imaging of intracranial bleeds - lieberman's...
TRANSCRIPT

Head TraumaHead Trauma Imaging of Intracranial BleedsImaging of Intracranial Bleeds
Srishti Gupta, Harvard Medical School – Year IIIGillian Lieberman, MD
November 2000Srishti GuptaGillian Lieberman, MD

November 2000
2
Our PatientOur Patient
• 85 y/o woman fell at home, hitting R temple on corner of table
• ambulated then became unresponsive• In the ED . . .
– Patient lethargic– No external signs of injury– pupil size R 3.5 L 2.5 responsive to light– BP 208/palpable HR 112
Srishti GuptaGillian Lieberman, MD

November 2000
3
Menu of tests for imaging head traumaMenu of tests for imaging head trauma
1. Head CT2. Head MRINoncontrast Head CT is the test of choice as:• The patient is accessible if emergency resuscitation is needed• IV contrast is not needed• Fast• Great for identifying fractures and bone fragments• Great for identifying acute bleeds; they appear hyperdense• Great for evaluating edema and shift/herniation
Srishti GuptaGillian Lieberman, MD

November 2000
4
Bone is whiteCalcium is white;Acute hemorrhage is usually white
Brain parenchyma is light grey;White matter is darker than grey matter
CSF is very dark grey;Sulci, cisterns and ventricles
Air is black;Nasal cavity, sinuses, mastoid air cells
White
Light Grey
Charcoal Grey
Black
