imaging abdomen trauma liver part 2 dr ahmed esawy
TRANSCRIPT


An Article By
Dr. Ahmed Esawy
MBBS M.Sc MD


Of all patients with blunt trauma to the
abdomen, about 15% to 20% involves the
liver. Isolated injuries to the liver occur in
less than 50% of blunt trauma victims.
LIVER TRAUMA

CT CRITERIA FOR STAGING
LIVER TRAUMA BASED ON
THE AAST (AMERICAN
ASSOCIATION OF
SURGEONS IN TRAUMA)
LIVER INJURY SCALE
INCLUDE THE FOLLOWING:
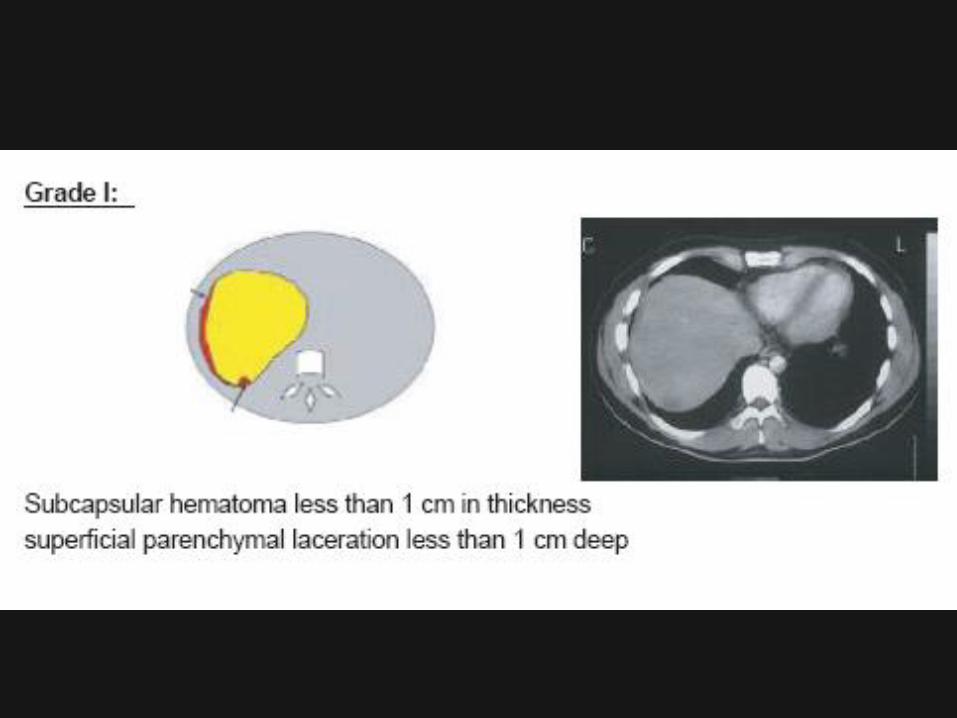




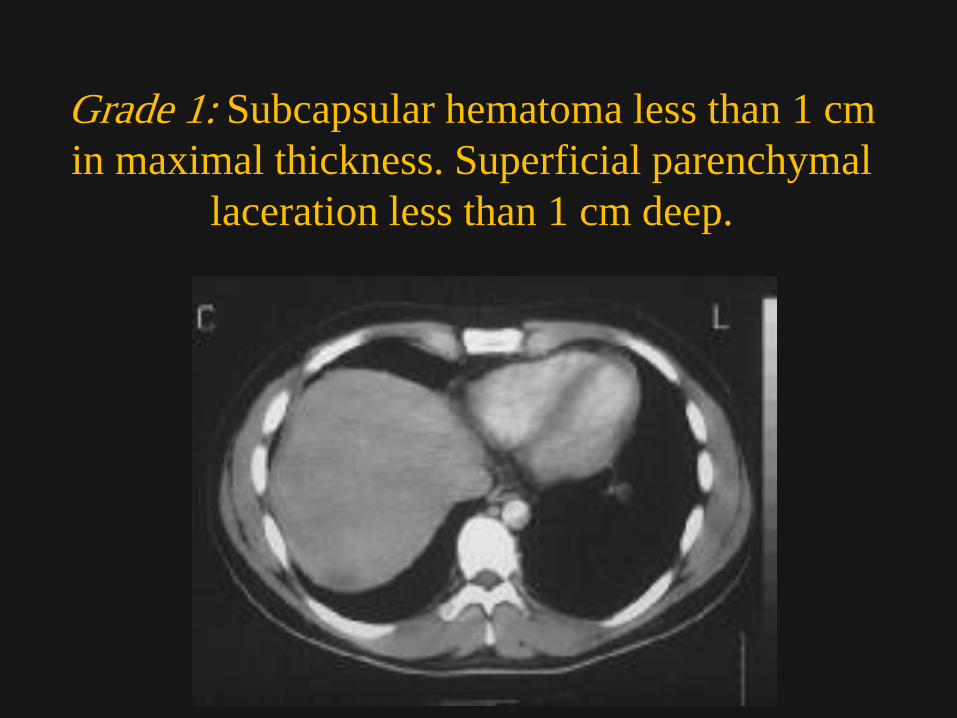
Grade 1: Subcapsular hematoma less than 1 cm
in maximal thickness. Superficial parenchymal
laceration less than 1 cm deep.

