imaging ischemic heart disease role of echocardiography · pdf fileimaging ischemic heart...
TRANSCRIPT

Imaging Ischemic Heart Disease
Role of Echocardiography
Danilo NegliaFTGM, Pisa, Italy
Chair NC&CCT SectionVice-President EACVI
Thanks to:Eugenio Picano, Rosa Sicari and Emilio PasanisiIFC CNR and FTGM, Pisa, Italy
Fausto Rigo Mestre-Venezia Hospital, Italy
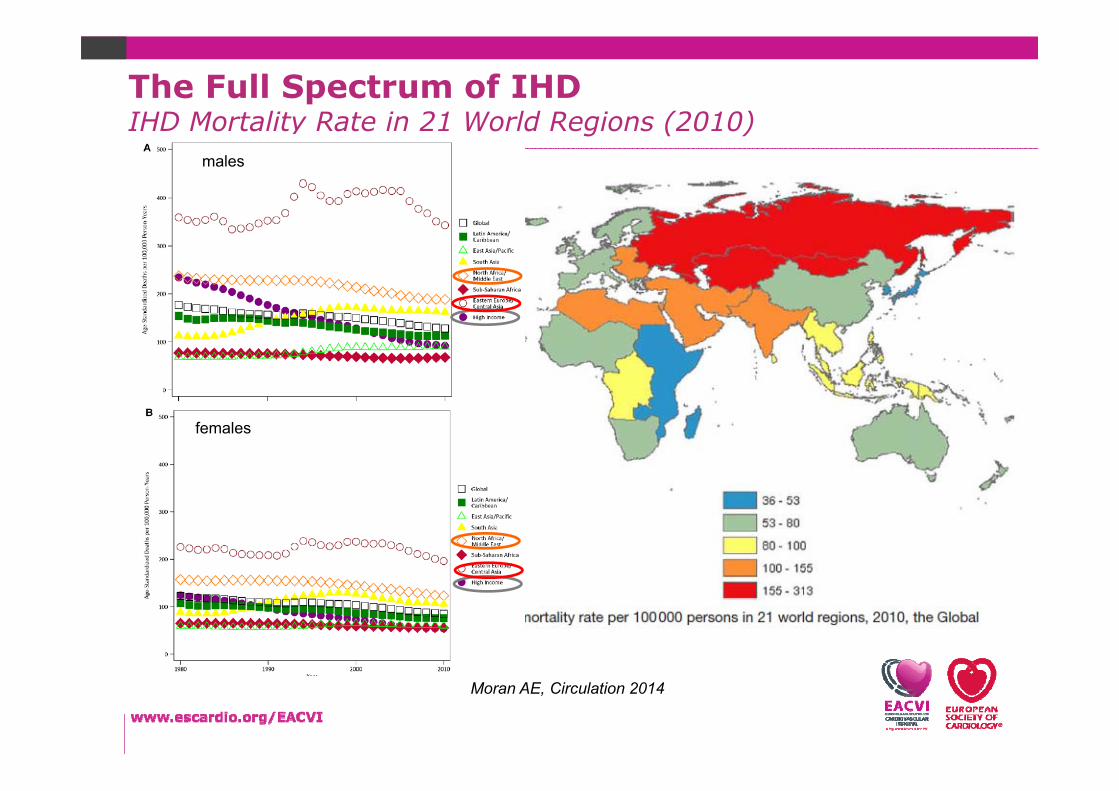
The Full Spectrum of IHDIHD Mortality Rate in 21 World Regions (2010)
males
females
Moran AE, Circulation 2014
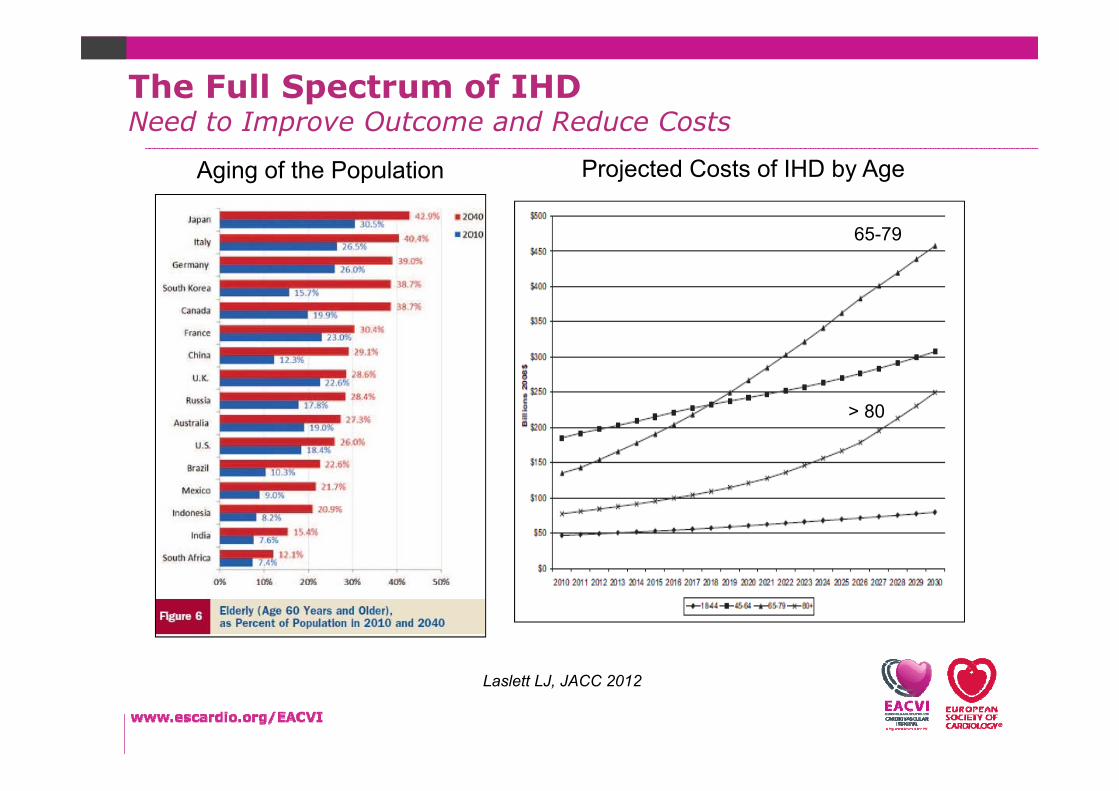
Aging of the Population Projected Costs of IHD by Age
65-79
> 80
The Full Spectrum of IHDNeed to Improve Outcome and Reduce Costs
Laslett LJ, JACC 2012

Danilo Neglia
Cardiovascular ImagingNeed for “WISE and PERSONALIZED” use in clinical practice
Increase in use: 70% (in 2000‐2007)Patients: 10 million /yearCosts: $ 80 billion /year
Shaw LJ…and Douglas PS, JACC Cardiovascular Imaging 2010
ACS
Stable IHD

Speaker
SuspectedACS
STEMI
ST/T wavechanges
Normalundiagnostic
ICAPCI
2D-ECHO for DD(Pulm. Embol./AorticDiss./Pericardial Eff.)
Hs-Tn > 99°percentile
Hs-Tn <= 99°percentile
ECG hs-Tn Testing (0-3 hours) Clinical/ECG
On-GoingChest Pain
No On-GoingChest Pain
< 20% increaseStable
< 50% increse
Cardiac Imaging/Invasive
SIGNIFICANTHigh ValuesOr Increase
2D-ECHO (Resting WM) (in-patient testing)
2D-ECHO (Resting WM) StressECHO (Stress WM)(in-or-outpatient testing)
Modified from Garg P et al. , Nature Reviews 2016
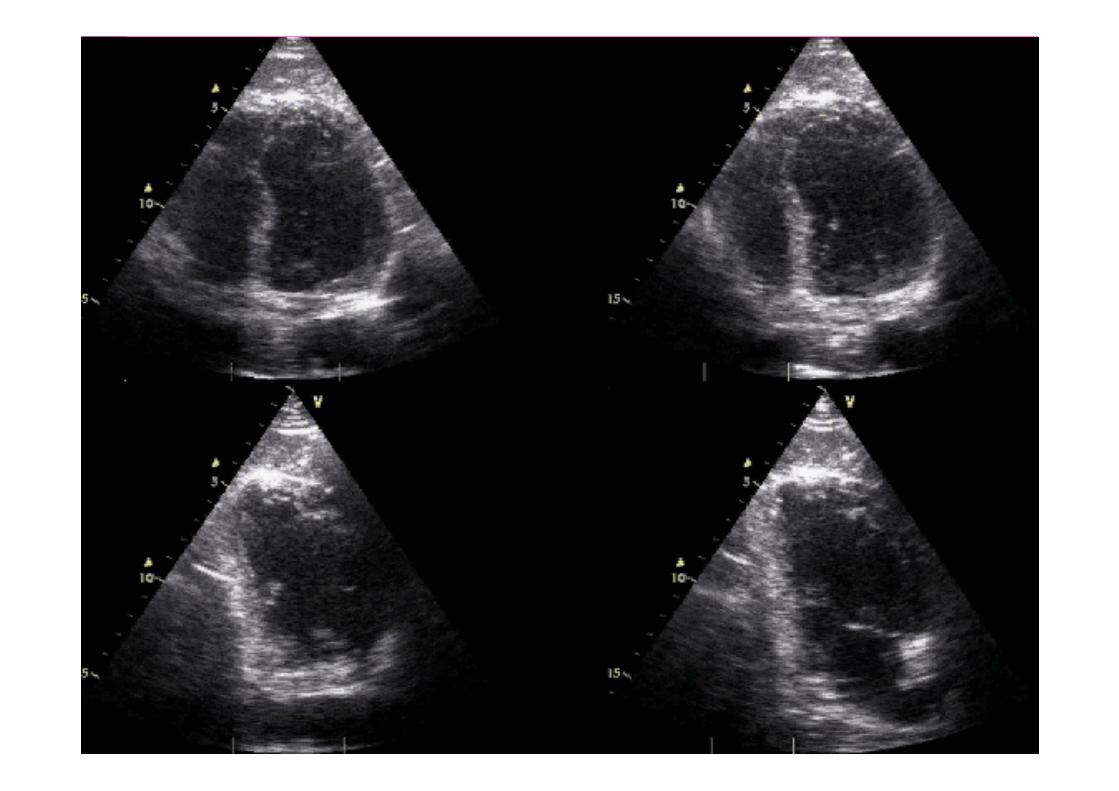
Acute Coronary SyndromesRole of Echocardiography in Suspected ACS