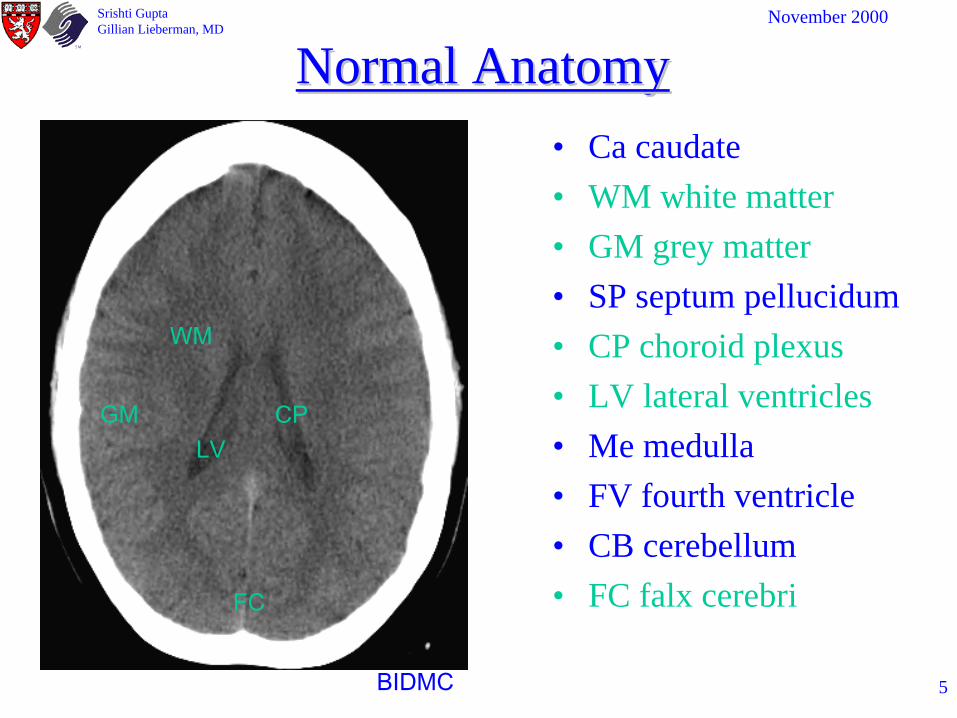
In order to recognize the abnormal, you first need to know the appearance of the normal.
On non-contrast head CT:
Srishti GuptaGillian Lieberman, MD
November 2000
5
Normal AnatomyNormal Anatomy• Ca caudate• WM white matter• GM grey matter• SP septum pellucidum• CP choroid plexus• LV lateral ventricles• Me medulla• FV fourth ventricle• CB cerebellum • FC falx cerebri
LV
FC
CP
WM
GM
BIDMC
Srishti GuptaGillian Lieberman, MD
November 2000
6
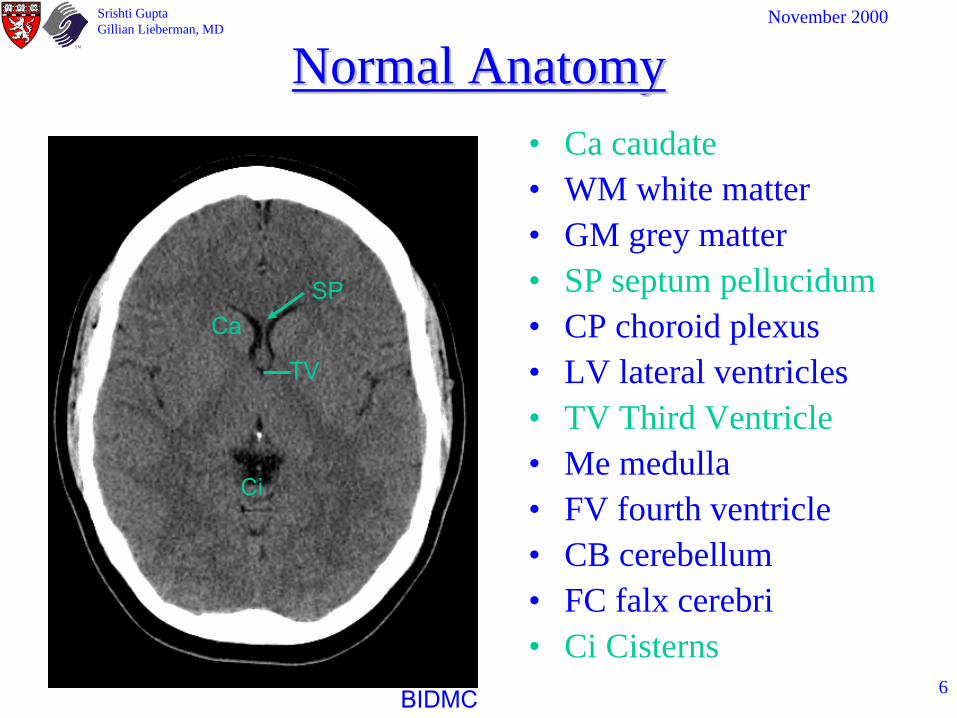
Normal AnatomyNormal Anatomy• Ca caudate• WM white matter• GM grey matter• SP septum pellucidum• CP choroid plexus• LV lateral ventricles• TV Third Ventricle• Me medulla• FV fourth ventricle• CB cerebellum • FC falx cerebri• Ci Cisterns
CaSP
TV
Ci
BIDMC
Srishti GuptaGillian Lieberman, MD

November 2000
7
Normal AnatomyNormal Anatomy• Ca caudate• WM white matter• GM grey matter• SP septum pellucidum• CP choroid plexus• LV lateral ventricles• Third Ventricle• Me medulla• FV fourth ventricle• CB cerebellum• FC falx cerebri
Me
CB FV
BIDMC
Srishti GuptaGillian Lieberman, MD

November 2000
8
Normal AnatomyNormal Anatomy• Sutures• Sinuses
– FS Frontal– EA Ethmoid Air Cells– SS Sphenoid– MS Maxillary– MA Mastoid Air Cells
• NA Nasal Airway• EC Ear Canal
FS
MA
BIDMC
Srishti GuptaGillian Lieberman, MD