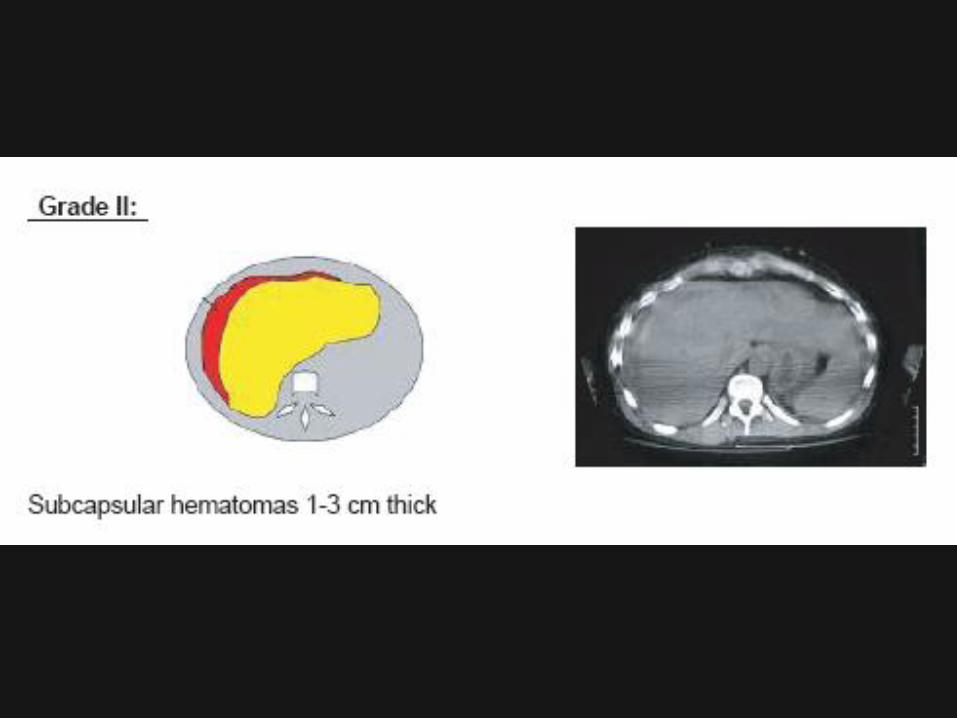
Grade 2: Parenchymal laceration 1-3 cm deep
and parenchymal/subcapsular hematomas 1-3 cm
thick