Garg P et al. , Nature Reviews 2016
Acute Coronary SyndromesRole of Echocardiography in Suspected ACS

Speaker
Acute Coronary SyndromesRole of Echocardiography in Suspected ACS
Speaker
Acute Coronary SyndromesRole of Echocardiography in Suspected ACS
Take Home Messages
2D-ECHO can complement history, ECG, and cardiac biomarkers for timely identification or ruling out of acute coronary syndrome (ACS). It is the first-line imaging test in patients with suspected ACS
ADVANTAGESBedside, widely available, low cost, RCT supported, Strain technique and Contrast ECHO might improve accuracy and prognostic information
Stress ECHO adds diagnostic and prognostic value in patients with suspected ACS (with inconclusive ECG, clinical and biomarkers findings). Exercise ECHO is superior to EET (and similar to exercise MPS) in risk stratification
LIMITATIONSPoor acustic window, contraindications to pharmacological stress, available only in centers with expertise in stress ECHO.
Redrawn from Gould et al Am J Cardiol 1974
2
4
6
EXERCISE Myocardial Oxygen Consumption
Myocardial B
lood
Flow
Detection of CAD‐IHDImaging

Coronary
Atherosclerosis
Medical TreatmentATS
Obstructive
CAD
Medical TreatmentRevascularization
CAD
Endothelial/Microvascular
Dysfunction
Medical TreatmentRisk Factors
Myocardial
Damage/Dysfunction
Medical TreatmentDevices
Heart Failure
Scar
Stable Ischemic Heart DiseaseRole of Non-Invasive Imaging
Myocardial
Ischemia
Medical TreatmentIschemia
Diagnosis >> Treatment >> Outcome
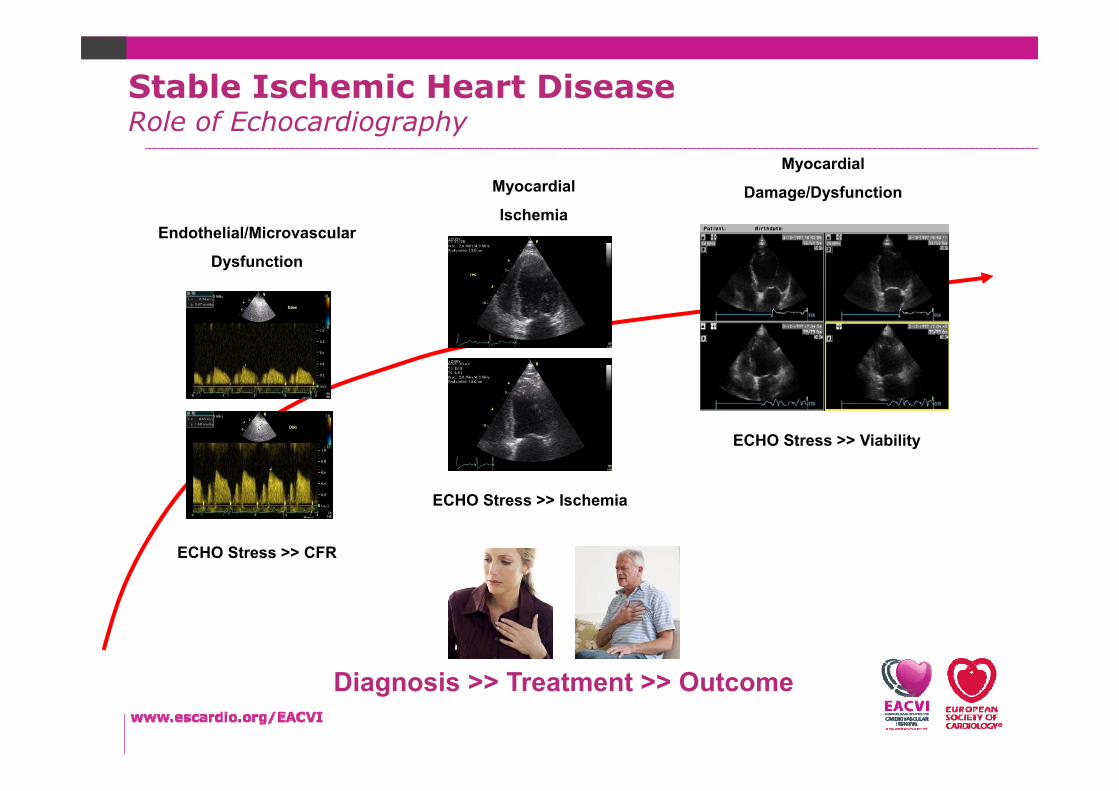
Endothelial/Microvascular
Dysfunction
ECHO Stress >> CFR
Myocardial
Damage/Dysfunction
ECHO Stress >> Viability
Myocardial
Ischemia
ECHO Stress >> Ischemia
Diagnosis >> Treatment >> Outcome
Stable Ischemic Heart DiseaseRole of Echocardiography
Male 65 yrs – Recent onset Typical AnginaHypercholesterolemia, Hypertension
Is Ischemic Heart Disease causing his SYMPTOMS?
Which is his LIFE RISK?
Which TREATMENT does he require to improve
SYMPTOMS and reduce RISKS?
Which are the MECHANISMS?


Pre-Test Probability of CAD D&F (Genders)

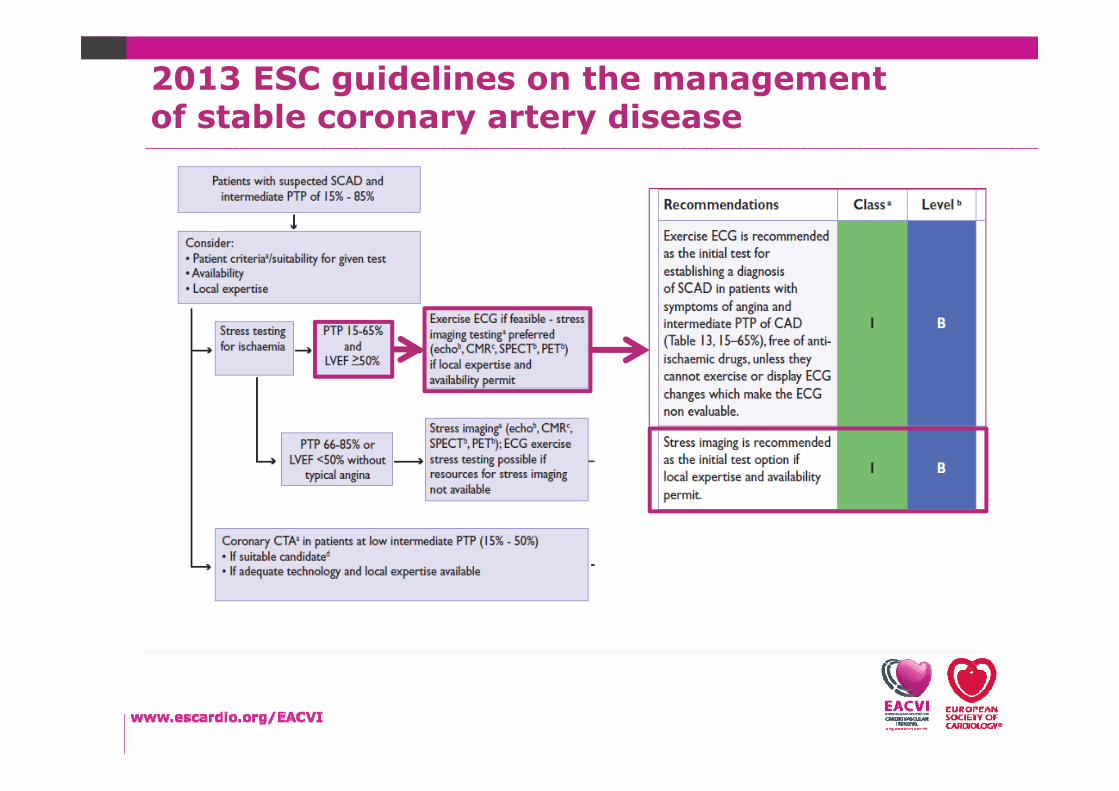
2013 ESC guidelines on the managementof stable coronary artery disease

