in specific populations during the pandemic should bestudied well so that we can respond to next possible influenza witha more efficient coping strategy.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgments
We thank the staff members of the Center for Disease Control ofLiaoning Province (particularly Wei Zhao and Ling Sun) for their

R. Zheng et al. / Human Immunology 73 (2012) 906–911 911
assistance with virology laboratory analyses for 2009 H1N1 influ-enza A. We thank the resident physicians for their efforts towardstreatment of patients. We thank Hongbo Liu for her assistance instatistical analysis. We thank anonymous reviewers for their con-structive comments on this manuscript. The authors wish toacknowledge financial support from the following sources: X.Q.and R.Z. were supported by the Natural Science Foundation ofLiaoning Province.
References
[1] World health organization. H1N1 in post-pandemic period. Availablefrom: http://www.who.int/mediacentre/news/statements/2010/h1n1_vpc_20100810/en/index.html
[2] Jamieson DJ, Honein MA, Rasmussen SA, Williams JL, Swerdlow DL, BiggerstaffMS, et al. H1N1 2009 influenza virus infection during pregnancy in the USA.Lancet 2009;374:451–8.
[3] Mangtani P, Mak TK, Pfeifer D. Pandemic H1N1 infection in pregnant women inthe USA. Lancet 2009;374:429–30.
[4] Jamieson DJ, Theiler RN, Rasmussen SA. Emerging infections and pregnancy.Emerg Infect Dis 2006;12:1638–43.
[5] Cono J, Cragan JD, Jamieson DJ, Rasmussen SA. Prophylaxis and treatment ofpregnant women for emerging infections and bioterrorism emergencies.Emerg Infect Dis 2006;12:1631–7.
[6] Neuzil KM, Reed GW, Mitchel EF, Simonsen L, Griffin MR. Impact of influenzaon acute cardiopulmonary hospitalizations in pregnant women. Am JEpidemiol 1998;148:1094–102.
[7] Dodds L, McNeil SA, Fell DB, Allen VM, Coombs A, Scott J, et al. Impact ofinfluenza exposure on rates of hospital admissions and physician visitsbecause of respiratory illness among pregnant women. CMAJ: Can MedAssoc J 2007;176:463–8.
[8] Freeman DW, Barno A. Deaths from Asian influenza associated with pregnancy.Am J Obstet Gynecol 1959;78:1172–5.
[9] Nuzum JW, Pilot I, Stangl FH, Bonar BE. 1918 pandemic influenza andpneumonia in a large civil hospital. IMJ: Ill Med J 1976;150:612–6.
[10] Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC,et al. Infectious Diseases Society of America/American Thoracic Societyconsensus guidelines on the management of community-acquiredpneumonia in adults. Clin Infect Dis 2007;44(Suppl. 2):S27–72.
[11] Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M,Quinones-Falconi F, Bautista E, et al. Pneumonia and respiratory failure fromswine-origin influenza A (H1N1) in Mexico. N Engl J Med 2009;361:680–9.
[12] Jain S, Kamimoto L, Bramley AM, Schmitz AM, Benoit SR, Louie J, et al.Hospitalized patients with 2009 H1N1 influenza in the United States,April–June 2009. N Engl J Med 2009;361:1935–44.
[13] Cao B, Li XW, Mao Y, Wang J, Lu HZ, Chen YS, et al. Clinical features of theinitial cases of 2009 pandemic influenza A (H1N1) virus infection in China. NEngl J Med 2009;361:2507–17.
[14] Cui W, Zhao H, Lu X, Wen Y, Zhou Y, Deng B, et al. Factors associated withdeath in hospitalized pneumonia patients with 2009 H1N1 influenza inShenyang, China. BMC Infect Dis 2010;10:145.
[15] Ou Q, Lu Y, Huang Q, Cheng X. Clinical analysis of 150 cases with the novelinfluenza A (H1N1) virus infection in Shanghai, China. Biosci Trends2009;3:127–30.
[16] Nahmias A, Danielsson D. Introduction to the evolution of infectious agents inrelation to sex. Ann N Y Acad Sci 2011;1230:xiii–xix.
[17] Richardson K, Weinberg A. Reduced immunogenicity of influenza vaccines inHIV-infected compared with uninfected pregnant women is associated withregulatory T cells. AIDS 2011;25:595–602.
[18] Shackelford PG, Granoff DM, Madassery JV, Scott MG, Nahm MH. Clinical andimmunologic characteristics of healthy children with subnormal serumconcentrations of IgG2. Pediatr Res 1990;27:16–21.
[19] Fried AJ, Bonilla FA. Pathogenesis, diagnosis, and management of primaryantibody deficiencies and infections. Clin Microbiol Rev 2009;22:396–414.
[20] Ramphal R, Cogliano RC, Shands Jr JW, Small Jr PA. Serum antibody preventslethal murine influenza pneumonitis but not tracheitis. Infect Immun1979;25:992–7.
[21] Palladino G, Mozdzanowska K, Washko G, Gerhard W. Virus-neutralizingantibodies of immunoglobulin G (IgG) but not of IgM or IgA isotypes can cureinfluenza virus pneumonia in SCID mice. J Virol 1995;69:2075–81.
[22] Logtenberg SJ, Pasma FH, Wolfhagen MJ, Dikkeschei LD, Bilo HJ. Disappearanceof immunoglobulins in acute phase of influenza A infection. Lancet2006;368:1546.
[23] Gordon CL, Johnson PD, Permezel M, Holmes NE, Gutteridge G, McDonald CF,et al. Association between severe pandemic 2009 influenza A (H1N1) virusinfection and immunoglobulin G(2) subclass deficiency. Clin Infect Dis2010;50:672–8.
[24] Chan JF, To KK, Tse H, Lau CC, Li IW, Hung IF, et al. The lower serumimmunoglobulin G2 level in severe cases than in mild cases of pandemic H1N12009 influenza is associated with cytokine dysregulation. Clin VaccineImmunol 2011;18:305–10.
[25] Zhou B, Zhong N, Guan Y. Treatment with convalescent plasma for influenza A(H5N1) infection. N Engl J Med 2007;357:1450–1.
[26] Fatemi SH, Folsom TD, Rooney RJ, Mori S, Kornfield TE, Reutiman TJ, et al. Theviral theory of schizophrenia revisited: abnormal placental gene expressionand structural changes with lack of evidence for H1N1 viral presence inplacentae of infected mice or brains of exposed offspring. Neuropharmacology2012;62:1290–8.