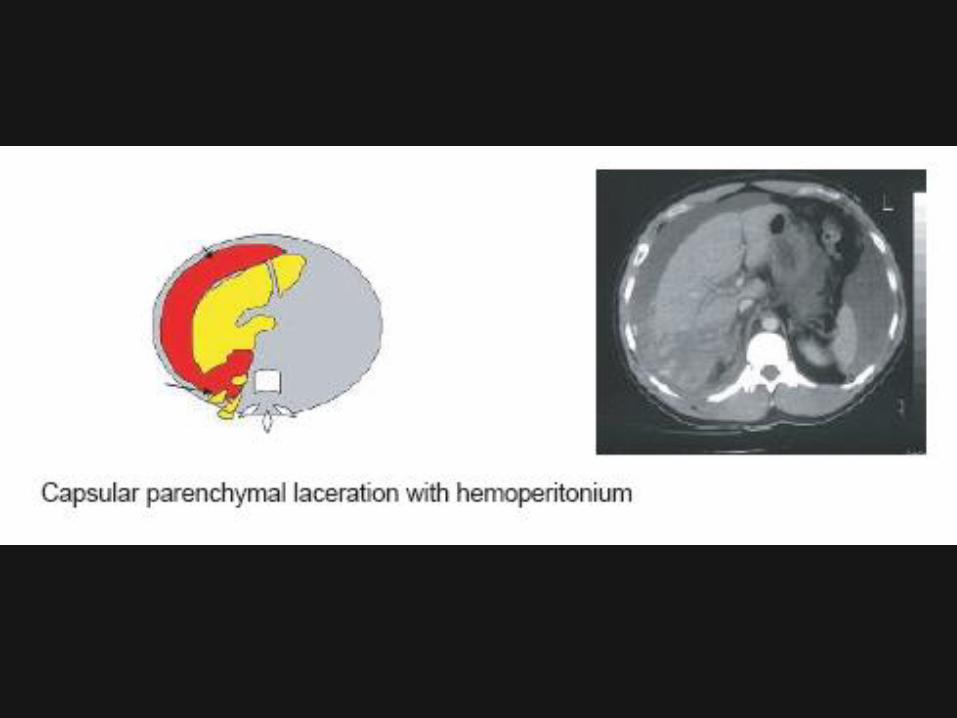
Grade 3: Parenchymal laceration more than 3 cm
deep and parenchymal or subcapsular hematoma
more than 3 cm in diameter