Stress Echo Lab (Exercise)
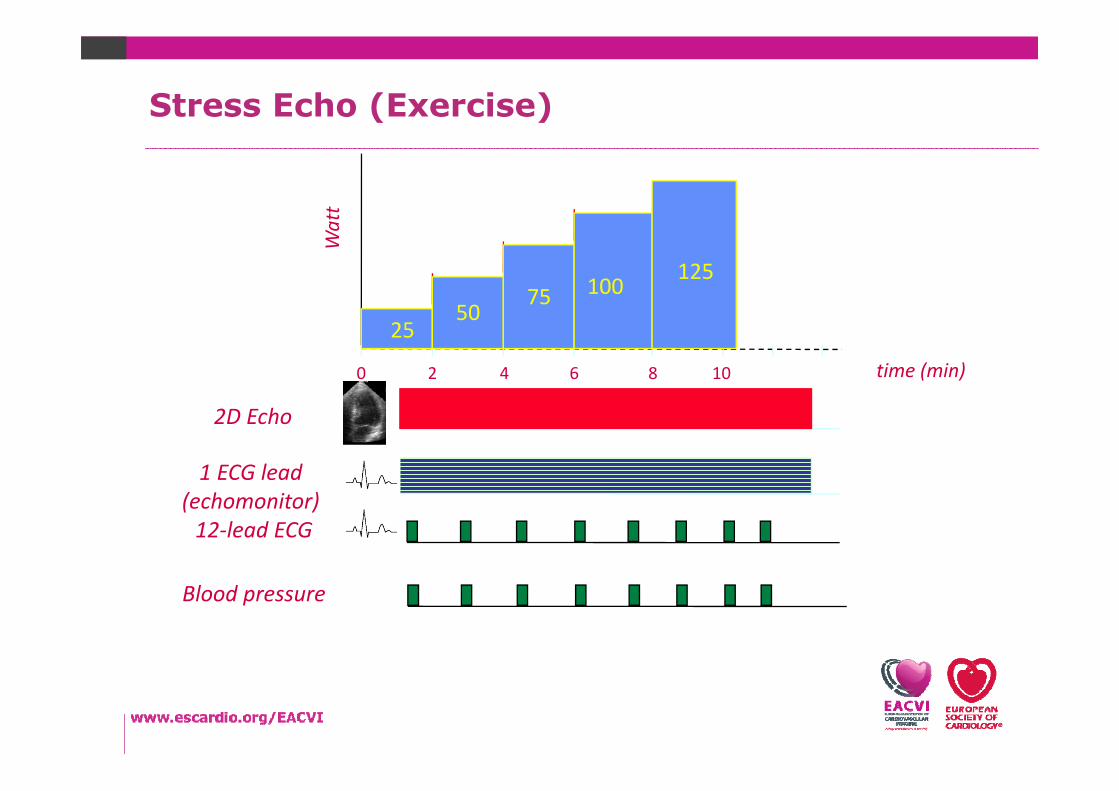
2D Echo
Blood pressure
12‐lead ECG
1 ECG lead(echomonitor)
time (min)0 108642
2550
75 100 125
Watt
Stress Echo (Exercise)

Exercise Stress EchoPositive WM (3 segments)
rest peak
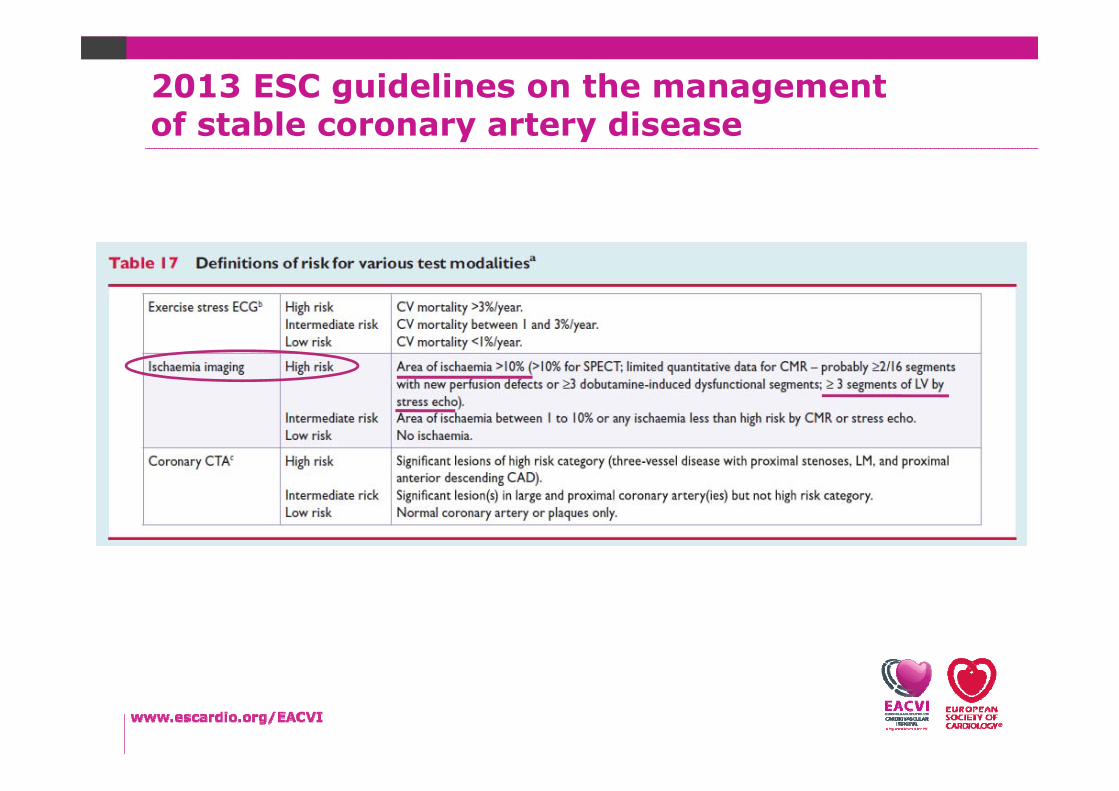
2013 ESC guidelines on the managementof stable coronary artery disease