November 2000
9
Normal AnatomyNormal Anatomy
• Sutures• Sinuses
– FS Frontal– EA Ethmoid Air Cells– SS Sphenoid– MS Maxillary– MA Mastoid Air Cells
• NA Nasal Airway• EC Ear Canal
EA
SS
MA
NA
EC
BIDMC
Srishti GuptaGillian Lieberman, MD
November 2000
10
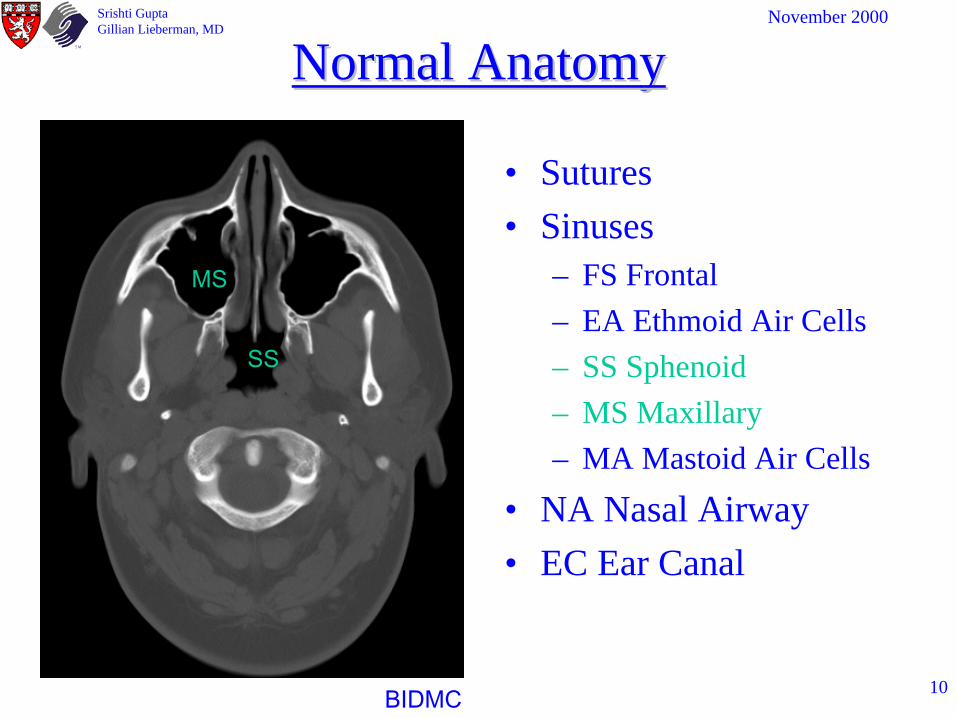
Normal AnatomyNormal Anatomy
• Sutures• Sinuses
– FS Frontal– EA Ethmoid Air Cells– SS Sphenoid– MS Maxillary– MA Mastoid Air Cells
• NA Nasal Airway• EC Ear Canal
MS
SS
BIDMC
Srishti GuptaGillian Lieberman, MD

November 2000
11
Systematic Approach to reading a Systematic Approach to reading a Head CTHead CT
I. Quality Control– Check patient name, study date, time– Check standard views are included
• properly positioned contiguous images from foramen to cranial vertex
• correct scanner settings; Brain W/L: 80/40 Bone W/L: 2000/350
– Determine if IV contrast was given
Srishti GuptaGillian Lieberman, MD

November 2000
12
Systematic Approach to reading a Systematic Approach to reading a Head CT (cont’d)Head CT (cont’d)
II. Check Brain Parenchyma• Check grey/white differentiation• Gyri• Look for blood• Surgeons need to know . . . (size of hematoma, extent of midline shift,
herniation)
III. Check CSF spaces: Ventricles, Cisterns and Sulci• CSF spaces (ventricles and cisterns)
– size, symmetry, midline shift– herniation
• Subfalcine – cingulate gyrus crosses falx• Transtentorial – temporal lobe into tentorial notch • Cerebellar – cerebellum into foramen magnum
Srishti GuptaGillian Lieberman, MD

November 2000
13
Systematic Approach to reading a Systematic Approach to reading a Head CT (cont’d 2)Head CT (cont’d 2)
IV. Check face and skull bones on bone windows– Do not confuse sutures with fracture especially in
pediatric patients
V. Check “air spaces”– Sinuses– Nasal airway– Ear Canals and Mastoid air cells
Srishti GuptaGillian Lieberman, MD

