illustration of statewide adoption of nqf standards: identification of substance use conditions...
TRANSCRIPT
Illustration of Statewide Adoption of NQF Standards:
Identification of Substance Use Conditions
Rachel Gonzales, Ph.D.
Thomas E. Freese, Ph.D.
UCLA ISAP
Substance Abuse Research Consortium 2009 Meeting Series
Presentation ObjectivesPresentation Objectives
Provide you with an overview of the NQF Domain I: Identification of Substance Use in relation to: – What we know?What we know? – California’s Response
History of SBIRT development
Current efforts
The future

What do we know?
NQF: Identification DomainNQF: Identification Domain
Screening & Case Finding– Evaluation process allows for
determining whether an individual is at risk for or has an alcohol or drug problem
Assessment & Diagnosis– In-depth clinical process to determine
the specific tx needs of the individual when “screening” identifies risk for an alcohol or drug problem

Identification of Substance UseIdentification of Substance Use is a is a
Public Health PriorityPublic Health Priority……
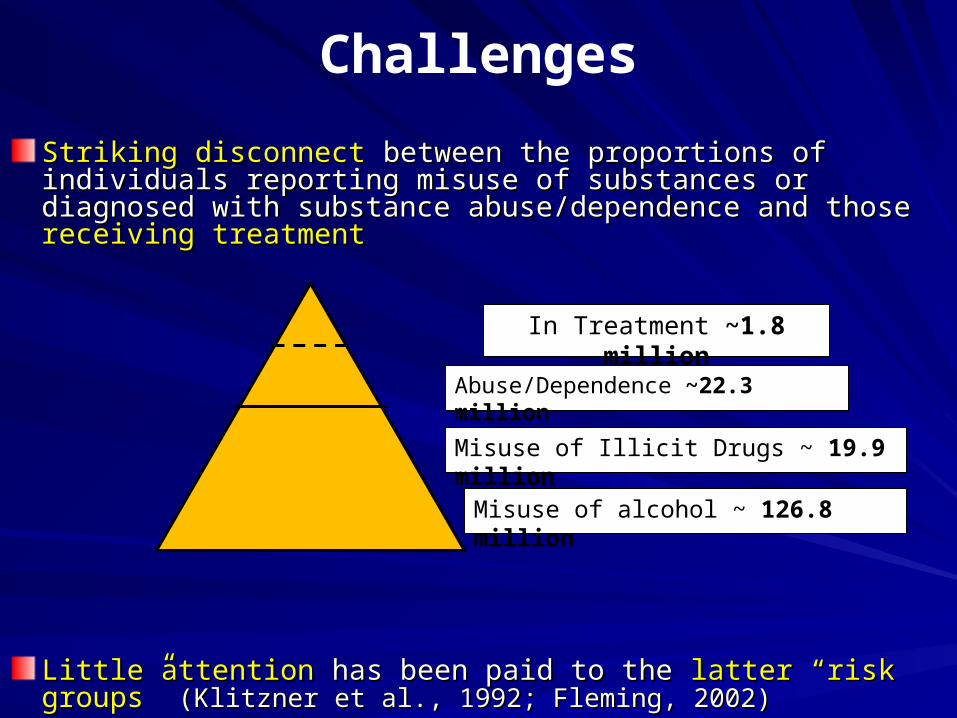
Challenges
Striking disconnect Striking disconnect between the proportions of individuals between the proportions of individuals reporting misuse of substances or diagnosed with substance reporting misuse of substances or diagnosed with substance abuse/dependence and those abuse/dependence and those receiving treatmentreceiving treatment
Little attention Little attention has been paid to the has been paid to the latter “risk groups” latter “risk groups” (Klitzner et al., 1992; Fleming, 2002)(Klitzner et al., 1992; Fleming, 2002)
In Treatment ~1.8 million
Abuse/Dependence ~22.3 million
Misuse of alcohol ~ 126.8 million
Misuse of Illicit Drugs ~ 19.9 million

Targeting Latter Risk Groups
AOD risk settings….
AOD Risk Settings
Health (including mental) Care– Primary care
– Emergency Rooms/Trauma Centers [40% 40% of visits are injury-related and 50% of them of visits are injury-related and 50% of them are alcohol-related (Nilsen et al., 2008)]are alcohol-related (Nilsen et al., 2008)]
Educational institutions
Criminal justice settings
Others…– Dental offices