Hachamovitch R, et al. Circulation. 2003
Revascularization reduces mortality only in the presence of large perfusion defects
Non Invasive detection of HIGH RISK CAD Efficacy of Revascularization
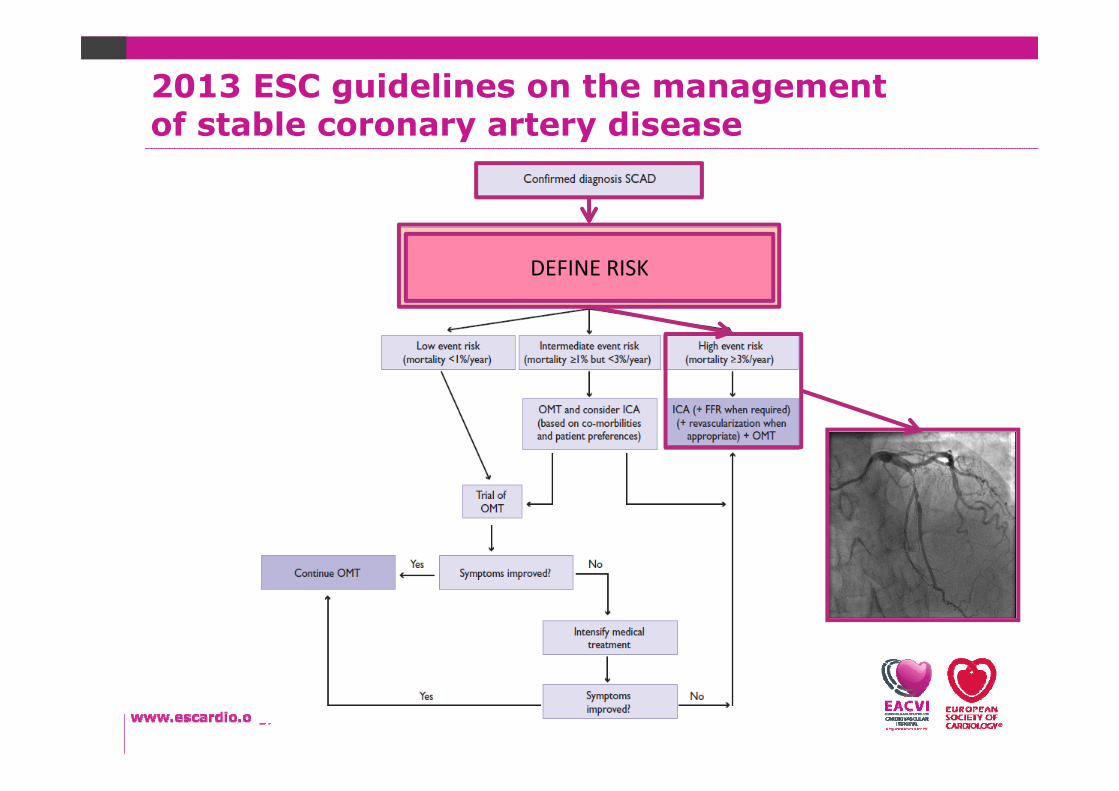
2013 ESC guidelines on the managementof stable coronary artery disease
DEFINE RISK
Speaker
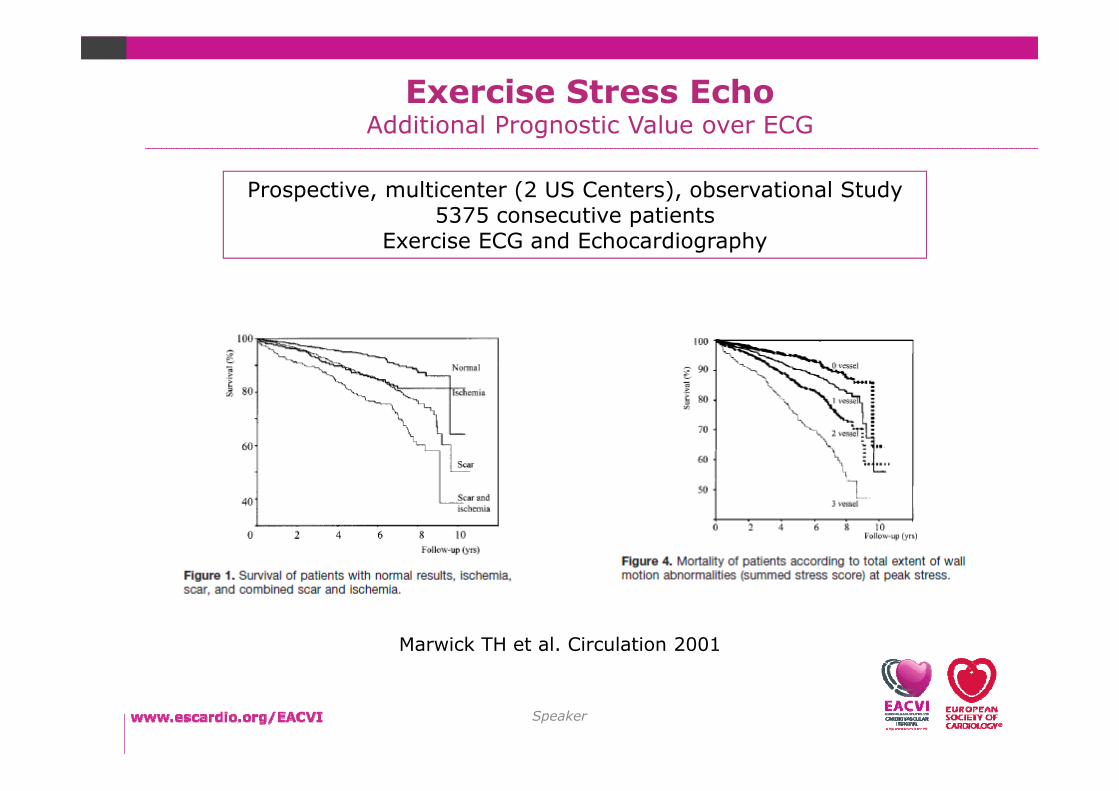
Exercise Stress EchoAdditional Prognostic Value over ECG
Marwick TH et al. Circulation 2001
Prospective, multicenter (2 US Centers), observational Study 5375 consecutive patients
Exercise ECG and Echocardiography

Male 65 yrs – Recent onset Typical AnginaHypercholesterolemia, Hypertension
Is Ischemic Heart Disease causing his SYMPTOMS?
Which is his LIFE RISK?
Which TREATMENT does he require to improve
SYMPTOMS and reduce RISKS?
Which are the MECHANISMS?
Yes
Obstructive CAD
High
Revascularization

Female 55 yrs – Atypical AnginaHypertension, Post-traumatic Hip Prothesis
Is Ischemic Heart Disease causing her SYMPTOMS?
Which is her LIFE RISK?
Which TREATMENT does she require to improve
SYMPTOMS and reduce RISKS?
Which are the MECHANISMS?
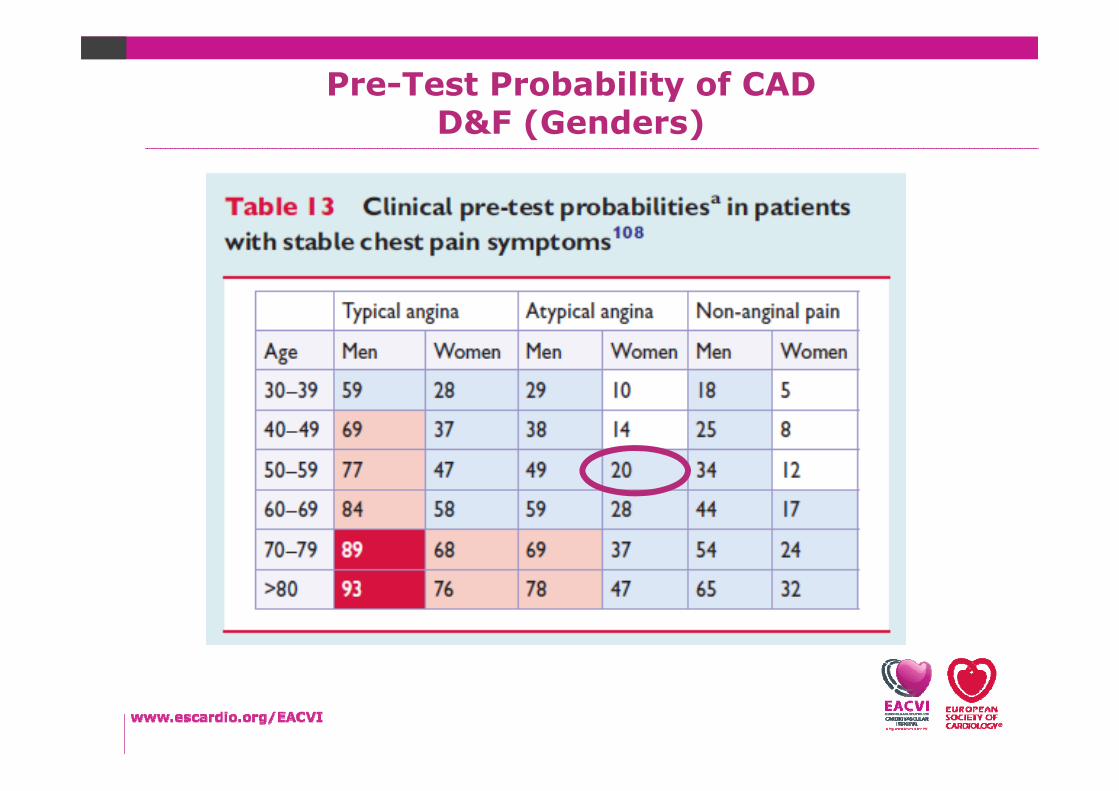
Pre-Test Probability of CAD D&F (Genders)
2013 ESC guidelines on the managementof stable coronary artery disease

Stress Echo Lab (Pharmacological)