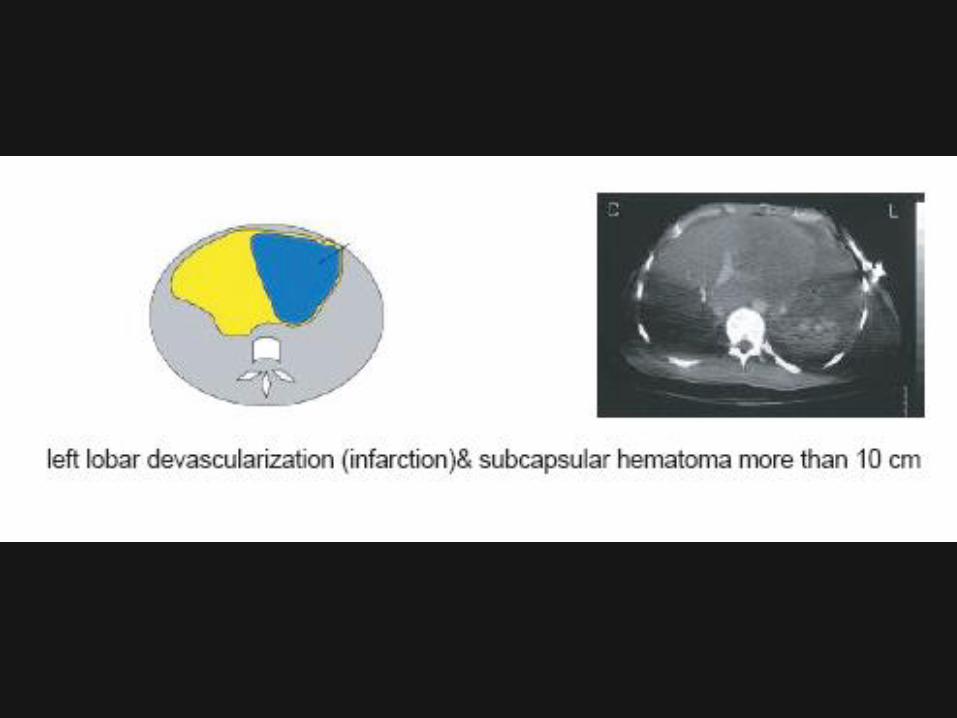
Grade 4: Parenchymal/subcapsular hematoma more
than 10 cm in diameter, lobar destruction, or
devascularization
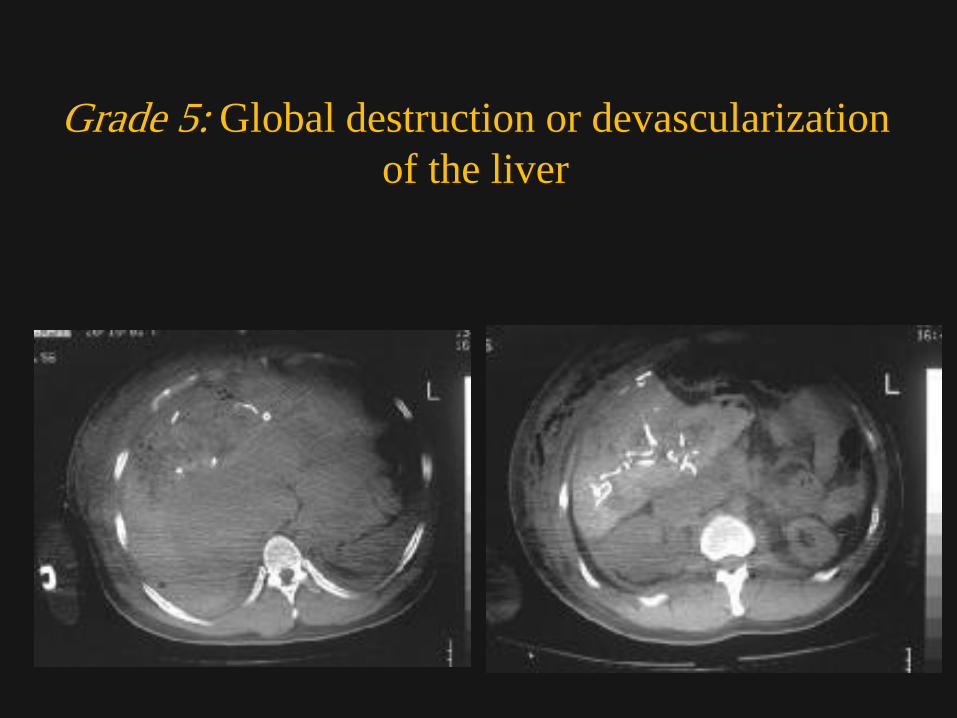
Grade 5: Global destruction or devascularization
of the liver

Grade 6 : Hepatic avulsion

The intravenously and oral
enhanced CT examination
of the abdomen
demonstrates the
presence of a linear area
of low attenuation within
the posterior segment of
the right lobe of the liver
(arrow heads). Fluid is
noted within Morrison's
pouch as well.
LIVER LACERATION

Interventional radiology for liver injury
concerns in embolization for active liver
bleeding
The dual blood supply of the liver makes
postembolization infarction less likely.
Penetrating injuries of the liver from stab
and gunshot wounds have been managed
successfully with transcatheter
embolization using similar criteria as those
in blunt hepatic injuries.
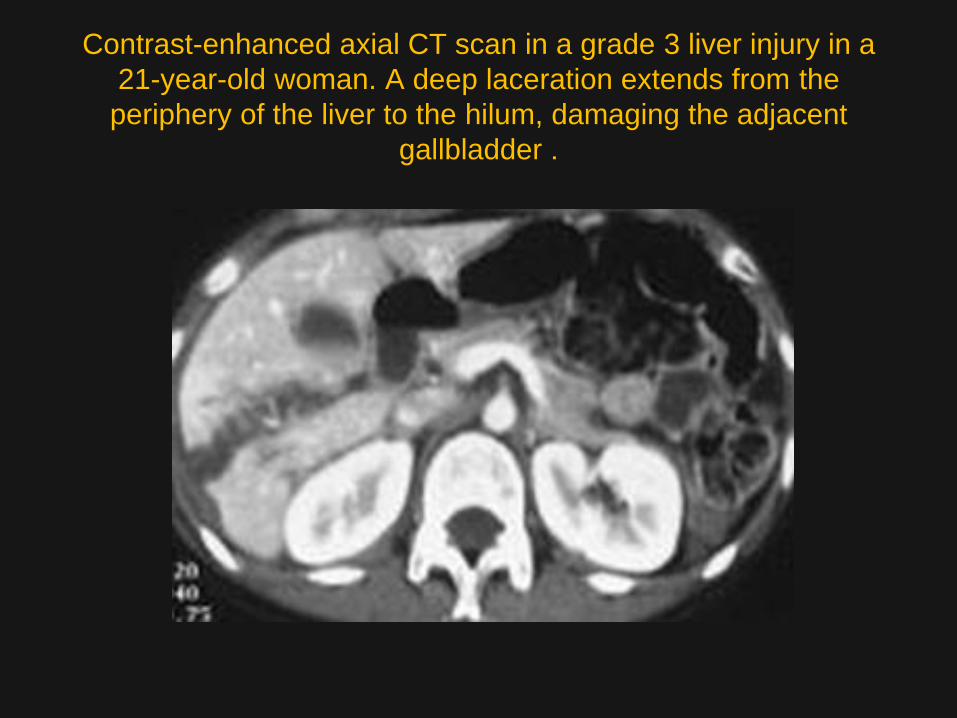
Contrast-enhanced axial CT scan in a grade 3 liver injury in a
21-year-old woman. A deep laceration extends from the
periphery of the liver to the hilum, damaging the adjacent
gallbladder .
Although CT remains the examination
of choice in the evaluation of liver
trauma, the procedure of choice to
evaluate bile leaks is 99mTc IDA
scanning