Research of Identification in Health Care Settings
CASA Health care study: included 650 primary care physicians with over 500 patients in tx for chronic diseases:Findings: – LESS than 1/3 of PCP’s Screen
for Substance Use– ~50% of patients said “PCP
asked nothing of AOD use”– 10% said “PCP asked, but did
nothing”
Missed Opportunity: National Survey of Primary Care Physicians and Patients, the National Center on Addiction and Substance Abuse (CASA) @ Columbia University, NY 2000

Results from a member survey of American Association for the Surgery of Trauma:– Majority (~50%) screen
LESS than 25% of their patients – Issues:
>80 % no training in AOD screening75% not familiar with standard screening instruments
Research of Identification in Health Care Settings
Arch. Surg. Vol 134, May 1999

Why SBIRT?Why SBIRT?
A Public Health Early Intervention Solution:Screening, Brief Intervention & Referral to
Treatment - SBIRTIdentify patients who may not perceive a need for behavior change
Approaches are clinically effective and cost-efficient
Focus on at-risk vs. dependent individuals
Approaches are deemed an evidence based practice
SBIRT Approaches: Definitions
Screening: assesses the severity of substance use & identifies the appropriate response
Brief Intervention: focuses on increasing insight & awareness regarding substance use and motivation toward behavioral change:
Give feedback about screening results, inform patient about consuming substances, advise on and assess readiness to change, establish goals and strategies for change, and follow-up
SBIRT Approaches: DefinitionsBrief Treatment: consists of a limited number of
highly focused and structured clinical sessions with the purpose of eliminating hazardous and/or harmful substance use -- usually increased intensity and shorter duration than traditional treatment
Referral to Treatment: provides those identified as needing more extensive treatment with increased access to specialty treatment

Screening Score
SBIRT Approach Framework:Response Depends on Score*
Negative Screen
Positive Reinforcement
Brief Intervention
Brief Treatment
Referral to Treatment
Moderate Use Moderate/High Use Abuse/Dependence
*Severity & Consequences of use
Positive Screen

Overall SBIRT Goals
Increases access to care for persons with or at-risk for substance use disorders
Improves linkages between at-risk & AOD settings
Fosters a continuum of care: integrates prevention, intervention, and treatment services
Takes advantage of the “intervention moment…”

The Good News…
It Works!