0 6 10 min
DIP 0.84 mg/kg in 6’
TIMELINE
1 lead ECG
12 lead ECG
BP recording
Drugs infusion AMINO 120 mg in 1’ (up to 240 mg in 2’)
CFR‐PW
2D echo
Continuous monitoringand Pulsed recording
Continuous monitoringand Pulsed recording
on the echo‐monitor
Stress Echo (Dipyridamole)
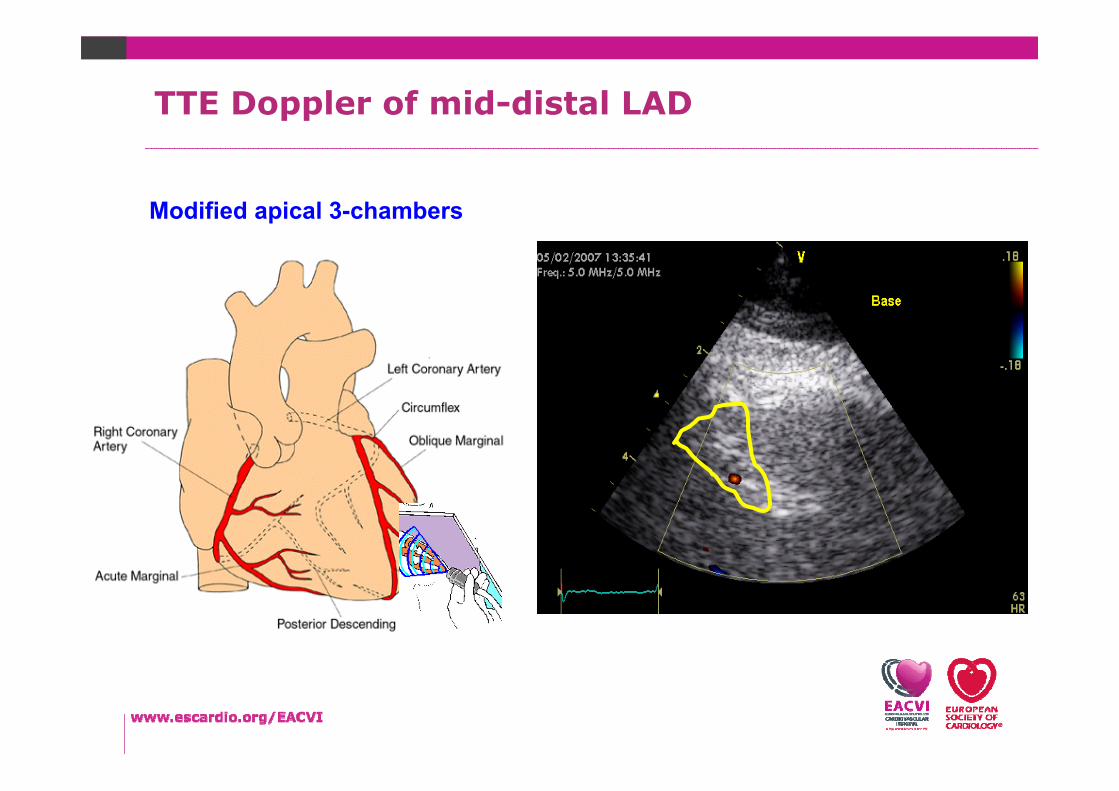
Modified apical 3-chambers
TTE Doppler of mid-distal LAD
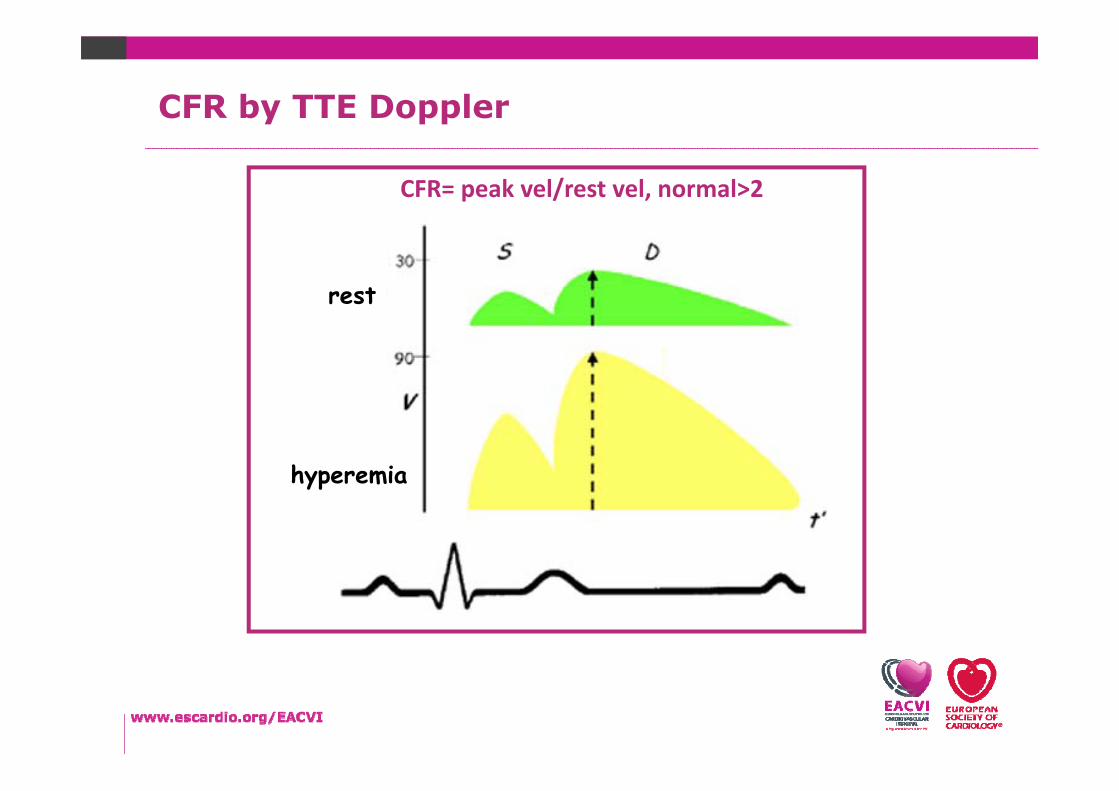
rest
hyperemia
CFR= peak vel/rest vel, normal>2
CFR by TTE Doppler
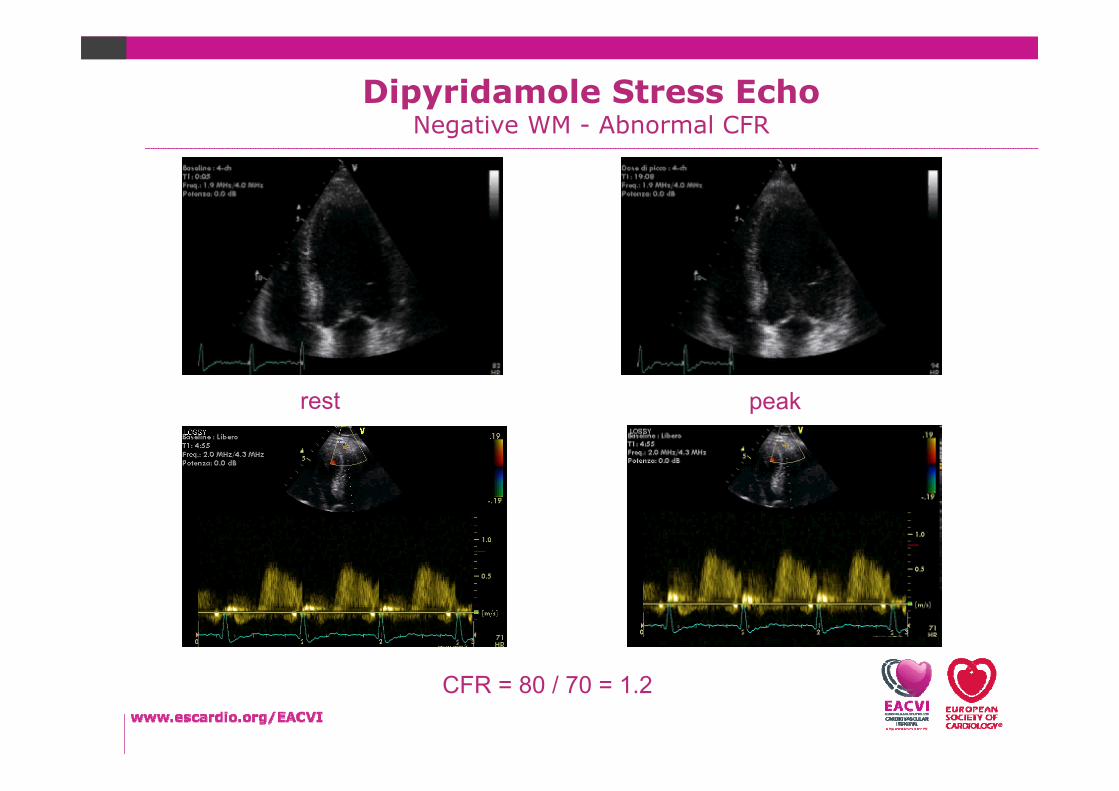
Dipyridamole Stress EchoNegative WM - Abnormal CFR
CFR = 80 / 70 = 1.2
rest peak
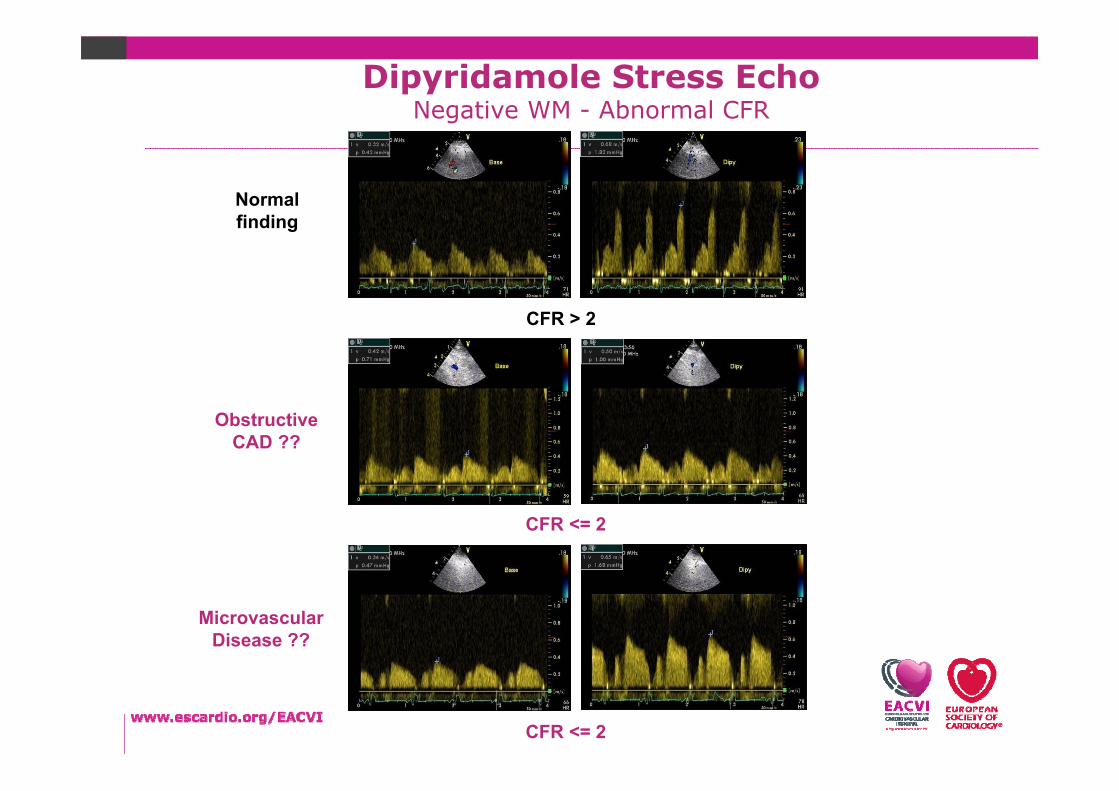
CFR > 2
Normal finding
Obstructive CAD ??
CFR <= 2
MicrovascularDisease ??
CFR <= 2
Dipyridamole Stress EchoNegative WM - Abnormal CFR