November 2000
14
A Head CT with out IV contrast was obtained on our patient. Let’s review it
first fast and then systematically.
Srishti GuptaGillian Lieberman, MD

November 2000
15BIDMC
Emergency Head CT w/o contrast 2h s/p fall. W/L: 80/40
November 2000Srishti GuptaGillian Lieberman, MD

November 2000
16
BIDMC
Emergency Head CT w/o contrast 2h s/p fall.W/L: 2000/350
November 2000Srishti GuptaGillian Lieberman, MD

November 2000
17
Our Patient’s Head CTOur Patient’s Head CT
• R frontoparietal subdural hematoma (6 mm)
• Midline marker• R temperoparietal epidural
hematoma (1.8 cm)• 6 mm leftward shift of lateral
ventricles• Right lateral ventricle• Left lateral ventricle• Effacement of R sulciBIDMC
Srishti GuptaGillian Lieberman, MD
Film findings:

November 2000
18
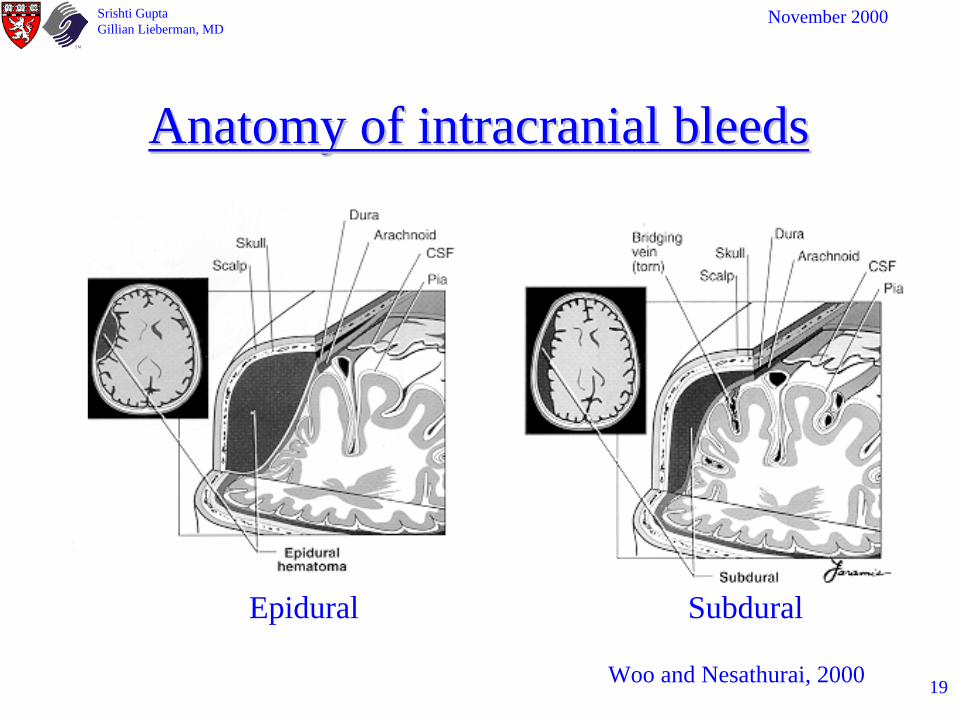
Locations for intracranial blood include:1. Epidural hemorrhage2. Subdural hemorrhage3. Subarachnoid hemorrhage4. Intraparenchymal hemorrhage
Differentiation between epidural and subdural maybe difficult
Srishti GuptaGillian Lieberman, MD
November 2000
19
Anatomy of intracranial bleedsAnatomy of intracranial bleeds
Woo and Nesathurai, 2000
Srishti GuptaGillian Lieberman, MD
Epidural Subdural
November 2000
20
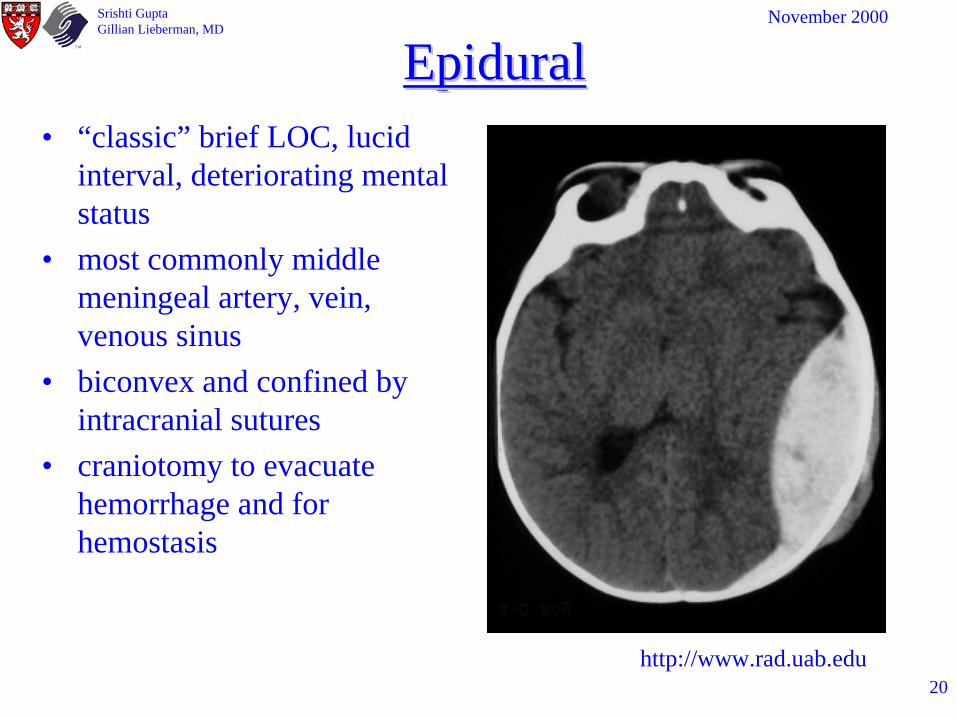
Epidural Epidural • “classic” brief LOC, lucid
interval, deteriorating mental status
• most commonly middle meningeal artery, vein, venous sinus
• biconvex and confined by intracranial sutures
• craniotomy to evacuate hemorrhage and for hemostasis
http://www.rad.uab.edu
Srishti GuptaGillian Lieberman, MD