It Works!
Well supported in health care settings
– Major impact on reducing morbidity & mortality
– Saves $: each dollar spent on SBIRT saves 4 dollars in other health-related costs
So…
– SBIRT required for certification of all Level I & II Trauma Centers
– U.S. Preventive Services Task Force recommends routine SBIRT in primary care settings
Babor & Kadden, 2005; Gentilello et al, 2005
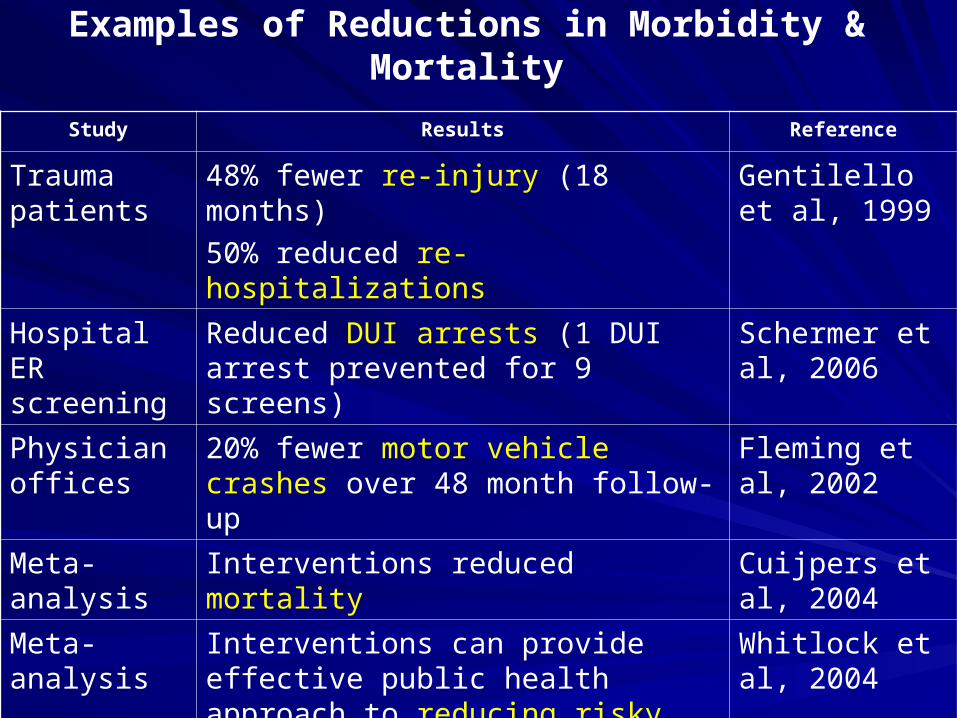
Examples of Reductions in Morbidity & Mortality
Study Results Reference
Trauma patients
48% fewer re-injury (18 months)
50% reduced re-hospitalizations
Gentilello et al, 1999
Hospital ER screening
Reduced DUI arrests (1 DUI arrest prevented for 9 screens)
Schermer et al, 2006
Physician offices
20% fewer motor vehicle crashes over 48 month follow-up
Fleming et al, 2002
Meta-analysis
Interventions reduced mortality Cuijpers et al, 2004
Meta-analysis
Interventions can provide effective public health approach to reducing risky use.
Whitlock et al, 2004
Research To date: Mostly Alcohol
Evidence for illicit drugs sparse…but promising
– Burke et al. 2003: Meta-analysis
– Bernstein et al. 2005: Randomized Controlled Trial
– WHO study 2008: Randomized Controlled Trial in multiple sites internationally
– Madras et al. 2009: SAMHSA program evaluation at multiple sites (intake vs 6 mo follow-up)
Overall Findings: SBIRT efforts related to positive outcomes (abstinence, increased health, social, legal,
economic, and vocational outcomes)
California Response
How has California been responsive to initiatives that use ‘screening & case finding’ techniques to identify individuals with substance use disorders?
SBIRT is a system change that will move a core mission of ADP forward…
…moving the AOD system to a comprehensive and integrated continuum of services system model
Importance of SBIRT in California?
Source: UCLA ISAP State Treatment Needs Assessment, 2001.
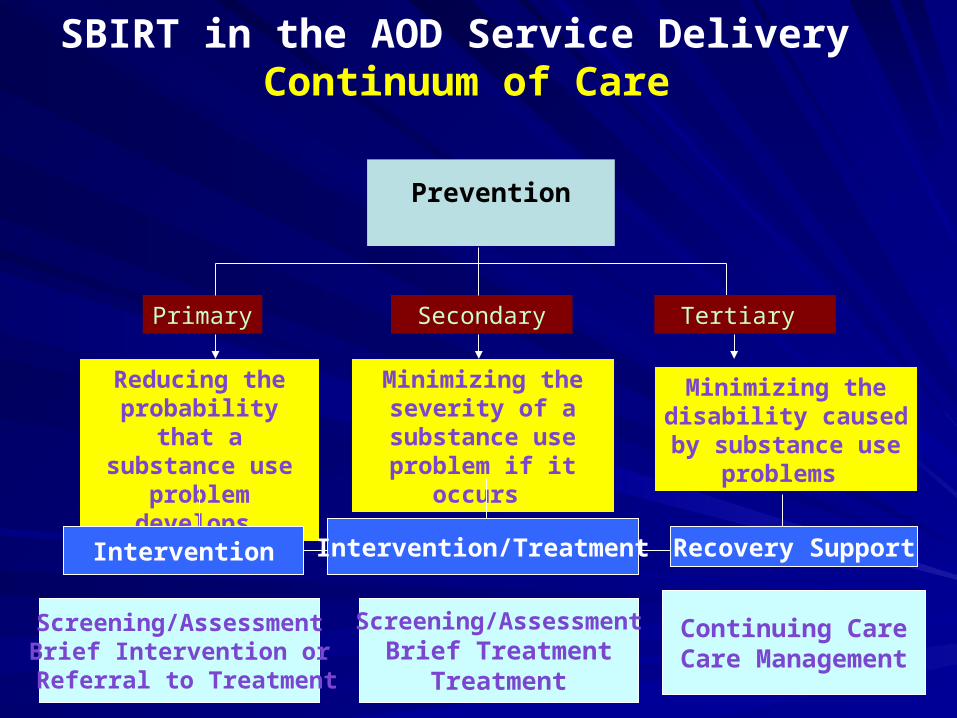
Prevention
SBIRT in the AOD Service Delivery Continuum of Care
Primary Secondary
Reducing the probability that a
substance use problem develops
Screening/AssessmentBrief Intervention or
Referral to Treatment
Screening/AssessmentBrief Treatment
Treatment
Continuing CareCare Management
Intervention Intervention/Treatment Recovery Support
Tertiary
Minimizing the severity of a
substance use problem if it occurs
Minimizing the disability caused by
substance use problems