2013 ESC guidelines on the managementof stable coronary artery disease

Speaker
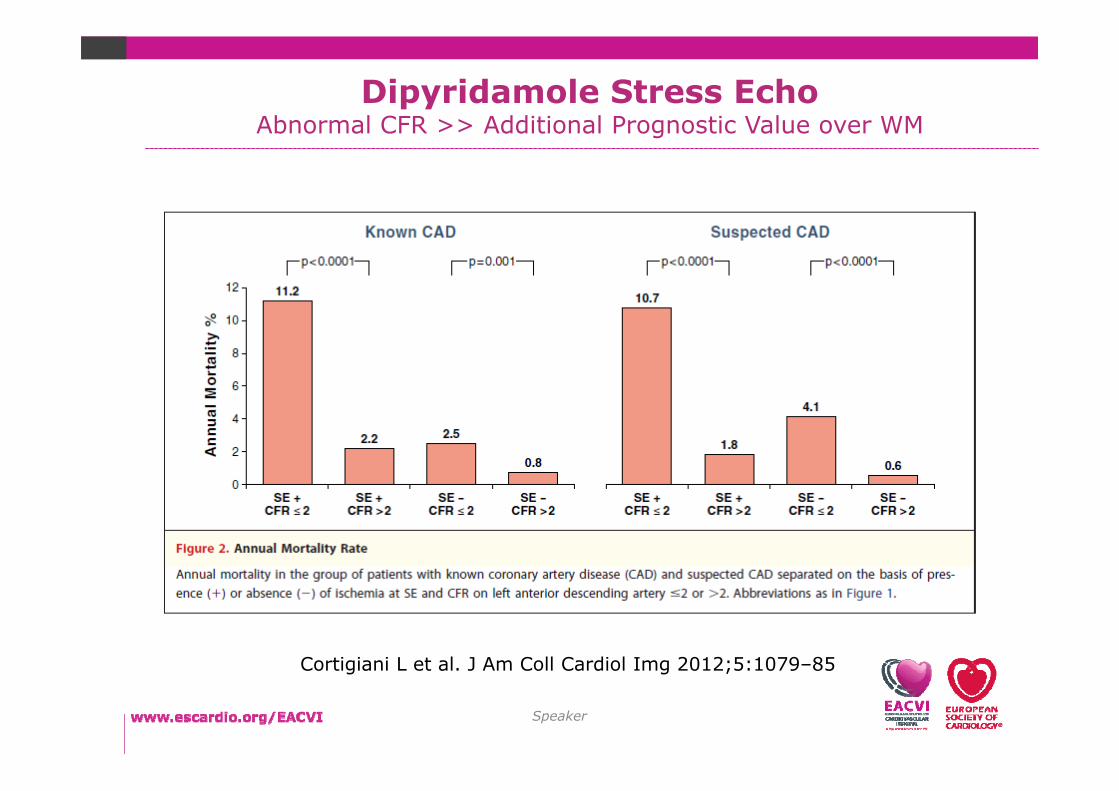
Prospective, multicenter, observational study
4,313 patientsknown CAD (n 1,547)
suspected CAD (n � 2,766)
High-dose Dip Stress ECHO CFR evaluation of LAD by Doppler
CFR on LAD is a strong and independent
indicator of mortality, over wall motion analysis, in patients with
known or suspected CAD. A negative result confers an annual risk of death <1% in
both patient groups.
(J Am Coll Cardiol Img 2012;5:1079–85)
Dipyridamole Stress EchoAbnormal CFR >> Additional Prognostic Value over WM
Speaker
Dipyridamole Stress EchoAbnormal CFR >> Additional Prognostic Value over WM
Cortigiani L et al. J Am Coll Cardiol Img 2012;5:1079–85
Female 55 yrs – Atypical AnginaHypertension, Post-traumatic Hip Prothesis
Is Ischemic Heart Disease causing her SYMPTOMS?
Which is her LIFE RISK?
Which TREATMENT does she require to improve
SYMPTOMS and reduce RISKS?
Which are the MECHANISMS?
Yes
Microvascular Coronary Disease
Intermediate
Medical

Dorbala S and Shaw LJ, J Nucl Cardiol 2016

2D Echo
Blood pressure
12‐lead ECG
1 ECG lead(echomonitor)
time (min)0 20156 9 10 123 5
510
2030
Dose
5
1020
3040
ischemia
viability
Stress Echo (Dobutamine)
Speaker
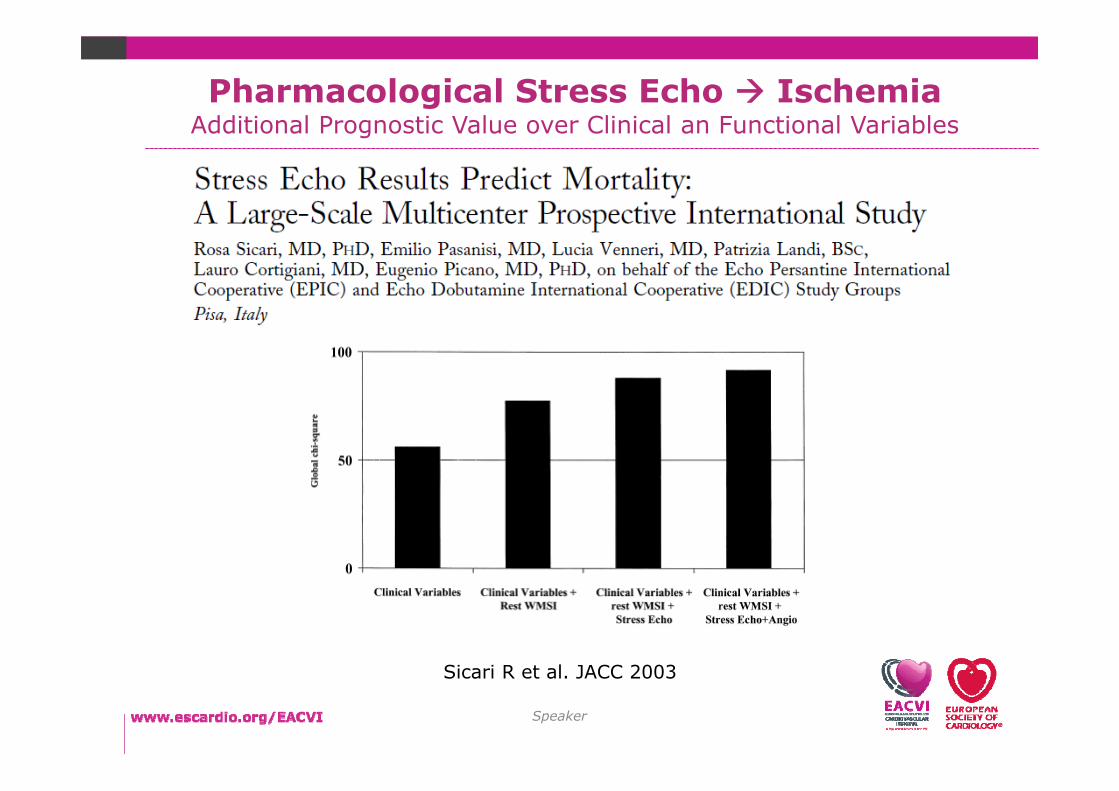
Pharmacological Stress Echo IschemiaAdditional Prognostic Value over Clinical an Functional Variables
Sicari R et al. JACC 2003