November 2000
21
Subdural HematomaSubdural Hematoma• altered consciousness, pupil
abnormalities• shearing of bridging veins• concave, not confined by
sutures• mass effect can cause
herniation or reduced perfusion
• blood toxic effect on tissue• monitor ICP, high mortality
rate• acute, subacute, chronic or
combination depending on time of presentation
http://www.med.wayne.edu/diagRadiology/TF/Neuro/
Srishti GuptaGillian Lieberman, MD

November 2000
22
Subarachnoid HemorrhageSubarachnoid Hemorrhage• shearing of microvessels in
subarachnoid space• often benign in trauma• most commonly associated
with ruptured aneurysm “worst headache of my life”
• hyperdensities indicate blood in– interhemispheric fissure– suprasellar cistern– sylvian cistern– perimesencephalic cistern– ambient cistern– quadrageminal plate cistern
Araiza & Araiza, 1997
Srishti GuptaGillian Lieberman, MD

November 2000
23
ParenchymalParenchymal HemorrhageHemorrhage
• presents with behavioral and cognitive changes
• round or irregular high density lesions
• damage to small arterioles in brain parenchyma
• result from lacerations or coalescence of contusions
• often associated with coup countrecoup injuries
• most common in frontal and temporal lobes
http://www.xray2000.f9.co.uk/Ibase2/Brain/
Srishti GuptaGillian Lieberman, MD