CT and ultrasonography can both help
detect intra-abdominal fluid, but
differentiation between loculated
ascitic fluid and hematoma, abscess,
and biloma may not be always
possible.

LARGE HEPATIC HAEMATOMA

SMALL PARENCHYMAL INJURY OF
THE LIVER

Contrast enhanced spiral CT: wide hematoma in the right lobe of the
liver with deep laceration extending to the IVC

Contrast enhanced spiral CT: another deep laceration is visible extending from
the hematoma to the inner hepatic border. Moreover the right adrenal is
disrupted and replaced by an extensive hemorrhage

Subcapsular haematoma

Subcapsular haematoma

Subcapsular haematoma

A)Grade 3 liver injury in a young male patient who fell off a bike. Transaxial CT
scan shows 5-cm-thick subcapsular and parenchymal hematoma containing
both high-density clotted and low-density unclotted blood
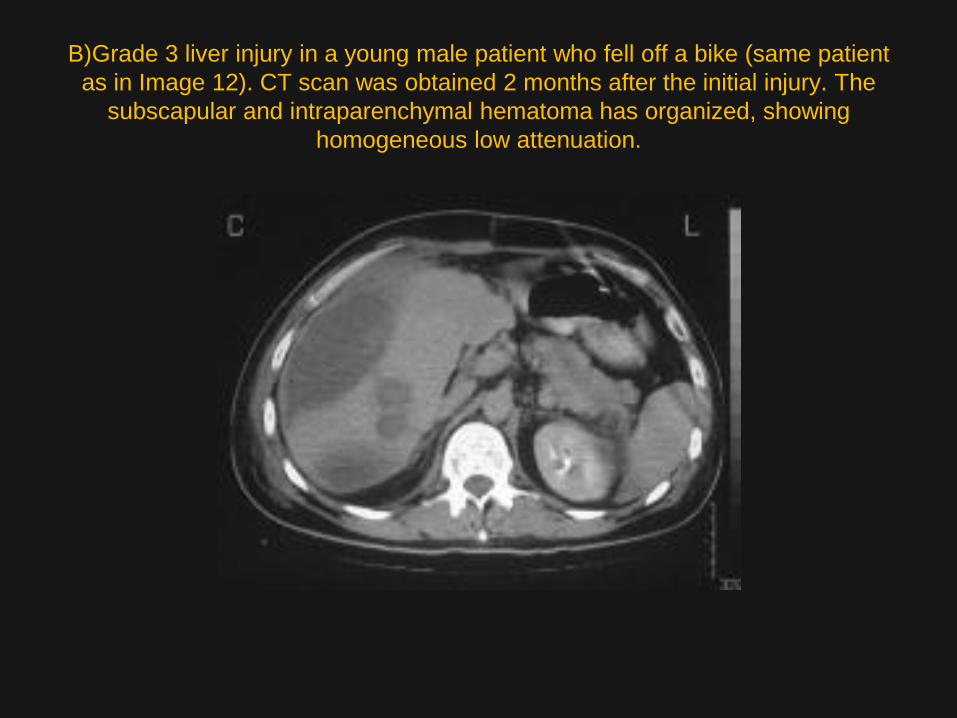
B)Grade 3 liver injury in a young male patient who fell off a bike (same patient
as in Image 12). CT scan was obtained 2 months after the initial injury. The
subscapular and intraparenchymal hematoma has organized, showing
homogeneous low attenuation.