Speaker
Dobutamine Stress EchoViability
Speaker
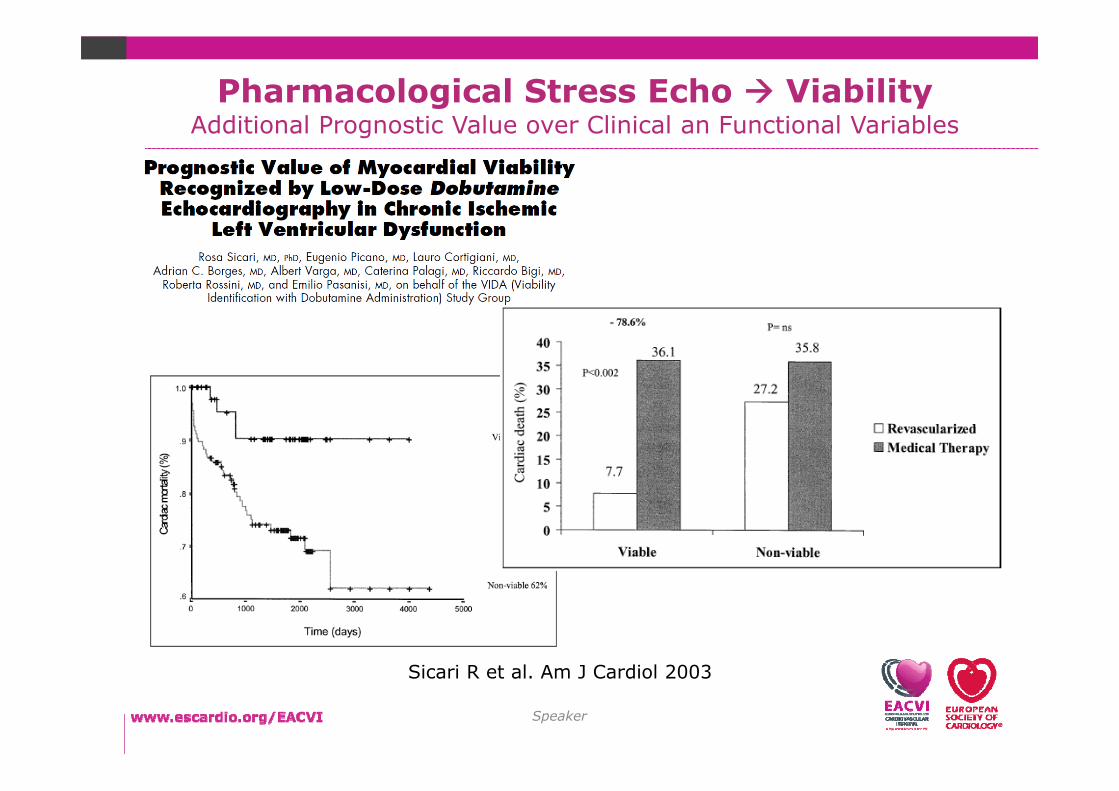
Pharmacological Stress Echo ViabilityAdditional Prognostic Value over Clinical an Functional Variables
Sicari R et al. Am J Cardiol 2003

Speaker
2013 ESC guidelines on the managementof stable coronary artery disease
Speaker
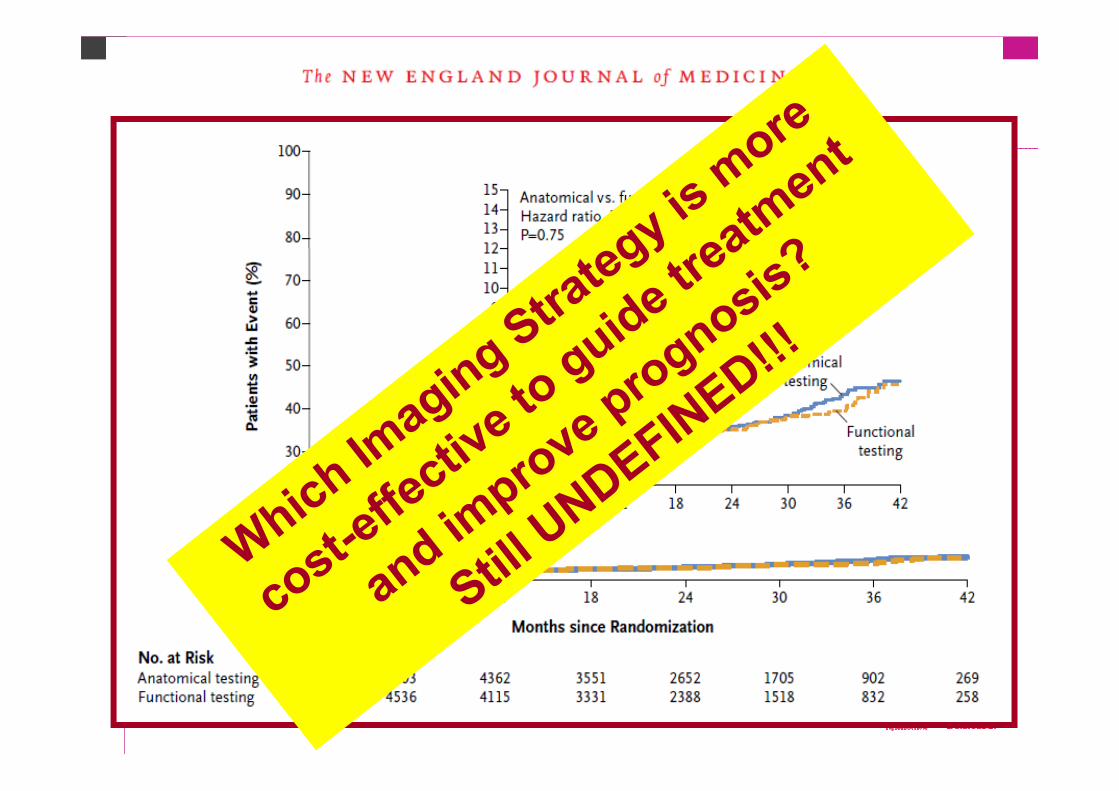
Comparative DIAGNOSTIC performance
Comparative impact on OUTCOME
Comparative COST-EFFECTIVENESS
OPEN ISSUES in STABLE IHDECHO and Non-Invasive Imaging

Taquety VR and Di Carli MFProgress in CV Diseases, 2015
The “Ischemic” CascadeEchocardiography
Sentitivity Specificity

Performance of Diagnostic Tests in TrialsRetrospective or Prospective studies comparing 1 or 2 modalities Patients with ~50% prevalence of disease (>50% stenosis at ICA)
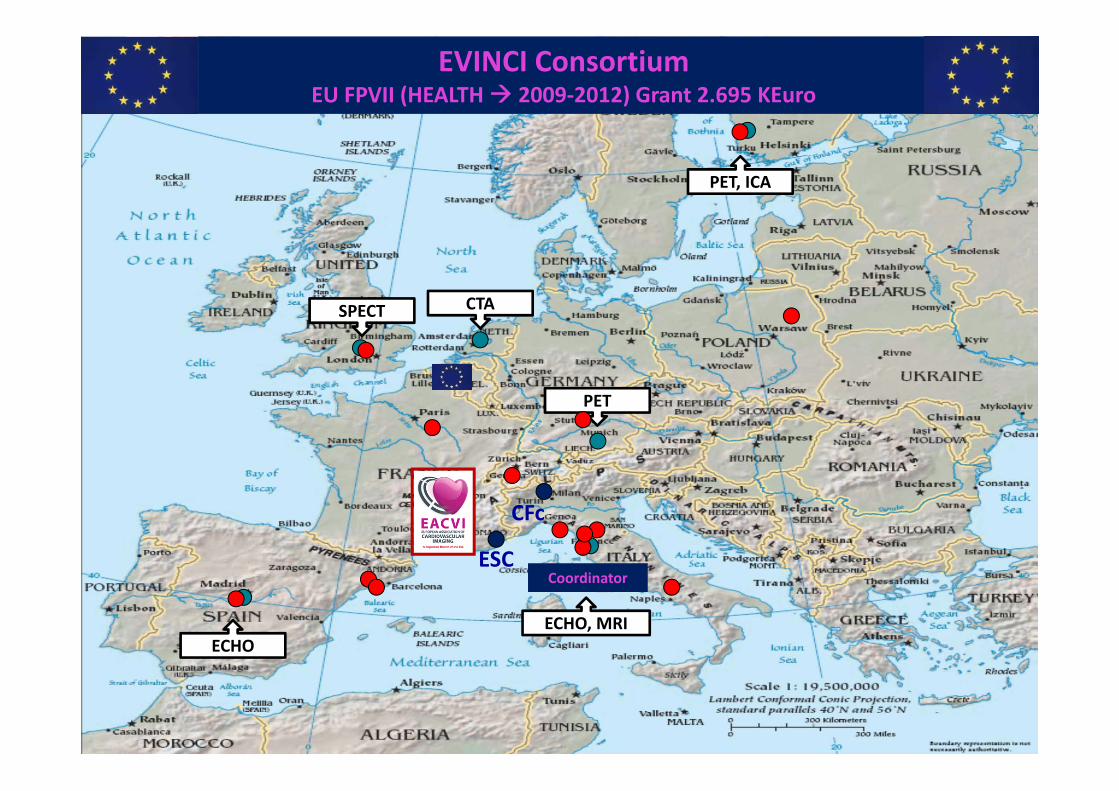
CFc
Coordinator
PET, ICA
ECHO
CTASPECT
ECHO, MRI
PET
EVINCI ConsortiumEU FPVII (HEALTH 2009‐2012) Grant 2.695 KEuro
ESC