Brief History: SBIRT Efforts in CA
California was selected as 1 of 7 states to participate in a national SBIRT demonstration project funded by SAMHSA (5-year cooperative agreement) – called CASBIRT
CASBIRT initiative – Administered by CA ADP – Managed by San Diego County, Alcohol & Drug Services
AND San Diego State University, Center on Alcohol and Other Drug Studies & Services

What is the CASBIRT Model?
SBIRT implemented in trauma, emergency (chest pain urgent care), & primary care settings throughout San Diego County
Patients 18+ are routinely screened by certified Health Educators during their visit using a standardized, scripted screening instrument
SBIRT service response made depending on score
CASBIRT staff: conduct evaluation by tracking patients deemed as “at-risk”, provide follow-up booster calls, and facilitate their participation in appropriate services

CASBIRT Effectiveness
To date, over 500,000 patients have received SBIRT services in SD county
Between 2005-06 alone, SBIRT performed with 125,000 patients– 48% of high risk clients completed at least one
Brief Treatment session – 74% stopped or reduced their substance use
Current status: funding by San Diego county AOD agency supported CASBIRT services through June 2009 (now looking to other grant mechanisms)
SBIRT in Educational SettingsSAMHSA Cooperative Agreement to implement SBIRT in College setting: UCLA Access to Care Project (2006-2009)
1st pick: Student Health Center (although not interested)
2nd pick: Counseling & Psychological Services– Given the prevalence of co-occurring substance
abuse/mental health disorders, counseling centers are good places for early intervention
– Serves over 6,000 students a yearSpear & Rawson