November 2000
24
Potential Shortcomings of CT in the Potential Shortcomings of CT in the Imaging of Head TraumaImaging of Head Trauma
• Location of pathology– Temporal– Posterior Fossa
• Isointense bleeds– anemia– coagulopathies– dilution of blood with
CSF
http://www.med.wayne.edu/diagRadiology/TF/Neuro/
Srishti GuptaGillian Lieberman, MD
November 2000
25
Management PrioritiesManagement Priorities
Medical Therapy– diuretics– blood pressure control– elevation of head– seizure prophylaxis– sedation– mild hypothermia
Surgical– Ventriculostomy– Evacuation– Craniotomy
Maintain perfusion and oxygenation of brainICP at or below 15 mm Hg
Srishti GuptaGillian Lieberman, MD
November 2000
26
Patient’s coursePatient’s course
• AD taken emergently to OR for evacuation of R frontal temporal hematomas
• Significant improvement in neurological function post operatively
• Patient discharged to home on POD# 5 in stable condition
Srishti GuptaGillian Lieberman, MD

November 2000
27
Our Patient’s FollowOur Patient’s Follow--up scansup scans
POD #1
BIDMC BIDMC
Srishti GuptaGillian Lieberman, MD
s/p
evacuationOn presentation

November 2000
28
FollowFollow--up scansup scans
POD # 1
Craniotomydefects
SurgicalSubdural air
BIDMC BIDMC
Srishti GuptaGillian Lieberman, MD
s/p
evacuation

November 2000
29
SummarySummaryTYPE Clinical Signs CT signs
EPIDURAL Lucid interval followed by deteriorating mental status
biconvex (lentiform) confined by sutures
SUBDURALAltered consciousness, pupil abnormalities, can be gradual in onset
Bi concave, not confined by sutures
SUBARACHNOID“Worst headache of life” more often associated with aneurysm, HTN
Hyperdensities in cisterns (star pattern)
PARENCHYMALBehavioral and cognitive changes, coup countrecoup injuries
round or irregular hyperdense lesions
Srishti GuptaGillian Lieberman, MD

November 2000
30
Head Injury FactsHead Injury Facts• 8 million people in the U.S. suffer head
injury each year• 500,000 hospitalized• Leading causes MVA (50%) Falls (21%)• Leading cause elderly falls (75%)
• Please buckle up and wear helmets on bikes, scooters, and rollerblades.
Srishti GuptaGillian Lieberman, MD
November 2000
31
ReferencesReferences• Grossman R. I., Yousem D. M. Neuroradiology: The Requisites 1st edition, 1994• Woo B.H., Nesathurai S. The Rehabilitation of People with Traumatic Brain Injury 1st edition, 2000• Novelline, R. A. Squire’s Fundamentals of Radiology 5th edition, 1997• Kushner D. “Mild Traumatic Brain Injury: Understanding Manifestations and Treatment” Archives
of Internal Medicine 158 (15) 1617-24• Haydel MJ, Preston CA, Mills TJ, Luber S, Blaudeau E, DeBlieux PMC “Indications for computed
tomography in patients with minor head injury “ NEJM 343 (2):100, 2000• Araiza J., Araiza B. “Neuroimaging” Emergency Medicine Clinics of North America 15 (3), 1997• http://www.radiology.wisc.edu/Med_Students/neuroradiology/NeuroRad/NeuroRad.htm• http://brighamrad.harvard.edu/education.html• Johnson KA & Becker JA, http://www.med.harvard.edu/AANLIB/home.html• http://www.neuropat.dote.hu/nrad2.htm• Zapawa,JE & Alcantara AL,
http://www.med.wayne.edu/diagRadiology/Anatomy_Modules/brain/brain.html• http://www.med.wayne.edu/diagRadiology/TF/Neuro/NeuroTF.html• http://www.rad.uab.edu• http://www.xray2000.f9.co.uk/Ibase2/Brain/
Srishti GuptaGillian Lieberman, MD

November 2000
32
AcknowledgementsAcknowledgements
• Vasant Narasimhan• Daniel Saurborn M.D.• Wayne Monsky M.D.• Beverlee Turner for her support and
PowerPoint expertise.
The end.The end.
Srishti GuptaGillian Lieberman, MD