65%49 %
29%15%
0
20
40
60
80
D&F Probability
Genders Probability
Prevalence Significant
CAD
Prevalence High Risk CAD
Revascularized20%
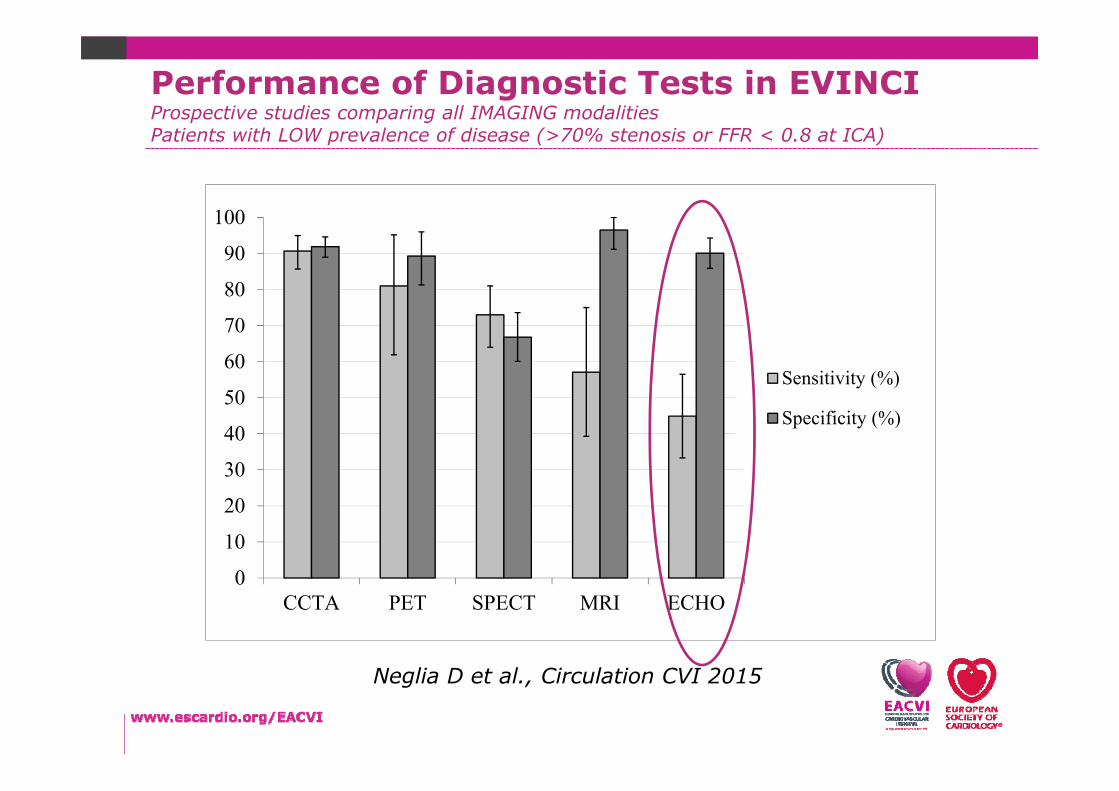
Performance of Diagnostic Tests in EVINCI Prospective study comparing all IMAGING modalities Patients with LOW prevalence of disease (>70% stenosis or FFR < 0.8 at ICA)
Neglia D et al., Circulation CVI 2015
0
10
20
30
40
50
60
70
80
90
100
CCTA PET SPECT MRI ECHO
Sensitivity (%)
Specificity (%)
Neglia D et al., Circulation CVI 2015
Performance of Diagnostic Tests in EVINCI Prospective studies comparing all IMAGING modalities Patients with LOW prevalence of disease (>70% stenosis or FFR < 0.8 at ICA)

0
20
40
60
80
100
120
SensSpec
Taquety VR and Di Carli MFProgress in CV Diseases, 2015
0
20
40
60
80
100
120
CCTA SPECT PET Hybrid ECHO CMRwm
SensSpec
Neglia D et al. EVINCI Trial Circulation CVI 2015Liga R et al. EHJ CVI 2016
Metanalyses
EVINCI Trial
Performance of Diagnostic Tests in EVINCI Comparison with recent Metanalyses
Frequent suboptimal imaging protocol: Sub-maximal stresswas reported in 41% of Echo examinations and 23% ofpatients remained on medical therapy
Lack of quantitative measurements: MBF by PET, perfusionby CMR and CFR by TTE-Doppler were not included in the mainanalysis
Population: low prevalence of High Risk CAD
Primary End-Point: did not include criteria for High Risk CAD
EVINCI Study: ECHO Limitations
Neglia D et al., Circulation CVI 2015

The 5 years EVINCI Follow-up will be presented at AHA 2016!

Patients withLow‐IntermediateProbability of CAD
CTCA Stress Imaging ICA PCI/CABG
OMT
OMT
+ +
-
OMT
-
+
OMT
-
EVINCI Study: Health-Economic Analysis
The EVINCI H-E Analysis will be presented at AHA 2016!
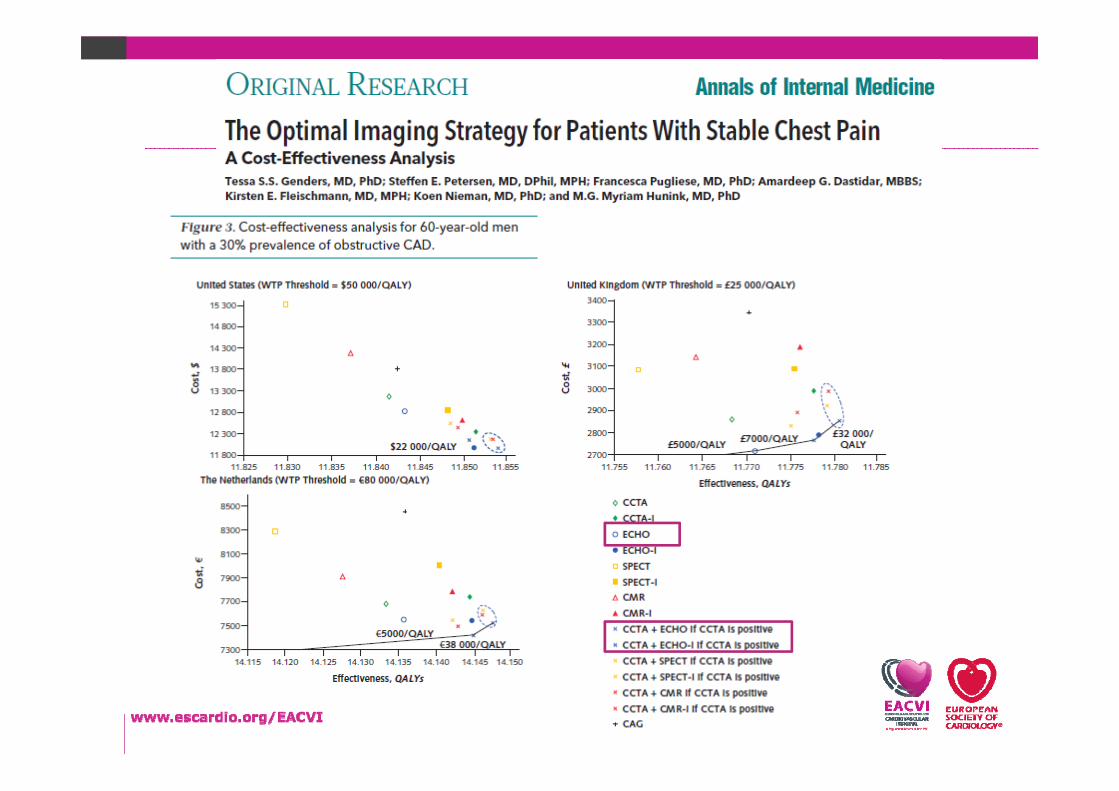

Exciting advances are occurring faster thanevidence can accumulate and are increasing health care
costs.
A joint effort by all stakeholders, including cardiologists,radiologists, nuclear imaging scientists, professional societies,
policy makers, and industry partners, is required.
The evidence base must be improved in order to evaluate thecomparative cost effectiveness of imaging-based decisionmaking on outcomes, quality of life, cost-effectiveness, and
downstream resource utilization. Shaw LJ, JACC 2010
The Integration of Cardiovascular ImagingNeed for “Discussing” and “Promoting” New Research
Danilo Neglia
Danilo Neglia
The EACVI Team Thanks

Teaching Courses 2016
Nuclear Cardiology in Practice 2016• European Heart House, Nice
November 17-19
Teaching Course Cardiac CT• EuroECHO Congress, Liepzig
December 7
eduCAD WEB & LIVE• www.educad.org• Ekaterinburg – September 23• Pisa – November 21• Minsk – December
Danilo Neglia
EuroEcho-Imaging 20167-10 December 2016 Leipzig,
GERMANY

7-9 May 2017, Vienna AUSTRIA
Call for abstracts & clinical cases15 Sept – 21 Nov 2016
Early registration fee deadline 27 February 2017
ICNC 2017

Speaker

The Integration of Cardiovascular ImagingNeed for a “Integrating Competence” in Cardiac Imaging
Danilo Neglia
Lancellotti P, EHJ 2015

www.educad.org • EVINCI study consortium• ESC‐EACVI• GE healthcare
New Contract EACVI‐GEHC:Health‐Economics, TranslationsOne new case per monthE‐Learning (CME)
Educational tool focused on the appropriateness of the diagnostic pathway
32000 visits930 users training on eduCAD clinical cases
54% from European countries27% .com15% .net4% not EuropeanC
EVINCI Study:WEB eduCAD 2016-2017

0
20
40
60
80
100
CTCA‐PET CTCA‐SPECT CTCA‐CMR CTCA‐ECHO
ICA Avoided (TN)
Diagnosis Done (TP)
Diagnosis Lost (FN)
ICA Unuseful (FP)
Number of Patients (over 100 with suspected CAD)
EVINCI Study: Integrated Imaging Strategies
Neglia D et al., Circulation CVI 2015