Access to Care Project Team
• SBIRT Implementation: UCLA Counseling & Psychological Services center clinical staff (n=28):
•Psychologists & LCSWs
•Interns (social work, post-docs)
• Project Liaison: ensure proper implementation by clinical staff
• SBIRT Evaluation: UCLA ISAP team (Spear, Rawson, Ransom)
Spear & Rawson
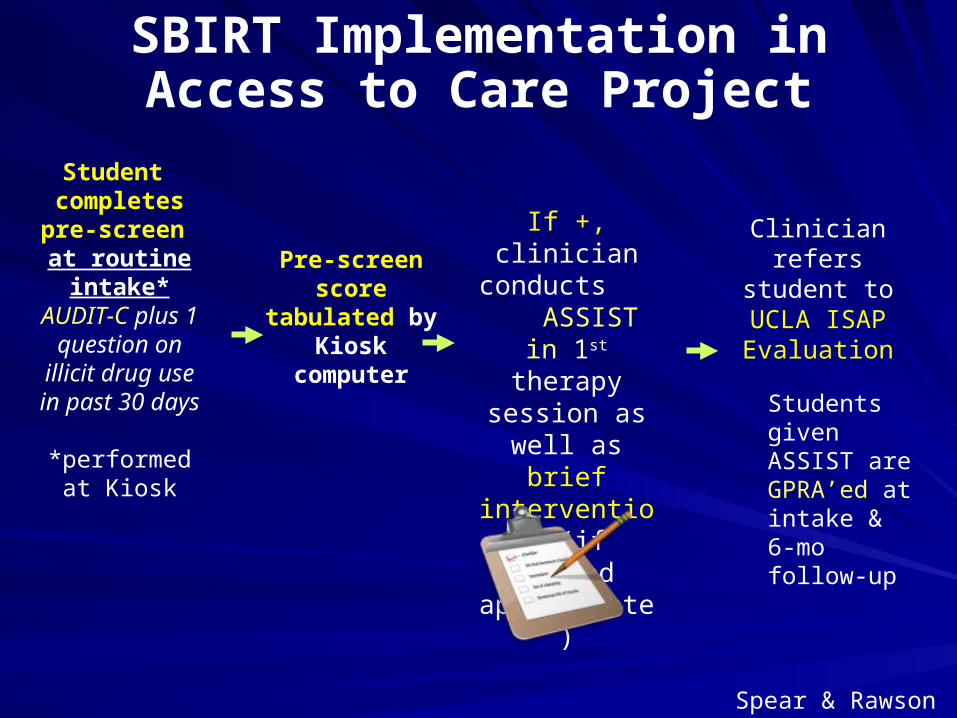
SBIRT Implementation in Access to Care Project
Pre-screen score
tabulated by Kiosk
computer
If +, clinician conducts ASSIST in 1st
therapy session as well as brief intervention (if
deemed appropriate)
Clinician refers student to UCLA ISAP
Evaluation
Student completespre-screen at routine
intake*AUDIT-C plus 1
question on illicit drug use in
past 30 days
*performed at Kiosk
Spear & Rawson
Students given ASSIST are GPRA’ed at intake & 6-mo follow-up
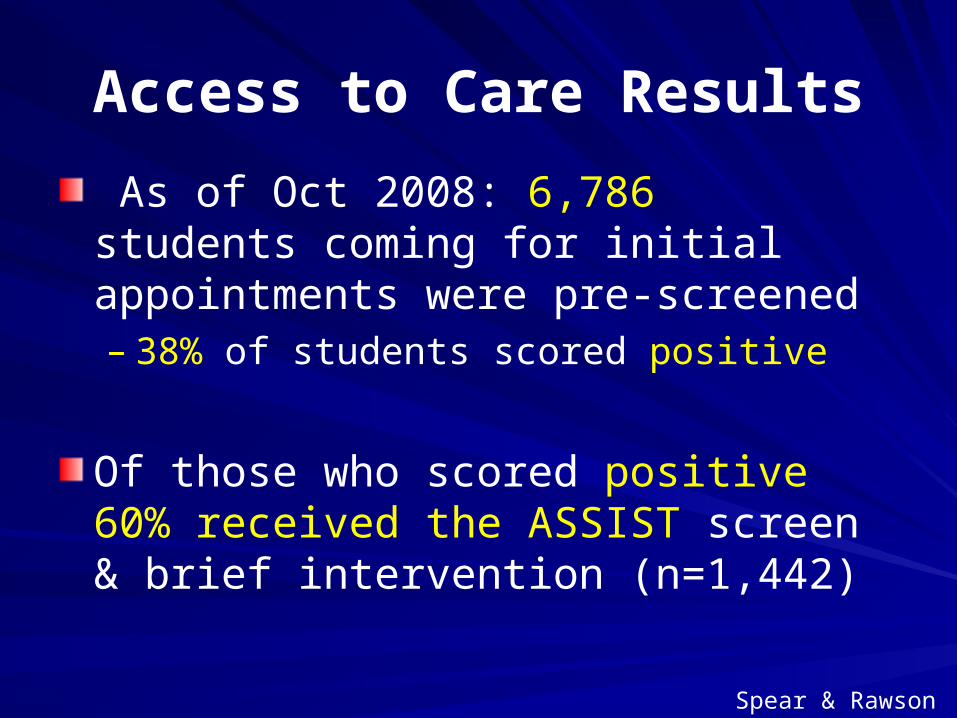
As of Oct 2008: 6,786 students coming for initial appointments were pre-screened– 38% of students scored positive
Of those who scored positive 60% received the ASSIST screen & brief intervention (n=1,442)
Access to Care Results
Spear & Rawson
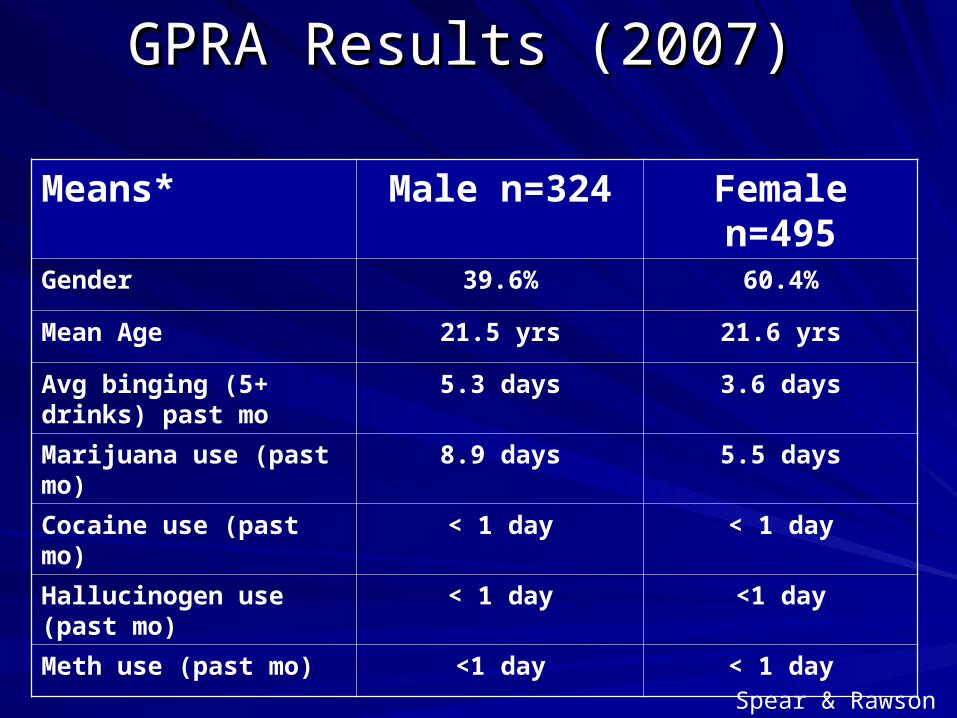
GPRA Results (2007) GPRA Results (2007)
Means* Male n=324 Female n=495
Gender 39.6% 60.4%
Mean Age 21.5 yrs 21.6 yrs
Avg binging (5+ drinks) past mo
5.3 days 3.6 days
Marijuana use (past mo) 8.9 days 5.5 days
Cocaine use (past mo) < 1 day < 1 day
Hallucinogen use (past mo)
< 1 day <1 day
Meth use (past mo) <1 day < 1 day
Spear & Rawson