A)Abdominal sonogram in a 35-year-old male bouncer after blunt
abdominal injury shows a crescent-shaped hyperechoic
collection along the right lateral aspect of the liver consistent with
subcapsular hematoma

C)Image in a 35-year-old male bouncer after blunt abdominal injury
(same patient as in Images 14-15). Diagram of the CT scan in Image

B)Image obtained in a 35-year-old male bouncer after blunt abdominal injury (same
patient as in Image 14). Nonenhanced axial CT scan of the abdomen demonstrates a
large subcapsular hematoma measuring more than 10 cm. The high-attenuating areas
within the lesion represent clotted blood. The injury was classified as a grade 4 liver injury

B)Diagram of the CT scan in Image 18 in a 39-year-old man with a grade 4 liver
injury shows a large parenchymal hematoma in segments 6 and 7 of the liver
with evidence of an active bleed.

A)Contrast-enhanced axial CT scan in a 39-year-old man with a grade 4 liver
injury shows a large parenchymal hematoma in segments 6 and 7 of the liver
with evidence of an active bleed. Note the capsular laceration and large
hemoperitoneum.
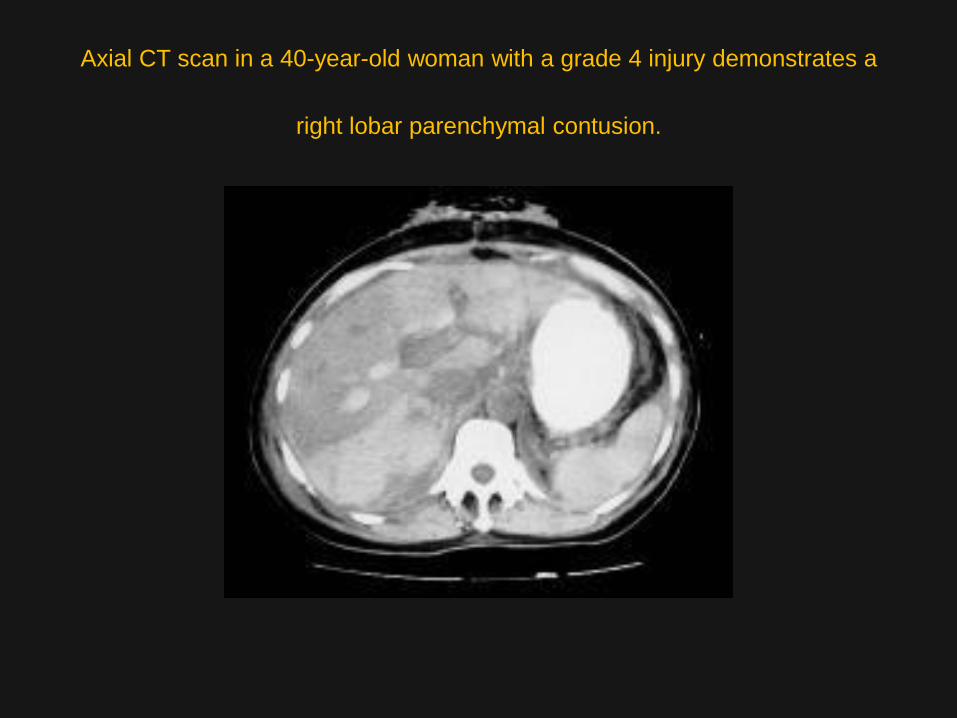
Axial CT scan in a 40-year-old woman with a grade 4 injury demonstrates a
right lobar parenchymal contusion.

THANK YOU