GPRA Results: Binge DrinkingGPRA Results: Binge Drinking
85% of binge drinkers (n=425) received a brief intervention
46% of binge drinkers reported no binging at 6-mo follow up
Spear & Rawson
GPRA Results: MJ UseGPRA Results: MJ Use
37% (n=303) of students reported any marijuana use in past 30 days at intake Of these students, 87% (n=264) received a brief intervention Half (53%) of marijuana users reported no use at 6-month follow up
Spear & Rawson

Lessons learned: SBIRT in Educational Mental Health Settings
Has made mental health staff more aware of substance use issues among students
Offers mental health staff a more systematic approach for identification (less of a “judgment call”)
Allows college students to:– express concerns about their substance use– “shift their thinking” about their use
Spear & Rawson

Lessons learned: SBIRT in Educational Mental Health Settings
Implementation challenges
– Interrupts routine clinical flow: difficulty dedicating 15-20 minutes of customary 50-minute routine intake session to SBIRT
– Not enough time to do (and score) SBIRT in routine assessments (generally 30 minutes)
To address: UCLA ISAP team developed & pilot-tested a self-administered computer version of ASSIST (which is now used)– Briefer, efficient, feasible
Spear, S.E., Tillman ,S., Moss, C., Gong-Guy, E., Ransom, L., Rawson, R. Another way of talking about substance abuse: Substance abuse screening and brief intervention in a mental health clinic. In press. Journal of Human Behavior in the Social Environment.

Sustaining Implementation of SBIRT within College Campuses
System-wide training across the State

1st Training: March 2008
CSU Bakersfield
UC Merced
UC San Diego
UC Irvine
University of San Diego
CSU Long Beach
UC Riverside
Vanguard University
Occidental College
UC Santa Barbara
Woodbury University
UCLA hosted and trained (1 day) 11 counseling centers on SBIRT & use of the ASSIST
Spear & Rawson
Evaluation of 1st Training
Survey sent assessing implementation of the screening tool at their centers (n=11)
7 centers responded:
– 3 reported using the ASSIST
– 4 reported not doing any screening, but indicated that they “intend to use” the ASSIST when they have more time and staff to develop a plan
Spear & Rawson

2nd Training: Oct 2008
UCLA conducted day long SBIRT training with 7 additional colleges
Hosted at UCSF
UCSF
San Jose State University
CSU Sacramento
Notre Dame de Namur University
San Francisco State University
Santa Clara University
UC Berkeley
Spear & Rawson
Evaluation of 2nd Training
Survey sent related to implementation of screening tool – Only 2 implementing ASSIST
Barriers cited included: – Lack of time– Short staffed– Clinicians focused on other priorities– Limited resources – Need additional training – ASSIST doesn’t relate to students
Spear & Rawson

Integrating SBIRT into California Trauma
CentersTimeline: April 09-Nov 09
Under collaboration with ADP, UCLA is conducting large scale SBIRT training effort– Series of day-long
workshops on SBIRT with trauma centers, emergency departments & primary health care settings
Trainings offered during Spring, Summer and Fall 2009
Participant Counties (n=9)– Alameda– Ventura– Los Angeles– Santa Clara– Contra Costa– Santa Barbara– Fresno– Solano– Nevada
Data collection: GPRA
Freese & Rawson
Integrating SBIRT in CA Criminal Justice Settings
Implementation by CASCs– Homeless Healthcare LA– Behavioral Healthcare Services
Community Transition Unit Participants– LA County Jail (Twin Towers)– LA County Police Department (Parker Center)
Evaluation: UCLA doing GPRA
Rawson & Freese
Integrating SBIRT in CA Criminal Justice Settings
Under a SAMHSA grant, ADP, LA County (DPH, ADPA) & UCLA are conducting a 2-year pilot demonstration project: – Implementing SBIRT in 2 Community Transition
Units
Phase I: training staff on SBIRT & the ASSIST Phase II: Pre-screening all short-term stay detainees to identify AOD risk (low vs high) using AUDIT-C+ (3 etoh/2 drug)Phase III: ASSIST & BL GPRAPhase IV: Follow-Up (6-mo GPRA)
Rawson & Freese

Criminal Justice SBIRT Flow Chart
Short-term Detainees Pre-screened with
AUDIT-C+
Low-Risk DetaineesCASC
ASSISTModerate –
High Risk Detainees
Parker Center(n=5,000)
Information and Referrals Provided
Brief InterventionReferral if indicated
GPRA6-Month Follow-up
Twin Towers(n=5,000)
Rawson & Freese

Integrating SBIRT in CA Tribal Settings
Under a SAMHSA initiative, UCLA partnered with California Rural Indian Health Board (CRIHB) to provide SBIRT training for tribal organizations– Phase I: CRIHB identified specific tribal organizations and
clinics interested in training (Oct 08 – Mar 09) N=24– Phase II: UCLA conducted SBIRT/ASSIST training with
identified tribal organizations (2 large trainings: Apr 09 & Aug 09)
– Phase III: ASSIST implementation by tribal organizations
Depending on tribal community desires: ASSIST will be conducted with paper and pencil, using a personal interview or via computers
– Phase IV: Evaluation of adoption in tribal communities (future)
Rawson, Freese, Dickerson
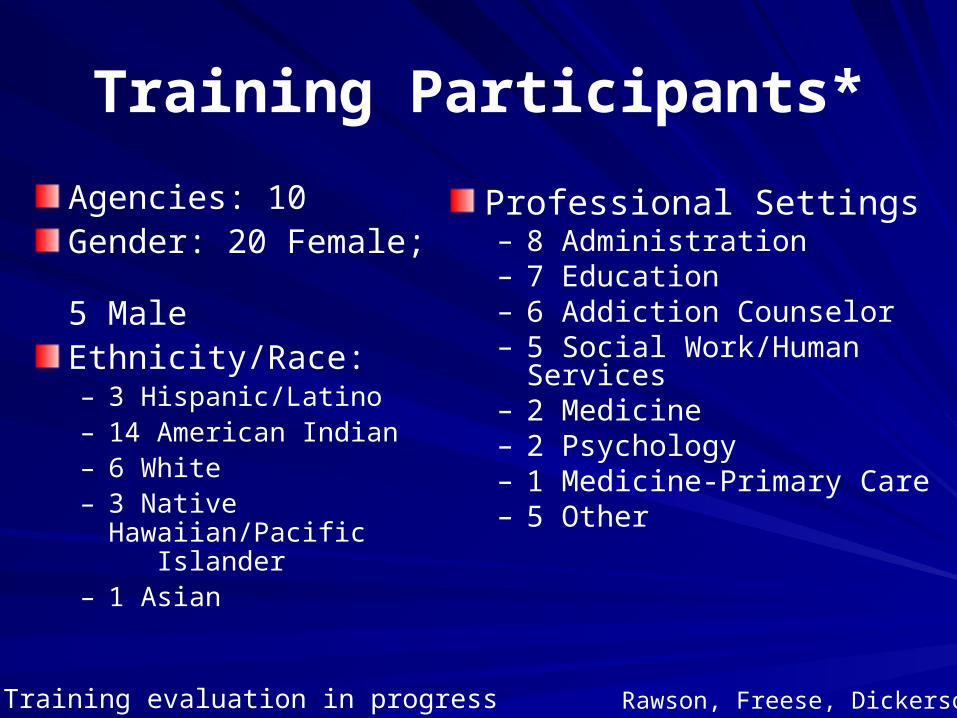
Training Participants*
Professional Settings– 8 Administration – 7 Education– 6 Addiction Counselor– 5 Social Work/Human Services– 2 Medicine– 2 Psychology – 1 Medicine-Primary Care– 5 Other
Agencies: 10Gender: 20 Female; 5 MaleEthnicity/Race:– 3 Hispanic/Latino– 14 American Indian– 6 White– 3 Native Hawaiian/Pacific
Islander– 1 Asian
*2nd Training evaluation in progress Rawson, Freese, Dickerson
Assessment & Diagnosis

What is Assessment/Diagnosis?Gathering information to:
Confirm the presence of an AOD problem
Identify the severity of the AOD problem & factors that affect AOD problems:– Social support networks– Employment– Health– Housing– Motivation to change– History of physical/sexual abuse– Mental illness status
Determine what services/treatment would be most effective
California Illustration II
Identification of Substance Use Disorders domain: Diagnosis and Assessment
California initiatives that require or recommend the use of a standardized biopsychosocial tool(s) for diagnosing and assessing individuals with substance use disorders
Pilot Project Efforts Underway
UCLA-ADP COSSR Evaluation work– Alameda working on developing a framework
to address this area
Issues:– Clarity on difference between assessment
and diagnosis (where does placement fit in?)– Identification on specific instrument to use for
each– Who should do the assessing & diagnosing?
Issues with staffing, training, conflicts of interest
Future Efforts
•Continuing evaluation of current efforts
•Establishing more funding to keep activities ongoing
•Expanding partnerships into other diverse settings, i.e., EDD, dental offices, juvenile justice, high schools, etc.
•White paper on SBIRT to disseminate CA experience

Acknowledgements
State ADPMichael Cunningham
Tony Becerra
UCLA ISAPRichard A. Rawson
Suzanne SpearLoretta RansomThomas Freese
Jerry CartierDan DickersonAnne Bellows
For More Information
http://sbirt.samhsa.gov/grantees/statecali.htm
http://www.casbirt.org/
www.uclaisap.org
www.sbirt.samhsa.gov
www.psattc.org

Thank you!Thank you!
Contact: – Rachel Gonzales
[email protected] (310) 267-5316– Thomas Freese
[email protected] (310) 267-5397
“Be kind, for everyone you meet is fighting a great battle.”
Philo of Alexandria